
Abstract
Significant contributors to rising health care costs are diseases influenced by lifestyle, such as cardiovascular disease, diabetes, and cancer. Unfortunately, American medical education devotes disproportionately little time training future doctors in prevention. Approach. With the support of medical education leadership, medical students collaborated with a faculty advisor at Wake Forest School of Medicine to test the feasibility of a broad-based, student-led lifestyle medicine curriculum. After 3 introductory sessions delivered to an entire medical school class, a smaller pilot series with 16 first-year medical students was held after-hours, featuring experiential learning in nutrition and cooking, physical activity, and sleep. The 8 modules were designed to improve student health, wellness, and knowledge of health behaviors. Feedback. The program was implemented into the first-year medical school class. An unforeseen benefit of the pilot was increased student volunteering in community-based wellness activities and research. Two components of success were the hands-on, experiential modules and being student-led. Details on curriculum development, schedule, and content are provided.
‘. . . the American medical education system devotes disproportionately little time training future doctors in prevention of chronic diseases.’
The United States spends $3.2 trillion annually on health care, an average of nearly $10 000 per person. 1 Much of this expenditure can be directly attributed to management and treatment of cardiovascular disease, diabetes, and cancer. While these diseases are multifactorial, they are greatly influenced by lifestyle and can be prevented or reduced through diet, physical activity, and healthier sleep patterns. The financial implications and anticipated decrease in national life expectancy attributable to these preventable diseases illuminate the need to address these illnesses at their roots. 2
Unfortunately, the American medical education system devotes disproportionately little time training future doctors in prevention of chronic diseases. Less than 30% of medical schools required the recommended 25 hours of nutrition education, 3 and only 25% required a dedicated course on nutrition. 4 Furthermore, less than a third of medical interns felt they received adequate education on clinical nutrition. 5 Sleep, stress management, and exercise/physical activity are equally neglected in medical education, and also contribute greatly to obesity and chronic disease outcomes. In addition to improving their own well-being, medical students with healthier lifestyles are more invested in preventive counseling for their patients. 6
Schools of medicine and allied health professions are beginning to address this issue. Many schools are focusing curriculum innovations to increase student and physician competence in counseling patients about their physical activity.7,8 A systematic review in 2014 described 10 educational programs focusing on physical activity counseling in medical schools, showing increased attention to the issue. The authors concluded more information is needed to determine how these curricula affect physician practice and patient outcomes. 8
Hands-on approaches provide students opportunities to learn while interacting with patients. At the University of Central Florida, medical students were trained as lifestyle coaches to work with football players as a means to improve players’ athletic performance. 9 A more widespread curriculum was implemented at a medical school in Israel that included over 58 hours across 5 of the 6 years of medical school, including training in nutrition, physical activity, smoking cessation, and health coaching, with opportunities to “practice” with friends, family, and patients. 10 The curriculum and opportunity to coach was well accepted, and students noted increased interest in their own health.
Students at Wake Forest School of Medicine (a private medical school in Winston-Salem, North Carolina) aimed to address lifestyle issues in medical students and increase their knowledge base and confidence in personal health behavior change. Not wanting to solely focus on nutrition, as in culinary medicine, 11 students desired to include other lifestyle behaviors. Two first-year medical students who volunteered with a pediatric weight management program (Brenner FIT, www.brennerchildrens.org/brennerfit) were inspired to include health behavior elements into the medical school curriculum. Using their experiences in medical school to guide planning and implementation, the students worked with a faculty advisor to develop a curriculum. The overall goal of the curriculum was to teach medical students, in a personal and experiential fashion, about health behaviors and health behavior change. Given the difficulty of incorporating new elements into a full medical school curriculum, the group decided to test the idea as a pilot program. The purpose was to assess feasibility of scheduling and operations, and if students would participate in such a program (acceptability). This student-led pilot highlighted the use of a community-based teaching kitchen, where students experienced and practiced with different foods, recipes, and skills, through an existing partnership with the YMCA. This report describes development and implementation of this program.
Approach
At the end of their first year, 2 medical students approached a faculty advisor with a background in obesity treatment with the idea of lifestyle medicine activities. They met with the medical school’s Associate Dean for Student Affairs, who suggested adding the program to a newly designed 4-week orientation program. This orientation, focused on personal wellness and self-care, was designed to address high rates of student burnout and to better prepare first-year students for the rigors of medical school.
Curriculum Development
Students at Wake Forest are actively engaged in curriculum development and evaluation. The student leaders and faculty advisor jointly developed the following core principles to guide curriculum development:
Activities would involve hands-on, experiential learning, with minimal didactic presentations.
The curriculum would go beyond nutrition and physical activity and include sleep and health-supporting behaviors such as cooking, meal planning, and grocery shopping.
Curriculum must be evidence based in its content.
Stress management was thoroughly covered during student orientation, so it was not formally included in this curriculum, although it was hoped the pilot sessions would reduce stress among participants.
Using foundational principles of pediatric and family-based lifestyle modification from Brenner FIT (Families In Training), 12 core health behaviors were identified and incorporated throughout the program. Learning objectives were developed for each activity, focusing on behaviors surrounding health and health outcomes. Modules were designed to complement the first-year medical school curriculum with experiential, and hopefully enjoyable, activities, as similar programs have accomplished. 7 An example was a nutrition activity featuring micro- and macronutrients. While nutritional biochemistry is a “block” module of the larger biochemistry class, it does not incorporate nutritional recommendations. Thus, this new curriculum aimed to integrate the nutritional behavior of building a balanced plate (www.myplate.gov) with the biochemistry learned in the classroom. Additionally, during the anatomy section, clinically relevant implications of exercise science on the muscles, bones, or other anatomy are not covered in the laboratory. Therefore, an activity module was planned to demonstrate bone- and muscle-strengthening exercises to students. Under the guidance of the faculty advisor, the students collated the evidence base on which to build the curriculum, primarily through literature searches (with a focus on position statements and guidelines), professional organizations (American College of Lifestyle Medicine, American Heart Association, American College of Preventive Medicine), and one-on-one meetings with the faculty advisor. The students assisted in developing presentations and planning activities aimed at the learning level of a first-year medical student, with a focus on engaging and enjoyable sessions.
Orientation and Recruitment
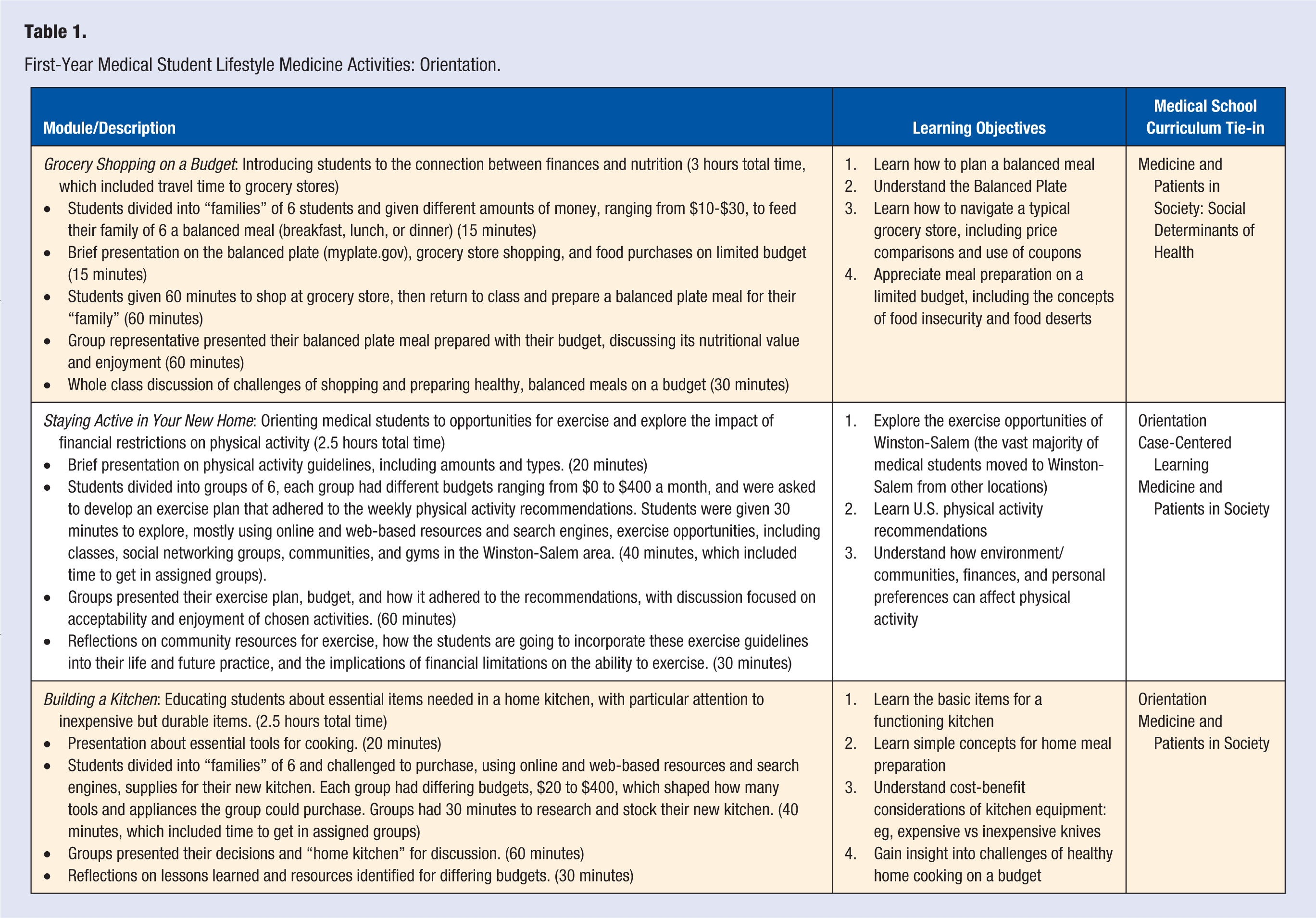
Medical education leaders asked that all 120 incoming medical students receive some exposure to the first 3 activities during orientation (Table 1). After the first 3 modules, a survey was sent to all students providing information on the year-long pilot, with brief questions assessing their interest in participating and availability to attend all classes. The student leaders and faculty advisor selected respondents who were willing to commit to the full year of classes; expressed interest in the topics of nutrition and exercise; did not express adherence to or support of fad or non–evidence-based diets; and did not express explicit weight bias. Program leaders sought to include students with varied backgrounds, diverse interests, and different experiences in wellness. From a group of 26 applications, 16 students were selected to participate.
First-Year Medical Student Lifestyle Medicine Activities: Orientation.
Lifestyle Medicine Program
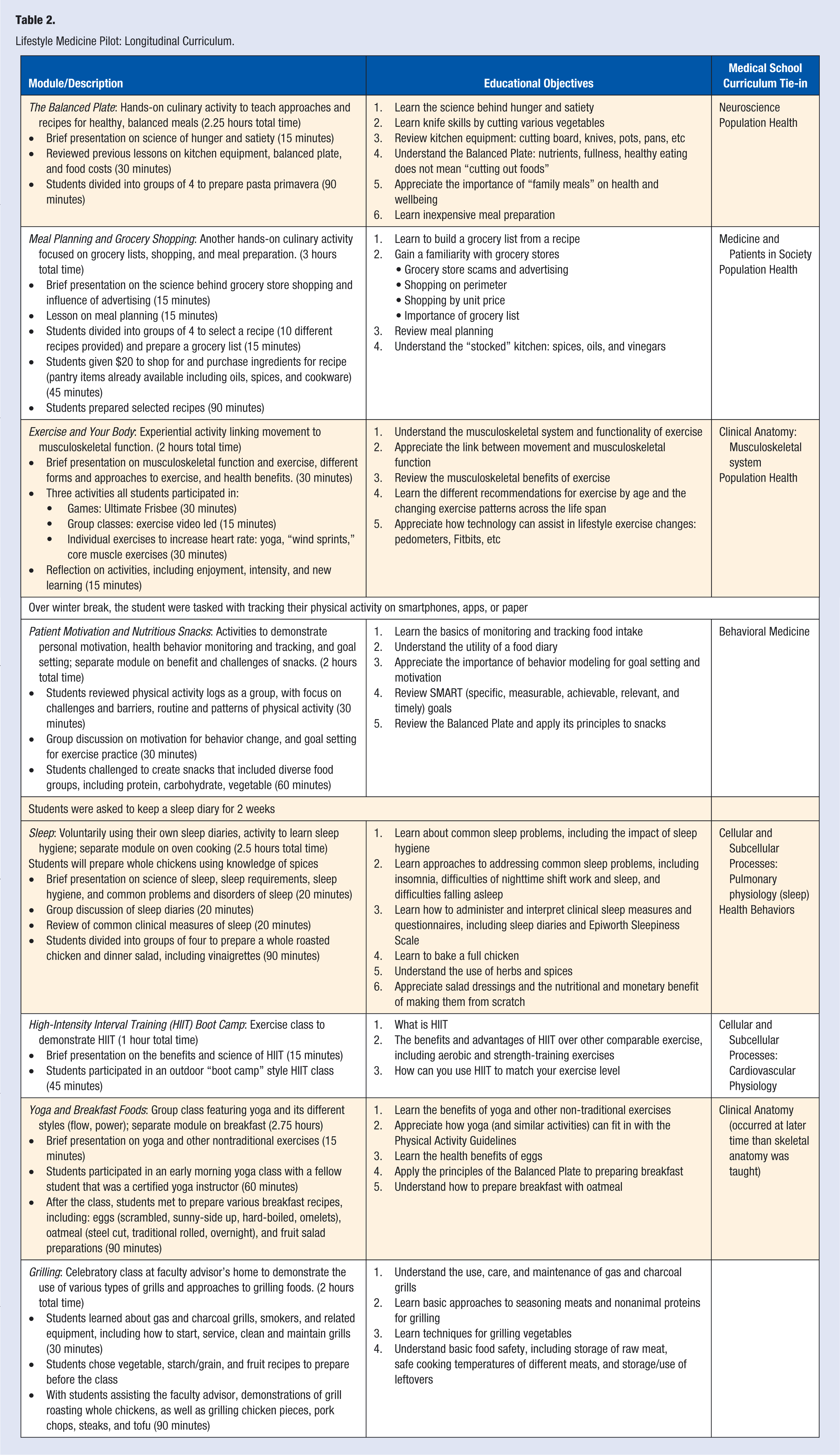
Student leaders and faculty advisor jointly developed educational topics, experiential activities, and learning objectives. Modules 1 to 3 were conducted with the entire first-year medical school class (Table 1) during the month-long orientation. Limited funds for implementation drove the decision to test the rest of the curriculum in a smaller group of students; this also maximized hands-on participation. The longitudinal curriculum for the pilot group of 16 students, Modules 4 to 11, was begun in the third month, with sessions typically held on weekday evenings; a few were held on weekend mornings (Table 2).
Lifestyle Medicine Pilot: Longitudinal Curriculum.
Student Experience and Feedback
This pilot program was not formally evaluated, as the focus was on development and implementation. Through existing evaluation mechanisms, students provided some anonymous feedback on the curriculum. In general, comments were positive, with participants feeling the sessions were informative and helpful, and hoped to incorporate into their daily lives. The introductory 3 sessions were well received and repeated in subsequent years, with Grocery Shopping on a Budget being the favorite. The experiential nature of the learning, particularly cooking activities and those that provided a patient-level experience, and a focus on health habits were the favorite aspects of the program. Many commented that they enjoyed activities and spending time with their peers outside of the medical classroom. Overall, the curriculum was well received with students desiring to continue activities beyond the first year.
Lessons Learned
Schedules
As seen in similar programs,9,10 the main challenge was negotiating student schedules and testing cycles, including those of the student leaders, who had different testing and class schedules than the first-year participants.
Student Expectations
A few students wanted activities to be more focused on patient education and counseling, as they were very confident in their own wellness. Students also had different expectations depending on their interests: Students with more interest in exercise (and less in cooking) requested more modules on physical activity; others were less comfortable in group exercise sessions and wanted more cooking lessons.
Capacity
Curriculum was limited to 16 students due to space, time, and funding. Many others in the first-year class (and even in the second-year class) wanted to participate in the pilot. This was a challenge, as the experiential nature of the pilot was a key component but limited our ability to scale up the program.
Experiential Activities
Students enjoyed the hands-on learning activities. They particularly enjoyed being able to cook their food and eating the meal as a reward. Eating meals cooked in the module was helpful in incorporating classes into student schedules. The feedback was so positive, additional experiential activities were included in later sessions, such as sleep (Table 2), where students completed sleep diaries and sleep disorder measures. This learning is supported by the literature; for example, Dacey et al 8 conducted a systematic review of physical activity counseling education in medical schools, finding that experiential activities and focusing on personal physical activity behaviors had the best student results.
Group Activities
Engaging a small group with shared interest in learning more about health and wellness allowed students to connect with peers and create community. Small group activities also allowed students to engage with others whom they might otherwise not meet.
Linking to Medical School Curricula
The most successful linkage with the formal curriculum was the exercise physiology module. A conscious effort was made to schedule this activity while students were learning about upper and lower extremities during anatomy. Students noted a deeper understanding of exercises performed because of the concomitant anatomy lessons and laboratories. This was also true for the sleep module, which occurred a few weeks after the neurology lectures.
Community Engagement
Seven of the 16 participants began volunteering in community-based wellness classes, particularly in the Brenner FIT program, which regularly holds physical activity and cooking classes in the community. Four of the 16 students trained to become lead-teachers in the programs.
From this pilot group, other activities developed,
A student developed a summer cooking camp at a local YMCA. The following summer, 2 student participants designed and implemented a summer research project to evaluate the summer camp.
A student is actively developing a new culinary program for first-year medical students.
Three students applied for and obtained funding to expand culinary activities as a student wellness initiative.
Student involvement in community wellness activities was not originally anticipated to arise from this pilot but was a welcome result. At Wake Forest School of Medicine, service-learning is highly valued, which is a certificate-granting component of medical education. At other institutions, such as Tulane, the Culinary Medicine program features volunteerism and service learning as key components of their initiatives. 13 Lifestyle medicine curricula could serve as a way to increase community engagement of medical schools and students.
Overall, students were actively engaged in all sessions, and were enthusiastic learners. Students became very comfortable with each other and provided motivation when trying something challenging, such as attempting high-intensity interval training.
Limitations
This pilot program was not formally evaluated, so more quantitative outcomes could not be assessed, nor did our sample size of 16 participants produce enough data for a qualitative analysis. This substantially limits the interpretation and generalizability of the pilot program, though the process in which it was developed and instituted can be beneficial to others considering such a program.
Next Steps and Future Plans
Students generally enjoyed the pilot program, which was feasible to implement in an already rigorous first-year medical school curriculum. However, quantitative measures are still needed for specific learning outcomes. These would include knowledge gained, impact on personal health behaviors and health parameters, and influence on student well-being as assessed by burnout, stress, and overall quality of life. Patient education and clinical care delivery would need to be included in future iterations as well. These skills could be added to the existing Introduction to Clinical Skills course or incorporated into clinical rotations in the third and fourth year of school. Also unknown is the curriculum’s impact on later medical practice, including self-efficacy and effectiveness on nutrition, exercise, and sleep counseling, as has been tracked in culinary medicine programs. 14 There is evidence in young children that physical activity can improve education outcomes, 15 which could also occur in medical students. Finally, although more funding was obtained to continue the pilot and train additional student leaders, a larger budget is required for an entire class of medical students to participate.
Student leaders discussed several approaches to addressing challenges. They suggested that students in the group should be responsible for coordinating class scheduling. Given the social nature of the sessions, scheduling them for Friday afternoons (when there are fewer classes) might be optimal, but they would need to end before students might travel for the weekend. There are plans to incorporate more direct teaching on patient education and counseling approaches, and to split pilots into separate exercise and nutrition programs to allow for student preference. To increase capacity, some modules may be combined so the pilot can be offered twice a year. One change already implemented was creating a separate volunteer training program for students, and training for students to instruct cooking classes in the community. This changed helped accommodate the increasing numbers of student volunteers. Student and faculty leaders are considering various avenues for future funding, such as the medical school leadership, local philanthropic groups, food companies, and fund-raisers.
Culinary medicine is firmly established at many medical schools,13,14,16,17 and many schools are broadening beyond nutrition and cooking to lifestyle medicine.9,10,18 Students should be aware of funding and awards to implement programs at their local schools. For example, the Donald A. Pegg Award was established to provide allied health students with funds to support student-led lifestyle medicine interest groups. 19 Established in 2016, this scholarship provides 4 students a year with the means to grow lifestyle medicine activities at their schools, and an opportunity to attend the annual American College of Lifestyle Medicine conference.
In summary, a student-led lifestyle curriculum was successfully implemented in a small group of first-year medical students. Experiential activities were well-received, engaged the medical school curriculum outside the classroom, and connected students with other community-based opportunities to share their knowledge. Challenges of implementation included how to fit sessions within a rigorous medical school curriculum and students’ other life events. Students increased their participation in service learning projects focused on health and nutrition. There has been sustained involvement by students in volunteering, with several students leading subsequent years of the pilot. This report and our experience could serve as a guide to students, educators, and professional schools looking to institute lifestyle medicine curriculums.
Footnotes
Acknowledgements
The authors thank Karen Klein (in the Wake Forest Clinical and Translational Science Institute (UL1 TR001420; PI: McClain) for editing the manuscript; they would also like to thank the Wake Forest School of Medicine for support of the pilot program.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.