
Abstract
Interprofessional care improves outcomes for medically complex patients and may be a valuable addition to standard lifestyle medicine practice, but implementation barriers exist. The purpose of this study was to explore the key features, perceived impact, and implementation considerations related to holding interprofessional team meetings as part of an intensive lifestyle medicine program. In this mixed-methods study, focus groups were conducted with 15 lifestyle medicine clinicians from various healthcare disciplines who had participated in interprofessional team meetings. Quantitative descriptive statistics of the meeting minutes were also calculated. Clinician-perceived benefits from participating in interprofessional team meetings included increased acquisition of knowledge, access to other clinicians, collaborative decision-making, patient satisfaction, and achievement of patient-centered goals. Participants described the importance of preparing an agenda for the interprofessional team meetings in advance, but a major implementation challenge was the time required to prepare for and conduct the meetings. Commitment and financial support by organization and program leadership were reported as key facilitators to implementing the meetings. Clinicians perceive significant value from incorporation of interprofessional team meetings into an intensive lifestyle medicine program, but successful implementation of meetings requires investment from all levels within a healthcare system.
Keywords
“Lifestyle medicine care team members who participate in interprofessional team meetings view the meetings as invaluable to their medical practice and to the treatment of their patients.”
Introduction
Lifestyle medicine is a holistic approach to treat, prevent, and reverse lifestyle related chronic disease. It uses interventions that cross multiple health domains including nutrition, exercise medicine, sleep medicine, smoking cessation, and mental health.1,2 Nevertheless, lifestyle medicine clinicians often practice in isolation as solo practitioners,3,4 and when lifestyle related intervention is delivered by multiple clinicians to a single patient, communication and coordination of services across the disciplines is difficult. To address this challenge, some lifestyle medicine clinicians use a multidisciplinary approach in which they harness a strong referral network of clinicians in other disciplines to facilitate patients in making a lifestyle change.4-6 However, in this multidisciplinary care model, clinicians still draw on their own discipline-specific expertise and essentially “stay within their boundaries.” 7
In contrast, interdisciplinary care is a model in which clinicians “analyze, synthesize, and harmonize links between disciplines into a coordinated and coherent whole.” 7 In the interdisciplinary model, care provided by each clinician is influenced by collaboration with the other clinicians in the group. Collaboration typically occurs via regularly scheduled team meetings and communication between meetings. Interdisciplinary care is standard practice in many medical specialties which routinely manage patients with complex needs. Examples include cancer care, organ transplant medicine, cardiac rehab, and inpatient rehabilitation.8-13 When compared to single provider or multidisciplinary models, interdisciplinary care has resulted in improved clinical outcomes, especially for patients with conditions such as heart disease and diabetes in which patient engagement and sustained behavior change are essential to disease management.14-18 Other documented benefits of interdisciplinary team-based care include: enhanced clinician expertise across all relevant treatment domains due to transdisciplinary education among clinicians, improved understanding of patients’ needs, consistent messaging from the clinician team to patients, greater patient access to resources which can facilitate sustained behavior change, and improved patient satisfaction with care.14,18-24
Given the complexity and multimorbidity of patients who benefit from lifestyle medicine care, interprofessional team meetings could be a valuable component to standard practice for lifestyle medicine clinicians from various clinical disciplines who collaboratively treat patients in an intensive program approach. However, logistical time-related and financial barriers to implementation of interprofessional team meetings exist,25-27 and there is an evidence gap regarding the impact of interprofessional care specifically in the lifestyle medicine setting. The overall purpose of this study was to explore the perceived added value and implementation considerations regarding incorporation of interprofessional team meetings as part of an intensive lifestyle medicine program. Specifically, we aimed to investigate the key features, perceived impact, and considerations for replication of interprofessional team meetings in an intensive lifestyle medicine program setting from the perspective of lifestyle medicine clinicians across multiple healthcare disciplines.
Methods
This was a mixed-methods study which involved focus groups and collection of descriptive quantitative data. The study was conducted according to the World Medical Association Declaration of Helsinki. Washington University Institutional Review Board approval was obtained, and participants provided verbal consent prior to participating in the focus groups (IRB number 202105008). The study reporting follows the Standards for Reporting Qualitative Research (SRQR) guidelines. The focus groups were conducted in June 2021. Quantitative data were collected from June 2021 through January 2022.
Lifestyle Medicine Program
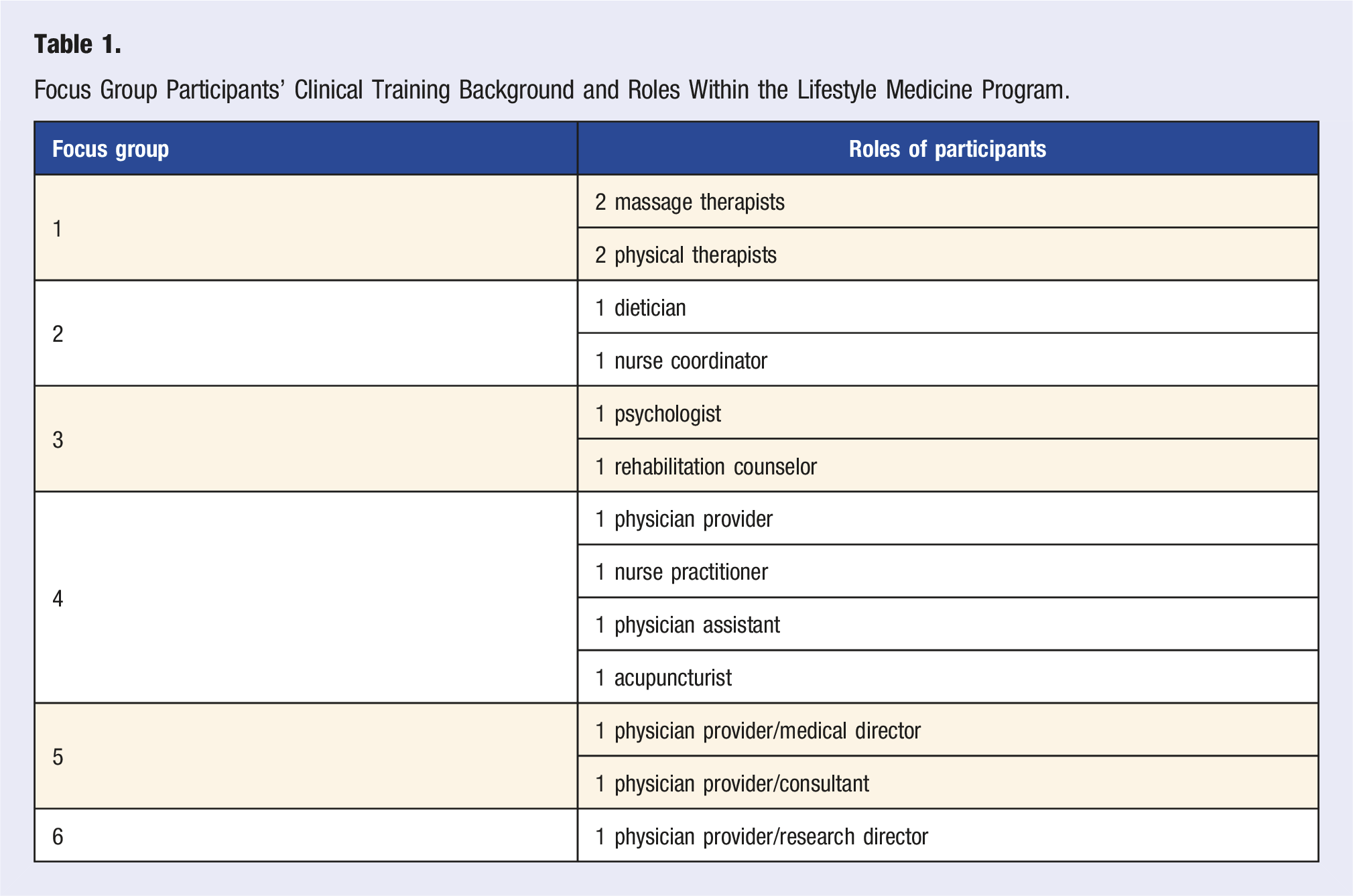
Data collected for this study were obtained from a single lifestyle medicine program. The program has previously been described. 28 In brief, the program was established in June 2020 and is housed within the Orthopaedic Surgery department of a tertiary care academic institution in the United States. Patients self-refer or are referred to the program if they have functional impairments and coexisting metabolic and/or psychological comorbidities. At the patient intake evaluation, a patient-centered functional goal is identified. Example goals include losing a predetermined amount of weight to minimize obesity-related perioperative risk during joint replacement surgery, improving walking tolerance to resume daily walks in the park with a loved one, and/or weaning off opioid medications by reducing pain and learning self-management skills. Patients’ self-selected functional goals are used as their primary motivators for behavior change during and after participation in the program. The intensive lifestyle medicine program is designed to be a 90–120 day experience. Program providers include physical medicine and rehabilitation physicians (physiatrists), a physician assistant (who provides sleep hygiene counseling), a nurse practitioner (who provides smoking cessation counseling), a dietician, a psychologist, a rehabilitation counselor, physical therapists, an acupuncturist, massage therapists, and a nurse coordinator.
All patients complete an initial evaluation with a physician, the physician assistant, or the nurse practitioner. A comprehensive history is obtained which includes patients’ medical histories, current physical and mental health symptoms, and readiness, motivators, and barriers to change. Patients are determined to be appropriate for the intensive lifestyle medicine program if they have a functional goal, coexisting metabolic and/or psychological comorbidities which can be addressed with 2 or more of the disciplines offered by the program, and are interested in making lifestyle changes. All patients who are enrolled in the intensive program are added to a participant list which is reviewed at regularly scheduled interprofessional team meetings by the program clinicians. These meetings had been occurring for 2.5 years prior to conduct of the focus groups for this study.
Participants and Recruitment
Participants for the focus groups were identified by the lifestyle medicine program’s leadership team and were considered eligible for participation if the individual (1) provides care and/or supports program activities, and (2) has participated in the interprofessional team meetings. Eligible participants were invited to voluntarily participate in one focus group with other individuals with similar roles or areas of specialization. Participant recruitment was initiated by the lifestyle medicine program’s leadership team, who sent an email to all eligible participants, explained the goal of the focus group sessions, and described the collaboration between the leadership team and the trained qualitative research team. A second email from the research team was sent to confirm interest in participation and identify availability for participation.
Semi-Structured Focus Groups
Qualitative data were collected using guided focus groups. The semi-structured focus group guide was developed in collaboration between trained qualitative researchers and the leadership team of the lifestyle medicine program (Supplement Appendix 1). The guide included questions related to the evaluation question, “What is the value-add of interprofessional meetings among clinical team members of a lifestyle medicine program?” Participants were asked about key ingredients of the interprofessional team meeting process; barriers and facilitators to participating in the interprofessional team meetings/approach; the perceived impact of the interprofessional team meeting on clinicians’ practice, patient outcomes, and engagement with community partners; and key ingredients which would be needed to replicate the model. The focus groups were conducted and recorded via secure, encrypted audio/video conferencing technology (Zoom HIPAA), each lasting approximately 45-60 minutes. Sessions were led by either one or two trained qualitative researchers (EMS and MWR), with a lead facilitator and a note taker when possible.
Qualitative Data Analysis
De-identified audio transcripts were professionally transcribed (Rev.com), and the transcripts were formatted and checked for accuracy by one study team member (EMS, MWR). Transcripts were coded using a directed thematic content analysis approach by two study team members independently (EMS, MWR) using computer-assisted software (NVivo 12.0). A directed thematic content codebook was developed, and the codebook was tested using two transcripts across multiple coders to ensure the dyad achieved inter-rater reliability kappa of >.8 and came to consensus of any changes to the codebook before proceeding with individually coding the remaining transcripts. Working in pairs, the research team identified themes from node reports. A directed analysis of the qualitative data was conducted to produce theme reports. Theme aggregation and refinement was conducted using an iterative process.
Quantitative Data Collection and Analysis
To provide added context regarding the key features of the interprofessional team meetings, meeting minutes were recorded for 7 months. Variables recorded included the total meeting duration and the amount of time spent discussing: newly enrolled patients, patients who had achieved their functional goals (i.e., ready for “graduation”), patients who had developed challenges to meeting their goals, all other patients enrolled in the program, and administrative topics. During one meeting, the number and type of management changes that were made during the meeting were also documented. Raw data and univariate descriptive statistics are reported for these variables.
Results
Focus Group Participants’ Clinical Training Background and Roles Within the Lifestyle Medicine Program.
Key Features of the Interprofessional Team Meetings
The lifestyle medicine program leadership attributed the idea of conducting interprofessional team meetings to their prior experience in physical medicine and rehabilitation (PM&R) residency training during which they worked in an acute inpatient rehabilitation setting where interprofessional team meetings between physicians, physical therapists, occupational therapists, speech therapists, psychologists, and social workers is standard practice. Implementation of the meetings was then adapted to fit an exclusively outpatient care setting.
Preparation for the Meetings
Preparation for each meeting is supported by a nurse coordinator who coordinates and schedules meeting times and ensures that patient data and changes to patients’ care plans are compiled and shared with team members and staff in advance. This preparation by the nurse coordinator can take up to a full day for each meeting. Other care team members also spend 15–30 minutes prior to each meeting to review the compiled patient information that will be discussed. This preparation is seen as critical to ensuring that the interprofessional team meetings run smoothly and efficiently.
Logistics of the Meetings
Meetings occur monthly in the late afternoon immediately after typical billing hours, usually from 4:15pm–5:15pm on a Tuesday. Attending members include the medical director, other physician providers, physician assistant, nurse practitioner, dietician, psychologist, rehabilitation counselor, physical therapists, acupuncturist, massage therapists, nurse coordinator, and patient intake specialists. The meetings are facilitated by a clinical leader, and the team works through a predetermined agenda in a systematic approach. As the overall number of patients in the intensive lifestyle medicine program has increased over time, the focus of the meetings has evolved from discussing all patients per meeting to using established criteria to focus discussion on a subset of patients (e.g., patients new to the program, patients nearing program graduation, patients encountering challenges or barriers to progress). With this new approach, an average of 16 patients are discussed each meeting (Table 2). “We used to try and plow through everybody, and it got to be ‘quantity over quality.’ And now… we kind of drill down more on, okay, ‘Who are the patients that we think we need to talk about?’ Anybody can bring up any patient if they want, but we're not covering every patient every time. And that has improved the quality of the discussions. It still goes on for an hour.” Summary of Meeting Minutes for Seven Representative Monthly Interprofessional Team Meetings.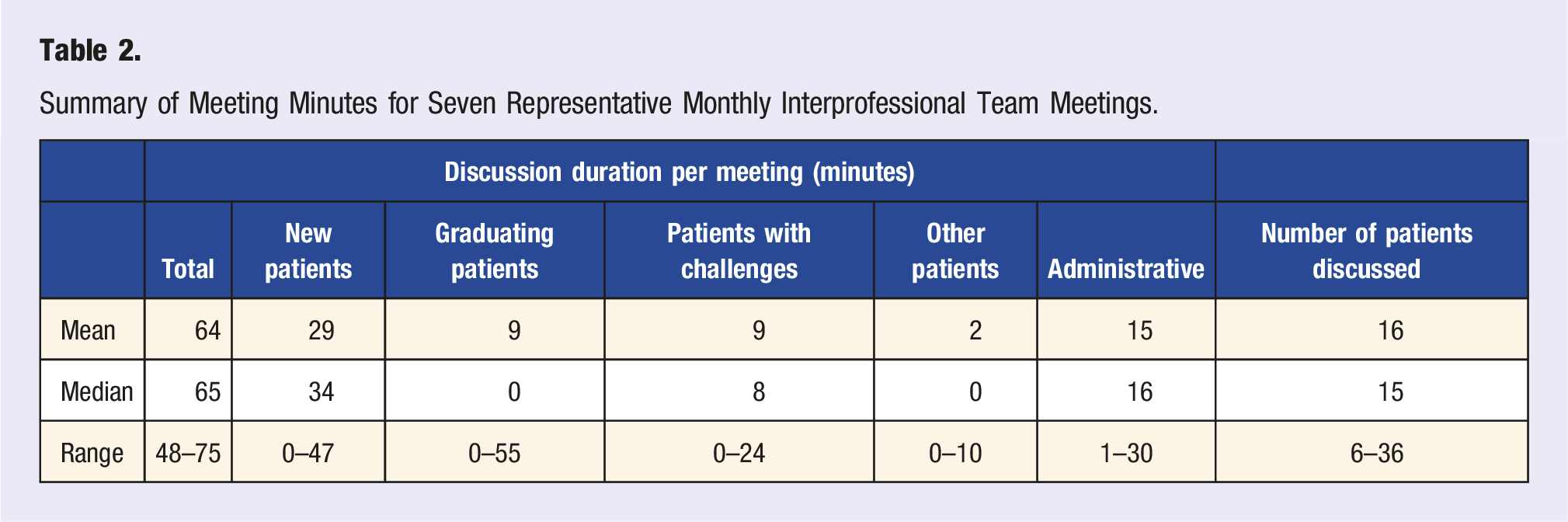
Content Discussed during the Meetings
Topics discussed are contingent upon each patient’s unique issues, and care team members discuss patients from the perspective of their healthcare specialty. As relevant, the team discusses the patient’s motivating factors for obtaining care through the intensive lifestyle medicine program, the patient’s goals and barriers to treatment during the intensive program, the patient’s behaviors thought to be important in sustaining self-care and management, the patient’s successes and challenges with treatment from each specialist’s perspective, and recommendations for changes to the patient’s care plan. The goal is for the group to come to a consensus regarding each patient’s key challenges to meeting predetermined goals and then to identify whether modifications to the care plan are needed.
Despite the predetermined structure of the meeting, conversations about patients are dynamic, and the content of meetings varies each month (Table 2, Figure 1). Overall, over the course of 7 months, increasing emphasis was placed on discussing patients who are approaching graduation from the program to ensure they are equipped with self-management tools and follow-up materials in case of a relapse in lifestyle habits. Occasionally, educational content is shared at the meetings that is not patient-specific. “It's systematic…it starts with the patient, but if the issue comes up about their weight, then nutrition comes in next. If the issue comes up about their being deconditioned, you might hear from the physical therapist next…it's somewhat dynamic, but it's also structured.” “Each discipline gives their two cents, and then we decide if we're going to make any changes to their care plan, whether they’re ready to graduate at the next session, whether we need to get their labs…‘Let's add a medicine, let's add a service.’…And then…periodically we have educational content at the meeting. So we've had each discipline present 10 minutes of what they do, and have a bit of a discussion so that everybody understands each other.” Distribution of meeting minutes for each of seven representative interprofessional team meetings. (For Meeting 4, a referring provider was invited to the meeting, and the majority of time was spent discussing that provider’s patients in the program).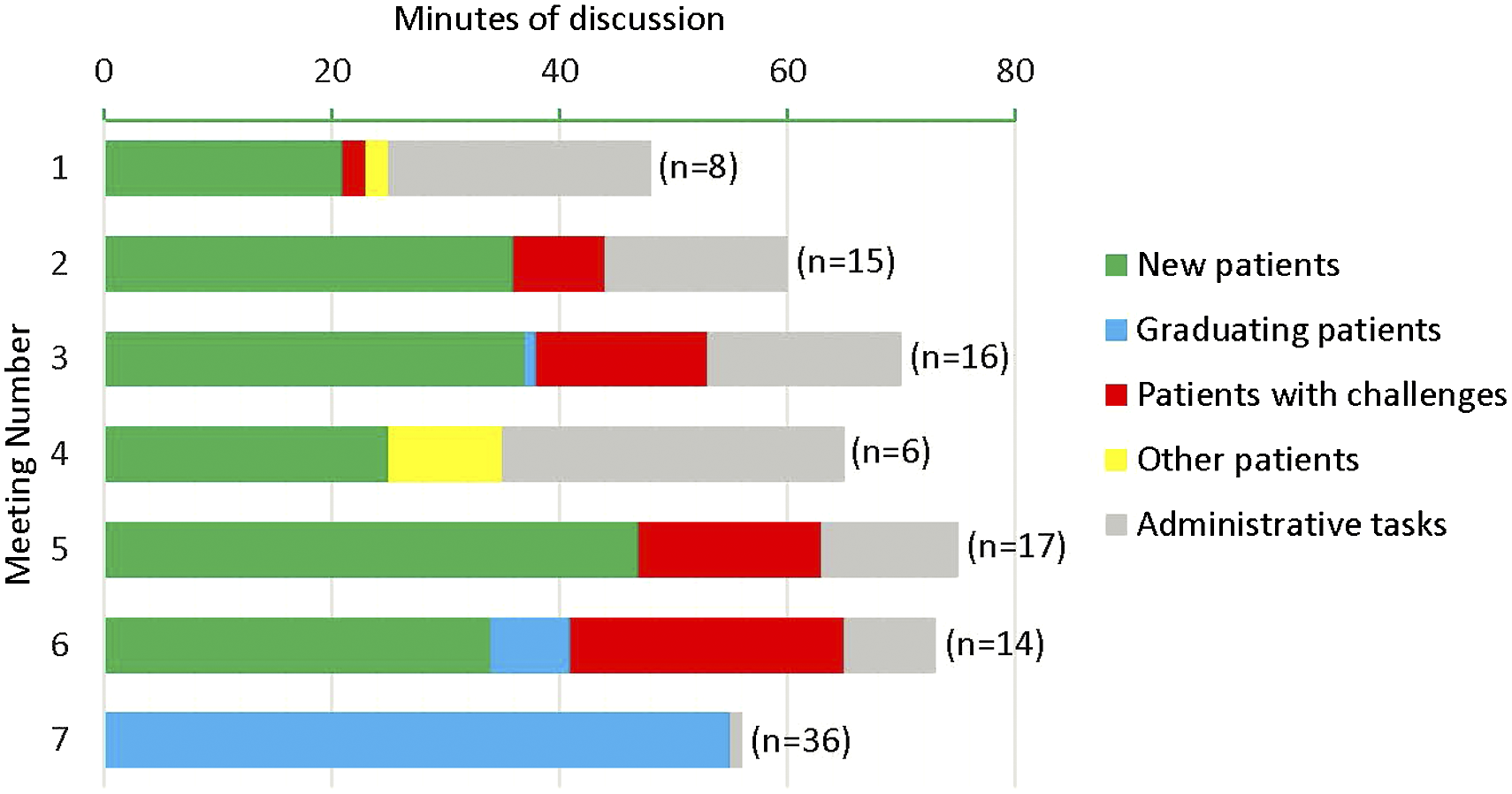
As an example of changes to patients’ care plans that result from the meetings, the following group decisions were made during Meeting 2 (Figure 1): a treatment discipline within the lifestyle medicine program was added, removed, or re-visited (n = 6 patients); after discussion with the patient, referral to a service outside the lifestyle medicine program was made (i.e., cognitive assessment, referral for bariatric surgery evaluation) (n = 2); increased guidance on a self-directed exercise program was provided (n = 1); and the team’s motivational approach for a patient was revised because a team member identified a new motivator for change (n = 1).
Perceived Impact of Interprofessional Team Meetings
Participating care team members described a positive impact of the interprofessional team meetings that were perceived to benefit the practice as a whole and also directly to patient care.
Perceived Benefits to Practice
Perceived Impact of Interprofessional Team Meetings: Representative Quotes Organized by Themes and Subthemes.
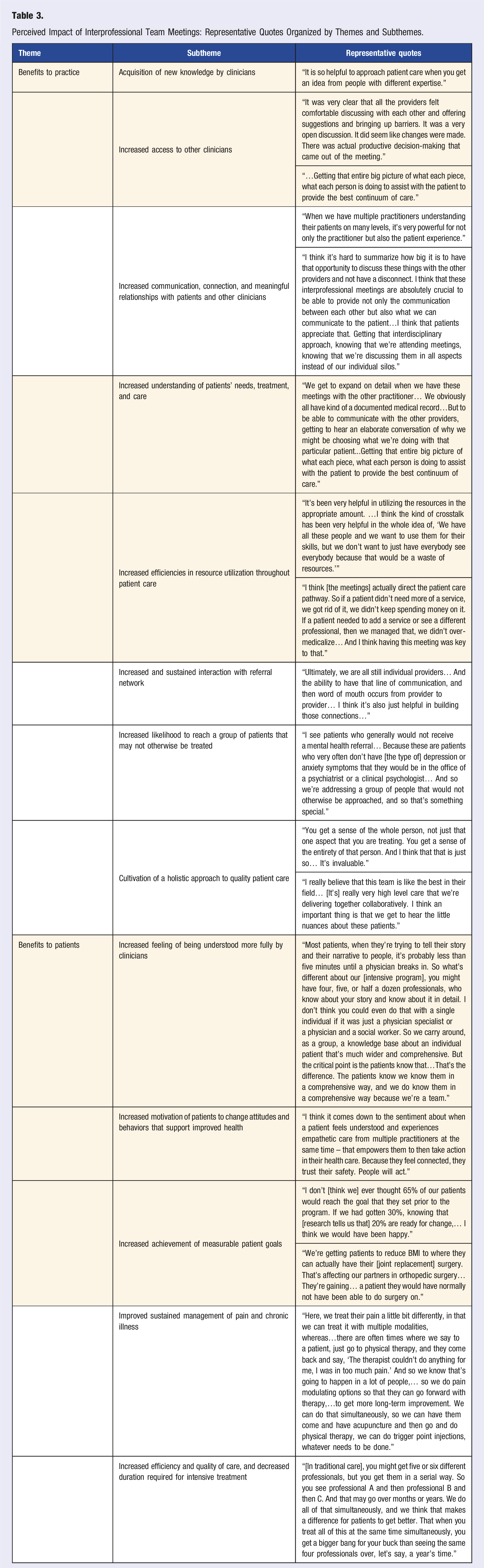
Perceived Benefits to Patients
Care team members also described several perceived benefits to the patient experience, patients’ clinical outcomes, and patients’ cost of care due to clinician participation in the interprofessional team meetings (Table 3).
Considerations for Replication of Interprofessional Team Meetings in Lifestyle Medicine Care Settings
Care team members shared common ideas about the key factors needed to replicate the interprofessional team meeting approach within other lifestyle medicine programs. First and foremost, the participants reported that implementation of these meetings requires a team of committed, passionate professionals with clear roles and responsibilities. Additionally, several specific implementation barriers were described, as well as facilitators which have been useful to overcome some of the barriers.
Barriers to Implementation
Considerations for Replication of Interprofessional Team Meetings: Representative Quotes Organized by Themes and Subthemes.
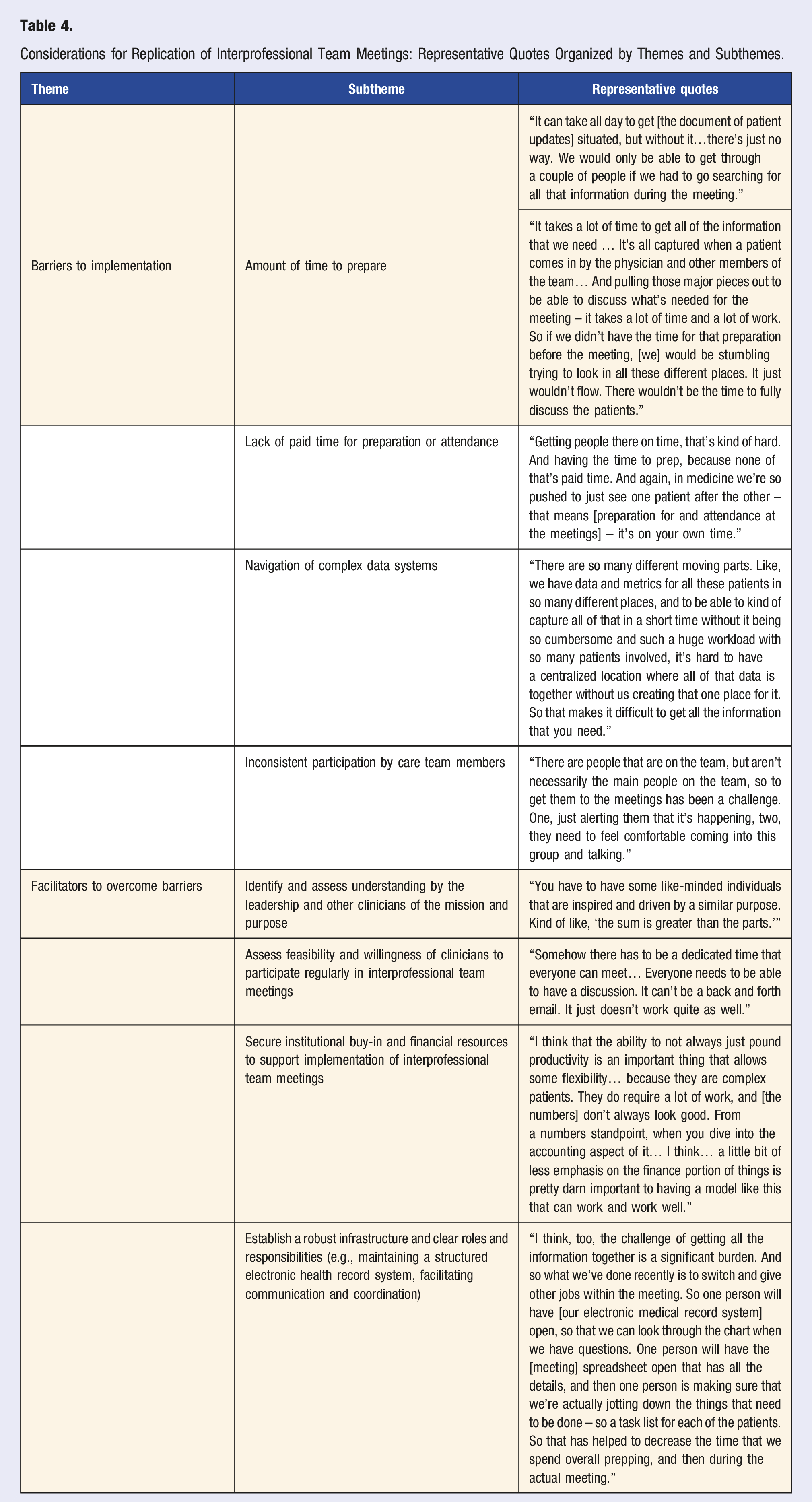
Facilitators to Overcome Implementation Barriers
Several strategies were identified that contribute to overcoming the identified implementation barriers. On a high level, care team members reported that the importance of the interprofessional team meetings must be understood and supported at all levels within the healthcare organization (Table 4). More specifically, the following practical strategies were suggested: • Secure dedicated administrative support (e.g., paid time for care team members to prepare for and participate in the interprofessional team meetings) • Increase the frequency of interprofessional team meetings to bi-monthly (to better respond to dynamic, relevant patient challenges and to mitigate some of the challenges with preparation for the meetings) • Streamline data management processes to increase efficiency of meeting preparation • Hold at least some meetings in person (rather than virtual) to increase engagement and a sense of team camaraderie
Discussion
In this study, we explored the added value and implementation considerations regarding incorporation of interprofessional team meetings as part of an intensive lifestyle medicine program. We found that clinicians use these meetings as a dedicated time and space to leverage the care team’s collective expertise in a coordinated manner to develop holistic plans for patients. They perceive that attending the meetings increases their own clinical knowledge base and helps them reach more patients in need, deliver more patient-centered care, reduce patient use of unnecessary healthcare resources, and improve patient outcomes. Successful implementation of these meetings requires investment from all levels within a healthcare organization.
Our study findings are aligned with prior investigation into interprofessional team meetings in non-lifestyle medicine settings. Prior investigation into the topic has documented key barriers to implementation related to staff availability and protected time, in addition to key benefits such as improved inter-provider management of each patient’s unique needs, development of more realistic and relevant patient goals, and improved patient outcomes.21,29,30 Our identified strategies to overcome implementation barriers (i.e., robust infrastructure and strong institutional and leadership buy-in to facilitate protected time and access to resources) similarly overlap with prior investigations.21,29,30
Implications
In lifestyle medicine, we know that sustainable financial compensation models are essential to the growth of the field.4,31 Building from our understanding of the value of team meetings, we advocate that interprofessional team meetings should become a standard component of intensive lifestyle medicine programming and should be counted as billable work hours which contribute to lifestyle medicine related patient care. Reimbursement codes already exist for interprofessional team meetings between primary care providers and psychiatric consultants (i.e., 99492, 99493, 99494, and G2214 CoCM), 32 and application of these or similar codes to cover interprofessional team meetings in the lifestyle medicine setting would be a natural extension of the nationwide push toward a collaborative care treatment model for complex patients. Of note, Medicare reimburses for existing collaborative codes, but some state Medicaid programs and commercial insurers have lagged behind. 32 Alternatively, participation in a value-based care payment model such as Primary Care First could be a streamlined approach to ensure lifestyle medicine clinicians can appropriately prioritize interprofessional care. 33
Strengths, Limitations, and Next Steps
To our knowledge, this is the first description of a truly interprofessional team meeting as a core element of an intensive lifestyle medicine program. Our findings provide (1) guidance related to optimizing patient-centered, goal-directed care for other lifestyle medicine programs, and (2) preliminary support for motivation for third party payers to support a compensation model for providers’ time and effort related to interprofessional team meetings in the lifestyle medicine setting. This study also has limitations. First, this was a single-center study of a unique healthcare model and, thus, the findings may have limited generalizability across different settings. For instance, as evidenced by the evolution of the meeting structure described by this study’s care team members as their program grew and matured, intensive lifestyle medicine programs of various sizes may require adaptations to optimize meeting logistics. Second, patient perspectives and quantitative data regarding the impact of interprofessional team meetings on patients’ clinical outcomes was not obtained in this current study. Future work should capture patients’ perceived and measurable value of including interprofessional team meetings as part of a lifestyle medicine care program. The impact of participation in interprofessional team meetings on provider satisfaction could be examined, as well.
Conclusion
Lifestyle medicine care team members who participate in interprofessional team meetings view the meetings as invaluable to their medical practice and to the treatment of their patients. Key benefits of the interprofessional team meetings include improved collaboration and interprofessional learning, improved communication about patient care plans, and increased patient motivation due to a sense of connectedness with the care team. We advocate for increased incorporation of these meetings into intensive lifestyle medicine programs, and we present strategies to facilitate their implementation. The primary systematic barrier to implementation of these meetings is financial support, which can be addressed by investment from program leadership, healthcare organizations, and third party payers. Additional work is needed to assess patients’ perceived value and measurable impact on clinical outcomes as a result of including interprofessional team meetings as part of a lifestyle medicine care program.
Supplemental Material
Supplemental Material - Provider-Perceived Value of Interprofessional Team Meetings as a Core Element of a Lifestyle Medicine Program: A Mixed-Methods Analysis of One Center’s Experience
Supplemental Material for Provider-Perceived Value of Interprofessional Team Meetings as a Core Element of a Lifestyle Medicine Program: A Mixed-Methods Analysis of One Center’s Experience by Abby L. Cheng, Elsa M. Snider, Heidi Prather, Nikole L. Dougherty, Myisha Wilcher-Roberts, and Devyani M. Hunt in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
The authors thank the Washington University Living Well Center clinical team for facilitating conduct of this study. We also thank Adriana Martin for her assistance with manuscript preparation and submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was supported by the National Institute of Arthritis and Musculoskeletal and Skin (K23AR074520); Doris Duke Fund to Retain Clinical Scientists; and Jacqueline N. Baker Washington University Living Well Center Baker Fund.
Data Availability Statement
The full qualitative datasets generated during the current study are not publicly available because it would risk anonymity of the participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.