
Abstract
Each year, more than 1 in 4 older adults in the United States report a fall and 1 in 10 a fall injury. Using nationally representative data from the 2016 US Behavioral Risk Factor Surveillance System, we evaluated demographic, geographic, functional, and health characteristics associated with falls and fall injuries among adults aged 65 years and older. Analyses included descriptive statistics and multivariable logistic regression to produce crude and adjusted percentages by characteristic. Characteristics most strongly associated with increased fall risk in order of adjusted percentage were depression, difficulty doing errands alone, and difficulty dressing or bathing. Characteristics most strongly associated with fall injury risk in order of adjusted percentage were depression, difficulty dressing or bathing, and being a member of an unmarried couple. The diverse health and functional characteristics associated with increased falls and fall injuries confirm the importance of screening and assessing older adult patients to determine their individual unique risk factors. Health care providers can use tools and resources from the Centers for Disease Control and Prevention’s STEADI (Stopping Elderly Accidents, Deaths, and Injuries) initiative to screen their older adult patients for fall risk, assess at-risk patients’ modifiable risk factors, and intervene to reduce risk by prescribing evidence-based interventions.
‘Overall, older adult unintentional injury death rates are about 25% higher in nonmetropolitan areas than in metropolitan areas, and falls account for 50% of these deaths . . .’
Introduction
Falls and their resulting injuries are a common occurrence among older adults (65 years and older) in the United States, with 29% reporting 1 or more falls and 11% reporting at least 1 fall injury in 2014. 1 Older adult falls resulted in 3.2 million emergency department visits, more than 900 000 hospitalizations, and more than 29 000 deaths in 2016. 2 The estimated annual medical costs for fatal and nonfatal falls are $50 billion. 3 Older adult falls are a growing burden, with the age-adjusted, older adult fall death rate increasing 30% from 2007 to 2016. 4 With 10 000 people turning 65 years old each day, the number of falls, fall injuries, and deaths will increase along with medical costs unless effective fall prevention strategies are implemented.1,3
Multiple characteristics are associated with increased fall and fall injury risk in older adults. Demographic characteristics associated with an increased risk of falls and fall injuries include being female, older age, single, or of non-Hispanic white or American Indian/Alaskan Native race/ethnicity or having a lower income.1,5,6 Health characteristics, including diabetes, arthritis, osteoporosis, heart disease, stroke, and cognitive impairment, increase the odds of an older adult experiencing 1 or more falls.5,7 In an analysis of the 2004 and 2006 Health and Retirement Study, the factors with a statistically significant association with a fall included difficulty with knees, cognitive impairment, activities of daily living limitation, poor self-reported health, use of prescription drugs, and having experienced a stroke. 5
In the United States, there is geographic variation in falls, with the percentage of older adults reporting at least 1 fall in 2014 ranging from 21% (Hawaii) to 34% (Arkansas) and at least 1 fall injury ranging from 7% (Hawaii) to 13% (Missouri). 1 The reasons for these state variations are not clear. Overall, older adult unintentional injury death rates are about 25% higher in nonmetropolitan areas than in metropolitan areas, and falls account for 50% of these deaths, but there is no difference in older adult fall death rates between metropolitan and nonmetropolitan areas.4,8
The Behavioral Risk Factor Surveillance System (BRFSS) surveys a nationally representative sample of US adults on health-related risk behaviors, chronic health conditions, and use of preventive services (http://www.cdc.gov/brfss), including, for those respondents 45 years of age and older, whether they experienced a fall or fall injury in the past year and demographic, geographic, health, and functional characteristics. A recent publication analyzed the 2014 data to produce descriptive analyses of older adult falls by health status, demographics, and state. 1 There are multiple analyses of older adult falls using BRFSS data9-12 but no recent multivariable analyses that include the multiple types of characteristics related to an older adult fall or fall injury. None of the studies have controlled for geographic indicators such as region and rural/urban status. The objective of this study is to use the BRFSS 2016 data to determine the adjusted fall and fall injury rates for demographic, geographic, functional, and health characteristics associated with increased fall and fall injury risk.
Materials and Methods
The BRFSS is an annual, random-digit–dialed telephone survey of the noninstitutionalized US civilian population aged ≥18 years conducted annually in all 50 states, the District of Columbia, Guam, Puerto Rico, and the US Virgin Islands. Detailed information regarding the survey is available online (https://www.cdc.gov/brfss). The median response rate for 2016 was 47.0%. This analysis was limited to adults ≥65 years old in all 50 states and the District of Columbia who were asked the questions about falls.
The falls questions asked in 2016 were, “In the past 12 months, how many times have you fallen?” If the response was one or more times, they were asked, “How many of these falls caused an injury? By an injury, we mean the fall caused you to limit your regular activities for at least a day or to go see a doctor.” The first question was used to estimate the percentage of older adults who reported 1 or more falls; the second question was used to estimate fall injuries. Response options ranged from zero to 76 or more, with reported means of 0.74 falls and 0.18 fall injuries. The percentages and numbers of falls and fall injuries included all adults aged ≥65 years in the denominator. Adults with responses of “Don’t know/Not sure,” “Refused,” or “Not asked or missing” for questions about falls or demographic, geographic, health, and functional characteristics were excluded, reducing the sample to 148 257 adults for fall analysis. All adults in the falls analysis were included in the fall injury analysis, with the exception of those who answered “Yes” to the fall question but responded “Don’t know/Not sure,” “Refused,” or “Not asked or missing” for the fall injury question, reducing the sample to 148 045 for fall injury analysis.
An additional factor used for analyses was alcohol use, divided into 3 categories: (1) nondrinker, has had no alcoholic drinks in the past 30 days; (2) drinker, has had 1 or more drinks in the past 30 days but no binge drinking episodes (ie, 4/5 drinks on 1 occasion for women/men); and (3) binge drinker, has had 1 or more alcoholic drinks and binge drinking episodes in the past 30 days. Rural/urban status was assigned based on the 2013 rural-urban continuum code (RUCC) for the county and state of the respondent’s residence. The 9 RUCCs were collapsed into 2 levels: urban (RUCC 1-3) and rural (RUCC 4-9; USDA, 2016). States were grouped into 10 geographical regions using the Health and Human Services region categorization (Figure 1). 13
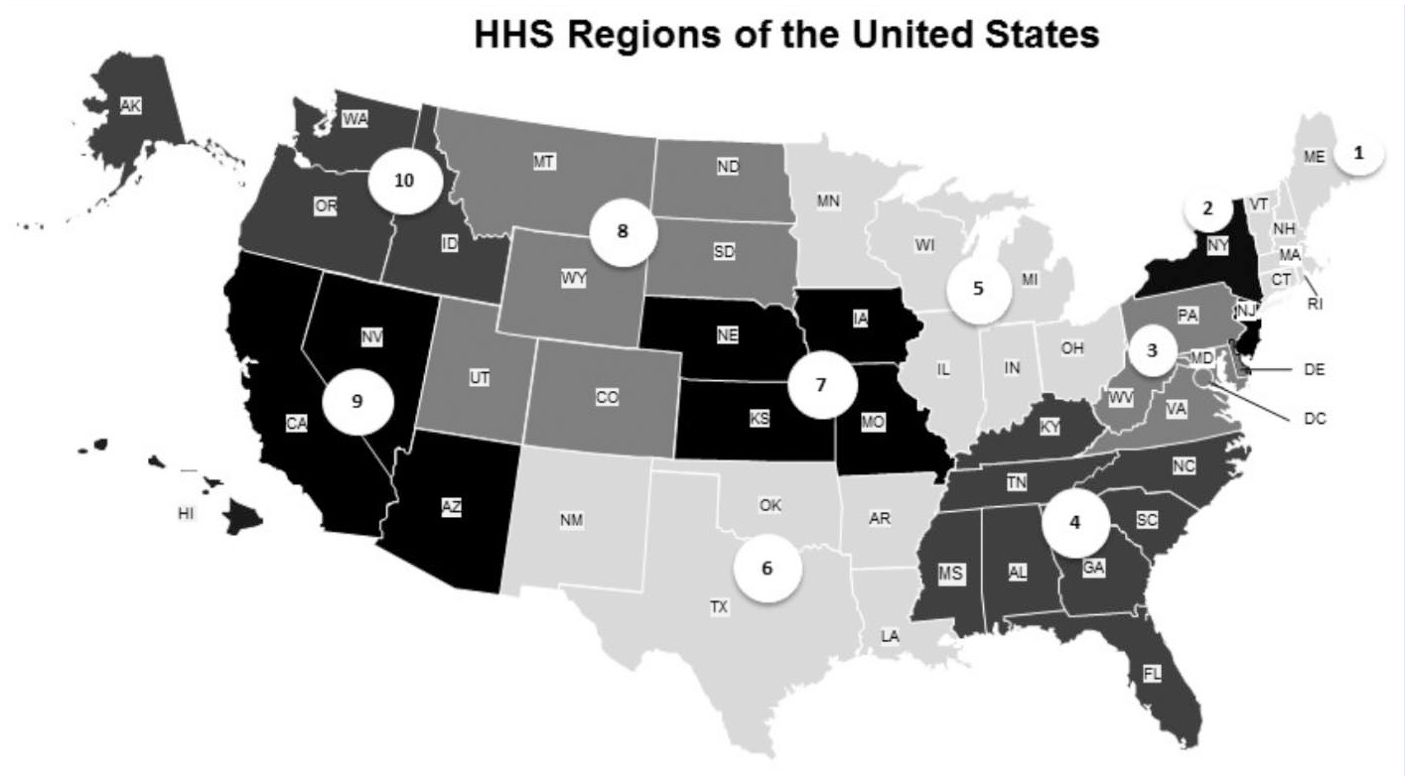
Health and Human Services regions of the United States.
Crude percentages of falls and fall injuries were calculated across the following subgroups: demographics (sex, age group, race/ethnicity, marital status, education); geographic location (urban/rural status, region); functional ability (blind or difficulty seeing; has difficulty dressing or bathing, walking or climbing stairs, doing errands alone, and/or concentrating or making decisions); and health (self-reported health status [poor, fair, good, very good, or excellent], alcohol use, stroke, arthritis, depression, and diabetes). Adjusted percentages of falls and fall injuries were calculated using logistic regression while controlling for demographic, geographic, functional, and health characteristics. For all crude and adjusted percentages, 95% CIs were calculated. Pairwise comparisons were made among subgroups for demographic, geographic, functional, and health characteristics by evaluating a 2-sample t-test at the significance level of α =.05. Linear trend tests for age group, alcohol use, education, and health status were conducted by modeling each variable as continuous. The 2016 BRFSS data were weighted by iterative proportional fitting (raking) to represent state-level population estimates and aggregated to represent a nationwide estimate. All results presented are weighted. Analyses were conducted using statistical software (SAS-callable SUDAAN v11.0.1) to account for the complex sampling design. 14
Results
Demographic Characteristics
In 2016, 29.6% of older adults reported falling one or more times, with women reporting a significantly higher percentage of falls (31.6%) compared with males (27.1%; Table 1). Falls increased significantly with age group (P < .0001), from 28.2% for 65- to 74-year-olds to 29.9% for 75- to 84-year-olds, and 37.0% for 85 years and older. American Indians/Alaskan Natives (34.7%) and multirace/other races (35.2%) reported higher percentages of falls compared with non-Hispanic blacks (23.6%), Hispanics (27.0%), and Asian/Pacific Islanders (20.5%). Those who were divorced (32.7%), widowed (33.2%), never married (31.3%), or member of an unmarried couple (34.6%) reported higher percentages of falls compared with those who were married (26.9%).
Crude and Adjusted Percentages of Older Adult Fall and Fall Injuries by Demographic, Geographic, Health, and Functional Characteristics; Behavioral Risk Factor Surveillance System, 2014. a
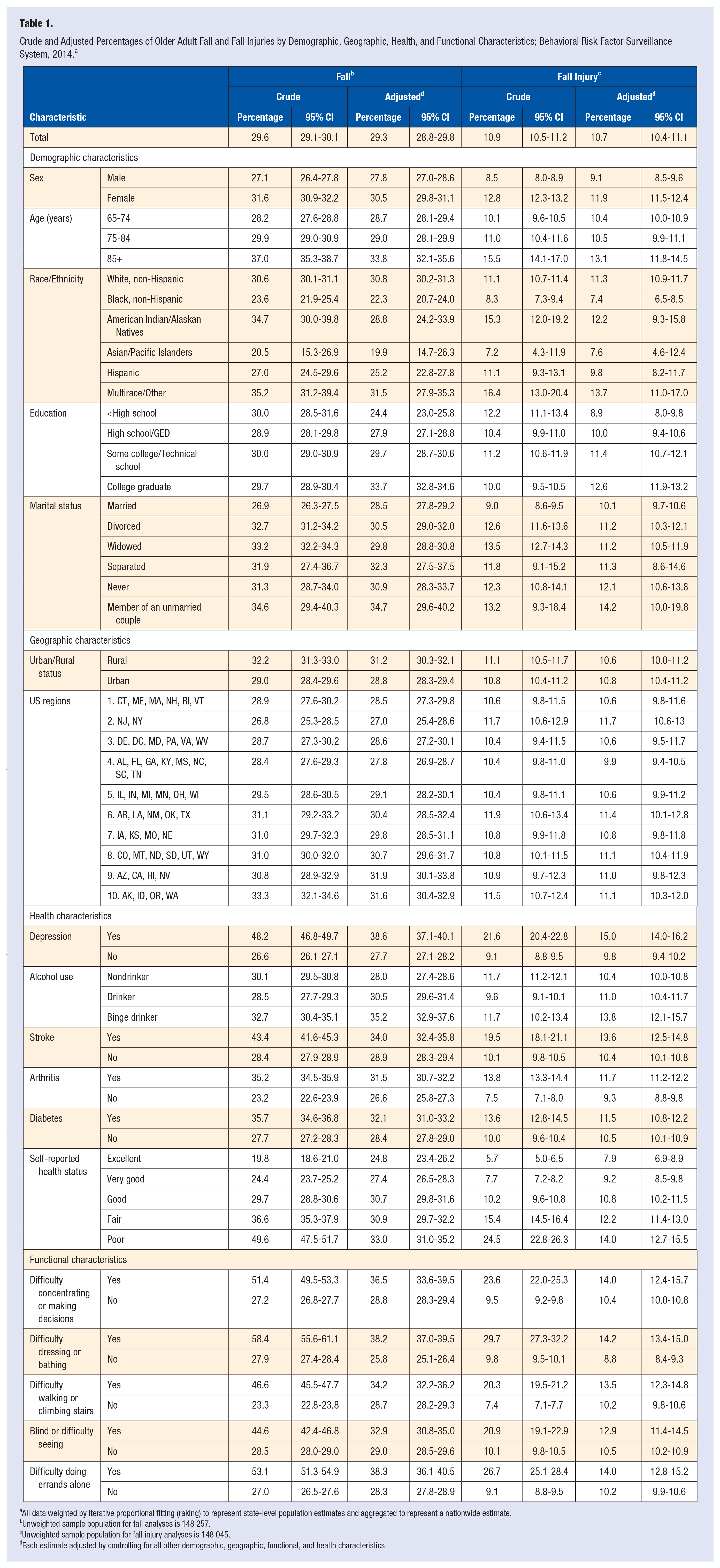
All data weighted by iterative proportional fitting (raking) to represent state-level population estimates and aggregated to represent a nationwide estimate.
Unweighted sample population for fall analyses is 148 257.
Unweighted sample population for fall injury analyses is 148 045.
Each estimate adjusted by controlling for all other demographic, geographic, functional, and health characteristics.
After adjusting for all other characteristics, fall percentages remained significantly higher among women and those 85 years and older. Non-Hispanic whites, American Indians/Alaskan Natives, and multirace/other races reported higher adjusted fall percentages compared with non-Hispanic blacks, as did those who were a member of an unmarried couple compared with those who were married. Adjusted fall percentages increased significantly (P < .0001) as educational level increased.
About one-tenth (10.9%) of older adults reported at least 1 fall injury. Women reported a significantly higher fall injury percentage (12.8%) compared with men (8.5%). Fall injury percentages increased with age group (P < .0001), from 10.1% for 65- to 74-year-olds to 11.0% for 75- to 84-year-olds, and 15.5% for those 85 years and older. American Indians/Alaskan Natives (15.3%) and multirace/other races (16.4%) reported higher fall injury percentages compared with non-Hispanic whites (11.1%), non-Hispanic blacks (8.3%), and Asian/Pacific Islanders (7.2%). Those with less than a high school education reported higher fall injury percentages of 12.2% compared with high school and college graduates (10.4% and 10.0%, respectively). Divorced, widowed, and never married older adults reported higher fall injury percentages (12.6%, 13.5%, and 12.3%, respectively) compared with those who were married (9.0%).
After adjusting, fall injury percentages remained significantly higher among women and non-Hispanic whites, American Indians/Alaskan natives, and multirace/other races compared with non-Hispanic blacks. Adjusted fall injury percentages increased with educational level increases (P < .0001).
Geographic Characteristics
A significantly higher percentage of older adults in rural areas (32.2%) reported 1 or more falls compared with those in urban areas (29.0%). By region, the percentage of respondents reporting falls ranged from 26.8% in region 2 (NJ and NY) to 33.3% in region 10 (AK, ID, OR, WA). Region 2 had a significantly lower percentage of falls at 26.8% compared with region 5 (IL, IN, MI, MN, OH, WI), region 6 (AR, LA, NM, OK, TX), region 7 (IA, KS, MO, NE), region 8 (CO, MT, ND, SD, UT, WY), region 9 (AZ, CA, HI, NV), and region 10 (29.5%, 31.1%, 31.0%, 31.0%, 30.8%, and 33.3%, respectively). After adjusting, rural older adults had a higher adjusted fall percentage compared with those who resided in urban settings. The percentage of respondents reporting fall injury ranged from 10.4% in regions 3, 4, and 5 to 11.7% in region 2.
Health Characteristics
Health characteristics associated with higher percentages of older adults reporting a fall included depression (48.2%), stroke (43.4%), arthritis (35.2%), and diabetes (35.7%). Those who drank alcohol reported a significantly lower percentage of falling (28.5%) compared with nondrinkers (30.1%) and binge drinkers (32.7%). Self-reported fall percentages increased significantly (P < .0001) as health status decreased, from 19.8% for excellent to 24.4% for very good, 29.7% for good, 36.6% for fair, and 49.6% for poor health status. After adjusting, the highest fall percentages were for those who reported depression and stroke. Adjusted fall percentages increased with increasing alcohol use (P < .0001), from 28.0% for nondrinkers to 30.5% for drinkers and 35.2% for binge drinkers. Adjusted fall percentages also increased with decreasing health status (P < .0001), from 24.8% for excellent to 27.4% for very good, 30.7% for good, 30.9% for fair, and 33.0% for poor health.
The highest fall injury percentages were among those who reported depression (21.6%) and stroke (19.5%). Nondrinkers and binge drinkers reported a higher fall injury percentage (11.7% and 11.7%, respectively) compared with drinkers (9.6%). Fall injury percentages increased significantly with health status (P < .0001), rising from 5.7% for excellent health status to 7.7% for very good, 10.2% for good, 15.4% for fair, and 24.5% for poor health status.
Those with depression reported the highest adjusted fall injury percentage. The percentage reporting fall injury increased with increasing alcohol use (P = .0005), from 10.4% of nondrinkers, to 11.0% of drinkers, and 13.8% of binge drinkers.
Functional Characteristics
The highest fall percentages were reported by those who also reported difficulty dressing or bathing (58.4%), difficulty doing errands alone (53.1%), difficulty concentrating or making decisions (51.4%), difficulty walking or climbing stairs (46.6%), and being blind or having difficulty seeing (44.6%). After adjusting, those who reported difficulty doing errands alone reported the highest fall percentage, followed by those having difficulty dressing or bathing and difficulty concentrating or making decisions. The highest fall injury percentages were for those who reported difficulty dressing or bathing (29.7%), difficulty doing errands alone (26.7%), and difficulty concentrating or making decisions (23.6%). Those who reported difficulty dressing or bathing, difficulty concentrating or making decisions, and difficulty doing errands alone reported the highest adjusted fall injury percentages.
Conclusions
Multiple characteristics are associated with falls and fall injuries, with several health and functional conditions especially related to increased risk. Depression had the strongest association after adjusting for all other characteristics, with about 40% of older adults who reported depression also reporting at least 1 fall and 15% at least 1 fall injury. Depressive symptoms in older adults increase the risk of falling by 50% based on a meta-analysis of 20 studies. 15 Falls and depression have many factors in common, including cognitive impairment, slow walking speed, poor balance, slow reaction time, weakness, low energy, and low activity levels.6,16,17 Medications used to treat depression can increase the odds of an older adult fall by 70%. 18 Interactions and precedence among falls, depression, medications, cognition, and strength and balance impairment are not well understood. Further research on these factors and their interconnectedness can inform effective prevention strategies. 15
Whereas fall and fall injury rates vary by state, 1 the current analysis by region showed no discernible patterns that might lend insight into why geographical variations exist. Living in a rural area was associated with increased fall risk but not increased fall injury risk. Overall unintentional injury death rates are higher in rural areas when compared with urban, but older adult fall death rates do not follow that pattern because they do not vary significantly by urban/rural status.4,19 Rural older adults report more chronic conditions and lower ability to independently perform activities of daily living along with higher limitation of activities caused by chronic conditions compared with urban older adults.20,21 Lower physical activity and the ability to independently perform activities of daily living are associated with increased fall risk. Older adults in rural areas may also have less access to high-quality health care. One study found that older adults with diabetes who saw a rural provider were more likely to receive an inappropriate medicine with side effects that increased their risk of falling compared with those who saw an urban provider. 22
Older adults who had difficulty concentrating or making decisions also reported high adjusted percentages of fall and fall injury. The Health and Retirement Survey study found that cognitive impairment was the strongest risk factor for a fall for those aged 77 years and older with no previous fall history and no limitations in activities of daily living. 5 Cognitive impairment is associated with gait and balance issues, which increase older adults’ fall risk. 23 Other cognitive issues such as declines in attention, psychomotor processing, problem solving, and awareness of self and surroundings detrimentally affect gait.6,23 Older adults who had difficulty walking or climbing stairs, and dressing or bathing were also at increased risk, and this is consistent with other research. 24
Those aged 75 to 84 years reported a higher percentage of fall injury compared with those aged 65 to 74 years old in the crude results but not after adjusting, suggesting that characteristics other than age are responsible for increased fall injuries in the older age group. Arthritis, vision problems, and diabetes are examples of health and functional characteristics that increase with age and are associated with increased fall risk. 6 Potentially, evidence-based strategies that prevent or reduce the impact of these risk factors could reduce fall injuries, independent of age. Adjusting for other characteristics also changed the relationship of drinking status to falls, so that fall risk increased with increasing levels of alcohol consumption. Nondrinking is associated with poorer health, 25 so adjusting for health conditions in our study possibly accounted for the differences between crude and adjusted percentages. Regular alcohol intake is associated with decreased lower-extremity strength and cognitive function, impaired balance, peripheral neuropathy, skeletal myopathy, and postural hypotension, all of which are fall risk factors. 26
This study has at least 5 limitations. First, BRFSS data are self-reported and subject to recall bias. Second, BRFSS does not include persons in long-term care facilities who are at higher risk for falls. 27 Third, the broad definition of fall injury used for this analysis might have resulted in a higher estimate of older adults suffering injurious falls compared with other reports. Fourth, the response rate (median = 47%) could have resulted in nonresponse bias; however, weighting procedures based on the survey methodology were used to adjust the estimates and reduce the effect of nonresponse bias. Finally, because of the cross-sectional nature of data collection, the temporality of the characteristics cannot be determined (ie, it cannot be determined whether someone’s poor health contributed to their fall or if the fall contributed to their poor health).
Effective older adult fall prevention strategies require understanding and addressing the characteristics associated with increased risk, including characteristics that are unmodifiable (demographics), difficult to modify (geography), and potentially modifiable (health and functional conditions). Designing and implementing evidence-based strategies to address modifiable characteristics can reduce fall risk. Unmodifiable characteristics can define groups to target for intervention and for research to determine modifiable fall risk factors that put these groups at higher risk. For example, older women’s increased fall risk may be partially explained by lower levels of physical activity and decreased lower-body muscle strength compared with older men, 2 risk factors that can be addressed with evidence-based exercise programs.6,28
The multiple characteristics associated with falls suggest that a comprehensive approach to reducing fall risk, which includes screening and assessing older adult patients to determine their unique, modifiable risk factors and then prescribing tailored care plans that include evidence-based interventions, is needed. The Centers for Disease Control and Prevention developed the STEADI (Stopping Elderly Accidents, Deaths, and Injuries) initiative (http://www.cdc.gov/STEADI), based on the American and British Geriatrics Societies’ Clinical Practice Guideline for Prevention of Falls in Older Persons, 29 to help clinicians screen, assess, and intervene to reduce fall risk. Whereas physicians cite a lack of time and educational materials as barriers to including fall prevention in their older adult practice, 30 STEADI provides an algorithm that can be modified to fit into clinical practice and provides educational materials to reduce these barriers. STEADI has been successfully implemented in outpatient health care, achieving high screening and reducing the odds of fall-related hospitalization.31-33 With the population aging, there will be an estimated 55% increase in the older adult population in 2030 compared with 2014. 1 Older adult falls will impose an increasing burden on the US health care system unless effective interventions, such as those encouraged through the STEADI initiative, are implemented to reduce fall risk factors and prevent falls.
Footnotes
Acknowledgements
We would like to acknowledge Robin Lee, PhD, and Marcie-Jo Kresnow, MS, both of the US Centers for Disease Control and Prevention’s National Center for Injury Prevention and Control, for their assistance in shaping the analysis and presentation of data. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.