
Abstract
Hypertension and type 2 Diabetes (T2D) are highly associated and can promote an additive risk of mortality and hospitalization, as well as a significant burden on the Brazilian Unified Healthcare System. Despite this, blood pressure and glycemic control are still suboptimal and remain a significant challenge in Brazil. As it will be reviewed in this paper, current evidence supports the effectiveness of various dietary, exercise, and lifestyle interventions for hypertension and T2D. Among dietary interventions, the DASH diet appears to be particularly effective in reducing blood pressure and decreasing the risk of cardiovascular mortality, with a moderate effect on glycemic control. Regular physical activity, including aerobic, resistance, or combined exercise programs, is also recommended to reduce blood pressure, improve glycemic control and also reduce cardiovascular disease risk. Stress reduction programs have also been shown to be effective in reducing blood pressure. However, although numerous lifestyle interventions are effective for hypertension and T2D, factors such as personal preferences, motivation, and cultural background should be considered to ensure the long-term sustainability of these interventions. In addition, there is a need for further research to determine the cost-effectiveness of lifestyle interventions in the Brazilian population to encourage the development of evidence-based health policies.
“Public healthcare expenditure in Brazil is still low compared to other countries in the Organization for Economic Cooperation and Development (OECD).”
Introduction
Hypertension is one of the leading risk factors for cardiovascular disease (CVD), stroke and chronic kidney disease worldwide. Data from several population-representative studies showed that in 2019, over 1 billion people worldwide had hypertension, defined as systolic blood pressure (BP) equal to or greater than 140 mmHg or diastolic BP equal to or greater than 90 mmHg. 1 Type 2 diabetes (T2D) is another risk factor that increases the risk for CVD, macrovascular and microvascular disease and frequently coexists with hypertension. Importantly, results from the International Diabetes Federation Diabetes Atlas estimated that in 2019 around 463 million people worldwide had diabetes. 2 In fact, hypertension seems to be twice as frequent in patients with T2D than in patients without T2D. 3
Specifically in Brazil, previous meta-analyses estimated that T2D prevalence in Brazil ranged from 5.6 to 11.9%, 4 while hypertension prevalence ranged from 20.6-25.2%. 5 Hypertension and T2D are also associated with a major burden on the Brazilian Public Unified Healthcare System (UHS). To illustrate that, in 2018, a study by Nilson et al. estimated that the cost attributable to hypertension and T2D to the UHS was 375 million and 195 million dollars, respectively. 6 However, hypertension and T2D control are still major challenges in Brazil. Significantly, a previous systematic review by Picon et al. that pooled data from 11 studies showed that only 43.7-67.5% of hypertensive patients achieved BP control. 7 Regarding T2D, a cross-sectional study including patients from 14 centers from five regions of Brazil showed that only 26% of T2D patients had an HbA1C <7%. 8
It is known that lifestyle interventions are cost-effective and are a main component of chronic disease management.9,10 This was illustrated in a previous randomized controlled trial (RCT) by Taheri et al, which showed that intensive-lifestyle intervention was associated with diabetes remission in over 60% of participants at 12 months. 11 Previous data from RCTs also showed that lifestyle interventions can reduce systolic BP by 4-11 mmHg, an effect size comparable to antihypertensive monotherapies.12,13 Therefore, this paper aims to comprehensively review evidence-based lifestyle medicine interventions that can aid hypertension control in T2D patients in Brazil.
The Hypertension-Based Chronic Disease Model
To face the burden of obesity and T2D, the American Association of Clinical Endocrinology (AACE) and the American College of Endocrinologists (ACE) introduced the Adiposity-Based Chronic Disease (ABCD) and Dysglycemia-Based Chronic Disease (DBCD) models.14,15 These chronic disease models provide a framework for risk-estimation and identify potential intervention targets to prevent ABCD and DBCD progression.14,15 Since ABCD, DBCD, hypertension, and dyslipidemia are highly associated with each other and with CVD, these cardiometabolic drivers were subsequently incorporated into the Cardiometabolic-Based Chronic Disease (CMBCD) model.9,10 The interactions between ABCD, DBCD, HBCD and complications are detailed in Figure 1.
In the CMBCD model, stage 1 (“risk”) describes the primary drivers that lead to initial cardiometabolic derangements; stage 2 (“predisease”) the mild anatomical or biochemical cardiometabolic derangements that lead to disease; stage 3 (“disease”) the more severe anatomical or biochemical cardiometabolic derangements that lead to complications; and stage 4 (“complications”) the significant morbidity/mortality attributable to CVD.9,10
Importantly, hypertension evolves in the same stepwise fashion as ABCD and DBCD drivers, progressing from stage 1 (due to interacting effects of primary drivers: genetics, environment, and behavior) to stage 2 (prehypertension), to stage 3 (hypertension) and, finally, stage 4 (hypertension complications).16–19 Based on this construct, hypertension can be formulated as an additional secondary/metabolic driver of CMBCD, to further improve the capability of risk-estimation of the CMBCD model and provide intervention targets before the development of complications.
20
This review will focus on lifestyle interventions that target not only HBCD but also ABCD and DBCD drivers to mitigate the risk of progression from stage 3 HBCD (hypertension) to stage 4 (complications). Adiposity- and dysglycemia-based chronic disease drivers and their relationship with hypertension-based chronic disease.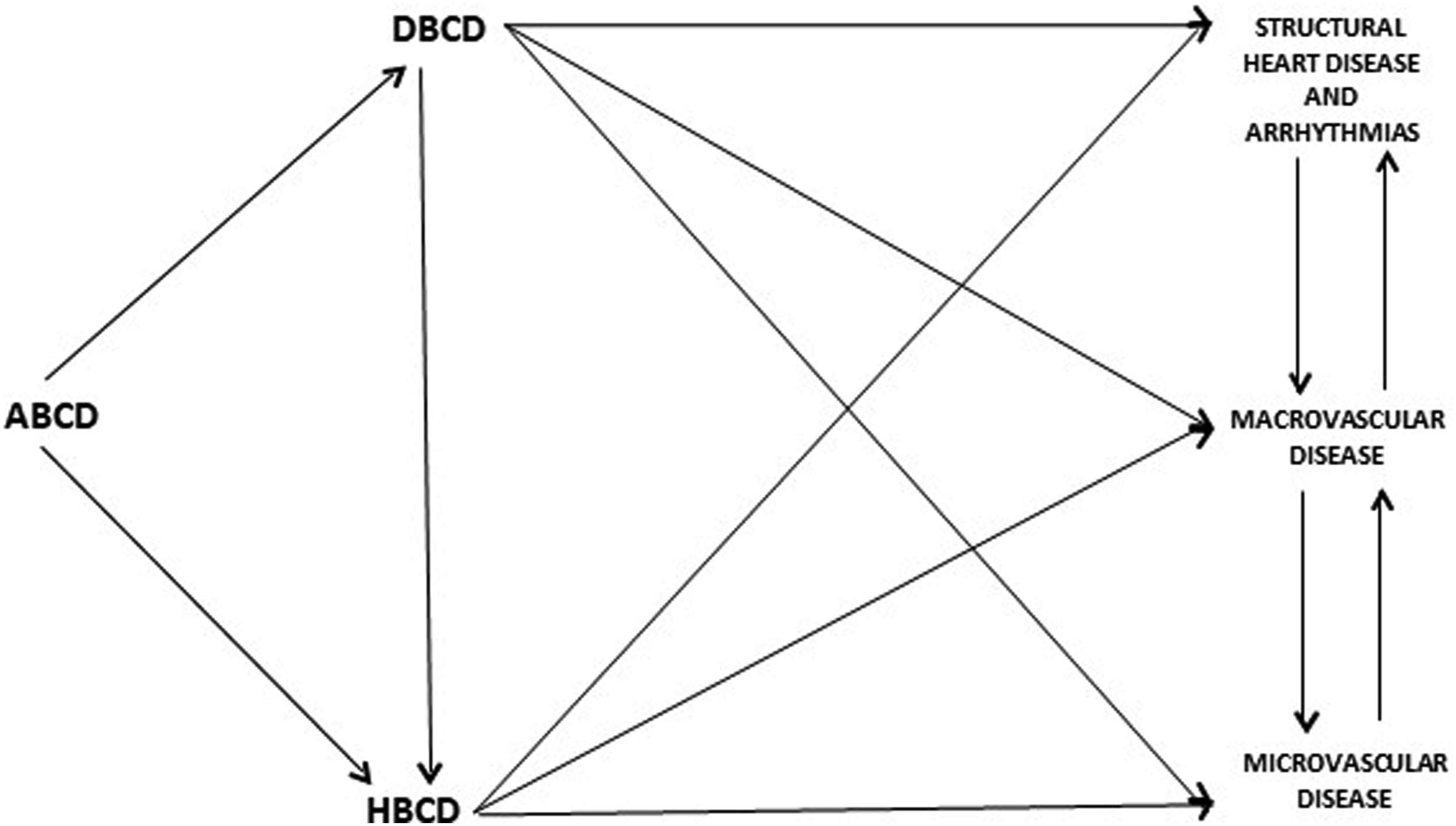
Hypertension and Diabetes Risk Factors in Brazil
It is known that environmental, cultural, and behavioral risk factors can increase the risk for cardiometabolic diseases such as hypertension and T2D. 9 Brazil has a population of over 210 million individuals, with a median age of 33.2 years and 90% of the population residing in urban areas.21,22 These demographic factors serve as critical considerations when examining the burden of cardiometabolic diseases and formulating effective preventive and intervention strategies in Brazil. Importantly, previous data from the Brazilian National Health Survey showed that the prevalence of HTN increases significantly in higher age categories, with 20.3% of individuals aged 30-59 years having hypertension, compared with 46.9% of individuals aged 60-64 years. 23 This same trend was observed for diabetes in Brazil, with an estimated diabetes prevalence of 2.5% in individuals aged 30-34 years and 12% in individuals aged 60-64 years. 24 Regarding HTN prevalence in urban compared to rural areas, previous studies showed a similar prevalence (21% and 20.1%, respectively). However, urban areas had a significantly higher prevalence of T2D compared with rural areas (6.5% vs 4.6%, respectively).
Previous data from the Brazilian VIGITEL study, which included over 54 000 adults nationwide, found a high prevalence of cardiometabolic disease risk factors. 25 For instance, among participants, 48.5% were overweight, 15.8% had obesity, 14.8% were smokers, 14% reported having a sedentary lifestyle, 17% reported high consumption of alcohol (five or more doses daily for men and four or more doses daily for women) and 29.8% reported consuming soft drinks over 5 days/week. 25 On the other hand, only 36% of subjects consumed fruits and vegetables at least 5 days/week and only 30.3% had an adequate amount of physical activity (at least 150 minutes of mild or moderate-intensity physical activity per week or at least 75 minutes of vigorous-intensity physical activity per week). 25
Certain dietary patterns (e.g., high sodium intake, high consumption of ultra-processed foods or soft drinks and added sugar intake) are also known to increase the risk for hypertension and T2D and are common in Brazil.26-30 For instance, a national cross-sectional study by Louzada et al showed that 21.5% of daily caloric intake was provided by ultra-processed foods, while processed foods provided 9% of caloric intake for Brazilians. 31 A cross-section analysis by Scapin et al. also showed that 71% of 4539 packaged products sold in a major Brazilian supermarket had some type of added sugar. 32 In addition, an analysis of a nationwide Brazilian survey by Levy et al. found that 16.7% of total energy consumption came from added sugars. 33 Beyond that, Levy et al. showed that the ratio of table sugar/sugar added to processed foods was inversely proportional to increases in income. 33 Moreover, an analysis of sweetened beverages consumption among adults in Brazilian capitols by Figueiredo et al. showed that in 2016, the average consumption of sweetened beverages was 287.6 mL daily, while 16.5% of participants consumed sweetened beverages ≥5 days per week. 34 Furthermore, estimates from the National Health Survey showed that Brazilians have an average consumption of 9.34 g of salt daily, much higher than the World Health Organization recommendation of 5 g/day. 35
Lifestyle Interventions to Manage Hypertension in Type 2 Diabetes
Weight Loss
Weight loss is widely known as one of the mainstay lifestyle intervention goals that can significantly improve BP and glycemic control in hypertensive and T2D patients. A meta-analysis by Neter et al. that included 25 RCTs showed that a weight reduction of 5.1 kg reduced systolic BP by 4.44 mmHg and diastolic BP by 3.57 mmHg. 36 In addition, this study found that per kilogram of weight-loss systolic and diastolic BP were reduced by 1.05 mmHg and .92 mmHg, respectively. 36 For patients with T2D and obesity or overweight, a systematic review by Gummesson et al. showed that for each kilogram of weight loss, there was a mean HbA1c reduction of .1%. 37 In addition, Gummesson et al. found that reductions in HbA1c related to weight-loss were significantly greater in patients with poor glycemic control compared with T2D diabetic patients with adequate glycemic control. 37 To achieve significant weight-loss current American Diabetes Association recommendation advise a daily energy deficit of 500-750 kcal, which can be achieved attained both through nutritional changes or an increase in energy expenditure. 38
Dietary Interventions
Transculturalization of Chronic Disease-Dietary Interventions
While numerous dietary strategies have been shown to improve BP control and decrease the risk of CVD in individuals with T2D, it is essential to personalize these interventions to each individual. Factors such as personal preferences, motivation, and cultural background should be considered to ensure long-term adherence and sustainability of the dietary plan.
DASH Diet
The Dietary Approaches to Stop Hypertension (DASH) diet is a dietary pattern that emphasizes the consumption of fruits, vegetables, whole grains, low-fat dairy products and lean protein sources while limiting the intake of saturated fat, total fat, and cholesterol. In a previous meta-analysis that analyzed 30 RCTs, comprehending 5545 participants with and without hypertension, DASH diet reduced systolic BP by -3.2 mmHg and diastolic BP by −2.5 mmHg. 39 Importantly, the presence of hypertension did not modify the effect of DASH diet on BP reduction. 39 In addition, in this same study, DASH diet reduced systolic BP by a greater extent compared with the control diet in RCTs with sodium intake >2400 mg/day. 39 The effect of DASH diet on BP reduction was further explored in a meta-analysis that included RCTs that investigated the effect of different dietary patterns specifically on patients with hypertension and T2D. 40 In this meta-analysis, a low-sodium diet was the most effective in reducing systolic BP, followed by high-fiber diet and DASH diet. 40 Nonetheless, in this study DASH diet had no effect on reducing diastolic BP, while a high-fiber diet was the most effective followed by low-fat and low-protein diet. 40 Furthermore, Sukhato et al. conducted an umbrella review that included 50 systematic reviews and meta-analyses of RCTs that studied the effect of dietary interventions on systolic and diastolic BP, such as DASH, Mediterranean, Nordic, vegetarian, low-salt, low-carbohydrate, low-fat, high-protein, low glycemic index, portfolio, pulse, and Paleolithic diets. 41 Importantly, in this study they found that the DASH diet was associated with the greatest overall reduction in BP. 41
Data from RCTs about the effect of DASH diet on hard outcomes in patients with hypertension is still lacking. However, a previous meta-analysis of observational studies, that included both hypertensive and non-hypertensive subjects, showed that each 5-point increase in adherence to the DASH diet was associated with a reduction of 5% in all-cause mortality, 4% in cardiovascular mortality and 3% in stroke compared with the control diet. 42 The association between DASH diet adherence and CVD mortality was further explored in a study by Talaei et al, that included 57 078 Asian subjects with and without hypertension. 43 In this study, the quintile with the highest adherence to DASH diet had a 24% lower risk of CAD mortality and 38% lower risk of stroke mortality compared with the quintile with the lowest adherence to DASH diet. 43 Although effective for hypertension control, it is still unclear if DASH diet can also aid glycemic control in patients with hypertension and T2D. However, two meta-analyses of RCTs that included patients with different chronic diseases found that DASH diet had no effect on blood glucose, insulin or HOMA-IR compared with control diets.44,45 A previous umbrella review of systematic reviews and meta-analysis by Chiavaroli et al. further studied the effect of DASH diet on outcomes and glycemic control and showed that the DASH dietary pattern was associated with a 20% lower risk of CVD, 21% lower risk of coronary heart disease, 19% lower risk of stroke and 18% lower risk of diabetes in cohort studies. 46 Moreover, Chiavaroli et al. also showed that DASH diet led to a significant average reduction of HbA1c by −.53%, fasting blood insulin by −.15 μU/mL and body weight by −1.42 kg in RCTs. 46 Due to these benefits, the 2023 American Diabetes Association Standards of Care in Diabetes recommends adopting the DASH diet to improve BP control in T2D patients. 47
The Modified DASH diet is similar to the original DASH diet in terms of macronutrient distribution, but includes a greater variety of foods and more flexible portion sizes, which could be useful to adapt this eating pattern to the Brazilian culture. A previous meta-analysis that included 10 RCTs showed that the modified DASH diet significantly reduced mean systolic BP by 3.26 mmHg and diastolic BP by 2.07 mmHg compared to the control diet in patients with prehypertension or hypertension. 48 Also, this meta-analysis showed that BP reduction was larger in patients with a mean baseline BP ≥140/90 mmHg. 48
Mediterranean
The Mediterranean diet is a dietary pattern that emphasizes the consumption of plant-based foods, such as fruits, vegetables, whole grains, legumes, and nuts. It also includes moderate amounts of fish and seafood, and small amounts of lean meats and dairy products. The Mediterranean diet is characterized by the use of olive oil as the primary source of fat, and the use of herbs and spices to flavor food. The Mediterranean diet also includes moderate amounts of wine, typically consumed with meals.
A previous meta-analysis that included 35 RCTs, comprehending 13 943 participants showed that the Mediterranean diet significantly reduced mean systolic BP by 1.5 mmHg and diastolic BP by .9 mmHg compared with control (usual diet or other dietary interventions). 49 However, when compared only with other dietary interventions (low-fat, low-carbohydrate, Brazilian, hypolipidemic, prudent and central European) the Mediterranean diet did not reduce systolic or diastolic BP. 49 Moreover, this same study showed that the mean diastolic BP reduction was higher in trials that included participants with a mean baseline systolic BP of 130 mmHg or higher, although a difference in systolic BP reduction was not observed. 49
Specifically, in patients with T2D, a meta-analysis of 9 RCTs, with 1178 participants, showed that the Mediterranean diet led to significantly higher reductions in HbA1c (−.30%), fasting plasma glucose (−.72 mmol/l), fasting insulin (−.55 μU/ml) compared with control diets. 50 Importantly, the Mediterranean diet was also associated with a systolic BP reduction of 1.45 mmHg and a diastolic BP reduction of 1.41 mmHg. 50 Furthermore, reductions in body mass index, body weight, total cholesterol and triglyceride were also observed, while HDL-c was increased. 50 Regarding outcomes in patients with diabetes, data from another meta-analysis that included 3 RCTs revealed that the Mediterranean diet reduced the risk of CVD incidence by 38% and myocardial infarction incidence by 35%. 51 In addition, in this study, authors combined data from 38 cohort studies and showed that the group with the highest adherence to the Mediterranean diet was associated with a 21% lower risk of CVD mortality, 27% lower risk of coronary heart disease incidence, 17% lower risk of coronary heart disease mortality, 20% lower risk of stroke incidence, 13% lower risk of stroke mortality, and 27% lower risk of myocardial infarction incidence. 51
Other Plant-Based Diets
Plant-based diets (e.g., vegetarian, veganism, flexitarian) are dietary patterns that primarily consist of foods derived from plants, including fruits, vegetables, whole grains, legumes, nuts, and seeds. These diets may include a variety of plant-based foods and may exclude or greatly limit animal products such as meat, dairy, and eggs.
A previous meta-analysis of RCTs that investigated the effect of different plant-based diets on BP showed that a vegan diet reduced systolic BP by 1.30 mmHg, lacto-ovo vegetarian by 5.47 mmHg, high-fiber by .65 mmHg, while high-fruit and vegetable reduced systolic BP by .57 mmHg, although the certainty of results was low for the vegan, high-fruit and vegetable and high-fiber diets. 52 Moreover, a meta-analysis of RCTs that focused specifically on vegetarian diets observed that vegetarian diets significantly reduced systolic BP by −2.66 mmHg and diastolic BP by −1.69 mmHg compared to omnivorous diets. 53 In addition, they found that vegan diet was associated with a greater reduction in systolic BP compared with the lacto-ovo-vegetarian diet. 53
In patients with T2D, a previous meta-analysis that included 6 RCTs showed that vegetarian diets were associated with a significant reduction in HbA1c by .39%, although there was not a significant reduction in fasting blood glucose compared with control diets. 54 Vegan diets also appear to improve glycemic control, with data from a systematic review of observational studies and RCTs showing that vegan diet was associated with an HbA1c reduction ranging from .3 to 1.4%. 55
Plant-based diets also appear to reduce the risk of CVD. 56 For instance, a meta-analysis of cohort studies including 698 707 participants showed that the highest adherence to plant-based diets was associated with a 16% lower risk of CVD and a 12% lower risk of coronary heart disease compared with the lowest adherence. 56 A systematic review and meta-analysis that included 67 studies, with a total of 3 826 137 participants further confirmed the protective effect of plant-based diets on health outcomes and showed that adherence to a plant-based diet was associated with a 20% lower risk of T2D, 11% lower risk of CVD and 15% lower risk of all-cause mortality. 57
Nordic
The Nordic diet is a dietary pattern that is characterized by a high intake of fish, whole grains, fruits and vegetables, and a moderate intake of dairy products and meat. The diet is based on traditional foods that are commonly consumed in Nordic countries (Denmark, Finland, Iceland, Norway, and Sweden). It emphasizes the use of locally-sourced, seasonal ingredients and is rich in healthy fats, antioxidants, and fiber. It also encourages a low intake of added sugars and processed foods.
A previous meta-analysis that included 3 RCTs that investigated the effect of the Nordic diet on BP showed that the Nordic diet significantly lowered systolic BP by 5.20 mmHg and diastolic BP by 3.85 mmHg. 58 Regarding outcomes, a meta-analysis that included 13 cohort studies, with over 930 thousand subjects, showed that the highest adherence to the Nordic diet compared to the lowest category of adherence was associated with a 22% lower risk for all-cause mortality, 12% lower risk for cardiovascular mortality, 14% lower risk for cancer mortality, 12% lower risk for stroke, 20% lower risk for myocardial infarction and 10% lower risk for T2D. 59 Concerning glycemic control, a meta-analysis of 6 RCTs did not find a significant effect of the Nordic diet on fasting blood glucose levels, although it significantly reduced serum insulin concentrations and the homeostasis model assessment for insulin compared to control diets. 60 However, further studies are still needed to find if the Nordic diet can significantly impact HbA1c levels in T2D patients.
Brazilian
The traditional Brazilian diet is characterized by a high intake of carbohydrates, such as rice and beans, as well as a variety of fruits and vegetables. Meat, particularly beef, is also an important part of the diet, and it's usually consumed in large amounts. The traditional diet also includes a moderate intake of dairy products and a low intake of fats. However, in recent years, the Brazilian diet has been influenced by modern eating habits, with a significant increase in processed foods and fast food, which has led to an increase in obesity and related health issues.
Dietary Interventions and Their Effect on Blood Pressure, Glycemic Control and Clinical Outcomes in Patients With Hypertension and Type 2 Diabetes.
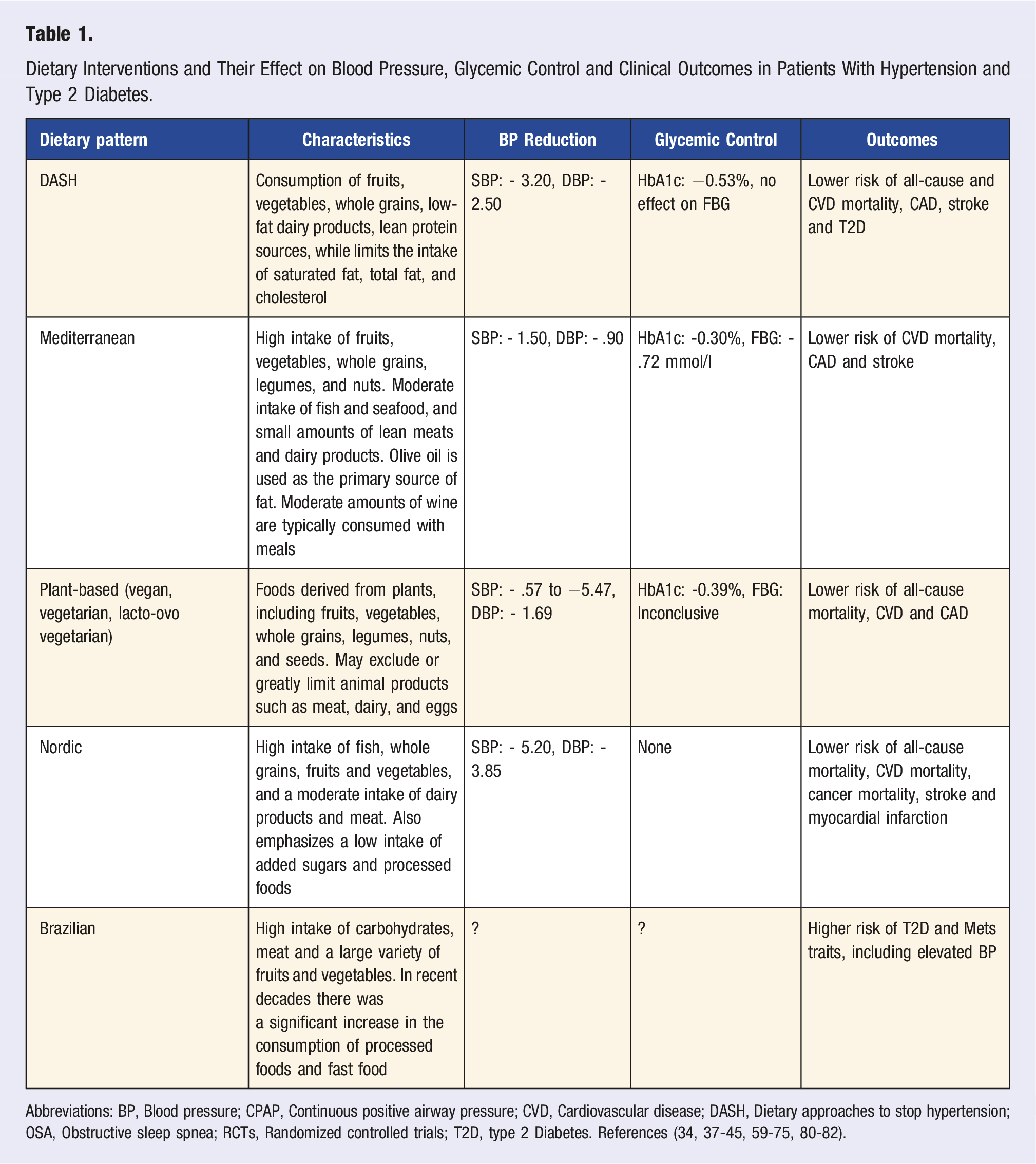
Abbreviations: BP, Blood pressure; CPAP, Continuous positive airway pressure; CVD, Cardiovascular disease; DASH, Dietary approaches to stop hypertension; OSA, Obstructive sleep spnea; RCTs, Randomized controlled trials; T2D, type 2 Diabetes. References (34, 37-45, 59-75, 80-82).
Sodium and Potassium
Robust evidence from several RCTs shows that sodium intake reduction significantly reduces systolic and diastolic BP linearly and this effect is even more pronounced in patients with higher BP levels. 62 A previous meta-analysis that included over 616 thousand subjects also showed that individuals with high sodium intake had a 19% higher risk of CVD compared with individuals with low sodium intake. 63 Moreover, this study showed that the risk of CVD increased by 6% for every 1 g increase in sodium intake. 63 A low-sodium diet should be encouraged and education regarding reduced sodium intake should be provided. Specifically, in patients with T2D, a meta-analysis of 8 RCTs showed that sodium restriction significantly reduced systolic BP by −5.57 mmHg and diastolic BP by −1.67 mmHg, an effect size similar to that of single drug therapy. 64 Consequently, the current American Diabetes Association recommends restricting sodium intake to less than 2300 mg/day for patients with hypertension and T2D. 47
Furthermore, potassium intake seems to be associated with BP reduction. To illustrate that, a meta-analysis that included 15 RCTs showed that potassium supplementation reduced systolic BP by 4.7 mmHg and diastolic BP by 3.5 mmHg in hypertensive or non-hypertensive patients without the use of antihypertensive medication. 65 In addition, in this same study, they found that the effect of potassium supplementation was significantly greater in hypertensive patients, with a reduction of systolic BP by 6.8 mmHg and diastolic BP by 4.6 mmHg. 65 Since potassium intake can also aid BP control, one of the pillars of a comprehensive lifestyle intervention would be to incorporate potassium-rich foods into the diet. This is reflected by the latest American Diabetes Association recommendations to increase the consumption of fruits and vegetables to 8-10 servings per day. 47
Strategies that reduce sodium and increase potassium intake, such as the use of salt substitutes may also be useful to increase BP reduction. For instance, a previous open label randomized trial showed that the use of a salt substitute (75% sodium chloride and 25% potassium chloride), significantly reduced the rates of stroke, cardiovascular events and all-cause mortality compared with regular salt in patients who had a history of stroke or were 60 years of age or older and had high blood pressure. 66
Alcohol Intake
Evidence on alcohol intake in hypertension and T2D is still controversial. To illustrate that, a meta-analysis that included 36 RCTs with 2865 subjects showed that a reduction in alcohol intake was not associated with BP reduction in participants who drank two or fewer drinks per day. 67 However, in this same study, a decrease in alcohol consumption was significantly associated with a reduction in systolic and diastolic BP in participants who drank more than two drinks per day. 67 For patients with T2D, evidence from a meta-analysis of RCT showed that moderate alcohol consumption had no effect on estimated insulin sensitivity or fasting blood glucose levels but significantly reduced HbA1c by .62% and fasting insulin concentrations by .19 units/L compared with the control group. 68 Regarding the risk of complications, a meta-analysis that included 27 observational studies with a total of 1 425 513 individuals showed that low alcohol intake (<15 g/day) was associated with a 15% lower risk of total stroke, 19% lower risk of ischemic stroke and 33% lower risk of stroke mortality in patients with or without hypertension. 69 On the other hand, heavy alcohol intake (>30 g/day) was associated with a 20% increased risk of total stroke, while moderate alcohol intake had no effect on the risks of stroke or stroke mortality in this same study. 69
In summary, evidence on alcohol intake in hypertension and T2D is still controversial, although it appears that moderate alcohol intake may have no detrimental effect or even a protective effect on patients with hypertension or T2D. In that way, current recommendations, such as the 2020 International Society of Hypertension guideline advise limiting alcohol consumption to 2 drinks/day (20 g of alcohol) for men and 1.5 drinks/day (15 g of alcohol) for women. 70
Physical Activity
Current recommendations from the Brazilian Society of Cardiology and the International Society of Hypertension guidelines advise that all adults with or without hypertension should practice at least 150 min per week of moderate physical activity or 75 min/week of vigorous activity.70,71 This is also supported by the American Diabetes Association recommendations for T2D patients. 47 A previous meta-analysis of 93 randomized controlled trials (RCTs) has shown that different modalities of exercise training, including endurance, dynamic resistance, and isometric resistance, are effective in reducing both systolic blood pressure (SBP) and diastolic blood pressure (DBP). 72 In particular, for patients with both hypertension and type 2 diabetes, a meta-analysis of 8 RCTs found that exercise interventions were associated with reductions in systolic BP of 5.25 mmHg, diastolic BP of 3.16 mmHg, body mass index of 1.47 kg/m2, and waist circumference of 2.91 cm. 73
An umbrella systematic review by Pescatello et al. that included 17 meta-analyses and one systematic review on the relationship between physical activity and blood pressure, with a total of 594 129 subjects, provided further insight into the effectiveness of physical activity on hypertension. 74 First, this umbrella review found that low- to vigorous-intensity physical activity in hypertensive adults was effective to reduce systolic and diastolic BP (5-17 mmHg for systolic BP and 2-10 mmHg for diastolic BP) compared with hypertensive adults that were physically inactive at baseline. Beyond that, this review showed that physical activity was associated with a significantly lower risk of CVD mortality, in a dose–response relationship, in subjects with hypertension. 74 Furthermore, the authors concluded that there was not enough evidence available to assess if variations in physical activity frequency, intensity, time or duration had a different effect on BP or CVD mortality in hypertensive patients. 74 Finally, this umbrella systematic review found that the effectiveness of different modalities of physical activity (aerobic, dynamic resistance or combined) on BP was similar among hypertensive subjects. 74
Behavioral and Environmental Interventions
Stress Management
Mindfulness-based stress reduction programs may also play a role in reducing BP.70,75 A systematic review of five trials showed that mindfulness significantly reduced systolic BP by 6.64 mmHg and diastolic BP by 2.47 mmHg in office settings but not in out-of-office settings. 75 Furthermore, Nagele et al. conducted a meta-analysis that included 17 RCTs that investigated the effectiveness of several stress reduction techniques (relaxation, hypnosis, biofeedback, combinations of interventions) in patients with HTN and concluded that stress reduction techniques appear to be effective in reducing diastolic BP and systolic BP, although the heterogeneity among the included studies was high. 76
Smoking
It is widely known that smoking increases the risk for many conditions such as cardiovascular diseases. 77 However, although its association with CVD risk is clear and the benefits of smoking cessation are well established, evidence on the association between smoking and BP is controversial. 78 Findings from a mendelian randomization meta-analysis showed that although there is indeed a causal association of smoking heaviness with higher levels of resting heart rate, they found no significant association between smoking heaviness and BP levels. 79
Pollution
Air and noise pollution have been a topic of interest in recent cardiovascular medicine research, with a growing body of evidence establishing a strong link between pollution and CVD risk. For instance, a previous meta-analysis showed that particulate and gaseous pollutants can increase systolic and diastolic BP and also increase the risk of hypertension. 80 Also, even indoor air pollution from solid fuels can increase the risk for hypertension. 81 Exposure to noise in a work or home environment has also been associated with 62% higher odds of hypertension. 82 A previous meta-analysis by Rabiei et al. that included 139 studies on the interaction between occupational or environmental noise and cardiovascular disease also showed that noise exposure can significantly increase the risk for CVD and the odds for hypertension. 83 However, there is no RCT to this date assessing whether interventions aiming to reduce ambient and noise pollution exposure would improve BP and glycemic control.
Sleep
Impact and Overall Recommendations for Different Lifestyle Interventions for Hypertension and Type 2 Diabetes.
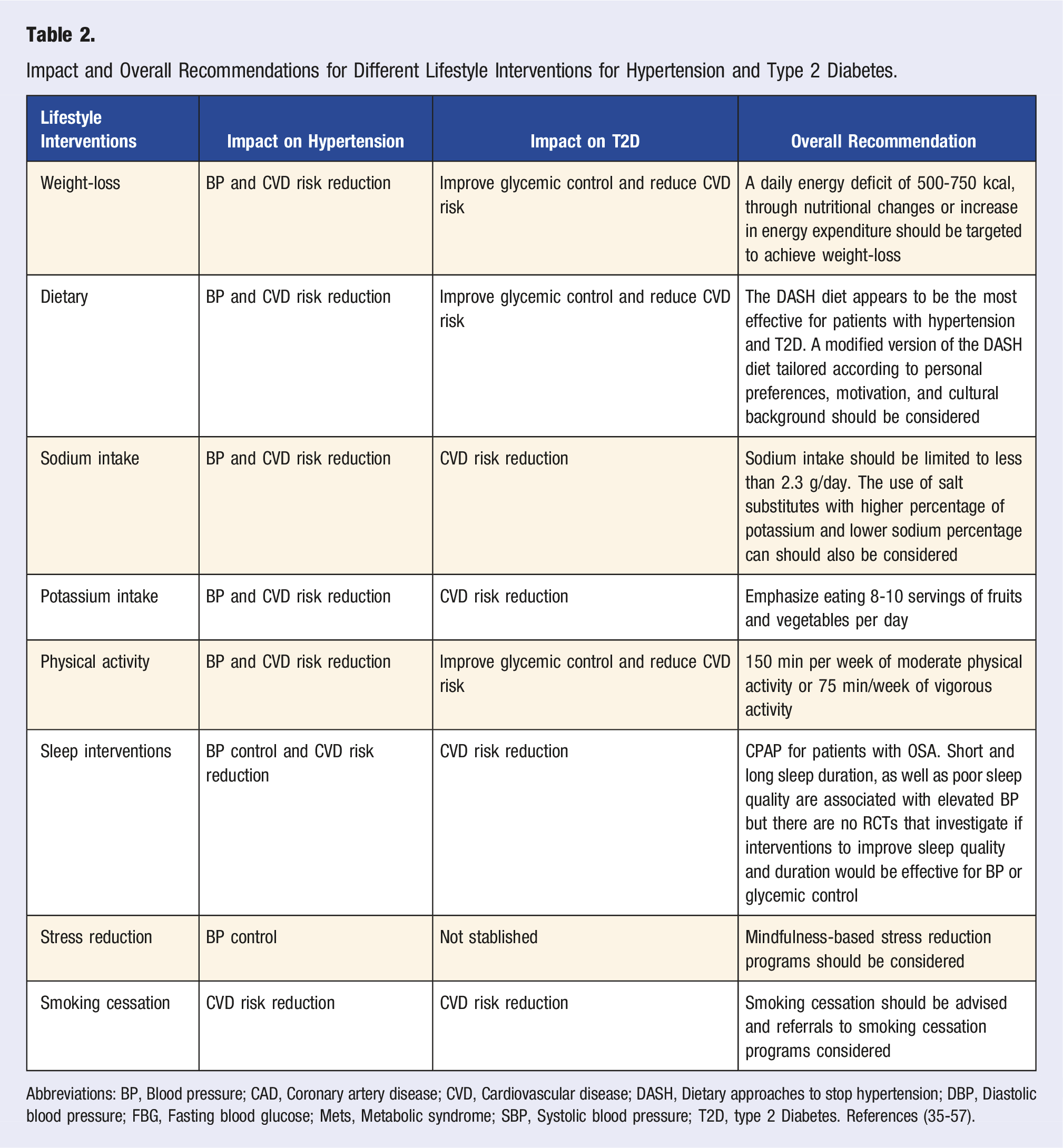
Abbreviations: BP, Blood pressure; CAD, Coronary artery disease; CVD, Cardiovascular disease; DASH, Dietary approaches to stop hypertension; DBP, Diastolic blood pressure; FBG, Fasting blood glucose; Mets, Metabolic syndrome; SBP, Systolic blood pressure; T2D, type 2 Diabetes. References (35-57).
Tailoring Lifestyle Interventions to Brazilian Patients
Public healthcare expenditure in Brazil is still low compared to other countries in the Organization for Economic Cooperation and Development (OECD). In 2019, public healthcare expenditure accounted for only 10.5% of the total Brazilian GDP, compared with an average of 15.3% of GDP expenditure from OECD countries. 87 Additionally, the GDP per capita in Brazil was 15 424 USD per year in 2019, which is significantly lower than the average of 46 668 USD per year for OECD countries, 88 resulting in an even lower healthcare expenditure per capita. Furthermore, unlike other OECD countries, in Brazil, approximately 90% of total pharmaceutical spending comes from out-of-pocket payments, 87 which creates barriers to accessing prescription drugs, thus causing a negative impact on hypertension and glycemic control. Although lifestyle interventions are generally considered to be cost-effective and are a pillar of hypertension and T2D management, adherence to these interventions can be a major challenge. First of all, Brazil is a culturally diverse country, with a mix of indigenous, African, and European influences. Therefore, it is important to consider cultural factors when tailoring lifestyle interventions for Brazilian patients. This can include adapting certain evidence-based dietary modalities, such as the DASH diet, to incorporate traditional Brazilian food. Tailoring the practice of physical activities according to the Brazilian culture and the individual’s preference may also be effective to ensure the long-term sustainability of these interventions. Furthermore, although a middle-income country, Brazil has a high level of mobile phone and internet penetration, which may be useful for delivering and monitoring lifestyle interventions. This can include using mobile apps to track adherence to diet and physical activity, sending reminders and motivational messages, and using telemedicine to provide remote support for patients. Notably, a previous review found across several systematic reviews and meta-analyses moderate to high strength of evidence to conclude that telemedicine interventions are effective to improve BP control and reduce BP in hypertensive patients. 89 Also, specifically in patients with both hypertension and T2D, previous RCTs showed that the use of telemonitoring in addition to nurse or clinician management was associated with greater reductions in BP, HbA1c, LDL cholesterol, and a greater proportion of BP control compared with usual care.90-94 A scoping review focusing on telemedicine interventions for hypertension in low and middle-income countries also found that telemedicine interventions promoted a significant reduction in BP, although there is a need for well-designed RCTs with a larger sample to strengthen the quality of evidence supporting this effect. 95 Other digital interventions, such as smartphone applications, have also been shown to aid hypertension control. For example, the HERB system is a smartphone app that encourages users to adopt lifestyle interventions to increase BP reduction. 96 To achieve its purpose, this app uses evidence-based interventions such as salt restriction, weight control, exercise, and alcohol restriction, as well as behavioral interventions. 96 Moreover, the app can personalize recommendations and strategies personality, according to the users’ personality, behavioral characteristics, and hypertension determinants, 96 which can be useful to tailor lifestyle interventions to different cultures. To illustrate its effectiveness, a RCT by Kario et al. showed that the HERB system plus standard lifestyle modification led to a significantly greater reduction in systolic BP compared with standard lifestyle modification alone (4.9 mmHg vs 2.5 mmHg reduction in systolic BP, respectively). 96
Brazil has a relatively well-structured primary healthcare system that covers 65% of the total Brazilian population, 97 although there is still a margin to increase coverage. In that way, primary care-based interventions could also be particularly effective to improve adherence to lifestyle interventions. This was shown in a previous RCT that yielded relevant data on the effectiveness of a high-intensity, lifestyle-based weight-loss program for obesity delivered in a primary care setting of low-income populations. 98 In this study, the intensive-lifestyle intervention consisted of reduced caloric intake and increased physical activity and was delivered through a program of weekly sessions delivered by health coaches for the first 6 months and monthly sessions for the remaining 18 months. 98 In conclusion, this study found that the high-intensity lifestyle intervention led to a significantly greater weight-loss at 24 months compared to standard care alone (4.99% loss of body weight and .48% loss of body weight, respectively). 98 Although this strategy was not validated for patients with hypertension and T2D, this model could serve as a framework to design future strategies to be used and tested by the Brazilian Primary Care system to improve adherence to lifestyle interventions, promote weight-loss, hypertension and T2D control. Furthermore, future studies are needed to validate strategies to improve the sustainability of dietary, exercise and behavioral interventions for Brazilian patients with hypertension and T2D. Cost-effectiveness analyses using Brazilian data would also be valuable to raise awareness among government and private organizations about the importance to increase adoption and adherence to evidence-based lifestyle interventions for patients with hypertension and T2D.
Conclusion
Hypertension and T2D are associated with a higher risk of mortality, hospitalization, impaired quality of life and cause a major economic burden on the Brazilian Healthcare System; yet, BP and glycemic control are still major challenges in Brazil. Current evidence supports the effectiveness of different dietary, exercise and behavioral lifestyle interventions for hypertension and T2D. Among dietary interventions, the DASH diet appears to be the most effective to increase BP reduction and reduce the risk of CVD mortality, with a moderate effect on glycemic control. A weekly routine of physical activity should be encouraged, with similar current evidence indicating similar effectiveness of aerobic, resistance or combined exercise training programs. Stress-based reduction programs also seem to aid BP reduction and should be encouraged. Finally, further studies are certainly needed to explore the overall effectiveness and cost-effectiveness of these different lifestyle interventions in the Brazilian population. The design of evidence-based public health policies focusing on the implementation and feasibility of lifestyle interventions will also be needed to ensure long-term adherence to lifestyle changes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.