
Abstract
Recently, lifestyle medicine (LSM) application has shown feasibility for musculoskeletal pain patients with co-existing lifestyle-related chronic diseases. This study describes early results of a LSM program for musculoskeletal patients with goals to optimize health prior to orthopedic surgery. Fifty-four patients (age: 61 ± 11 years; 39 [72%] females) completed the program from 3/8/22-12/1/23. Data included patient goals, utilization, goal attainment, and patient outcomes. Most patients (41/54 [76%]) enrolled with established surgical dates. Mean BMI was 43.2 ± 5.3 kg/m2, and 89% had ≥2 lifestyle-related chronic diseases. The majority reported impaired sleep (79%) and zero cumulative minutes of physical activity/week (57%). Mean program duration was 13 ± 8 weeks involving 5 ± 4 visits with members of the interprofessional team. Fifty-two (96%) patients successfully attained pre-program goals, and 49/54 (91%) met their surgical goal. Of the patients enrolled without surgical dates, 11/13 (85%) optimized their health and proceeded to surgery. Forty-two (78%) patients reported decreases in weight and BMI, averaging 11 ± 7 lbs and 1.8 ± 1.3 kg/m2, respectively. Rates of improvement in pain, PROMIS-10 physical and mental health, and PHQ-4 were 52%, 37%, 45%, and 47%, respectively. These data demonstrate the feasibility and effectiveness of a LSM program to address whole-person health optimization and enable orthopedic patients to improve lifestyle behaviors and proceed to orthopedic surgery.
Introduction
Lifestyle behaviors and lifestyle-related chronic disease impact the risks and outcomes of orthopedic surgery. Recommendations regarding necessary health optimization for modifiable risk factors in several domains prior to total knee arthroplasty (TKA) and total hip arthroplasty (THA) include morbid obesity, malnutrition, type 2 diabetes, smoking, opioid use, poor dentition, cardiovascular disease, preoperative anemia, staphylococcus colonization, and psychological disorders. 1 The presence of any one or combination of these health conditions has been linked to longer length of hospital stay, increased complications, higher early surgical revision rates, and increased re-admissions.2-9 A protocol to evaluate preoperative risk factors and delay surgery until risks are modified has been shown to shorten hospital length of stay and lower direct costs following total joint arthroplasty. 10 A lifestyle medicine (LSM) program utilizing the 6 pillars of health simultaneously has been shown to be feasible for patients with painful musculoskeletal conditions. 11 An investigation into the benefit of using the 6 pillars of health in a comprehensive program to help reduce risk of surgery and improve outcomes and health prior to an elective orthopedic surgery has not been reported.
Smoking and type 2 diabetes are independent risk factors for surgical site infections 12 that can increase morbidity, mortality, length of hospital stay, and health care costs.13,14 Kee and colleagues reported 40.4% of THA revision patients and 43.7% of TKA revision patients were found to have at least 1 modifiable risk factor, when the revision was performed within the 2 years following the primary surgery. 15 In addition to these complications, persistent pain is a concern that impacts surgical outcomes. The PAIN OUT quality improvement network utilized over 60 000 patient records to assess pain following orthopedic procedures. Despite an increased number of treatment interventions, U.S. patients reported more post-operative pain and chronic pain after TKA as compared to European patients. 16 A whole-food plant-predominant diet has been shown to reduce systemic inflammation. As this information becomes better recognized in the U.S. as a nutritional health choice that enables optimal health, we will likely learn better avenues to help manage osteoarthritis and care following joint arthroplasty in people with an elevated inflammatory state prior to and following surgery.
Understanding the implications of nutrition and pain will also be important. Sala-Climent et. al reported a correlation between an increase in anti-inflammatory food intake and improved sleep, stress, and pain in patients with chronic pain related to an inflammatory arthritis. 17 The bidirectional path between pain and poor sleep is important to recognize and treat. Sipila et al. reviewed these relationships and described how impaired sleep increases the risk of the onset of pain and exacerbation of existing pain. 18 This relationship can be profound in the post-operative period when patients can develop sleep impairments and experience severe pain. When perioperative pain is not managed, length of stay in the hospital can increase, recovery is delayed, patient satisfaction is reduced, and chronic pain can develop. 16 Collectively, managing systemic inflammation in the perioperative time period has the potential to decrease risks at the time of and following surgery, as well as to improve pain, sleep quality, and stress management. However, in a fee-for-service model of care in the U.S., it is difficult to deliver care to enhance health, as many services (e.g., dietitian, health coach) and access to mental health care are often not covered or have limited coverage by insurance companies. Access to providers in many regions can also be limited.
Whole-person health optimization happens when patients adopt lifestyle behaviors that are the foundational pillars for LSM. They include eating a whole-food plant-predominant diet, maintaining physical activity, practicing healthy sleep, managing stress, having positive social connections, avoiding tobacco, and limiting excessive alcohol use. 19 These lifestyle behaviors are among the many determinants of health defined by Healthy People 2020, which proposed 10-year evidence-based national objectives for improving health for all Americans. 20 Utilization of LSM to treat, prevent, and reverse lifestyle-related diseases has compelling and growing evidence of its benefits for these chronic diseases. Emerging data suggest the feasible and beneficial benefits of utilizing the application of LSM for patients with musculoskeletal conditions, 11 as lifestyle behaviors are linked to musculoskeletal conditions. In the U.S., 59% of people diagnosed with osteoarthritis also have metabolic syndrome. 21 These metabolic factors trigger the proinflammatory cascade leading to the onset of osteoarthritis, worsening joint damage, and exacerbating osteoarthritis symptoms.22-25 Hashem et al measured inflammatory markers in patients with chronic non-specific low back pain and compared them to patients with low back pain associated with a structural source of the pain. 26 Patients with chronic non-specific low back pain had higher inflammatory markers and reported greater physical inactivity. Another study assessing inflammation in patients with low back pain concluded that systemic inflammation may serve as a contributor to the relationship of mental health symptoms and pain intensity. 27 The application to LSM as a treatment plan is a natural next step, in that LSM aims to reduce systemic inflammation, the very factor that can contribute to the development and severity of a musculoskeletal condition.
The gap to bridge is how to implement LSM in a programmatic manner as part of the treatment pathway for patients with musculoskeletal conditions. Further, can a programmatic approach to health optimization utilizing LSM in the perioperative period for patients undergoing elective orthopedic surgery enable them to present to surgery with modified health risks? We have developed a LSM program for musculoskeletal patients with specific pathways based on the patient’s interest in the program and readiness to make lifestyle changes. For patients not interested in participating or ready to make a behavioral change, we provide a 1:1 meeting with a LSM provider (HP or KG) to review their health risks and provide education regarding the links between musculoskeletal health and the 6 pillars of LSM. For all other patients, we developed the intensive interprofessional LSM program to address lifestyle-related chronic disease and musculoskeletal conditions to enable patients to reach their health goals, utilizing the 6 pillars of health combined with usual musculoskeletal care. Our interprofessional LSM team includes a physiatrist and nurse practitioner (both Diplomats of the American Board of LSM), endocrinologist, dietitian, health coach, exercise physiologist, physical therapists, and smoking cessation advanced practice providers. Patients meet 1:1 and in group programming with providers simultaneously who were chosen based on the patient’s pre-program goals. A care navigator and scheduling specialist facilitate patient access and assist with problem solving through team communication. A monthly interprofessional team meeting is held to discuss patients’ progress and setbacks to enhance patient care and facilitate interprofessional communication and learning. A qualitative study has shown these interprofessional meetings to be valuable and improve provider satisfaction. 28 The purpose of this study is to describe the early outcomes of patients who completed an intensive LSM program prior to elective orthopedic surgery to optimize health prior to surgery.
Methods
Ethics and Patient Selection
This was a retrospective review of a prospectively collected LSM data repository approved by the Institutional Review Board at Hospital for Special Surgery. Adult patients over the age of 18 years with orthopedic musculoskeletal conditions who were electing to undergo orthopedic surgery to improve pain, function, and global health were referred to the interprofessional intensive LSM program prior to surgery. These patients were identified by their orthopedic surgeon as being at elevated risk for surgical complications and poor surgical outcome based on various lifestyle-related chronic diseases, including obesity, type 2 diabetes, hypertension, hyperlipidemia, cardiovascular disease, anxiety, and depression. Patients who were enrolled in the program from March 8, 2022, to November 1, 2023, were included. Patients who were in the program for non-surgical care, not interested in participating, or did not complete the program were excluded from this study.
Program Information
The intensive interprofessional LSM program is a patient-driven program for musculoskeletal patients with co-existing lifestyle-related chronic diseases at a single tertiary orthopedic medical center. Pre-surgical patients are referred to the program to optimize their health either (1) prior to a pre-program set date for elective orthopedic surgery or (2) to qualify for an orthopedic surgery they are unable to schedule. The inability to schedule a date for orthopedic surgery is due to the severity of their lifestyle-related chronic disease(s), as well as the risk that these chronic diseases pose at the time of surgery and post-operative period, which can lead to poor long-term outcomes following surgery.29-33 The patient care pathway in the program was developed based on the patient’s goals set at the time of the intake visit, which reviews the 6 pillars of health and records patient baseline data related to each pillar, including anthropometric, metabolic, pain, function, and mental health measures. To enhance patient activation in their care, a dedicated scheduler facilitates appointment scheduling, and a care navigator checks in with patients at regular time intervals throughout their time in the program to help with problem solving and communicating with team members to facilitate patient needs. The program can be delivered in-person or through virtual visits based on the patient’s choice.
Data Collection
All data were collected as standard of care in the electronic medical record system. Baseline data included age, sex, race, ethnicity, date of LSM program enrollment, presence of a surgical date at the time of enrollment, weight, BMI, lifestyle-related chronic diseases (number and type), musculoskeletal diagnosis, physical activity (cumulative minutes per week), sleep health (quality of sleep, number of hours of sleep per day, awakening related to pain), nutrition health (self-reported presence of a healthy diet, 24-hour intake recall, percent whole-food on plate), willingness to make a lifestyle change (0-10 scale; 10 = most willing), confidence in making a lifestyle change (0-10 scale; 10 = most confident), and patient goals. Patient goals were selected by the patient and included any of the following: optimize for surgery, qualify for surgery (i.e., no surgical date at the time of enrollment because of their chronic lifestyle-related disease(s)), weight loss, increase physical activity, reduce pain, improve sleep, improve nutrition, manage stress or anxiety, improve hypertension, improve diabetes, improve hyperlipidemia, reduce medication.
Program completion data included duration of time in the program, utilization, change in weight, change in BMI, and goal attainment. For utilization, the types of interprofessional providers seen and the number of visits with each provider were collected. Group medical visit participation was also tracked.
Patient-reported outcome measures were collected at baseline and program completion and included average and worst numeric pain rating scale (NPRS) scores (0-10 scale; 10 = worst pain), PROMIS-10 physical health, PROMIS-10 mental health, and PHQ-4 (0-12 scale; 12 = most severe psychological distress). Blood work was collected at baseline and/or program completion and included hemoglobin A1C (HgA1C), lipid panel, C-reactive protein, and vitamin D.
Statistical Analysis
All patients who met the eligibility criteria were included in the analysis. Descriptive statistics were employed. Continuous variables were summarized as means and standard deviations. Discrete variables were summarized as counts and percentages. Patient-reported outcomes measures at program completion were compared to those at baseline, and rates of improvement were calculated. Similarly, rates of improvement were calculated for lab measurements with available baseline and program completion data.
Results
Patient Program Pathway
Of the 294 patients enrolled in the intensive LSM program, 104 have been discharged to date. There were 13/104 nonoperative patients, and 37/104 surgical patients stopped the program prior to completion. Of the 37 surgical patients who left the program, 23/37 (62%) were nonadherent, 7/37 (19%) were unable to commit because of financial cost of the program, 6/37 (16%) felt the program did not meet their needs, and 1/37 (3%) transferred to a weight loss program (Figure 1). The remaining 54 surgical patients are included in this study. Patient flow diagram.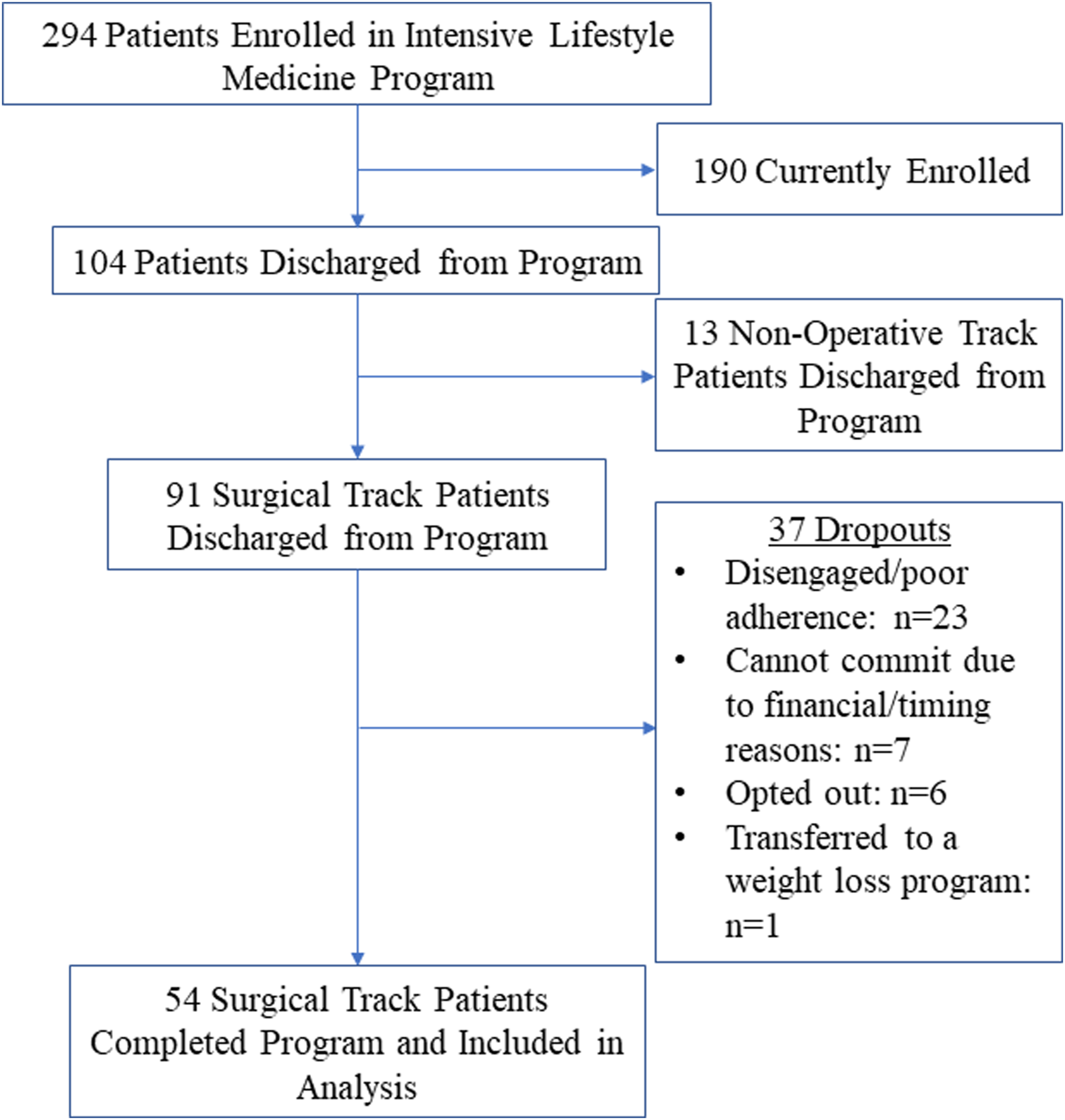
Baseline Patient Characteristics
Demographics and Baseline Characteristics.
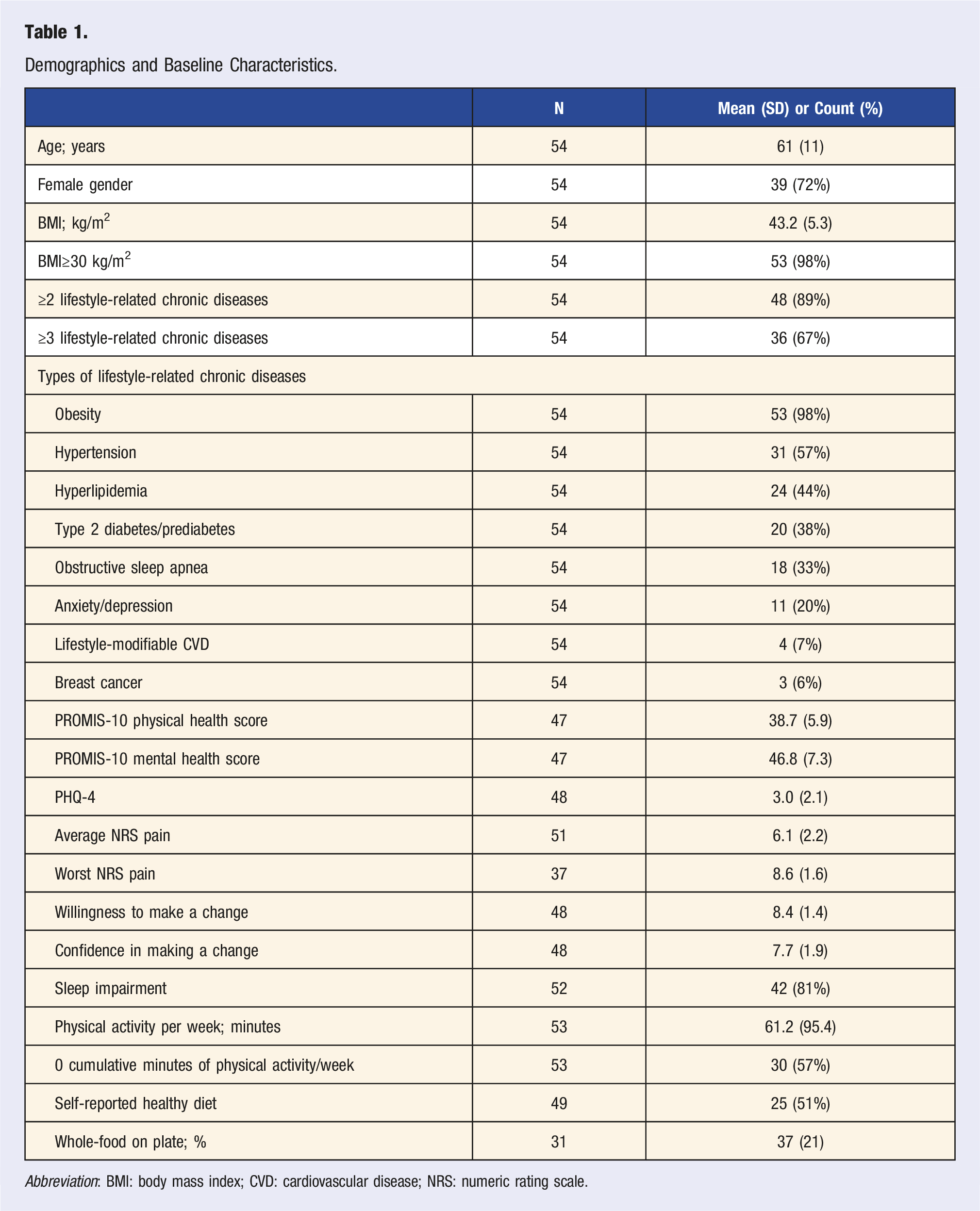
Abbreviation: BMI: body mass index; CVD: cardiovascular disease; NRS: numeric rating scale.
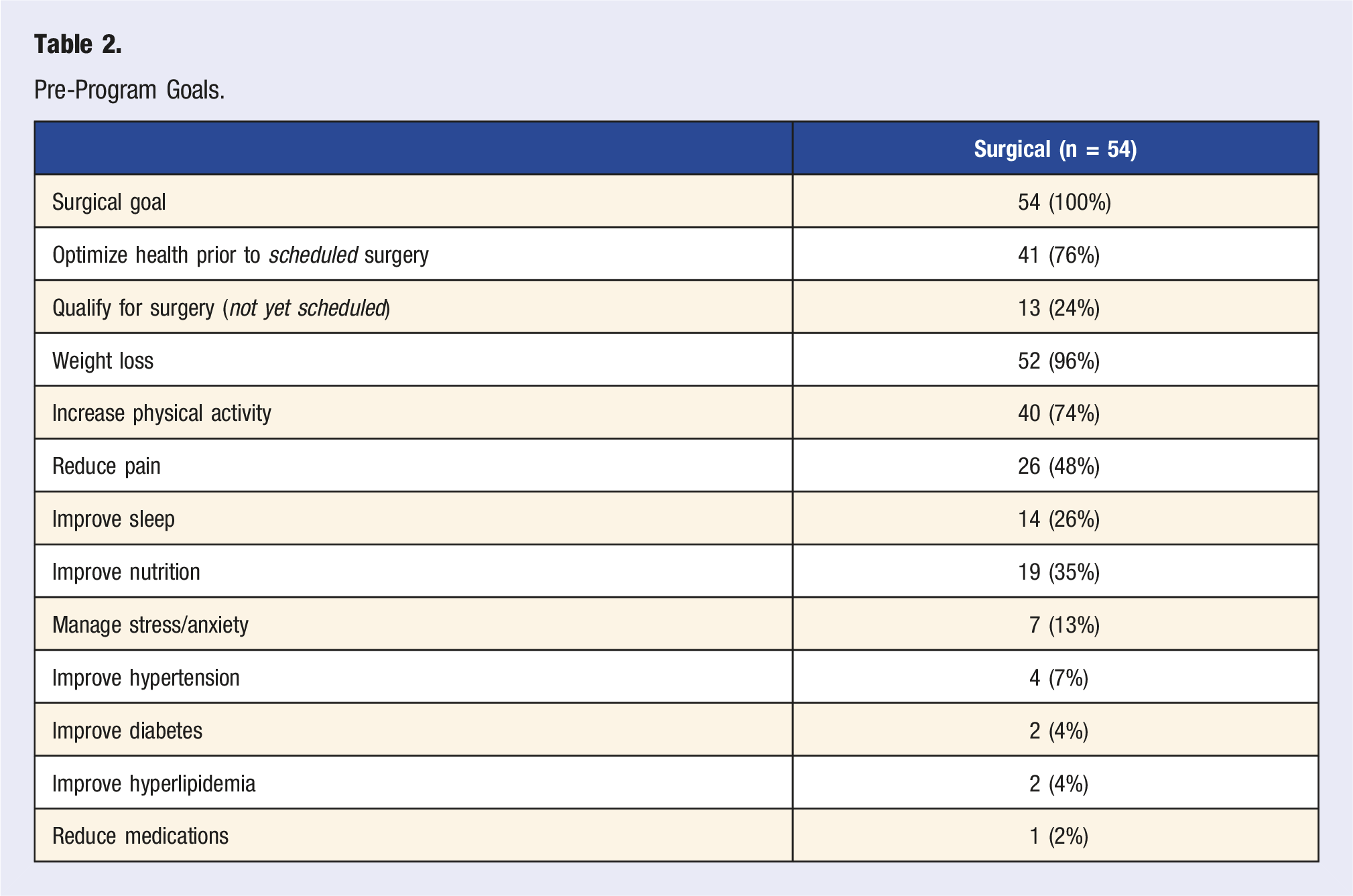
Pre-Program Goals.
Program Utilization and Outcomes
Program Utilization and Outcomes.
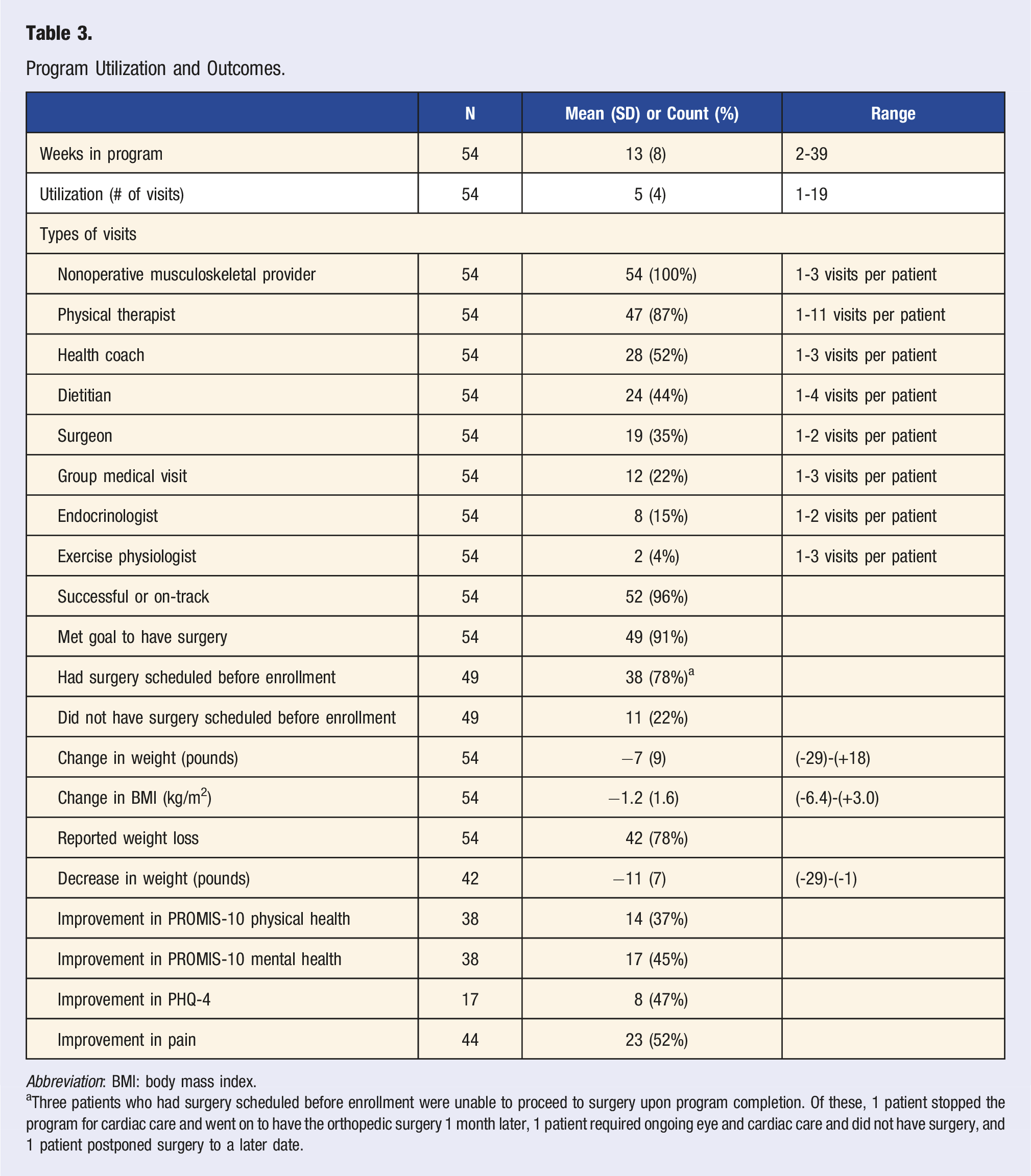
Abbreviation: BMI: body mass index.
aThree patients who had surgery scheduled before enrollment were unable to proceed to surgery upon program completion. Of these, 1 patient stopped the program for cardiac care and went on to have the orthopedic surgery 1 month later, 1 patient required ongoing eye and cardiac care and did not have surgery, and 1 patient postponed surgery to a later date.
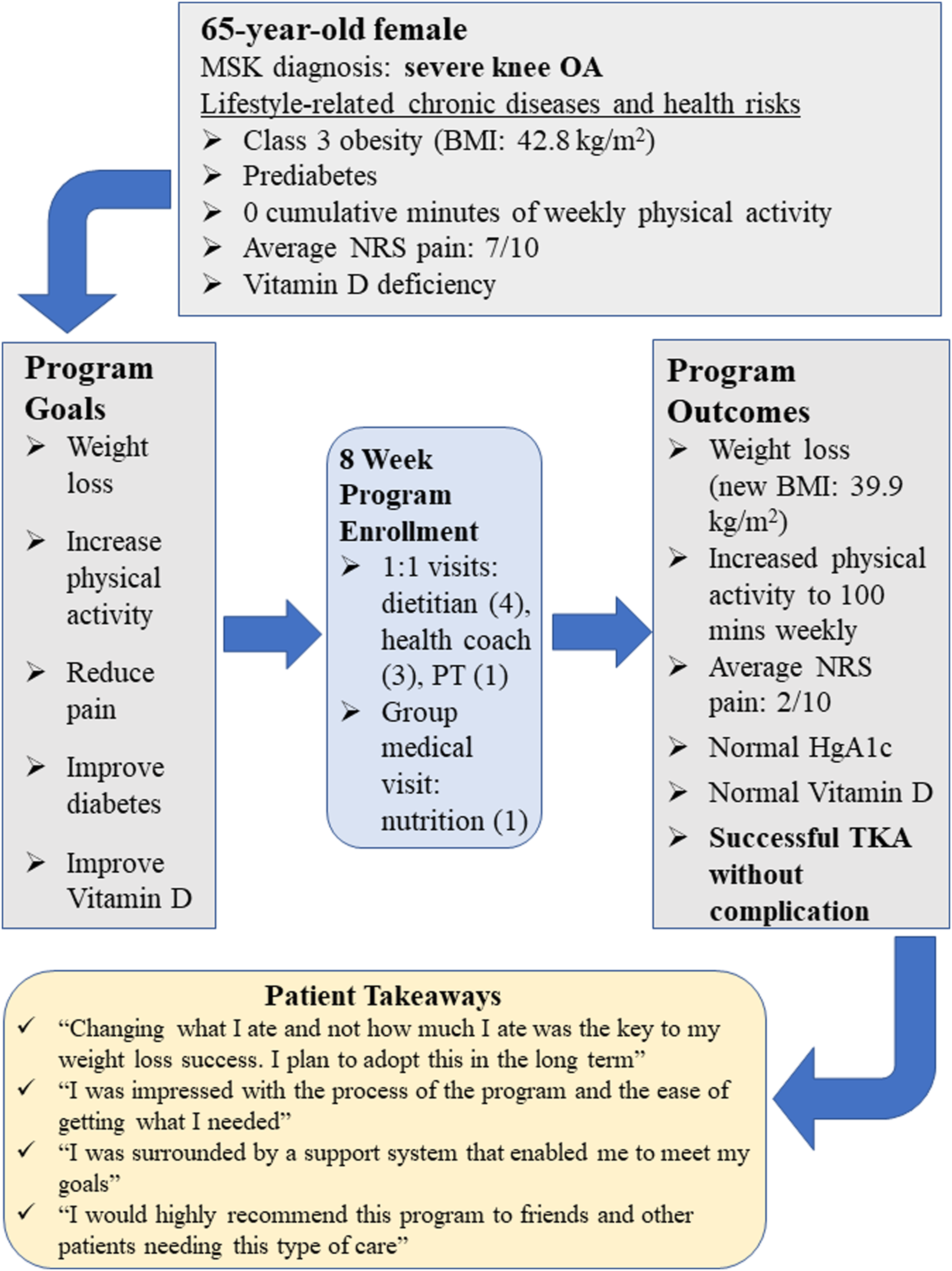
In this subgroup of 49 patients who went on to have surgery, 35/49 (71%) were female, and the mean program duration was 13 ± 7 weeks. Average willingness and confidence in making lifestyle changes prior to surgery were 8.5 ± 1.4 and 7.9 ± 1.8, respectively, which were slightly higher than the averages for those who did not proceed to surgery (willingness to make changes: 8.0 ± 1.2; confidence making lifestyle changes: 6.4 ± 1.9). The mean weight loss was 11±7 pounds, 8/14 (57%) had improvement in HgA1c, 3/4 (75%) had improved lipid panels, and 2/3 (70%) had improved vitamin D (Figure 2). Surgery types included TKA (32/49; 65%), THA (16/49; 33%), and lumbar spine surgery (1/49; 2%). An example of an individual patient journey through the LSM intensive program to successful TKA is described in Figure 3. Outcomes for patients who were able to have surgery. Percentages of patients who improved (dark blue) and did not improve (light blue) following completion of the lifestyle medicine program are shown. Weight, pain, PROMIS-10 (physical health and mental health), PHQ-4, HgA1c, lipid, and vitamin D data at program completion were compared to those at enrollment. Patient journey case schematic.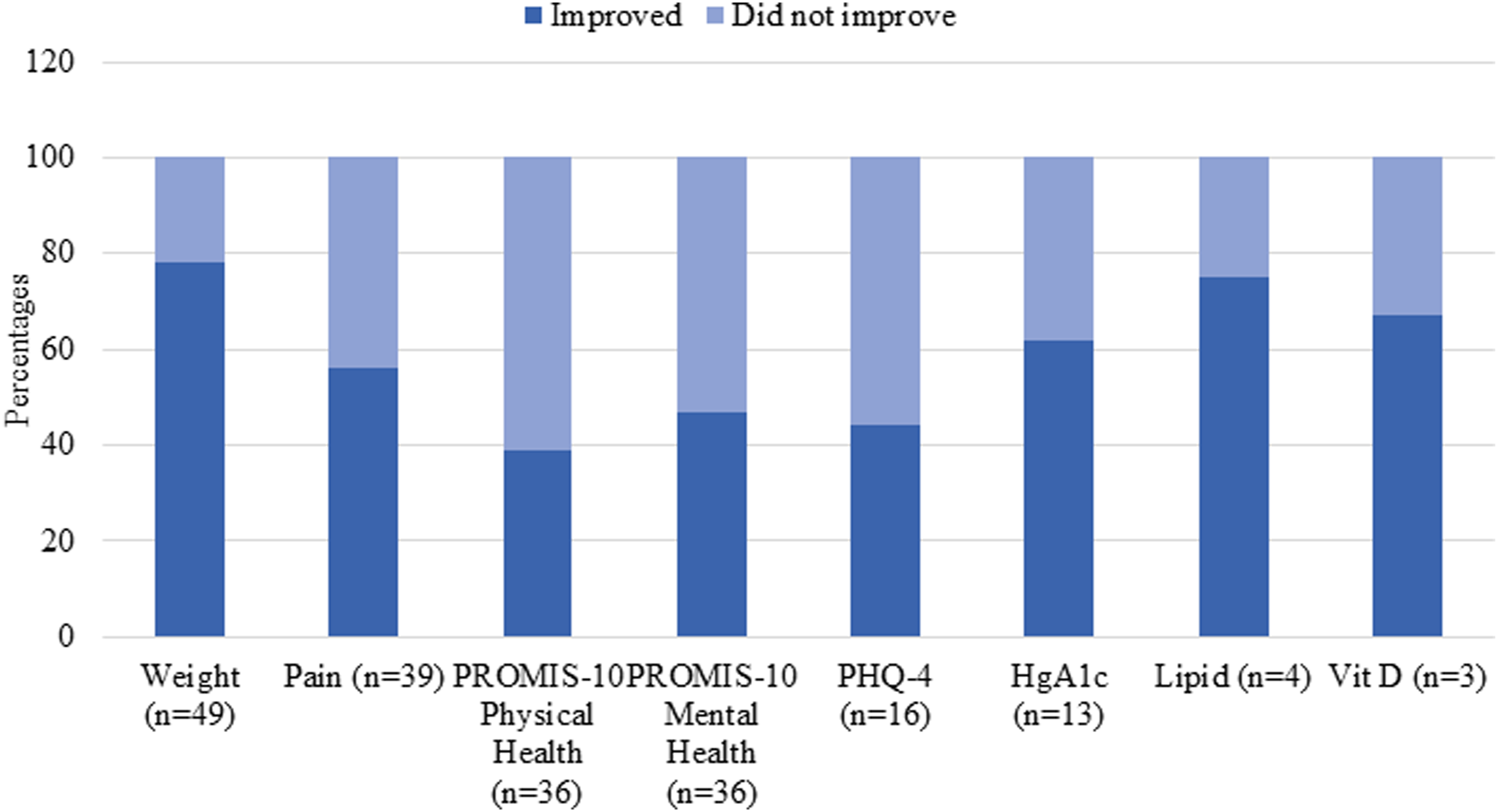
Discussion
This is the first study to describe pre-surgical orthopedic patient outcomes at the completion of a standardized LSM program designed to treat lifestyle-related chronic disease and musculoskeletal conditions in tandem, as a method to address health optimization prior to surgery. All patients were referred by their orthopedic surgeon and opted to participate in the program following an initial intake with a LSM provider (HP, KG). Ninety-three percent of patients with a surgical date at the time of entry into the program were able to improve their health and have their surgery on time. Of the patients whose surgeon deemed them too unhealthy to schedule a date for surgery, 85% were able to improve their health to qualify and proceed to surgery. This latter subgroup of patients who were able to qualify for surgery represents an increase in access to care for patients who, prior to the implementation to the program, would have been turned away. These results suggest that whole-person care utilizing the evidence-based implementation of the 6 pillars of health is beneficial for patients with musculoskeletal conditions attempting to optimize health prior to an elective orthopedic surgery.
Historically, health optimization prior to surgery has focused on pre-surgical weight, but more recent evidence is showing that weight loss in isolation may not be the entire solution. Roman et al conducted a meta-analysis including 6060 patients and found no associations between nonoperative weight loss interventions prior to surgery and a reduction in perioperative mortality or morbidity. 34 Of note, those patients who participated in a weight loss program had a 27% shorter hospital stay. Further, literature regarding bariatric surgery for weight loss prior to orthopedic surgery is not uniform and continues to present gaps in knowledge. A review by Murr et al evaluated the association between obesity, bariatric surgery, and orthopedic surgery. 35 Nine studies reported that prior bariatric surgery decreases complications, time in the operating room, length of hospital stay, and re-admissions within 90 days. In contrast, other studies found higher reoperation rates due to joint stiffness, infection, and a higher need for revision surgery in the first 90 days following a total joint arthroplasty. In a systematic review of the effect of bariatric surgery prior to lower-extremity total joint arthroplasty, Gu et al concluded the quality of evidence ranged from moderate to high, but no consensus could be determined on the effect of bariatric surgery on early to short-term total joint outcomes. 36 These data continue to evolve, and long-term conclusions are unclear at this time. 36 We intend to contribute to investigating the benefit of using all 6 pillars of health to not only enhance health but also mitigate risk, both at the time of surgery and post-operatively, and to assess outcome comparisons using this comprehensive approach, as compared to weight loss, diabetes, or cardiovascular conventional medical approaches implemented in isolation.
Health optimization prior to surgery often focuses on a specific modifiable lifestyle-related chronic disease in isolation and includes programs developed to specifically address each chronic disease, such as type 2 diabetes,37,38 obesity,39,40 and cardiovascular disease. 41 The application of LSM for pre-surgical health optimization allows us to deliver whole-person healthcare and address all aspects of lifestyle that can improve health and have the potential to reduce pain and improve outcomes. Outcomes in large patient volumes regarding the impact of the program on patient health, surgical risk reduction, and functional and patient satisfaction with their orthopedic surgery will need to be studied over time to determine the specific impact of the program. Additional investigations are planned to evaluate longer-term outcomes in patients with lower motivation and confidence for behavioral change (selective track patient cohort), as well as outcomes in patients who do not complete the intensive program for a variety of reasons we are tracking. Our findings are important and very applicable to patients undergoing similar procedures who are motivated to make behavioral changes and are able to complete the program, but there is a subset of patients who end up being disengaged for various reasons. It is important to investigate patient characteristics in these various subgroups of patients to better learn how to enhance their care. We have developed a LSM repository to enable us to partner with our orthopedic surgeons of all subspecialties to collaboratively report the outcomes regarding modifiable lifestyle-related health measures, perioperative patient course, and more long-term outcomes related to the continued adoption of lifestyle changes, improvement in pain and function, and patient satisfaction following their orthopedic surgery.
Currently, we are administering this program as a fee-for-service model with supplementation by the hospital for health coach services, IT support, and administrative support. Our goal is to find a sustainable financial model to increase patient access to the program. Our tertiary orthopedic surgical hospital setting provides us with the opportunity to best define the pre-surgical needs of musculoskeletal patients with concurrent lifestyle-related chronic diseases, as well as the interventions that optimally enable reduction of risk and improved outcomes and patient satisfaction.
Limitations
There are several limitations to this study. We report only the initial improvements measured in a small number of pre-surgical orthopedic patients upon completion of the intensive LSM program. More data are needed in a greater volume of patients to determine the immediate, intra-operative, perioperative, and long-term outcomes in patients completing the program. Long-term follow-up is key to determine patient adherence to behavioral change over time and its impact on long-term outcomes. Assessments of patients not completing the program, as well as the analysis of patient outcome comparisons prior to and following the establishment of the LSM program, are planned to help bridge the gap in our understanding of the impact of the program. Recently, the hospital mandated the program for patients at high intra-operative and perioperative risk. With over 32000 orthopedic surgeries performed annually and a supportive culture that enables us to provide care to improve whole-person health, we anticipate we will be able to report large data sets describing the short- and long-term impact on patient health, outcome, and satisfaction. Another limitation is these data are reflective of one center situated in a tri-state area, and therefore, the results may not be generalizable to other geographical sites. Further, the patient population reported here was primarily Caucasian. Barriers to care need to be identified, and solutions need to be found for the pre-surgical orthopedic patient population in order to provide the best access to evidence-based LSM care to all patients in need.
Other limitations include missing data points. Not all metabolic measures are available as discrete data points in the electronic medical record. The hospital has supported an extensive electronic medical record program built to allow us to measure real-time data. As we continue to fine tune the program, we have added discrete data to the electronic medical record regarding program completion, conversion of patients from the selective to intensive LSM program, charting changes of metabolic and anthropometric measures, medication deprescribing, and patient goal completion. We expect our data collection to continue to improve over time.
Conclusion
Pre-surgical orthopedic patients enrolled in an intensive LSM program for 13-14 weeks on average and were able to improve their health and pain following completion of the program. We were impressed by the speed at which pre-surgical orthopedic patients were able to make lifestyle changes. This may be attributed to the fact that pain and functional loss impacting quality of life may be the gateway for patients to progress to an active state of behavioral change. Musculoskeletal providers need further awareness and training in LSM in order to take advantage of the patients’ readiness for behavioral change. Pre-surgical orthopedic patients can be especially motivated to make changes because of the severity of their pain and functional impairment. We need to be ready to champion the patient in front of us. Lifestyle medicine programs for musculoskeletal patients can provide the gap in care that exists to enable metabolic and mental health improvements that are linked and, when present, prevent improvement in musculoskeletal conditions. Pre-surgical orthopedic patient data presented here show a promising potential application of LSM. More studies are needed to determine how intra-operative and post-operative risk can be mitigated by long-term behavioral change enabling improved whole-person health and orthopedic surgical outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: REDCap use was supported by grant number UL1TR002384 from the National Center for Advancing Translational Sciences of the National Institutes of Health and Sorenson Family Foundation grant support for the HSS Lifestyle Medicine Program.