
Abstract
Culinary-based self-care programs are innovative and increasingly utilized models for catalyzing behavior change and improving health and well-being. The content, duration, and delivery of existing programs vary considerably. Between January and August 2019, we developed a teaching kitchen and self-care curriculum, which was administered as part of a year-long worksite well-being program to employees at an academic healthcare system. The curriculum domains included culinary skills, nutrition, physical activity, yoga, stress management, mindful eating, and ethnobotany. An informal systematic literature search was performed to assemble and evaluate key principles and practices related to self-care domains, learning methodologies, and programmatic design considerations. Here, we provide a qualitative summary of the evidence-informed development of the curriculum intervention.
Culinary medicine and multidisciplinary teaching kitchen programs are emerging as new models for health promotion
Introduction
Approximately half of all deaths in the United States can be attributed to health behaviors such as poor diet, physical inactivity, smoking, and alcohol use. 1 Despite extensive research, translating the knowledge gained into actions has remained challenging. 2 A wide array of clinical and non-clinical approaches have been utilized to encourage healthy behaviors. Culinary medicine and multidisciplinary teaching kitchen programs are emerging as new models for health promotion. Although the focus of teaching kitchen programs is on basic cooking techniques, programs typically also include education on nutrition, physical activity (PA), mindfulness, and other self-care practices. 3 Research has shown that these programs increase participants’ overall cooking knowledge and confidence. 4 They also have positive effects on health outcomes such as improved intake of dietary sources of fat, fiber, sugar, and sodium 5 ; decreased serum cholesterol 6 ; and improved quality of life in participants with chronic diseases. 7 These noted benefits have also led to the United States Prevention Services Task Force (USPSTF) recommending that adults with a body mass index of 30 or higher be guided toward participation in multicomponent behavioral interventions by their clinicians. 8
Although the common aim of culinary-based teaching programs is to improve personal and public health through the adoption of healthier lifestyle habits, programs are generally customized for distinct populations and vary in their specific goals. 3 Since their inception in 1980, programs have differed considerably in terms of their rationale, design, outcome, and method of delivery. 9 Such non-uniformity makes evaluating and comparing programs difficult.
We provide the evidence behind the content, design, and delivery of a culinary medicine–based lifestyle program developed and implemented as a worksite wellness program at an integrated academic healthcare system. We aim to provide theoretical guidance in creating culinary medicine–based lifestyle programs in diverse settings.
Methods
Between January and August 2019, a teaching kitchen curriculum was developed and delivered as part of a year-long Emory Healthy Kitchen Collaborative worksite wellness program. The program content was multidisciplinary, including nutrition, culinary skills, PA, stress resilience, yoga, mindful-based eating, and ethnobotany. The teaching methods included didactic, experiential, and group learning. The program was delivered as five 4-hour classes (20 hours) held bi-weekly on Saturdays to 40 benefits-eligible employees.
Here, we summarize the literature on three aspects of our teaching kitchen methodology: (1) content, including key principles and practices incorporated into teaching kitchen curricula; (2) learning methods used in curriculum delivery; and (3) curriculum structure, including program duration and class frequency, length, and delivery (Figure 1). Although not exhaustive, this rationale can be applied by others interested in offering culinary-based wellness programs. Evidence-informed considerations for culinary-based interventions. *The behavioral interventions listed are ones included in the Emory Healthy Kitchen Collaborative. Other interventions could be included, such as sleep and social connectivity.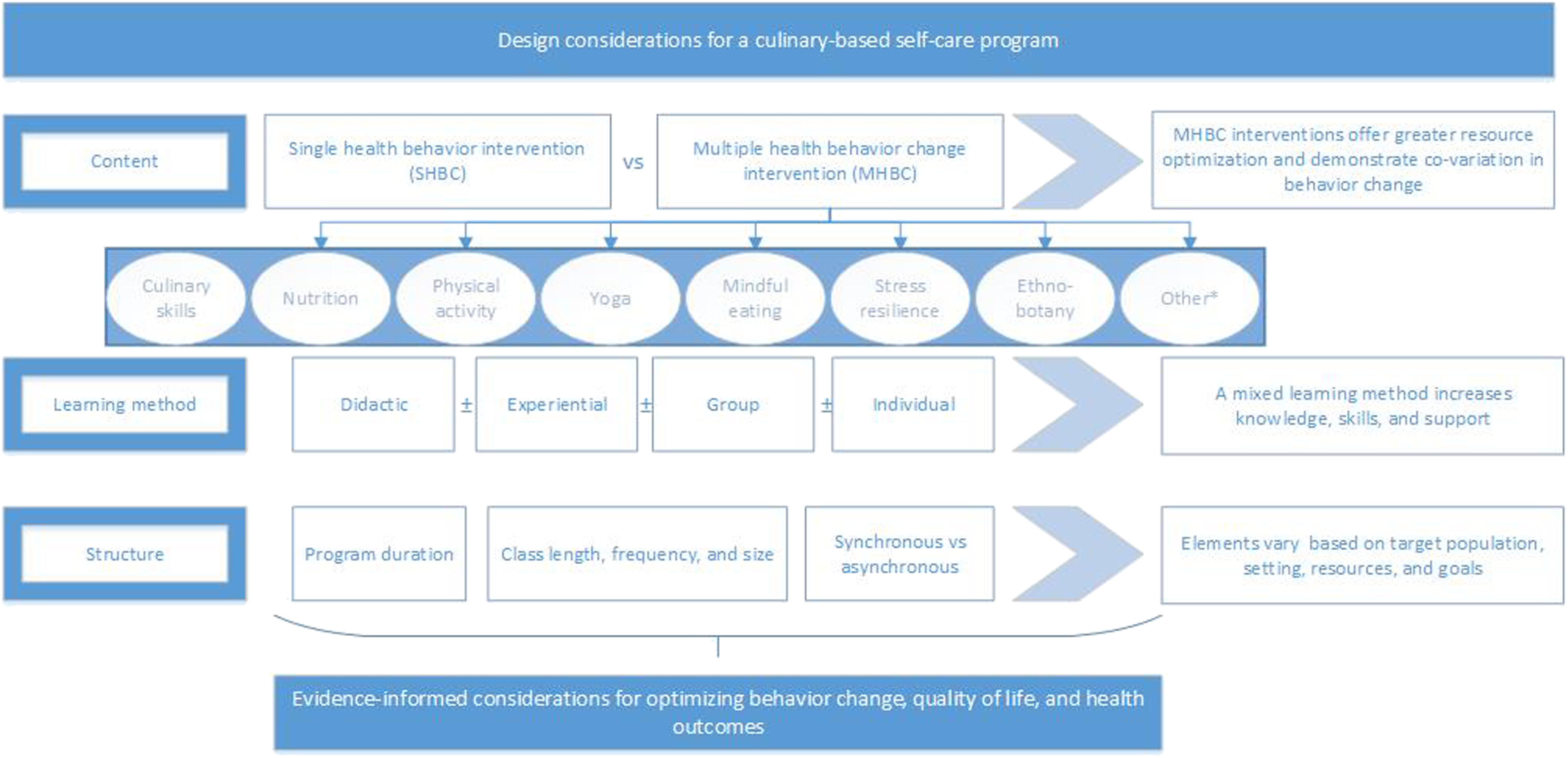
The Number and Composition of Health Behavior Interventions
Single vs Multiple Health Behavior Interventions
Multiple health behavior change (MHBC) intervention defines any treatment in which two or more behaviors are targeted for improvement either simultaneously or sequentially. 10 While single health behavior interventions may be more common, MHBC interventions allow a more resource-optimized method of delivery. They also provide greater real-world application for patients, healthcare systems, and affiliated organizations by providing information on effective treatments that can be utilized simultaneously. 11 Additionally, these types of interventions can help reduce healthcare costs by maximizing the intervention contact between providers and patients. 11 Popular interventions such as the Ornish, Pritikin, and Complete Health Improvement Program (CHIP) programs have utilized this approach in order to reverse cardiovascular risk factors and assist in prevention, treatment, and reversing of chronic disease. 12 While effective, these programs are typically viewed as intense due to the amount of sessions individuals participate in within the first 3–4 weeks of the program. The Ornish program includes two 4-hour sessions within the first week12,13; the Pritikin involves a 7-day-a-week live-in experience 14 ; and the CHIP program involves 18 group sessions spread out over 6–12 weeks. 15 MHBC interventions have been used to successfully target improvements in nutritional intake. In a study with simultaneously employed nutrition and PA interventions, fruit and vegetable intake (P < .001) and PA (P < .0001) increased moderately. 16 In a randomized controlled study of older adults comparing treatment effect of either PA, weight loss and PA, or a successful aging health education program, improvement occurred only in the group that received the multiple behavior intervention of weight loss and PA. 17
A systematic review that attempted to compare the effectiveness of single behavior change (SHBC) interventions to MHBC interventions among older adults concluded there are currently too few MHBC interventions for comparative interpretation. 18 In their analysis, there were substantially more SHBC interventions found than MHBC interventions (8:1 ratio). While gaps remain in MHBC knowledge and efficacy, multiple behavior change programs are conceptually more advantageous in terms of efficiency and health impact. 18 Based on the theoretical benefit and demonstrated co-variation of behavior change, where individuals taking effective action on one target behavior are more likely to make progress on another behavior, 19 we felt a MHBC design would be most efficacious in creating sustainable healthy behavior change.
Composition of Behavior Change Interventions
Nutrition
Knowledge about dietary intake is an integral component of a well-being curriculum as inadequate nutrient intake has been linked to one out of five deaths and 255 million years of healthy life lost worldwide. 20 Poor dietary intake ranks globally as the most important risk factor for mortality, causing more deaths than any other risk factor, including tobacco use, high systolic blood pressure, excess alcohol, and low PA. 20 While there is ample debate regarding the composition of the healthiest dietary pattern for human health, convergence of evidence from physiologic mechanisms,21,22 observational studies, 23 randomized controlled trials, 24 and centenarian studies 25 demonstrate the optimal dietary pattern for disease prevention and mental and physical performance is a predominantly whole food, plant-based dietary pattern. This dietary pattern emphasizes minimally processed foods predominantly plants, including ample fruits, vegetables, whole grains, legumes, nuts, and seeds. The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), vegetarian, vegan, and Paleolithic diets share encouragement of a whole food, plant-predominant dietary pattern. 26 Since a larger number of deaths are attributed to a lack of adequate intake of fruits, vegetables, whole grains, legumes, fiber, nuts, and seeds than to consumption of red and processed meat and sugar-sweetened beverages, 20 wellness curriculums covering benefits of a whole food, plant-based dietary pattern can lead to improved biometric and quality of life outcomes.
Culinary Skills
According to recent studies, 28% of Americans do not know how to cook. 27 This startling finding is one of the main reasons many persons choose to “eat out” and consume more ready-to-eat, calorie-dense food. In 2014, total food expenditure for food away from home rose to 50.1%, surpassing at-home food sales, 28 and 62% of the calories in the standard American diet were from processed foods. 29 Lack of culinary skills is one of the main barriers to healthful food preparation. 30 The prevalence of poor diet is increased in communities in which there is inadequate food access, low food and nutritional literacy, and a lack of practical cooking skills. Therefore, including culinary skills in a curriculum can encourage persons to eat at home and decrease consumption of low-quality foods with poor nutrient density. Cooking classes have been shown to decrease calorie percentage intake from fat, cholesterol, sodium, and carbohydrates. 31 Furthermore, exposing participants to new foods increases variety and facilitates greater adherence to dietary guidelines for fruit and vegetable consumption. Inclusion of culinary skills has also been shown to improve an individual’s cooking confidence and cooking and eating behaviors, leading to a positive effect on diet quality and obesity among adults. 32
Physical Activity
Physical activity has beneficial effects on depression, anxiety, self-esteem, and cognitive function. Improvements in these areas led to increased strength and flexibility, decreased intake of analgesics, improved overall health, and a better ability to manage stress and cope with workloads.33,34 Improving and maintaining health-enhancing levels of PA additionally leads to reductions in the metabolic, hemodynamic, body composition, epi-genetic, and functional status risk factors that heavily contribute to the development of many leading chronic diseases. As such, PA has a significant role, often comparable or superior to drug interventions. 35 Physical activity effectively helps prevent and treat more than 40 diseases such as heart disease, diabetes, hypertension, cancer, depression, anxiety, arthritis, and osteoporosis. 36 However, PA levels have remained flat for decades, 37 with only half of adults (53.3%) meeting the aerobic activity guidelines and 23% meeting both aerobic and muscle-strengthening guidelines. 38 Increasing PA via counseling in healthcare settings is supported by substantial international evidence.39,40
Stress Resilience
Stress has bidirectional interactions with many health-relevant pathways, including metabolic function, 41 appetite, mood, 42 the enteric microbiome, 43 cardiovascular pathophysiology, 44 and the sleep–wake cycle. 45 Given its interrelationship with other core areas of lifestyle medicine, tools for stress management and resilience-building are an important mediator of the salutary effects of MHBC interventions. 46 Stress resilience training includes approaches to cultivate and promote emotional competencies (e.g., emotion regulation and self-efficacy) as well as social competencies (e.g., interpersonal gratitude and social connection). 47 Integrative, mind-body interventions such as mindfulness meditation and compassion-based meditation practices target these competencies and have been shown to reduce psychological distress, depression, and anxiety and to increase positive emotions and quality of life.48,49
Yoga
Yoga is an intervention for stress reduction, among other benefits. Studies have shown after a brief intervention, participants show improvements in perceived stress, mindfulness, empowerment, positive affect, negative affect, self-compassion, total work engagement, vigor, sleep quality, resilience, satisfaction with life, as well as reduced professional burnout (all P values < .01). 50 As a contemplative activity incorporating attention training, breath awareness, and integration of breath and movement, yoga explores and strengthens the connection between the body, mind, and spirit. Evidence shows regular yoga practice leads to improvement in the cardiopulmonary risk profile, 51 anti-inflammatory effects, 52 relief of pain, 53 and attentional control, 54 as well as enhancement of executive functioning and working memory, buffering age-related decline. 54 Key concepts in yoga include respecting the state of each individual approaching the practice and adapting the practice to meet individual needs. Rather than striving to attain an ideal expression of a particular pose, the focus should be on using the practice as a tool to better understand the individual and deliver maximum benefit.
Mindful Eating Practices
Currently, no standardized set of practices define mindful eating. Fung’s 55 model identifies four foci: what to eat, why we eat, how much to eat, and how to eat. Protocols emphasize different aspects and may or may not include basic nutrition information or a weight reduction component. However, traditional weight loss diets promoting rigid or restrictive meal plans are eschewed based on the premise that eating that does not feel satisfying and enjoyable will undermine the long-term goal of sustainable weight management.
Research demonstrates mindful eating can improve adaptive eating behaviors (slow the pace of eating, increase healthy food choices, and decrease emotional eating/binge eating episodes) as well as improve psychological well-being, body satisfaction, and some biological indices. 56 Significant weight gain is not typical even though most individuals fear this will occur if they give up their unsuccessful “dieting” efforts. On average, stabilization of weight but not weight loss is reported in current studies, but additional research needs to be done before definitive conclusions can be reached about the long-term effects of mindful eating on weight and other health outcomes.
The practice of mindful eating has been promoted as a psychoeducational intervention for the general public 57 and has been embedded within programs targeting clinically significant disordered/binge eating. The latter type of program includes specific behavioral strategies, especially versions of self-monitoring, for example, Appetite Awareness Training developed by Craighead 58 and Mindfulness Based Eating developed by Kristeller. 59 Mindful eating practices have been taught across age groups60,61 and are considered to be particularly appropriate for children where emphasizing weight loss may be iatrogenic. Mindful eating is compatible with a range of culinary traditions and can be adapted to address a range of weight issues that may be unique to diverse samples. 62
Ethnobotany
Ethnobotany has been defined as the study of plants and their practical uses through the traditional knowledge of local culture and people. Certain plants have analgesic and anti-inflammatory effects leading to decreased inflammation and cortical vascular contractile dysfunction. 63 Intercultural health care, defined as the integration of traditional medicine and biomedicine, represents a key aspect of health, especially for minority and underserved communities. 64 Through encouraging participants to explore their own cultural and culinary connections to spices through the lens of ethnobotany, information regarding their health benefits, which include anti-diabetic, anti-inflammatory, anti-hyperlipidemic, and anti-hypertensive effects, 65 is made more accessible.
Learning Methods
Benefits and Limitations of Didactic Learning
Didactic learning is a teaching method that primarily seeks to improve student’s knowledge. In this educational model, the teacher functions as a guide or resource for students and as an authoritative figure. The benefits of didactic instruction are its familiarity and effectiveness at presenting large amounts of knowledge. Additionally, didactic methods are understandable, informative, and motivational. In a study investigating its effects on hypertension control in Vietnam, didactic teaching led to a decline of 5.5 mmHg. 66
Didactic learning research has shown that this method alone is limited in developing proficiency in situational problem-solving and application to clinical settings that require critical thinking skills. In a study looking at the effectiveness of didactic learning vs experiential learning in nursing students, post-test scores were significantly higher in the experiential vs didactic learning group. 67 These results suggest didactic learning can be utilized in a culinary curriculum to build participants’ knowledge base through the transfer of knowledge from the teacher to students. 68 However, additional learning methods help ensure the application of knowledge toward the development of behavioral skills.
Benefits and Limitations of Experiential Learning
Experiential learning provides an avenue for the application of theories into practice and is an important contributor to higher education. In comparison to didactic learning, experiential learning is effective first because it mimics a real-world problem, allowing for greater carry over to actual life situations. Second, it requires more involvement and engagement with participants, which leads to better learning and retention of new concepts. 69
The efficacy of experiential learning has been examined in a variety of curricula. In fifth grade students, student cognitive ability measured by achieving a minimum passing grade on a mathematic examination was shown to be higher in an experiential vs a control group. 70 In another study, experiential learning via virtual reality (VR) technology mimicked real-life experiences through enhanced vividness and led to an increased learning effect. 71 Additionally, in a student-run free medical clinic, experiential learning through clinical experience enhanced the knowledge and skills of medical students by helping them translate classroom learning into practical experiences. Experiential learning also contributed to the student’s belief that they can become competent practitioners within their fields. 72 Similarly, in a business studies curriculum, the use of case studies as a method of experiential learning proved more efficacious for learning than the use of decision-based situations. 73 While clearly a useful tool, one of the main limitations to experiential learning in workplace wellness programs is time availability. As noted by Kolb, there are four stages individuals must go through for effective experiential learning. The cycle involves concrete learning as well as reflective observation, abstract conceptualization, and active experimentation. 74 Class time constraints of both participants and instructors may lead to difficulty for participants to progress through these stages at their own speed.
Group Interaction for Promoting Wellness
Group interaction refers to the dynamics of a team and the interaction among its members. As a method of learning, group interaction provides opportunity for collaboration on challenging tasks in pairs or groups. Various studies have shown when used in combination with lifestyle change interventions, group interactivity can yield significant results. For example, in comparison of a group vs an individually delivered weight management intervention, participants receiving the group intervention reported greater weight change (mean difference of −1.4 kg) over one year (P-value = .03). 75 Another study showed more weight loss and reduction in hemoglobin A1c, fasting blood glucose, blood pressure, and medication use in the group-based intervention group compared to the routine, waiting list control, or the no intervention group. 76
Group interventions can also play an important role in improving outcomes by increasing participant confidence and levels of engagement. For example, when participants in a University of South Florida weight loss initiative reflected on the strengths and weakness of the program post-completion, they described the program’s teamwork structure as instrumental in providing encouragement and inspiration for putting forth more effort to establish healthier habits. 77
Due to the synergies between didactic, experiential, and group learning in blending knowledge, skills, and collaboration, many teaching kitchen programs have incorporated a mixed learning method. Examples include the prototypic teaching kitchen program piloted by Eisenberg et al., 78 the TEACH kitchen in Augusta, Ga, 79 the Veterans HTK Program, 80 and a childhood obesity program. 81 We similarly used a combination of didactic, experiential, and group discussion classes. The didactic classes included the scientific rationale, practical applications, and recommendations for implementing self-care components into participants’ daily lives. Experiential learning included hands-on cooking demonstrations, mindfulness-based lunches, a yoga session, and a group exercise session. Sessions were designed to extend learning outside of the classroom and increase relevance to everyday lives. Rather than being prescriptive, the lectures and demonstrations aimed to inspire self-designed and personalized alterations in dietary patterns and behaviors matching participants’ culture, preferences, and health conditions. Each class ended with a group discussion exploring successes and challenges of implementing skills.
Curriculum Duration and Design
Theoretical and Empiric Considerations for Program Duration
Culinary-based interventions aim to bring about sustained lifestyle changes. For this to occur, most individuals must go through a decision-making process. 82 This process was first evaluated by Prochaska in the 1970s and has become the basis for many behavioral change programs. According to this model, behavioral change is a slow, arduous cyclical process where individuals move through various stages (pre-contemplation, contemplation, preparation, action, and maintenance) to arrive at true habitual behavior change. 83 This trans-theoretical model is particularly useful for lifestyle change programs as it allows providers to not only address the needs of people who are prepared to take action but also those that are still in the contemplation stage. The greatest strength of this behavior change model is that it appeals to a large group of participants while providing the perception of personalization. The trans-theoretical model has been applied to a variety of health interventions, including those involving fruit and vegetable consumption, 84 condom use, 85 and smoking consumption, with positive results. 86
On a theoretical basis, programs aiming to improve health habits should be 66 days or longer, which is the mean duration needed for habit formation. 87 However, the literature on efficacy based on culinary curriculum duration is sparse. In one 6-week program, participants felt this duration to be too short for achieving their health goals. 77 In another, following an 8-week weight loss intervention, participants were able to routinize the recommended lifestyle changes. 88 Based on theoretical and scant empirical data, a suggested curriculum duration would be a minimum of eight to nine weeks. However, programs may need to incorporate follow-up and reinforcement for 12 months or longer for sustaining improvements in biomarkers. 78
Class Size, Frequency, and Length
The number and frequency of classes offered in teaching kitchen curricula have ranged from eight hours 79 to over 60 hours. 78 In a systematic review, 89 health interventions that included three, 90 four,90-95 six,96,97 eight, 98 and 38 sessions 99 demonstrated efficacy. A systematic review of MHBC interventions showed that there are major variations in terms of length of intervention (varying between 6 and 104 weeks), frequency of intervention delivery (varying between 3 and 88 sessions), how the interventions were delivered (over the phone, mail, or internet), as well as in the type of provider used (exercise physiologist, nurse psychologist, etc.). 16 The review also showed a disparity in the number of participants in the interventions (ranging from 14 to 641). 89 Efficacious outcomes have been demonstrated in studies ranging from 40 78 to over 300 100 participants. The tremendous variation in session length, class size, and frequency limits any conclusions about the optimal design of a culinary-based intervention.
Asynchronous vs Synchronous Delivery
Asynchronous delivery of instruction allows interactions between learners and teachers to occur independently. 101 This delivery style offers flexibility for both educators and students and can be more cost-effective. 102 However, asynchronous delivery places responsibility on the learner, which can be challenging for those who require higher levels of teacher involvement. 102 In a study examining the use of asynchronous delivery in emergency medicine rotations for medical students found a majority of participants preferred an asynchronous delivery style, but few participated. Less than half of the subjects viewed all of the teaching modules, and 44.8% viewed either one or zero modules. 103 Similarly, in a study evaluating the use of computer-assisted instruction in senior medical student sub-internships in emergency medicine, 65% preferred computer-assisted instruction as part of their curriculum but only 28% accessed it. 104
Synchronous learning is a traditional delivery method in which both the learner and instructor interact together in the same time and space, including a virtual environment. In contrast to asynchronous delivery, synchronous delivery is more conducive of active learning. It allows for immediate clarification of concepts and extension of knowledge,102,105 which has been found to be important for learners with limited exposure and higher difficulty perception of subjects. 106 Research has shown that active learning can increase lecture attendance, engagement, and acquisition of expert attitudes toward the discipline of choice. 107 In a study of students enrolled in science, engineering, and mathematics courses, students involved in active learning had an increase in exam performance, concept inventories, and other assessments. In comparison, students in the traditional lecture courses were 1.5 times more likely to fail than students in courses that involved active learning. 108
When comparing these delivery methods and their effect on learning outcomes, no single method emerges as superior. In the emergency medicine study, results showed no statistically significant difference in post-test scores between the different methods. 103 Similarly, when comparing these methods in Bachelor of Medicine and Bachelor of Surgery undergraduate students, there was no significant difference in post-test scores between the two groups (P = .507). 106
A novel approach blending the two methods is a “flipped classroom.” In this model, students watch pre-recorded lectures before class and the class time is reserved for discussion and problem-solving of relevant topics. 109 The flipped classroom was shown to have superior efficacy in a study evaluating graduate student performance on cardiovascular, respiratory, and renal physiology. Flipped course participants had significantly higher scores on the cardiovascular and respiratory sections (P < .05), in addition to higher scores on the renal section (P < .06). 110 In another study investigating the flipped classroom teaching model in an introductory epidemiology class, 80% of students found it effective and had student evaluation of education quality variable scores that were significantly higher than pre-implementation (P = .003). 111
Discussion
Teaching kitchen programs are innovative models for improving health-promoting behaviors but are at an early stage of development. Based on existing literature, programs that incorporate multiple behavior change interventions may be more resource-optimized and may facilitate greater health impact through co-variation in behavior change. The behavioral domains frequently utilized include culinary skills, nutrition, PA, and mindfulness. A large body of evidence supports the key principles in each of these domains, as well as the inclusion of other self-care practices such as mindfulness-based eating, yoga, and ethnobotany. The three primary methods of delivery explored—didactic, experiential, and group learning—offer distinct advantages, and blended utilization of these methods may lead to the greatest gains in knowledge, skills, and confidence. Asynchronous and synchronous program delivery demonstrate comparable efficacy, and novel “flipped classroom” models combining both may be superior. Programs vary considerably with regard to duration and class frequency and length. They are currently primarily based on program setting and population.
Teaching kitchens offer a unique gathering place for learning self-care skills. Among their advantages, they provide an engaging and enjoyable learning environment and can be implemented in ambulatory and hospital systems as well as in organizations and community centers. The primary limitation to creating an evidence-informed framework for a teaching kitchen health promotion model is the paucity of intervention programs utilizing a teaching kitchen setting. The program structure development rationale presented here relies heavily on outcomes from various clinical and non-clinical programs and, hence, provides a sound theoretical construct. The information presented provides guidance on the efficient use of resources for catalyzing improvement in behavioral and clinical outcomes and may enable the reproduction of subsequent programs. Future studies investigating the feasibility of teaching kitchens are needed to aid in the standardization of this intervention model.
Footnotes
Acknowledgments
The sponsor did not play a role in the development or preparation of this manuscript. We would additionally like to thank Dr. Felipe Lobelo for his contributions to the curriculum content for physical activity.
Author’s Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Emory Healthy Kitchen Collaborative was supported by a grant from the Ardmore Institute of Health (Award 0000050387; 1/05/2019-1/03/2021).
Ethical Approval
Ethical approval for this study was obtained from an ethics committee or institutional review board.