
Abstract
Objective
Sleep quality affects pregnant women’s health and quality of life. The aims of the study were to investigate the prevalence of sleep disorders and the effect of sleep health education on sleep quality in pregnant women with sleep disorders.
Methods
To examine the frequency of sleep disorders among pregnant women, a cross-sectional study was conducted with an initial enrollment of 370 participants. Subsequently, 162 pregnant women were recruited for a pretest-posttest quasi-experimental design study. The intervention group (n = 82) performed sleep health education for four weeks and the control group (n = 80) received standard care. Sleep quality was assessed with Pittsburgh Sleep Quality.
Results
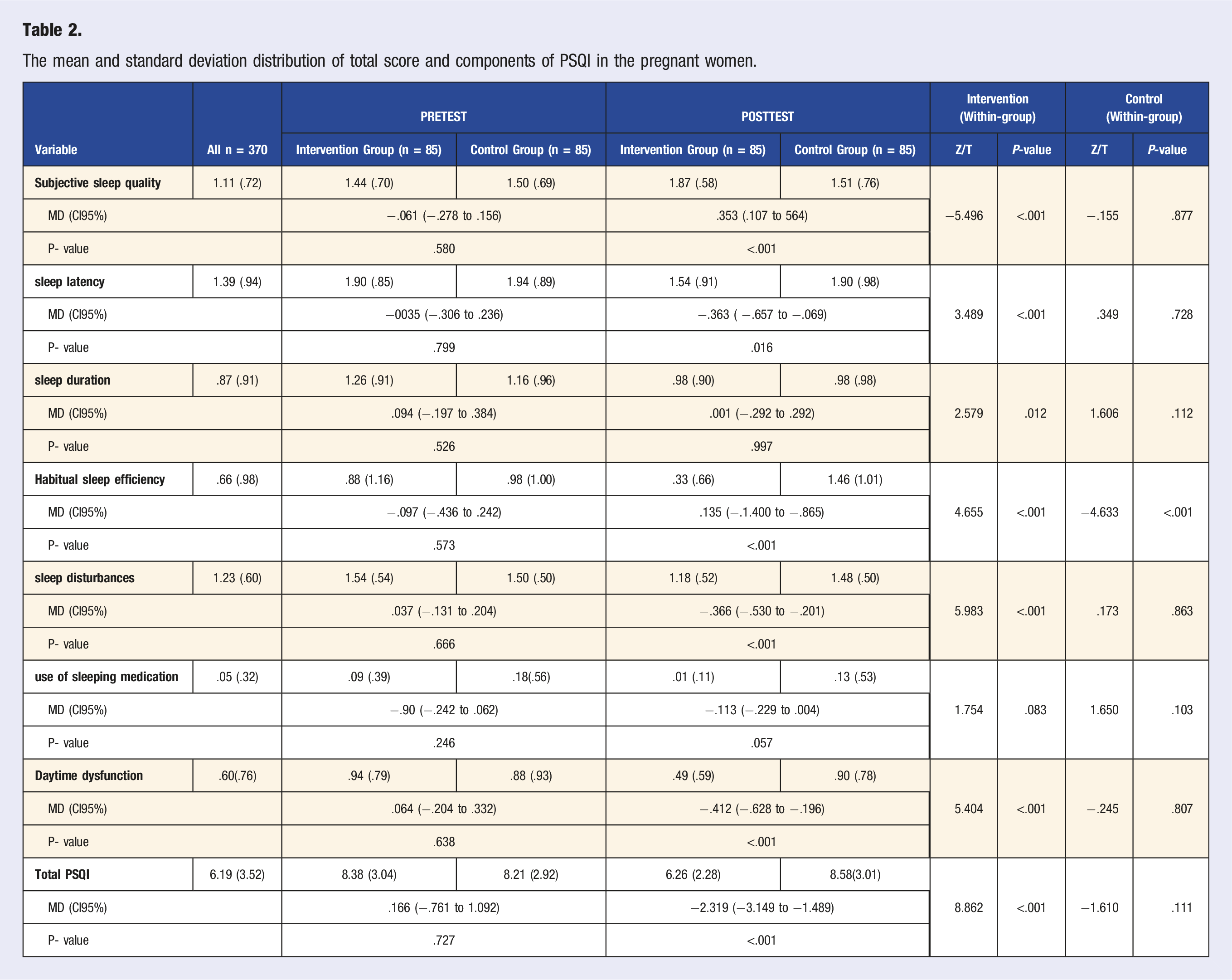
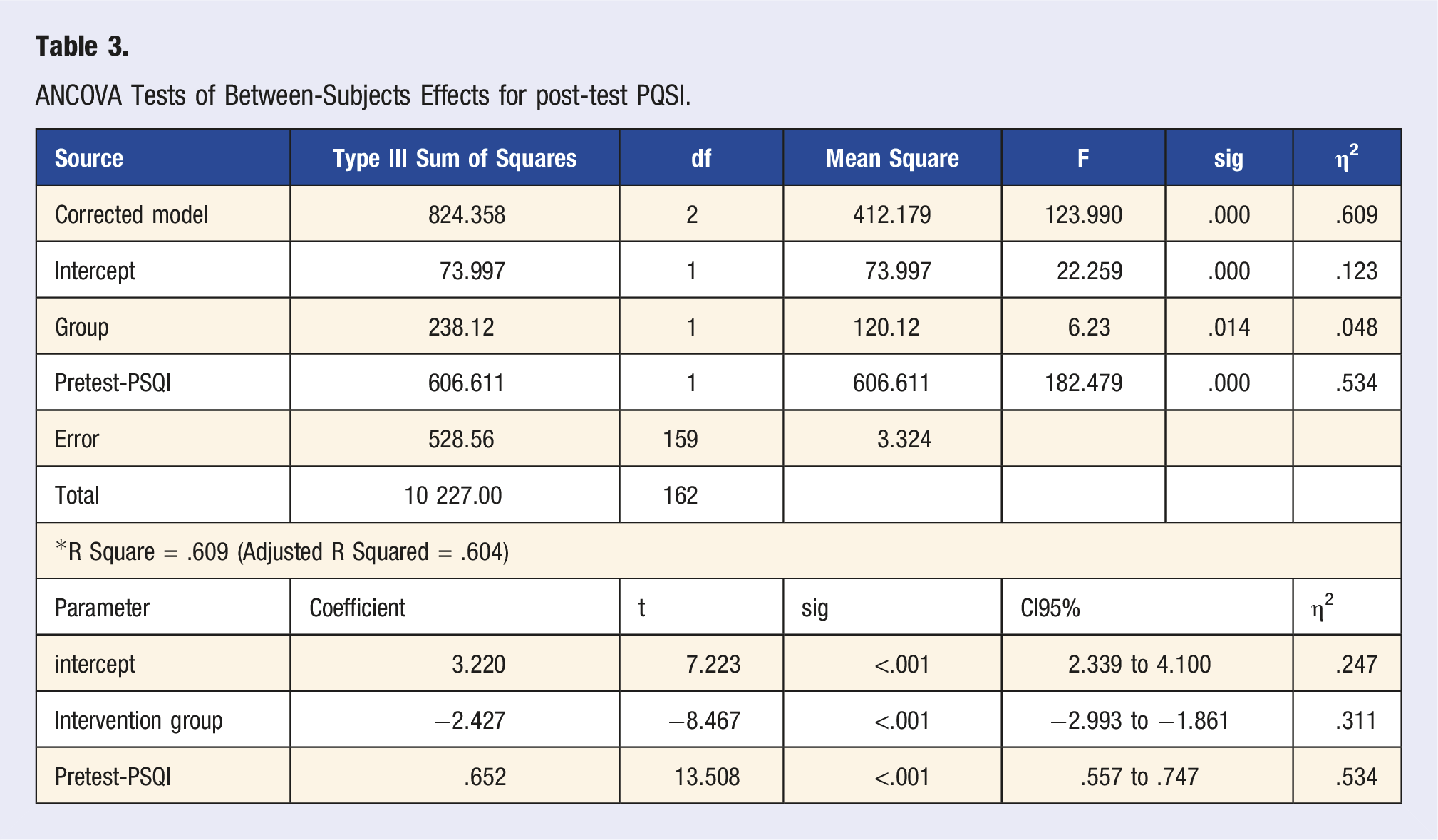
The prevalence of sleep disorder was 61.9 percent (CI 95% 56.85-66.69). It was determined that health education improved some sleep quality subscales including subjective sleep quality, sleep latency, sleep duration and habitual sleep efficiency, and sleep disturbances, daytime dysfunction, and global sleep quality. The difference was still significant after adjusting for the PSQI baseline (η2 = .311, P < .001).
Conclusion
These findings provide evidence of a relatively high prevalence of sleep disorders in pregnancy. Therefore, screening for sleep disorders and providing supportive programs and models to improve sleep quality during pregnancy should be considered as part of prenatal care.
Introduction
Sleep disorders are one of the most prevalent problems that tend to occur during pregnancy,1,2 dramatically increasing from 63% in the first trimester to 80% in the second trimester.3-6 Nonetheless, sleep disturbances in pregnancy have the highest prevalence in the third trimester.4,7 During pregnancy, various sleep disruptions can occur, ranging from insomnia, nocturnal awakenings, and parasomnias (with a particular emphasis on restless leg syndrome) to snoring and excessive sleepiness. 8 Pregnancy hormones, including growth hormone, prolactin, melatonin, cortisol, thyroid-stimulating hormone, and oxytocin, as well as placental hormones such as gonadotropin, progesterone, and estradiol, can impact the sleep cycle. 9 Sleep disorders can arise from a combination of psychological, physical, and metabolic changes. These disorders can also lead to psychological alterations1,7 so that the quality and pattern of sleep are associated with psychological factors, such as pregnancy depression. 10 Pregnant women who have trouble sleeping are also more likely to develop hypertension, preeclampsia, and intrauterine growth restriction (IUGR).2,11 Sleep assumes greater importance when considering that sleep disorders reduce people’s daily activities. 12 Sleep problems can generally reduce the quality of life in pregnant mothers,13,14 leading to increased treatment costs and consequent problems.15,16
Nowadays, it is recommended to use non-pharmacological and non-invasive methods, such as relaxation and sleep hygiene to improve sleep, especially in pregnant women, this methods are used to obtain greater satisfaction and reduce the probable side effects.17,18 Sleep hygiene includes all healthy habits (such as reduced TV time and fluid intake before sleeping). 19 Due to close associations between mental and physical health, as well as excessive vulnerability of pregnant women and direct impact of maternal health on the fetus, numerous researchers have turned their attention to non-pharmacological and applicable methods effective in physical and mental health of pregnant women. 13 Nevertheless, sleep disorders during pregnancy have remained a neglected issue. 20 Any attempt to eliminate sleep disorders and improve sleep quality during pregnancy can be a complex issue that should be considered by healthcare providers.7,21 As reported in previously conducted studies, the required measures for the enhancement of sleep quality could be different.14,21 Nonetheless, according to researchers, one of the vital requirements for improving sleep quality among pregnant women can be sleep health education. 22
Sleep hygiene training programs aim to prevent inappropriate individual behaviors that can disrupt the normal sleep pattern.23,24 These interventions aim to increase awareness of healthy behaviors, such as maintaining a good sleep environment, engaging in regular exercise, consuming a nutritious diet, and refraining from alcohol and cigarette use.24-26 A systematic review study of 16 articles involving 1252 pregnant mothers 7 assessed the effectiveness of various interventions, including cognitive-behavioral and pharmaceutical intervention, acupuncture, yoga, relaxation, and herbal medicines, and they concluded that there is a dearth of evidence in this field and pointed to an urgent need for high-quality studies to solve sleep problems during pregnancy and the implementation of effective programs in prenatal care.
In light of the aforementioned issues, the present study aimed to determine the prevalence of sleep disorders among pregnant mothers and assess the effect of sleep health education based on regular follow-up on sleep quality in pregnant women with sleep disorders.
Methods
Study Design and Participants
The study was conducted in two phases. Initially, a cross-sectional study was performed to assess the prevalence of sleep disorders. Subsequently, an open-label, parallel-group, two-arm quasi-experimental design based on a pretest-posttest approach was conducted in Tabriz, Iran, between January and May 2022. The study population comprised all pregnant women who attended the prenatal care unit in Azahra and Taleghani hospitals, which are two referral hospitals in the northwest region of Iran. The inclusion criteria for the intervention phase of the study were as follows: (1) singleton pregnant women who were 18 years old or older; (2) ability to read and write; (3) gestational age between 24-32 weeks based on early pregnancy sonography; (4) not using anti-anxiety and depression drugs; (5) absence of experiences of traumatic events in the past 6 months, such as the death of close relatives; and (6) pregnant women with a score of 5 or higher based on the Pittsburgh sleep quality scale and absence of chronic medical diseases. Exclusion criteria included absence in two or more sessions, use of any drugs and herbal medicines that affect the outcome of the study during the study, premature delivery, and not completing more than 10% of the questionnaires.
Sample Size and Sampling
The sample size was calculated 333 pregnant women based on the results of a study by Hung et al.
27
considering an acceptable error of 5% around the mean (7.3 m = ), 95% confidence interval, 90% statistical power and standard deviation of 3.4 for the sleep quality scale by the following formula. Considering 10% loss rate and invalid questionnaires, 370 questionnaires were planned to be collected.
Then for the intervention phase, the sample size was calculated at 79 subjects using according to formula and based on the score of sleep quality reported in the study by Jahdi et al. 28 Nonetheless, considering a 10% sample attrition in the intervention and follow-up program, the sample size was increased to 85 cases in each group and a total of 170 participants.
Alpha = .05, power = .80, m1 = 6.61, m2 = 7.85, sd1 = 3.16, sd2 = 2.38 Participant flow.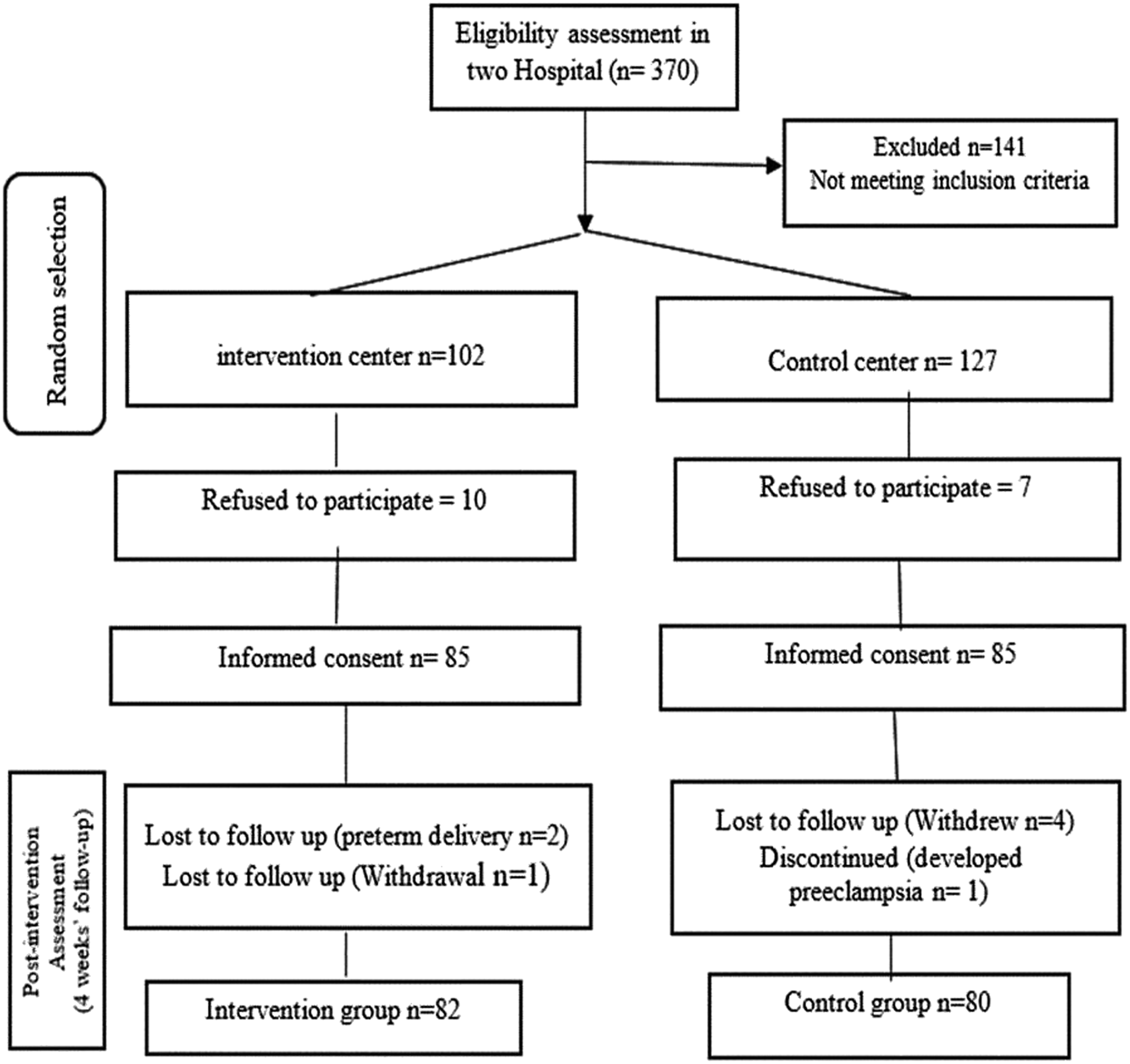
Data Collection Tools
Demographic and Obstetrics Characteristics
Including age, educational status, gravidity, family income, height and weight to calculate BMI (Based on the first visit of pregnant women in the first trimester, which in most cases is in the sixth week of pregnancy) and medical and obstetrical history.
Sleep Quality Assessment (PSQI)
The Pittsburgh Sleep Quality Index (PSQI) is an effective retrospective instrument adopted by Buysse et al, 29 (1989). It is used to measure the quality and patterns of sleep in adults. It differentiates “poor” from “good” sleep quality. It consisted of nineteen self-rated questions. The 19 questions consist of seven component scores (subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications, and daytime dysfunction over the last month); each component has a range of 0-3 points. A score zero indicates no difficulty, while a score 3 indicates severe difficulty. Then the seven components score added to yield a global score ranging from zero to 21, with higher scores indicating worse sleep quality. If the woman’s PSQI score was ≥5 considered poor sleeper. The Cronbach’s alpha of this questionnaire was calculated to be (.73). 30 HosseinAbadi, et al 31 (1387) reported the reliability (r = .88) and the reliability of the questionnaire via retest (r = .84) in Iran 32 . In our study, the Cronbach’s alpha of this questionnaire was calculated at .85.
Intervention and Implementation Steps
Pregnant women with inclusion criteria were included in the study and participants were divided into two groups based on the hospital. Before the study, the objectives of the study were expressed to the participants and informed written consent was obtained. In the intervention group, during a two to three-hour session, sleep hygiene was fully explained and taught to the participants.
The educational content covered topics such as normal sleep patterns and pregnancy-related sleep changes, as well as strategies for coping with physical changes that disrupt sleep. The program emphasized the importance of practicing good sleep hygiene, including establishing a regular bedtime routine, exercising regularly, eating a healthy diet, avoiding caffeine and nicotine before bedtime, and limiting intake of gas-producing foods and water. Participants were also advised to reserve their bedroom for sleep and sex only, and to create a comfortable sleeping environment by keeping the room dark, cool, and quiet. At the conclusion of the sessions, women were provided with an instructional guide.
After the training session which lasted for 60-90 minutes, every week until the end of the four weeks, the pregnant mothers were followed up by the researcher by sending daily text messages (SMS), and the educational materials were sent as a reminder to observe all the taught materials every week. The control group did not receive any sleep hygiene training while receiving routine prenatal care, which was based on Iranian prenatal care guidelines. In this guideline, there isn’t any screening program for sleep disturbances. It should be noted that at the end of the study, an educational file was provided to the control group. Finally, at the end of the fourth week of the training program, the Pittsburg questionnaire was completed again by the participants in both groups.
Data Analysis
Data were analyzed based on the per-protocol approach using SPSS v24.0 (IBM, Armonk, NY, USA). There were 10% missing data in demographic characteristics, which were imputed with the mean substitution method. Descriptive statistics are used to present the data. Differences in baseline variables between the two groups were evaluated with the t test and chi-squared test. The Wilcoxon, Mann–Whitney U test, paired t test, and t test were used to evaluate within-group and between-groups differences in subscales and total PSQI, respectively. ANCOVA was used to compare the total PSQI between the two groups by adjusting the pretest-PSQI as a confounding variable. The normal distribution of data was assessed using the Kolmogorov-Smirnov test, skewness, and kurtosis. Although the data were slightly skewed, the data were considered normal because skewness and kurtosis were 1 to −1. All P values are two-sided. P values less than or equal to .05 were statistically significant.
Results
In total, 370 pregnant women were enrolled in the cross-sectional phase. The average age of the participants was approximately 31.37 years, and 55.4% of them are over 30 years old. Besides, most of the pregnant women were housewives, 83.3% of them had a college education level or above. 58.6% of the pregnant women were nulliparous. The mean (SD) of total PQIS was 6.19 (3.52) and the prevalence of sleep disorder was 61.9 percent (CI 95% 56.85-66.69).
Baseline Characteristics of the pregnant women.
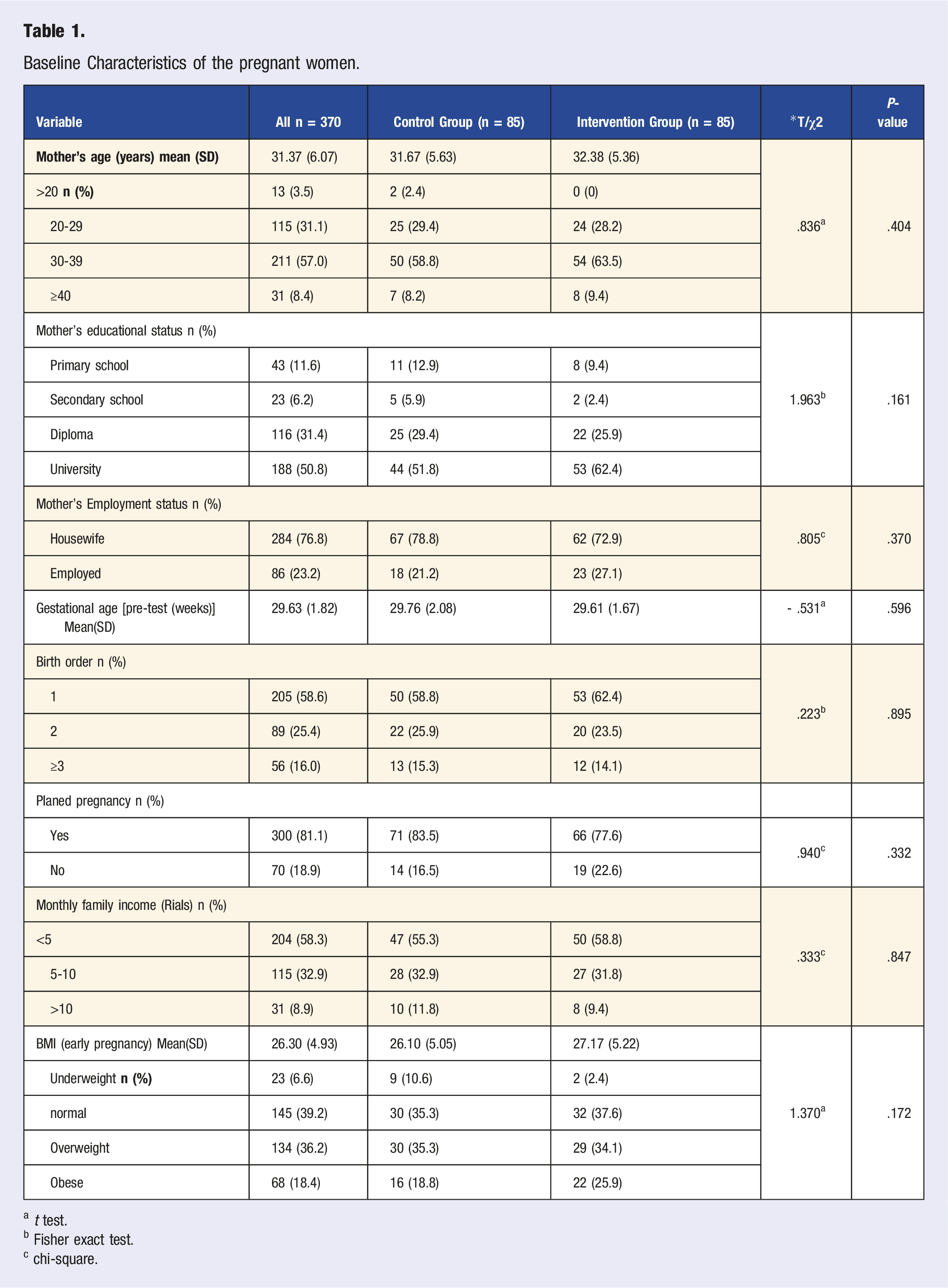
a t test.
b Fisher exact test.
c chi-square.
The mean and standard deviation distribution of total score and components of PSQI in the pregnant women.
ANCOVA Tests of Between-Subjects Effects for post-test PQSI.
Discussion
As evidenced by the results of the present study, approximately two-thirds of pregnant women (about 62%) suffer from sleep disorders. Moreover, this study demonstrated that the effect of sleep hygiene training and weekly follow-up for four weeks led to a reduction in sleep disorders and improved sleep quality in pregnant women. After the intervention, the intervention group had significantly lower PSQI (Pittsburgh Sleep Quality Index) scores, compared to the control group. This finding supports the study hypothesis. The assessment of sleep quality status in pregnant women participating in the present study pointed to a moderate to low PQSI total score. However, a significant percentage of pregnant women were reported to suffer from sleep disorders. Based on the literature review, the prevalence of sleep disorders has been reported from 6%-100% in other studies conducted in different parts of Iran.28,33,34
A study performed on 312 pregnant women in the second trimester pointed out that the prevalence of sleep disorders was 87%. 35 In another study that examined sleep quality among pregnant women in the third trimester, researchers reported that the prevalence of sleep disorders was about 90%. 34 A review of the literature also illustrated that the prevalence of sleep disorders is different in other parts of the world. 16 In a study on Taiwanese pregnant women in different trimesters, the average score for the overall sleep quality was 7.25, and the prevalence of sleep disorders was 65%. 27 In their study on 215 pregnant women between 15-25 weeks of gestation, Kamysheva et al reported an average sleep quality score of 6.1. 36 The results of recent studies are consistent with those obtained in the current research; for instance, in a study on the prevalence of sleep disorders among pregnant women in the third trimester in the United States, the average total sleep quality score was 8. 37 It can be stated that observed contradictions in the prevalence of sleep disorders in different studies can be ascribed to various reasons, such as different characteristics of pregnant women in terms of gestational age and considering the cut-off score to determine the rate of sleep disorders since in some studies, scores less than 5 have been regarded as the basis for the absence of sleep disorders.
Another aim of the present study was the assessment of the effect of sleep hygiene education and continuous weekly follow-up for four weeks on sleep quality among pregnant women with sleep disorders. Based on the results of the present study, the mean total PSQI score in the intervention group was significantly lower one month after sleep hygiene training, as compared to that before the intervention. However, the total sleep quality score slightly increased in the control group. That is to say, their sleep quality decreased, compared to the commencement of the study. The control between the two groups also displayed that the educational intervention improved sleep quality in the intervention group, and the observed difference between the two groups was significant. The total PSQI score in the intervention group was reduced by 2.427, compared to that in the control group considering the basic PSQI score as a covariate variable, and this difference was also statistically significant. The results obtained from the assessment of sleep quality subscales also demonstrated an improvement in sleep quality in pregnant women in the intervention group. Nonetheless, in the control group, the total score and scores of other subscales increased after four weeks, and the quality of sleep decreased. This decrease was especially significant in the habitual sleep efficiency dimension. Hung et al. 27 indicated a gradual linear decline in sleep quality as the pregnancy progressed. However, as demonstrated in the control group in the present research, in the stated study, the scores of sleep latency, average sleep efficiency, and subjective sleep quality scores increased significantly in the third trimester, which is indicative of poor sleep quality. The intervention used in the present study yielded results similar to those obtained by non-pharmacological interventions, such as relaxation exercises, 38 music listening, 26 distance education or Telehealth, 39 face-to-face sleep hygiene training, 28 and sleep hygiene practices 40 that improve sleep quality. In addition, studies on diabetic patients41,42 and hemodialysis patients43,44 have also indicated that continuous and follow-up care can improve sleep quality among the participants. The findings of the present study are supported by other researchers, including Rezaei, 45 and Al Saeed Mohammad, 40 who used behavioral interventions and sleep hygiene exercises, respectively. Along the same lines, Rezaei et al. 45 examined behavioral sleep training in pregnant women and its effectiveness in the reduction of depression in pregnancy and improvement of the overall score of sleep quality and its components, such as subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, and dysfunction in daily activities.
In their study on pregnant women, Marvi et al. 39 compared two training methods of continuous care and the remote health training model. They reported that although both methods could improve sleep quality in pregnant women, remote intervention yielded better results and was easy to use, while the results of a study by Holmqvist et al. 46 illustrated that both methods were equally effective. Continuous interventions and care are of paramount importance since the most appropriate programs lose their desired effect over time in the absence of control and follow-up. Proper follow-up, continuing counseling process, and phone calls according to client’s needs can be the main prerequisites to achieve the desired results of intervention programs.
Limitation
Among the notable limitations of this study, we can refer to convenience sampling and non-random allocation of participants, and the presence of selection bias which can affect the generalization of the results. Furthermore, the use of self-report questionnaires for data collection is subject to some biases and can affect the provided responses. Also, there was an unavailability of polysomnography data and therefore, the presence of sleep-disordered breathing could not be assessed. It is suggested, in future studies, researchers should design long-term training courses and conduct investigations to assess and improve sleep quality in high-risk pregnancies. It is also recommended to carry out interventions from the beginning of pregnancy and to investigate their effects. In addition, a future study would be nice to track if this intervention of sleep hygiene education has the potential to lower gestational diabetes, preterm birth, and preeclampsia.
Conclusion
The results of the current study pointed to a relatively high prevalence of sleep disorders in pregnancy; nonetheless, a proper sleep health education program can effectively improve sleep quality. Due to the high prevalence and variability of sleep disorders during pregnancy, sleep quality screening can significantly help identify pregnant women suffering from these problems. Moreover, intervention programs, as well as training and follow-up counseling, can be effective in the enhancement of sleep quality; therefore, such support programs should be a part of prenatal care.
CME/CE Article Quiz
American College of Lifestyle Medicine (ACLM) members can earn FREE CME/CE credit by reading this approved CME/CE article and successfully completing the online CME/CE activity. Non-members can earn CME/CE for $40 per article. Visit lifestylemedicine.org to join the ACLM.
AJLM CME/CE Articles and Quizzes are offered online only through the American College of Lifestyle Medicine and are accessible at lifestylemedicine.org/store. ACLM Members can enroll in the activity, complete the quiz, and earn this CME/CE for free. Non-members will be charged $40 per article.
A Passing score of 80% or higher is required in order to be awarded the CME/CE credit.
Supplemental Material
Supplemental Material - Prevalence of Sleep Disorders and the Effect of Sleep Health Education on Sleep Quality in Pregnant Women With Sleep Disorders
Supplemental Material for Prevalence of Sleep Disorders and the Effect of Sleep Health Education on Sleep Quality in Pregnant Women With Sleep Disorders by Kosar Sarvaran, Fatemeh Abbasalizadeh, Maede Alaei and Azita Fathnezhad-Kazemi in American Journal of Lifestyle Medicine.
Footnotes
Acknowledgments
We thank the women who participated in the study. We also appreciate the support from the Islamic Azad University of Tabriz Medical Sciences.
Declaration of Conflicting Interests
The authors declare that they have no competing interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical considerations in this research included protection of information confidentiality, obtaining informed written consent from participants, and the right to withdraw from the research at any time without penalty. This research has been approved by the Ethics Committee of Tabriz medical sciences Islamic Azad University, Iran (code number; ![]() ).
).
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.