
Abstract
Less than a quarter of the 116 million adults with hypertension in the United States have blood pressure (BP) lower than the guideline-recommended goal of 130/80 mmHg. There is a critical need for novel interventions that integrate evidence-based recommendations—such as lifestyle medicine and home BP monitoring (HBPM)—into clinical care. In this study, we tested the hypothesis that a four-part, primary care physician-led Virtual Group Visit (VGV) series combining lifestyle medicine, Health and Wellness Coaching (HWC), and HBPM could lead to a reduction in BP and antihypertensive medications. There was a decrease in systolic (β = −.108 mmHg per day; P = .046) and diastolic (β = −.058 mmHg per day; P = .026) BP. Thirteen of the 22 patients (59%) who started the VGV series on medications had at least one medication dosage reduced or discontinued during the VGV series, and 8 of the 18 patients (44%) who finished the VGV series on medications had at least one medication dosage reduced or discontinued in the 180 days after the VGV series. This pilot study demonstrates for the first time that lifestyle medicine VGVs, coupled with HWC and HBPM, are associated with improved BP control and medication deprescribing.
Keywords
Introduction
Less than a quarter of the 116 million adults with hypertension in the United States have blood pressure (BP) lower than the guideline-recommended goal of 130/80 mmHg. 1 Numerous factors may contribute to inadequate hypertension control, ranging from individual-level medication adherence patterns to national policy. 1 There is a critical need for novel interventions that integrate underutilized, evidence-based recommendations—such as lifestyle medicine and home BP monitoring (HBPM)—into clinical care.2,3 Lifestyle medicine promotes exercise and nutrition counseling to prevent and treat hypertension, and it is recommended for all patients in the United States with hypertension, including over 50 million adults who meet guideline recommendations for lifestyle modification alone.2,4 However, the majority of patients with hypertension do not receive appropriate lifestyle counseling as part of their clinical care. 4 Another underutilized component to hypertension care is HBPM, which generates data that effectively support the diagnosis of white coat and masked hypertension as well as the titration of antihypertensive medication dosages.2,5 Over 100 million adults in the United State meet criteria for HBPM according to recent guidelines, although many barriers limit the widespread use of HBPM.2,6 Gaps in guideline-concordant care have likely contributed to the development of a population of patients with hypertension who could 1) lower BP with lifestyle medicine and/or 2) achieve optimal medication regimens with HBPM.
Group medical visits, also known as shared medical appointments, are a care delivery tool that can support lifestyle medicine and HBPM. In group medical visits, multiple patients with the same condition, such as hypertension, meet with a provider in a group setting for at least an hour at a time. Importantly, individual care can also be provided in the context of a group, allowing for reimbursement of these medical visits. Group medical visits have already been studied extensively as a care delivery strategy for improving hypertension control.7-9 Group medical visits focused on lifestyle medicine education can also integrate Health and Wellness Coaching (HWC), a growing discipline that promotes healthy lifestyle changes through evidence-based coaching practices. 10
Since the onset of the COVID-19 pandemic, Virtual Group Visits (VGVs) have garnered increasing attention. 11 VGVs mitigate some common barriers to in-person group medical visits, such as the time and cost of transportation to brick-and-mortar facilities, while maintaining many benefits of group-based medical care. 12 There is little known about the effectiveness of VGV-based programs for hypertension management.
Methods
In this study, we tested the hypothesis that a primary care physician-led, four-part VGV series integrating hypertension management education, lifestyle medicine, HWC, and HBPM could lead to a reduction in BP and optimization of medication regimens. From June 2020 to October 2021, English-speaking adult patients with hypertension participated in the VGV series as part of standard care in the Massachusetts General Hospital (MGH) Division of General Internal Medicine Healthy Lifestyle Program (HLP) at the MGH Revere Healthcare Center. Revere, Massachusetts is a city located approximately 5 miles north of Boston and is comprised of a racially, ethnically, and socioeconomically diverse community with a large immigrant population.
Patients attended four 60-minute VGVs every two weeks in cohorts that typically consisted of 3–6 patients. All patients were provided complimentary BP cuffs connected to the electronic medical record and were educated on BP monitoring techniques prior to the first VGV (Figure 1). During the VGV series, patients learned about hypertension management (e.g., the health consequences of hypertension, the health benefits of hypertension control, etc.) as well as the influence of nutrition, sodium, exercise, weight loss, and stress on BP control. The physician group leader utilized a PowerPoint presentation created by clinician members of the HLP, which included patient-facing infographics from organizations such as the American Heart Association, Centers for Disease Control and Prevention, and American College of Lifestyle Medicine.13-15 Schematic of Virtual Group Visit series timeline. Abbreviations: HBPM = home blood pressure monitoring; VGV = Virtual Group Visit.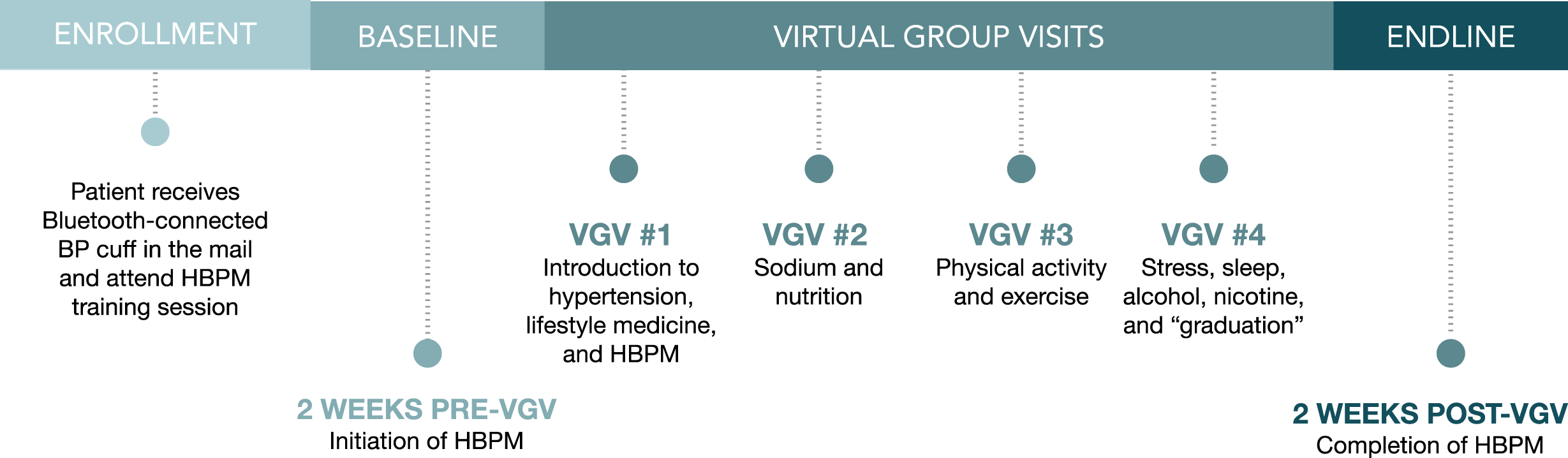
During each VGV, patients were encouraged to create behavior change goals, also known as “SMART goals,” and progress on prior goals was discussed in the group setting. 16 Patients were also offered complementary access to one-on-one HWC, in addition to virtual exercise classes, during and after the VGV series. Records of participation with HWC and virtual exercises classes were not available for analysis in the present study. Patients were invited to additional lifestyle medicine VGVs in the HLP after completion of the hypertension VGV series.
Patients also received an individual review of HBPM data at each VGV. The physician group leader used the electronic medical record to calculate the average BP over the 2 weeks prior to each VGV, and these averages were shared with each patient during the VGV in a group setting. When home BP measurement averages were either below or above the target of 130/80 mmHg, patients were offered the ability to reduce or increase antihypertensive medication dosages, respectively, with continued monitoring of HBPM data after titration.
Inclusion in analysis was based on attendance of all four VGVs in the series in addition to 10 or more HBPM measurements during the study period, defined as two weeks prior to the first VGV through two weeks after the fourth VGV. To assess BP changes during the VGV series, the mean BP in the two weeks prior to the first VGV and two weeks after the fourth VGV were calculated. In addition, linear regression models, estimated via generalized estimating equations with exchangeable working correlation structure, were used to assess changes in BP over the study period. To assess the long-term impact of the VGV series, subsequent non-urgent primary care office visits were interrogated for clinic-based BP readings (within 180–360 days after the last VGV); however, only nine patients had such visits. As a result, long-term BP analysis was not included in the present study. Antihypertensive medication prescriptions were evaluated at the beginning and end of the VGV series as well as 180 days following the last VGV. This project was undertaken as a Quality Improvement Initiative at MGH, and, as such, Institutional Review Board approval was not required.
Results
There were 38 patients who enrolled in a VGV series during the study period, and 23 patients (61%) met inclusion criteria. Of the 15 excluded patients (39%), six were for low attendance and nine were for insufficient HBPM data. Included patients had a median age of 67 (IQR, 56–70), 19 patients (83%) were White, and 17 patients (74%) were female; excluded patients had a median age of 65 (IQR, 59–70), 12 patients (80%) were White, and five patients (33%) were female. For included patients, the median number of BP data points per patient was 65 (IQR, 54–153; Figure 2). During the VGVs, patients regularly set behavior change goals such as, “I will buy low sodium ingredients when food shopping,” “I will walk twice daily for 30 minutes at a time,” and, “I will reduce caffeine intake to two cups of coffee daily.” Home blood pressure measurements of a representative Virtual Group Visit participant (groups on days 14, 28, 42, and 57) with locally estimated scatterplot smoothing curve overlayed. Abbreviations: BP = blood pressure; VGV = Virtual Group Visit.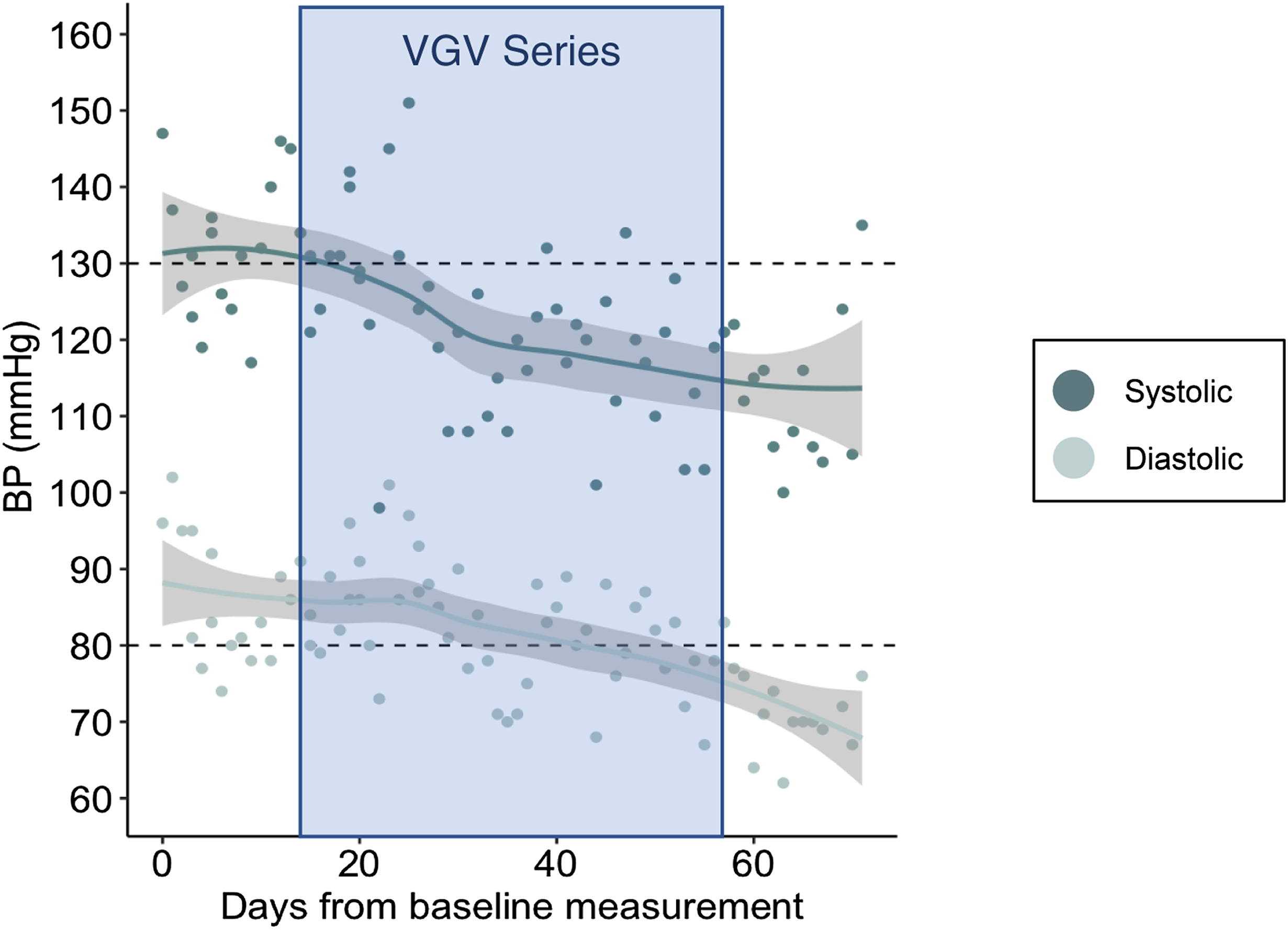
At baseline, the median BP was 128/78 mmHg (Figure 3A) and 10 patients (43%) were below the goal BP of 130/80 mmHg (Figure 3B). At the end of the VGVs, the median BP was 125/74 mmHg (Figure 3A) and 14 patients (61%) were below the goal BP of 130/80 mmHg (Figure 3B). There was a decrease in systolic (β=−.108 mmHg per day; P = .046 (95% CI −.214, −.002)) and diastolic (β=-.058 mmHg per day; P = .026 (95% CI −.109, −.007)) BP, with a 50-day estimated BP reduction of −5.4/−2.9 mmHg from baseline. A) Systolic and diastolic blood pressure pre- and post-Virtual Group Visit series (width of violin plot corresponds to probability density). B) Percent of patients at goal blood pressure, defined as a mean of systolic blood pressure <130 and diastolic blood pressure <80 (n = 10 pre-Virtual Group Visit series and n = 14 post-Virtual Group Visit series). Abbreviations: BP = blood pressure; VGVs = Virtual Group Visits.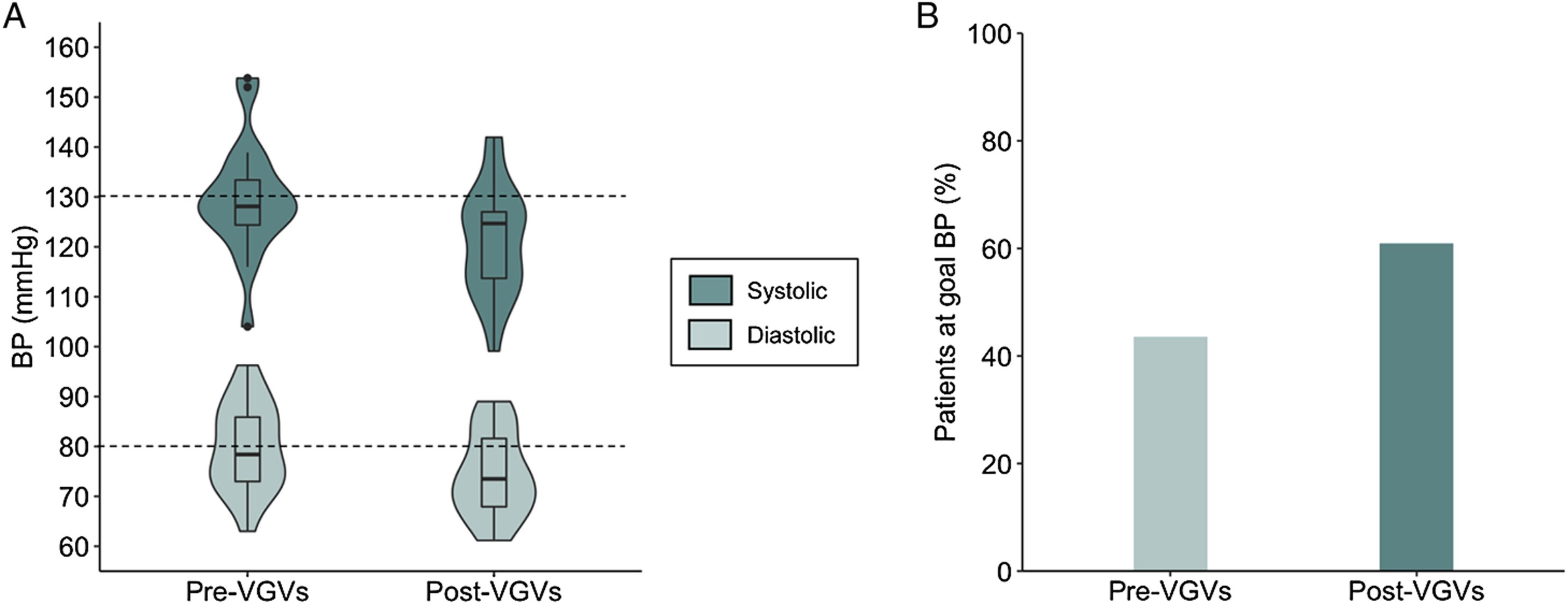
Among the 23 included patients, one (4%) began the VGV series without taking antihypertensive medications, and that patient did not start a medication during the VGV series. For the 22 patients who began the study on antihypertensive medications, the dosage was reduced or the medication was discontinued for 13 patients (59%), medication dosages remained the same for seven patients (32%), and medication dosages were increased or a new medication was added for three patients (14%; Figure 4). At least one medication was discontinued during the VGV series on 10 patients (45%), and four patients (18%) were taken off antihypertensive medications completely. Antihypertensive medication changes. “During VGVs” = patients on medications at the start of the Virtual Group Visit series (n = 22). “After VGVs” = patients on medications at the end of the Virtual Group Visit series (n = 18). “Reduced” = medication dosage reduction or discontinuation. “Increased” = medication dosage increase or addition of new medication. Abbreviation: VGVs = Virtual Group Visits.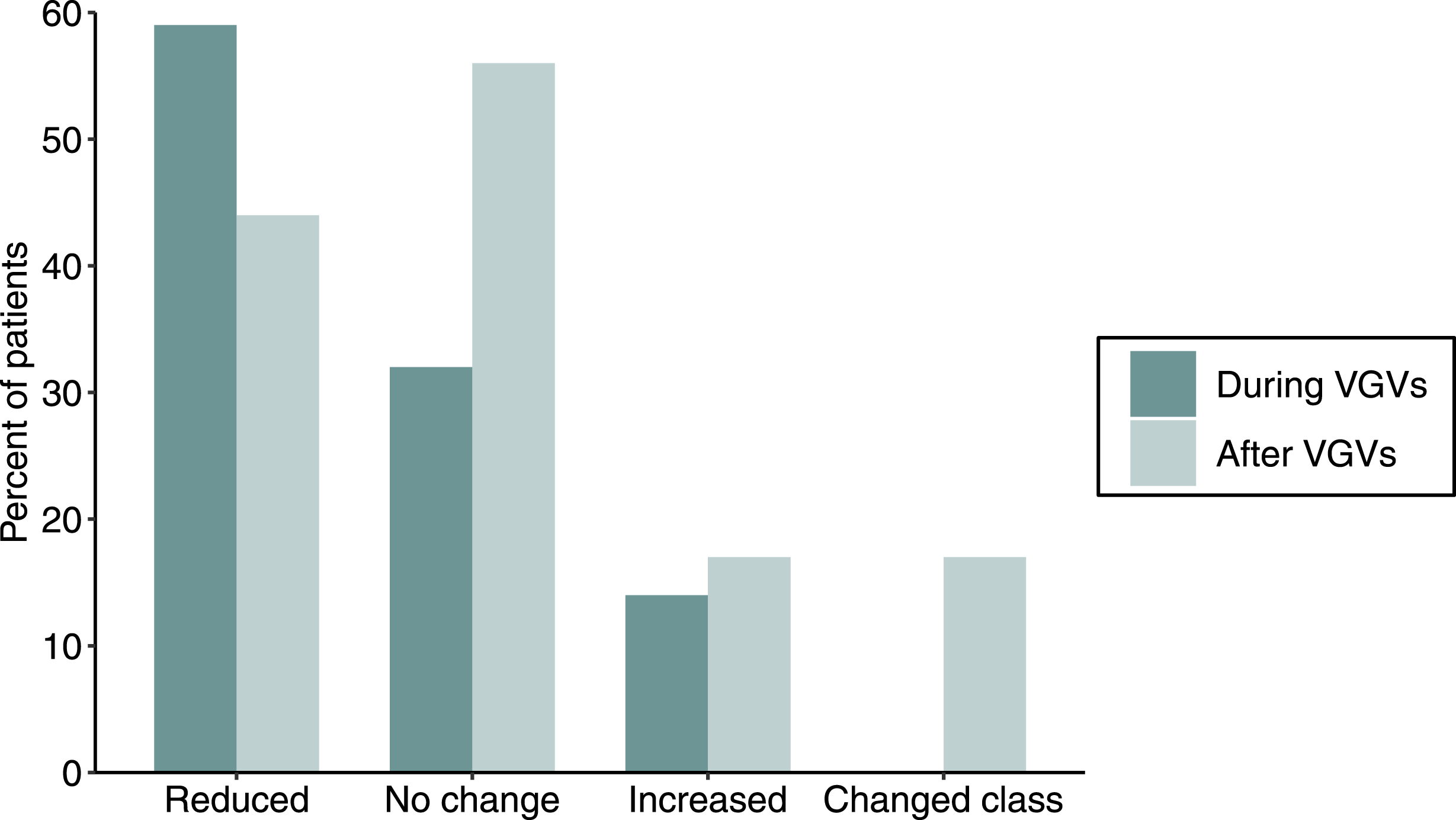
In the 180 days following the VGV series, none of the five patients who ended the VGV series off antihypertensive medications were started on a new medication. For the 18 patients on antihypertensive medications at the end of the VGV series, the dosage was reduced or the medication was altogether discontinued for eight patients (44%), medication dosages remained the same for 10 patients (56%), medication dosages was increased or a new medication was added for three patients (17%), and medications were changed to a different class for three patients (17%; Figure 4). One patient had a combination of multiple medication changes (i.e., one medication was discontinued and another medication was changed to a medication in a different class). The three patients who had medications increased after the VGV series all returned to their initial medication regimen at the beginning of the VGV series. At least one medication was discontinued after the VGV series on five patients (28%), and one patient (6%) was taken off antihypertensive medications completely, resulting in a total of six patients not taking antihypertensive medications by the end of the study.
Conclusions
This pilot study demonstrates that lifestyle medicine VGVs, coupled with HWC and HBPM, are associated with improved BP control. Previous studies have similarly demonstrated improvements in BP control for in-person group visits, although prior study designs included larger, multi-disciplinary teams and/or group visits that lasted up to 2.5 hours.7-9 To our knowledge, this is the first hypertension group visit study assessing 1) virtual group care delivery and 2) HBPM integration.
The estimated BP reduction over 50 days of −5.4/−2.9 mmHg from baseline is comparable to that seen in various lifestyle interventions in patients with hypertension, including salt restriction (2–3 mmHg reduction), weight loss (1 mmHg reduction per kilogram of weight loss), exercise (5–8 mmHg reduction), and alcohol restriction (5-6 mmHg reduction). 2 Although an average BP reduction of −5.4/−2.9 mmHg could be clinically insignificant in patients with very high blood pressure, the 40% increase in patients at goal BP over the course of the VGV series represents a clinically meaningful improvement in hypertension management.
The observed BP reductions also enabled medication deprescribing during the VGV series in 59% of the patients who began the study on antihypertensive medications. Moreover, additional deprescribing took place in 44% of the patients in the 180 days following the VGV series, likely in response to continued healthy lifestyle changes that were galvanized by the VGVs and/or HWC. There was only one patient without antihypertensive medications at the beginning of the VGV series, five patients without medications at the end of the VGV series, and six patients without medications 180 days after the end of the VGV series. Most prior in-person hypertension group visit studies have not directly assessed medication changes.7,8 One recent study, however, utilized pharmacist-driven protocols and demonstrated the utility of group-based medication titrations. 9 Similarly, the medication changes in this study highlight the clinically meaningful impact of combining lifestyle medicine, HWC, and HBPM in VGV-based programming.
The main limitation of this study is the lack of a control group. Other limitations include the small sample size; the inclusion of a mostly older, female, and White patient population who were highly adherent to VGV participation and regular HBPM; and the lack of HBPM or clinic-based BP data beyond two weeks after the VGV series. It is also unclear which of the various intervention components (i.e., VGVs, HBPM, HWC, and/or virtual exercise classes) contributed the most to the observed improvements in hypertension control. The influence of these free offerings is not addressed in this study because participation in HWC and virtual exercise classes was not recorded.
To support scaling this intervention, future randomized controlled trials are needed with longer interventions, accounting for participation with HWC as well as virtual exercise classes, and inclusion of larger and more diverse patient populations. Future studies need to also assess the barriers and facilitators of participation in VGVs in primary care clinics, especially for patient populations with low socioeconomic status and/or low English proficiency. For example, it is not known how this virtual intervention affects patients with hypertension who have limited access to the technology and/or high-speed internet needed for video telemedicine care. Although the current study took place in a clinic that serves a diverse patient population, the patients who attended VGVs were older and more likely to be White and female than those who did not attend. Moreover, it is unclear why several patients did not attend all four sessions or did not contribute a meaningful amount of HBPM data.
In summary, this study adds to the evidence base supporting the guideline-driven use of both lifestyle medicine and HBPM for improved hypertension control. 2 The combination of lifestyle medicine VGVs, HWC, virtual exercise classes, and HBPM may be a feasible and effective strategy for providing guideline-concordant hypertension management in primary care. This study provides credibility to the notion that VGVs are a valuable tool to grow clinical interventions that treat chronic disease through lifestyle medicine.11,12,17 Potential benefits of scaling this VGV program could include the integration of evidence-based lifestyle medicine and HBPM practices into clinical care, enhanced patient engagement with primary care services, reductions in medication costs and side effects, and improvements in population-level hypertension control.
Footnotes
Authors’ Note
Jacob B. Mirsky and Tiffany X. V. Bui contributed equally to this work.
Acknowledgements
The authors would like to acknowledge Anna Baggett; Barbara Canada, MBA; Nydia Febres; Daniel Horn, MD; Josh Metlay, MD, PhD; and Amy Wheeler, MD for their contributions to the clinical program described above.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.