
Abstract
Among Americans aged 65 years and older, falls are the leading cause of injury death and disability, and finding effective methods to prevent older adult falls has become a public health priority. While research has identified effective interventions delivered in community and clinical settings, persuading older adults to adopt these interventions has been challenging. Older adults often do not acknowledge or recognize their fall risk. Many see falls as an inevitable consequence of aging. Health care providers can play an important role by identifying older adults who are likely to fall and providing clinical interventions to help reduce fall risks. Many older people respect the information and advice they receive from their providers. Health care practitioners can encourage patients to adopt effective fall prevention strategies by helping them understand and acknowledge their fall risk while emphasizing the positive benefits of fall prevention such as remaining independent. To help clinicians integrate fall prevention into their practice, the Centers for Disease Control and Prevention launched the STEADI (Stopping Elderly Accidents, Deaths, and Injuries) initiative. It provides health care providers in primary care settings with resources to help them screen older adult patients, assess their fall risk, and provide effective interventions.
Among Americans aged 65 years and older, falls are the leading cause of injury death and disability. 1 In 2014, unintentional falls were responsible for 27 000 deaths and 2.8 million emergency department (ED) visits. 1 Each year more than 812 000 older adults are hospitalized for serious fall injuries, most often for hip fractures and head injuries. 2 In addition to their detrimental effect on older adults’ health and quality of life, falls are one of the 20 costliest medical conditions. 3 In 2014, the direct medical costs of falls, adjusted for inflation, totaled $31.3 billion. 4 However, this underestimates the total economic burden of falls because it does not include direct nonmedical, intangible, and indirect costs.
Fall Prevention Strategies
Finding effective methods to prevent older adult falls has become a public health priority. Extensive research on falls over the past 3 decades focused initially on identifying fall risk factors and subsequently on designing and testing falls interventions. At least 22 interventions, tested in randomized controlled trials (RCTs), have demonstrated that reducing or treating modifiable risk factors can reduce the risk of falls by up to two-thirds. 5 These evidence-based fall prevention interventions can be broadly categorized as single interventions that focus on a specific fall risk factor (eg, muscle weakness, poor balance, psychoactive medications, and home hazards) and multifaceted interventions that address a number of modifiable risk factors. Such interventions can be implemented in either clinical or community settings.
The most effective community-based intervention strategy is exercise to improve leg strength and balance, an approach that can reduce fall risk by an average 24%. 6 Various exercise interventions, including tai chi,7,8 group exercise classes,9,10 and home-based exercise programs,11,12 have been shown in RCTs to reduce falls among older adults living in the community. A number of community-based interventions that use occupational therapists to promote behavioral changes and reduce home hazards also have been shown to reduce falls.13-16
Effective clinical interventions can address either single or multiple risk factors. Examples of single interventions include withdrawing psychoactive medications, 17 supplementing vitamin D,18-20 and addressing foot and ankle problems. 21 Multifactorial clinical interventions are tailored to each individual patient and address his or her specific fall risk factors. Such interventions include reviewing and modifying medications, providing a referral to physical therapy or an exercise program that includes balance and strength training, treating postural hypotension, and addressing chronic conditions that can increase fall risk, such as arthritis, 22 coronary heart disease, 23 diabetes, 24 and Parkinson’s disease. 25
Attitudes and Beliefs
Although RCTs have identified effective fall prevention interventions, 5 persuading older adults to adopt these interventions has been challenging. Enrollment in exercise interventions averages less than 50% 26 and can be as low as 10%. 27 Older adults’ attitudes and beliefs about falls play a large role in limiting their acceptance and adoption of fall prevention strategies.
Beliefs about falls are important predisposing factors for rejecting fall prevention strategies. Many older adults believe that falls “just happen,” are a normal consequence of aging28,29 or are simply due todue to bad luck. 30 Older adults often do not acknowledge or recognize their fall risk. 31 Falls frequently are viewed as signs of physical decline and are considered relevant only for frail or very old persons. 32 Braun 33 reported that older adults felt that environmental factors, such as uneven pavement, were most likely to cause falls. In general, older adults are more likely to attribute falls to extrinsic, or external, factors (such as the home environment or daily activities) than to biological factors such as dizziness or muscle weakness.33,34
Although falls are common among people who have and have not fallen previously, many older adults do not recognize that they are at risk or believe that only others are at risk. 32 Some older adults who fell did not consider themselves to be fallers because they attributed their fall to a temporary condition or illness. One study found that perceptions of low personal risk were associated with being male, being younger than 80 years, having a partner, being privately insured, rating one’s general health positively, and not having experienced a fall or fall injury. 35 Another study reported that some older adults with visual impairments felt that, while they were not at risk, rushing and not being careful were reasons why other older people would fall. 36
Laing et al 37 surveyed 158 people aged 65 years and older who had either fallen in the past year, restricted their activities because of fear of falling, or reported feeling unsteady. Although almost half the participants had experienced a recent fall, one-third reported that falls were their least important health concern compared with other (unspecified) health and safety issues.
Some older adults believed there is a difference between “just falling” and falling while being engaged in an activity. 38 Older men in particular saw themselves as responsible and capable of dealing with their risk of falling when they chose to do something potentially hazardous such as climbing on a ladder. 34 In a qualitative study of 11 older women who had fallen in the past 12 months, 4 reported they did not seek medical help because they believed their fall was not serious enough and/or did not want to waste their doctor’s time. 39
Beliefs about the causes of falls are influenced by both gender and cultural expectations. Horton 34 reported that women were more likely than men to attribute falling to hurrying and not paying attention. These types of explanations were used frequently by older South Asians 40 and Chinese. 41 Focus groups and in-depth interviews of 30 Chinese older people revealed that these older adults were fatalistic, avoided talking about falls, and hid their falls from their adult children to avoid worrying them. 41 A focus group study of 15 Chinese older adults in Australia found that fear of falling was very common. 42 Some were concerned that they might become a burden to their children. Views were mixed about whether or not falls were preventable. Their main fall prevention strategy was to “take care and not rush.”
Fall Prevention Behaviors
Although there are evidence-based falls interventions, 5 fall prevention for many older adults consists simply of “being careful” 40 and holding on to things when moving about the house. 38 People who are afraid of falling tend to limit their activities in an effort to reduce falls, leading to a loss of muscle strength and increased fall risk. 28
Simpson et al 43 interviewed 32 older people who were concerned about falling to determine what they did or were willing to do to avoid falling. Participants reported that their strategy was to “take care” (eg, avoid activities seen as dangerous, hold on to supports, move slowly, and know their limitations). None mentioned exercise or physical activity and only one mentioned improving home safety. Most participants were not aware of the benefits of exercise in general or for improving balance and muscle strength.
Jansen et al 44 reported on an observational study of 936 community-dwelling older participants within the intervention arm of an RCT designed to prevent functional decline. Falling was identified as a condition for 380 (41%). However, only 62 (16%) participants acknowledged their fall risk and only 37 (10%) considered fall prevention a priority.
Yardley et al 32 conducted focus groups with a total of 66 people aged 61 to 94 years. For most, fall prevention meant reducing home hazards, using mobility aids, and restricting activity. Most participants were not aware that exercise to improve strength and balance could reduce falls. They had mixed responses to information about fall prevention. Many felt the advice was useful but only for other people and did not consider the information personally relevant.
A telephone survey of 1709 US adults aged 65 years and older found that 1 in 10 reported falling in the past 3 months and half had been injured in their most recent fall. 45 However, few of these respondents changed their behavior in order to prevent future falls. Sixty-five percent did not change their level of physical activity while 21% decreased their physical activity. Most people (97%) did not have their medications changed and 84% did not make any changes to their home environment. 45 Another study found that many people avoided fall prevention activities because it meant acknowledging their personal risk and being seen as weak, vulnerable, and potentially unable to live independently. 46
Strength and balance exercises, including tai chi, have been shown to reduce falls 30% to 55%. 5 However, a study of adults aged 60 to 70 years found that people who did not acknowledge their risk of falling were not motivated to exercise. 40 Many older adults felt that exercise for fall prevention was needed only after physical weakness became noticeable. 40 In the study by Yang et al 42 of 15 Chinese older adults, 12 participants exercised regularly but none knew about the benefits of exercise in preventing falls.
The acceptability of exercise for fall prevention is influenced by cultural values and beliefs. Researchers have reported that many older Latinos believed exercise was inappropriate or useless for older people 47 while many Asians felt old age was a time to rest or relax.40,48 A qualitative study of 38 older African Americans’ attitudes and beliefs about exercise found that participants preferred group exercises to exercising at home, expressed safety concerns about walking for exercise, and did not respond favorably to exercises using weights. 49
About half of all falls happen in and around people’s homes. 50 Fall prevention interventions that used occupational therapists to reduce home hazards and promote behavioral changes have been shown to reduce falls. 5 However, a qualitative study of 10 adults aged 60 years and older found that most were not interested in modifying their home environment to prevent falls. These participants saw falls as events that could not be controlled. 38 In general, study participants did not see falls as a problem, did not believe modifying their homes would prevent falls, and most importantly, did not like others telling them to make changes to their homes. 38 In another study of 60 community-dwelling older adults who had been treated in an ED for a fall, one-third felt their homes were safe enough and dismissed home safety recommendations. 51
Discussing Falls With Health Care Providers
Older adults are often reluctant to discuss falls with their providers, even after experiencing a fall, although a fall-related injury needing medical attention may trigger such a discussion. However, many falls do not cause serious injuries, which enable patients to avoid the issue. For many older adults, discussing falls provokes anxiety, which may be related to the stigma associated with aging in our society. 32 A national survey of Medicare beneficiaries found that, among those who fell, less than half talked to a health care provider about it, although women were significantly more likely than men to do so. 52
Many people fear that admitting to falling will lead to being labeled frail or disabled and may result in losing their independence. A qualitative study involving 65 individual interviews and 17 focus groups (n = 122) found that participants were reluctant to tell health providers they had fallen and many falls were not reported. Some older people believed falls were not a medical problem and therefore a doctor would not be interested, the doctor would be too busy to be bothered about their fall, or, if they had not been injured, that the fall was trivial. 53 However, patients sometimes reported a fall after seeing their doctor for another purpose, such as to renew a prescription. 53
Adopting Fall Prevention Strategies
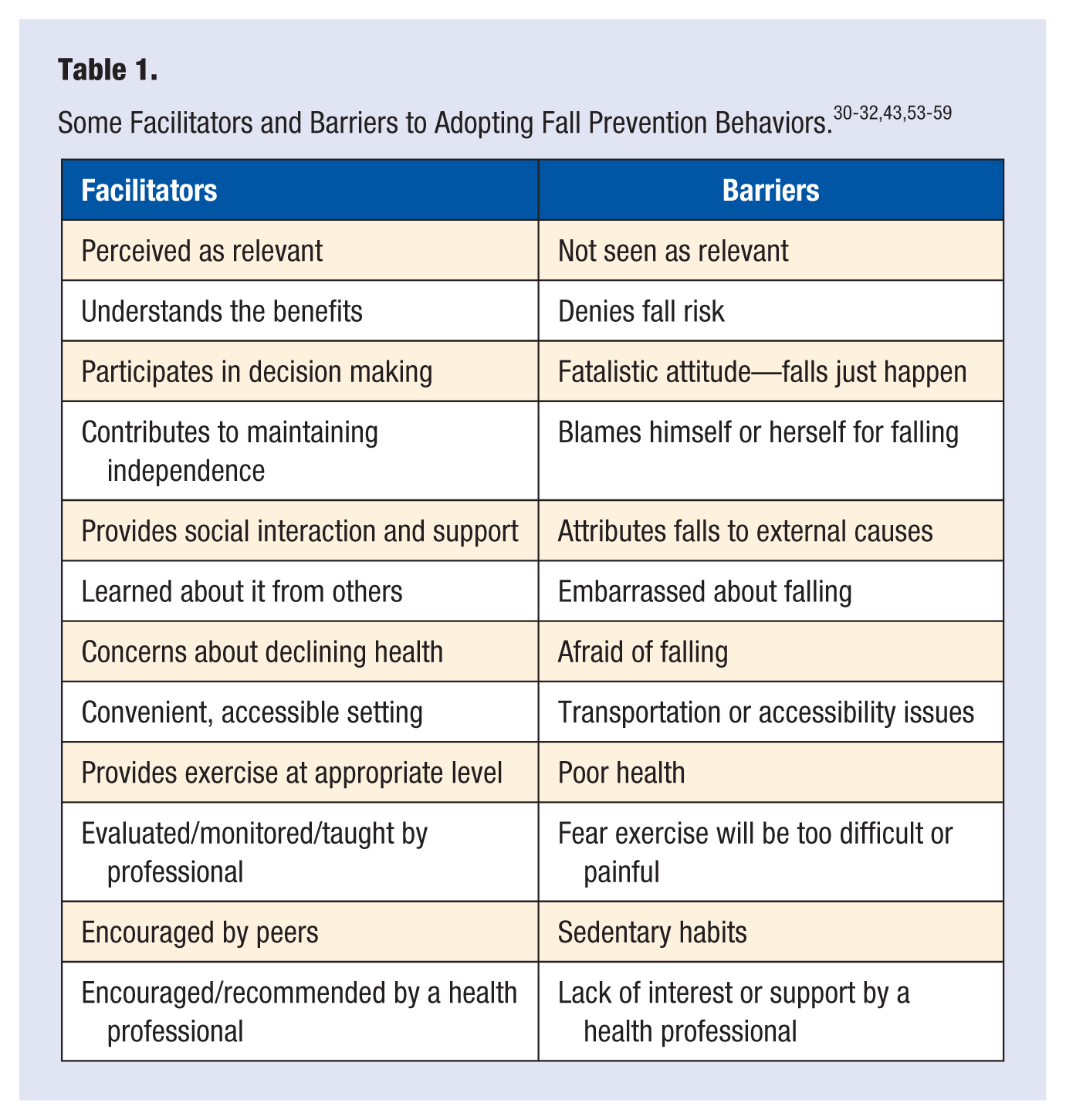
Table 1 lists some of the facilitators and barriers older adults face when making decisions about adopting fall prevention behaviors.30-32,43,53-59
Facilitators
There are multiple factors that support older adults’ acceptance and adoption of fall prevention behaviors. (Table 1) A systematic review by Bunn et al 30 found that participation in and adherence to fall prevention programs was better when participants felt the program was relevant and beneficial. Another key factor was social support that encouraged older adults to participate in fall prevention interventions, both at the individual level (ie, from health care professionals, family and friends) and at the societal level (ie, cultural norms that supported the idea of active aging). 30
Exercise to improve balance and leg strength is an effective fall prevention strategy. 5 However, some older people believe that physical activity is unnecessary or even potentially harmful. 54 Robinson et al 55 conducted a focus group study of 15 older people to better understand their views toward an exercise fall prevention program. The main reason participants gave for attending the program was to maintain their independence, not to reduce their fall risk. Dickinson et al 53 reported that facilitators to participating in an exercise program included hearing about it from others and being encouraged to attend and/or referred by a health care professional. It was important to participants that a program was accessible, that the facility was located in the community, and that the setting was comfortable. In addition, adherence to an exercise program was better if patients received positive reinforcement from their health care providers. 56
Older adults felt encouraged to attend exercise classes if these were well suited to their functional capacities and they did not feel overwhelmed. 53 Factors that motivated older adults with reduced functional abilities included concerns about their declining health, knowledge about how exercise could improve their strength and balance, and a desire to improve their overall health. 57 Group exercise classes were preferred to exercising individually as long as the members of the class had similar abilities.
In 10 semistructured interviews of older adults, De Groot and Fagerström 57 found that participants believed that health professionals knew what type of exercise would be most beneficial for them and where they could find local classes. As a result, they felt that information from health professionals would make them more likely to participate in an exercise group. In a study of 324 older adults’ preferences about various aspects of exercise, factors that participants considered very important included a doctor’s advice to exercise, a demonstration of the exercises by a professional, and an evaluation by a health professional to monitor the physiological effects of exercise. Important characteristics of exercise settings included the quality of the instructor, a convenient location, and the types of exercise. 58
Barriers
The greatest barriers to engaging in fall prevention were a fatalistic attitude, (eg, believing that falls just happen), and not feeling personally at risk. People with these views did not expect to benefit from falls interventions and were unlikely to take up activities or change their behavior to prevent future falls. Bunn et al 30 reported that many older adults believed that falls were due to external factors, chance, or bad luck and, as such, were not preventable. Many people attributed falls to environmental causes, such as uneven sidewalks, or to the inevitable and uncontrollable physical decline that came with aging. Others blamed themselves for falling because they were “rushing” or “not being careful.”60,61 Older adults who had not experienced a fall often did not acknowledge that they might be at risk and were unlikely to undertake activities—such as exercise or home modifications—to prevent falls.32,42,59 Others, who saw themselves as fit, healthy, and competent, felt that fall prevention exercises were not personally relevant. 31
In addition to believing falls were inevitable or not personally relevant, older adults faced other barriers to implementing fall prevention strategies. These included poor health, fear of falling, finding exercise painful, feeling self-conscious or embarrassed, 57 appearing dependent, and refusing to accept the need for an assistive device. 62
The Role of Health Care Providers
Health care providers can play an important role by identifying older adults who are likely to fall and providing clinical interventions to help reduce fall risks. A recent systematic review concluded that primary care providers have the opportunity to identify people at risk of falling. 56 They are uniquely positioned to encourage fall prevention among their older patients and promote and support behavior change. To help medical providers better address older adult falls, the American and British Geriatrics Societies (AGS/BGS) developed clinical practice guidelines that (a) encourage providers to conduct fall risk screening to identify high-risk patients, (b) conduct assessments to determine fall risk factors, and (c) describe evidence-based interventions that can be incorporated into a patient’s plan of care. 63
Many older people respect the information and advice they receive from their providers. However, patients can be discouraged from undertaking fall prevention if providers seem disinterested, do not seem to take patients’ concerns seriously, do not follow up after treating patients for fall-related injuries, or are not knowledgeable about locally available fall prevention programs. 53 Dickinson et al 53 found that older adults saw doctors as “navigators, referrers and information providers.” Patients were more likely to adopt a fall prevention intervention if it was recommended by a health professional. 53 However, it was counterproductive if the information was nonspecific (eg, “keep exercising and you’ll be fine”). In addition, many health care providers failed to refer patients to interventions or to follow up after a fall injury. 53
Providers need to take into account older peoples’ views and their desire for autonomy, as well as the reasons underlying their denial or risk-taking behaviors such as climbing on ladders or not using a prescribed walking aid.43,64 It is important to consult with patients and determine what behaviors they are willing to modify to reduce their fall risk. In addition, fall prevention strategies, especially those involving exercise, need to be culturally appropriate. 48
Maximizing Uptake
To maximize uptake, fall prevention programs should enhance self-efficacy and decrease the perception that falls are an inevitable consequence of aging and cannot be prevented. Older adults greatly value independence and self-reliance, so fall prevention messages for this population must have a positive focus, be seen as personally relevant, and emphasize the benefits to remaining independent rather than focusing on the negative outcomes of falls. 35
Based on the AGS/BGS guidelines, the Centers for Disease Control and Prevention (CDC) launched the STEADI (Stopping Elderly Accidents, Deaths and Injuries) initiative. STEADI provides health care providers in primary care settings—including physicians, physician assistants, nurses, and nurse practitioners—with resources to help them screen older adult patients, assess their fall risk, and provide effective interventions and education about preventing falls. The STEADI resources include guidance on talking about fall prevention with patients that incorporates the “stages of change” model. This resource is designed to help providers determine a patient’s willingness to acknowledge their risk of falling and readiness to act, and then guide them toward adopting healthier behaviors to prevent falls.
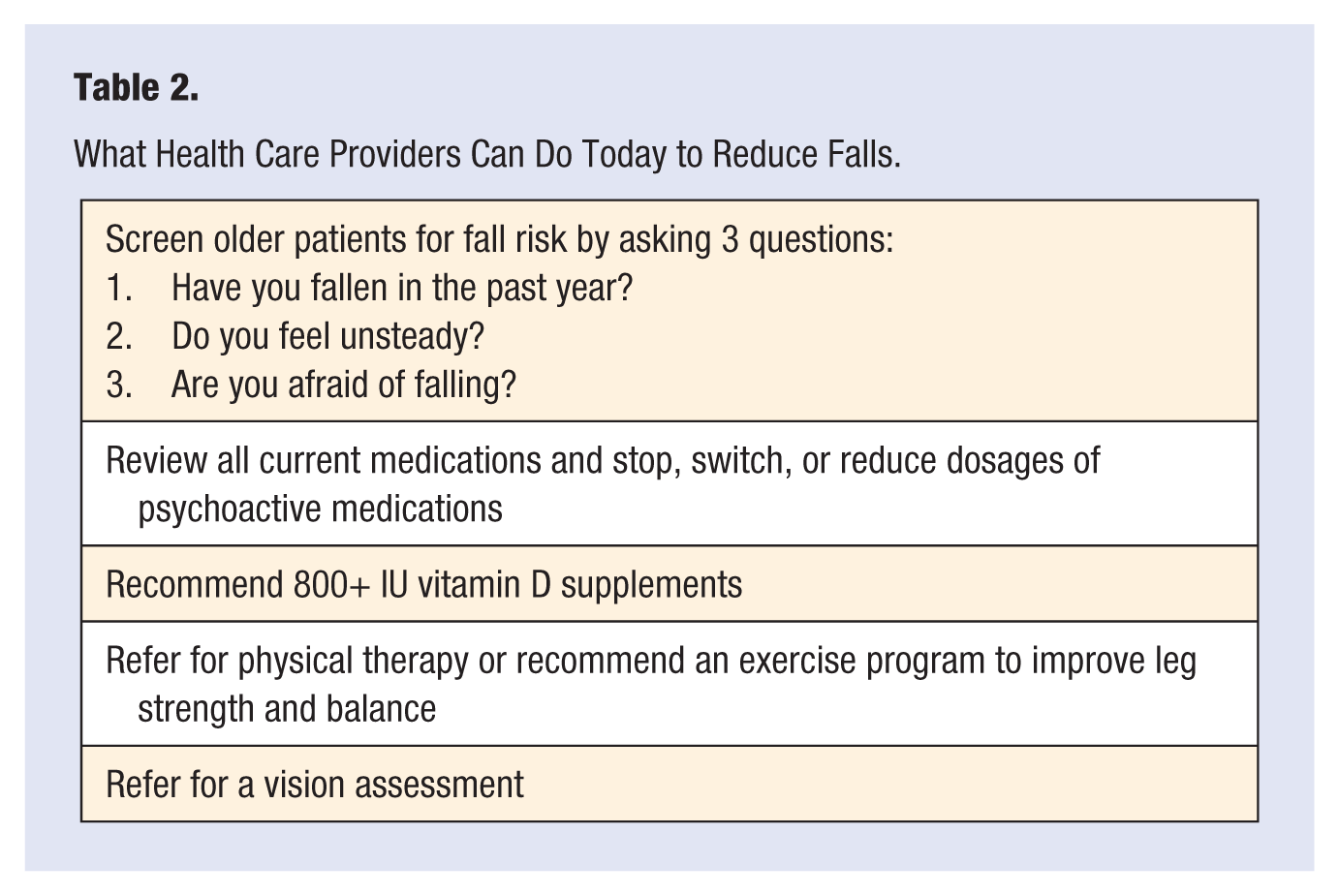
The annual Medicare wellness visit offers health care providers an opportunity to implement fall prevention. STEADI encourages clinicians to take 3 initial steps: (a) screen all older patients for fall risk by asking if they have fallen in the past year, feel unsteady, or worry about falling; (b) review each patient’s medications and stop, switch, or reduce the dosages of drugs that can increase the risk of falls, especially psychoactive medications; and (c) recommend vitamin D supplements of 800+ IU for improved bone, muscle, and nerve health. Additional steps include referrals to physical therapy, a community fall prevention, or exercise program; and referrals for vision assessment. Information about STEADI resources as well as online training courses for providers is available at http://www.cdc.gov/steadi.
In a pilot test of STEADI, CDC partnered with health departments and health systems in Oregon and New York to incorporate STEADI into primary care practices.65,66 Prior to implementing STEADI, clinicians in both sites rarely talked to their older patients about falls. After being implemented for 1 year in 19 New York practices, 65% of older patients were being screened and assessed for fall risk. 66 After being implemented in Oregon for 1 year, approximately half of older patients were being screened and assessed for fall risk. 65
Table 2 summarizes actions health care providers can take immediately to reduce falls among their older patients.
What Health Care Providers Can Do Today to Reduce Falls.
Conclusion
Health care providers face numerous challenges to reducing falls among their vulnerable older patients. Although clinicians can provide effective fall prevention interventions, many older adults do not recognize or admit that they are at risk of falling. To reduce falls, health care practitioners have to help patients understand and acknowledge their fall risk while emphasizing the positive benefits of fall prevention. They should offer patients individualized fall prevention interventions as well as provide ongoing support to help patients adopt and maintain fall prevention strategies and behaviors to reduce their fall risk. Implementing prevention programs such as CDC’s STEADI can help providers discuss the importance of falls and fall prevention with their older patients.
Footnotes
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.