
Abstract
“The physical, psychological, and social factors that affect strength training participation in individuals with RA makes prescribing strength training a complex and multifaceted endeavor.”
Introduction
Rheumatoid arthritis (RA) is an autoimmune inflammatory disease affecting 1% of the Canadian adult population.1,2 Pathological immune processes lead to dysregulated inflammation of the synovial membrane, resulting in structural joint damage and joint pain. 1 The systemic inflammation associated with RA often leads to other secondary complications including changes in body composition (e.g., rheumatoid cachexia with increased fatty infiltration into muscle), declines in functional ability, cognitive dysfunction, fatigue, as well as co-morbidities such as depression, cardiovascular disease, hypertension, dyslipidemia, and secondary osteoarthritis.1,3
Strength training is a safe intervention that can address many sequelae of RA. Strength training is done by sustaining or repeating muscular action with a goal to increase muscle strength and muscle mass. 4 It can be done with the use of one’s body weight, elastic resistance bands, household items, machines, or free weights. 5 In addition to increasing muscular strength, strength training has been shown to reduce pain, 6 lower inflammatory markers, 7 improve body composition (i.e., decreased fat mass, increased muscle mass),8,9 increase functional ability (e.g, walking performance),6,7 and lower cardiovascular and other comorbidity risk among individuals with RA.10,11 In addition to these benefits, even high intensity strength training has been found to be well tolerated by people with RA with no evidence of worsening disease activity nor radiological joint damage.7,12 In 2018, The European League Against Rheumatism (EULAR) published physical activity recommendations supporting strength training as an integral part of standard care in RA. Specifically, they provide strength training prescription recommendations (frequency, intensity, time, type, volume, progression; FITT-VP) and advise participation in strength training at least twice per week. 13
Despite its broad benefits, only 1–14% of people with RA engage in regular strength training.14,15 Barriers to participation in strength training identified in people with RA include challenges with recall of exercise technique, knowing how to adapt the exercise routine during a flare, knowing how to distinguish RA-related joint pain from delayed onset muscle soreness, and fearing that exercise may trigger symptoms. 16 Further, healthcare professionals including rheumatologists, nurses, and physical therapists acknowledge the importance of physical activity but the majority of those surveyed were uncertain on how to prescribe strength training to individuals with RA.17,18 While there is a focus on how to prescribe strength training based on FITT-VP parameters,7,13,19,20 it is equally important to highlight strategies that may facilitate the delivery of strength training prescriptions.21,22 The 2018 EULAR recommendations note that while the FITT-VP recommendations are well established, their feasibility amongst people with RA is not as well studied. Therefore, the purpose of this scoping review is to summarize current available recommendations from clinical practice guidelines, review articles, and recommendation papers that address participation factors to aid in the tailoring of strength training prescriptions for individuals with RA.
Materials and Methods
The scoping review methodology was based on the Arksey and O’Malley (2005) framework 23 which was updated by Levac et al. 24 (2010). Reporting was guided by the Preferred Reporting Items for Systematic Reviews and Meta Analyses—Scoping Review (PRISMA-ScR) checklist. 25 Scoping review methodologies are recommended for addressing exploratory research questions by “mapping” evidence to synthesize knowledge and determine gaps in the research area.23,24,26 Given the broad nature of the research question, a scoping review was conducted as opposed to a systematic review, which may be more suited towards answering a specific question addressing outcome measures of a certain treatment or practice. 27 Furthermore, the Arksey and O’Malley (2005) 23 scoping review framework includes an optional step in which stakeholders are consulted to offer their perspective on methodology and preliminary findings. We used an integrated knowledge translation approach, 28 whereby patient and healthcare professional partners were engaged in the scoping review process. Specifically, seven patient partners with arthritis, recruited from Arthritis Research Canada’s Arthritis Patient Advisory Board, 1 co-developed the research question, data extraction sheet, interpreted the data, and contributed to manuscript writing. The details of their involvement are described within each phase of the methods. The scoping review protocol was uploaded to Open Science Framework on July 10 2020 (https://osf.io/n4ygx/?view_only=8cbeb4acb6034606bb757e97ceb5f1c3at).
Identifying the Research Question
This scoping review addressed the broad question, “what are the available recommendations for tailoring strength training prescriptions for people with RA?” Seven patient partners, two of whom are physical therapists, co-developed the research questions and identified specific sub-questions to guide the scope of the research question. 29 The specific objective was to identify recommendations for tailoring strength training prescriptions for people with RA.
Identifying Relevant Studies
A medical librarian was consulted to develop the search strategy. The search was completed in May 2020. MEDLINE (OVID), Embase, and CINAHL were searched using the following keywords: (1) terms for strength training programs included resistance training OR strength training OR weight lifting OR resistance exercise OR strength exercise (2); terms for population included rheumatoid arthritis (3); terms for study designs included recommendation OR clinical practice guideline OR CPG OR prescription* OR review. Please see Supplemental Material 1 for a sample search strategy.
In addition, we searched gray literature including Canadian Agency for Drugs and Technologies in Health (CADTH), PROSPERO, Physiotherapy Evidence Database (PEDro), Canadian Medical Association (CMA), Clinical Practice Guidelines Infobase, National Institute for Health and Care Excellence (NICE), OTseeker, Guidelines International Network, Turning Research Into Practice (TRIP), Physiotherapy Association of British Columbia (PABC), The Scottish Intercollegiate Guidelines Network (SIGN), and Google Scholar. Reference lists of key articles were also searched. Two content experts identified from the author list of key articles were consulted to confirm the final list of articles.
Study Selection
Study inclusion criteria were (a) published articles and gray literature, (b) guidelines, recommendations, and review articles (with or without meta-analysis), (c) people with RA, (d) strength training prescription recommendations specific to RA. Exclusion criteria were articles (a) written in languages other than English, (b) that do not discuss a strategy for prescribing strength training or for addressing factors that affect strength training participation, (c) single studies. Patient and healthcare professional partners confirmed the criteria used for study selection were appropriate to answer the research question.
Following removal of duplicates, titles and abstracts were screened, and eligible articles were reviewed independently by JM and MW. Discrepancies were resolved by discussion and a third reviewer was involved (LL) if consensus was not reached.
Charting the Data
Previously reported RA-specific participation factors from semi-structured interviews were used to develop the first draft of the data extraction sheet (Supplemental Material 2). 30 A virtual meeting was held with the seven patient and healthcare professional partners to refine the data extraction sheet. Partners also suggested distinguishing recommendations based on individual characteristics such as age, disease severity, and strength training experience. An updated draft of the data extraction sheet was circulated by email to patient and healthcare professional partners for edits and approval. JM and MW independently and iteratively extracted information from the first seven articles and reached consensus on both the data extracted and the process of extraction. MW charted the remaining articles and JM checked for accuracy.
The following data were extracted from each article: year of publication, article title, type of article, number of studies analyzed (if a review), countries represented by authorship team (all represented countries were considered for articles with multi-country collaboration.), article objective, target audience, prescription parameters, recommendations that address strength training participation factors (knowledge, memory, stiffness, pain, flares, fatigue, joint deformities, co-morbidities, fluctuating nature of the disease, fear of causing further damage, motivation, access to resources, sleep, mental health, medication side effects, other), recommended adaptations based on individual characteristics (age, disease severity, strength training experience), and suggested future research directions. The Association of the Scientific Medical Societies Guidance Manual and Rules for Guideline Development was used to classify any identified guidelines as (a) a systematic literature review including a subsequent synthesis of the evidence and a structured consensus process completed by a representative committee (S3), (b) a systematic literature review and synthesis of the evidence only (S2e), (c) a structured consensus process completed by a representative committee only (S2k), or (d) an informal consensus process by a group of experts (S1). 31 The full data extraction sheet can be found in Supplemental Material 3.
Quality Appraisal
All guidelines (including expert recommendations, evidence-based guidelines, and consensus-based guidelines) were assessed using the Appraisal of Guidelines for Research and Evaluation Instrument (AGREE II). 32 It contains 23 items encompassing 6 domains including scope and purpose, stakeholder involvement, rigor of development, clarity of presentation, applicability, and editorial independence. 33 The quality of systematic reviews was evaluated using the 16-item AMSTAR 2 tool (A Measurement Tool to Assess systematic Reviews). 34 Narrative reviews were not evaluated with AMSTAR 2. AMSTAR 2 has yielded evidence of acceptable inter-rater agreement for most items when tested on a sample of 54 systematic reviews across 3 pairs of raters. 34 AGREE II and AMSTAR 2 scoring was done independently by JM and MW, and discrepancies were resolved through discussion. LL acted as a third reviewer to resolve discrepancies. While not appraised for quality, recommendations that were supported by sources other than guidelines or systematic reviews (e.g., non-systematic reviews) were flagged as limitations in the discussion.
Summarizing and Reporting the Findings
Descriptive analysis was conducted on article characteristics. Key findings and recommendations were categorized into factors that affect strength training participation by the core research team (MW, JM, and LL). These recommendations and their categorizations were presented to patient and healthcare professional partners to ensure relevance to end-users.
Results
Characteristics of Included Studies
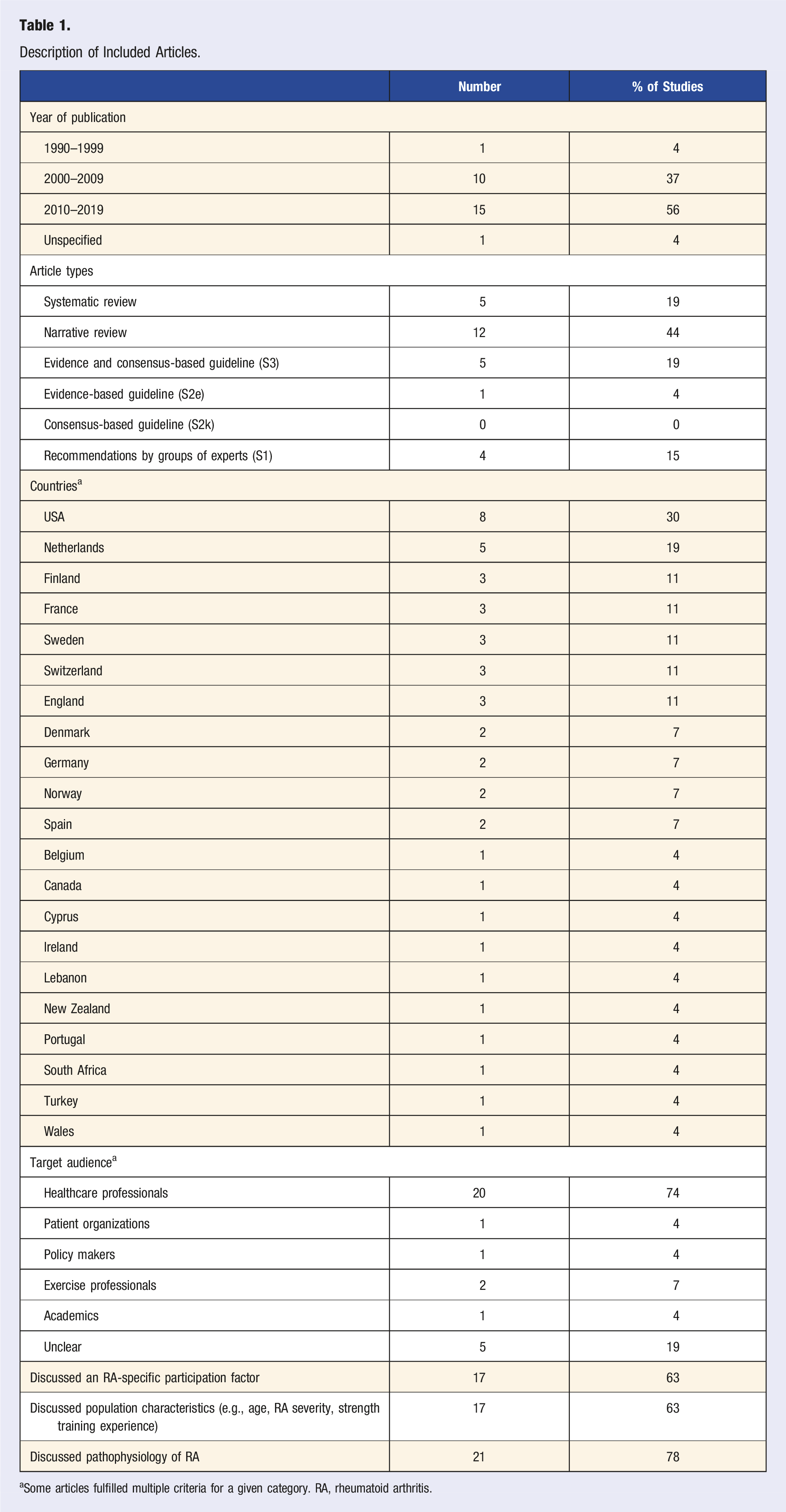
The search strategy retrieved 266 articles, 160 of which were screened for title and abstract. Of those, 101 were excluded with 59 articles proceeding to full text review. 32 full text articles were not eligible, leaving 27 articles eligible for review (Figure 1). Articles included in this scoping review were published between 1996 and 2019, with the majority (n = 15) published in 2010 or later (Table 1). Of the 27 articles, there were 12 narrative reviews, 5 systematic reviews, 5 consensus-based guidelines, 4 expert recommendations, and 1 evidence-based guideline. The majority of articles were targeted towards healthcare professionals (n = 20). Our full data extraction sheet is found in Supplemental Material 3. PRISMA Flow Diagram. Description of Included Articles. aSome articles fulfilled multiple criteria for a given category. RA, rheumatoid arthritis.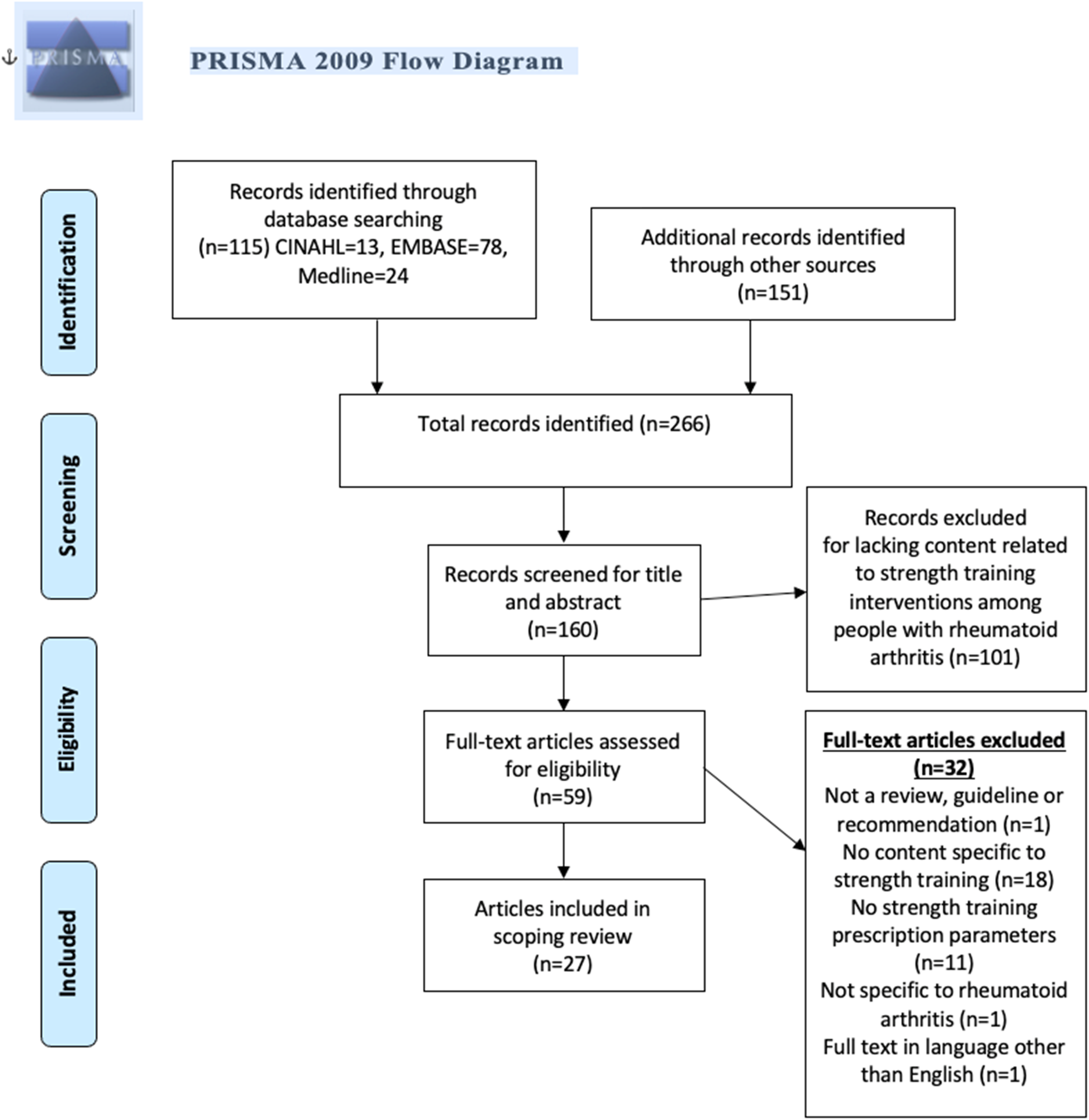
Recommendations for Tailoring Strength Training Prescriptions for People with RA
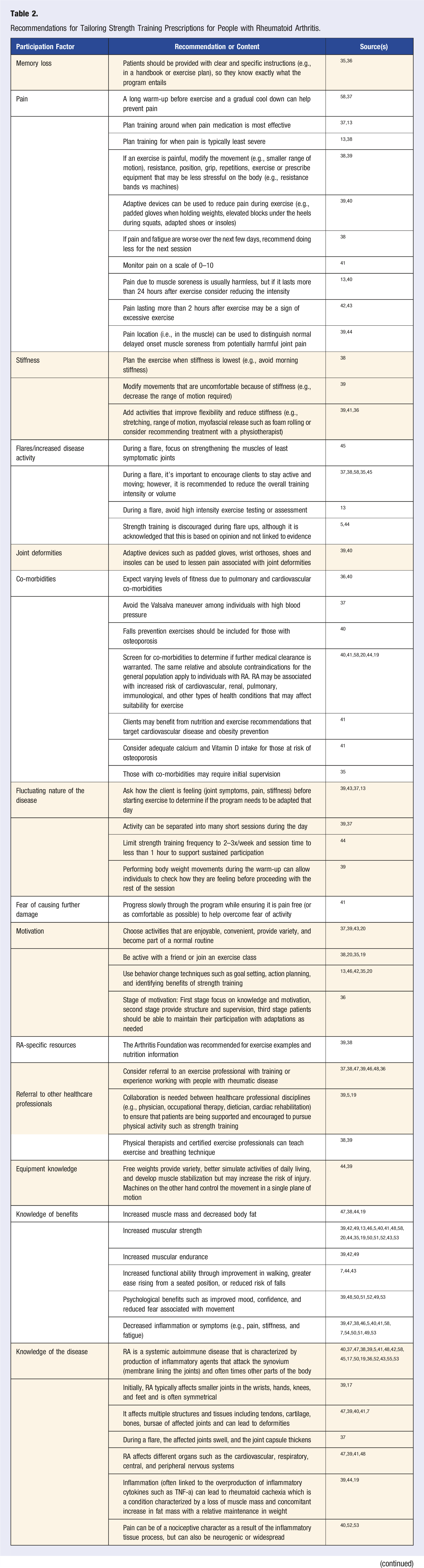
Recommendations for Tailoring Strength Training Prescriptions for People with Rheumatoid Arthritis.
Strength training prescription recommendations based on individual characteristics.
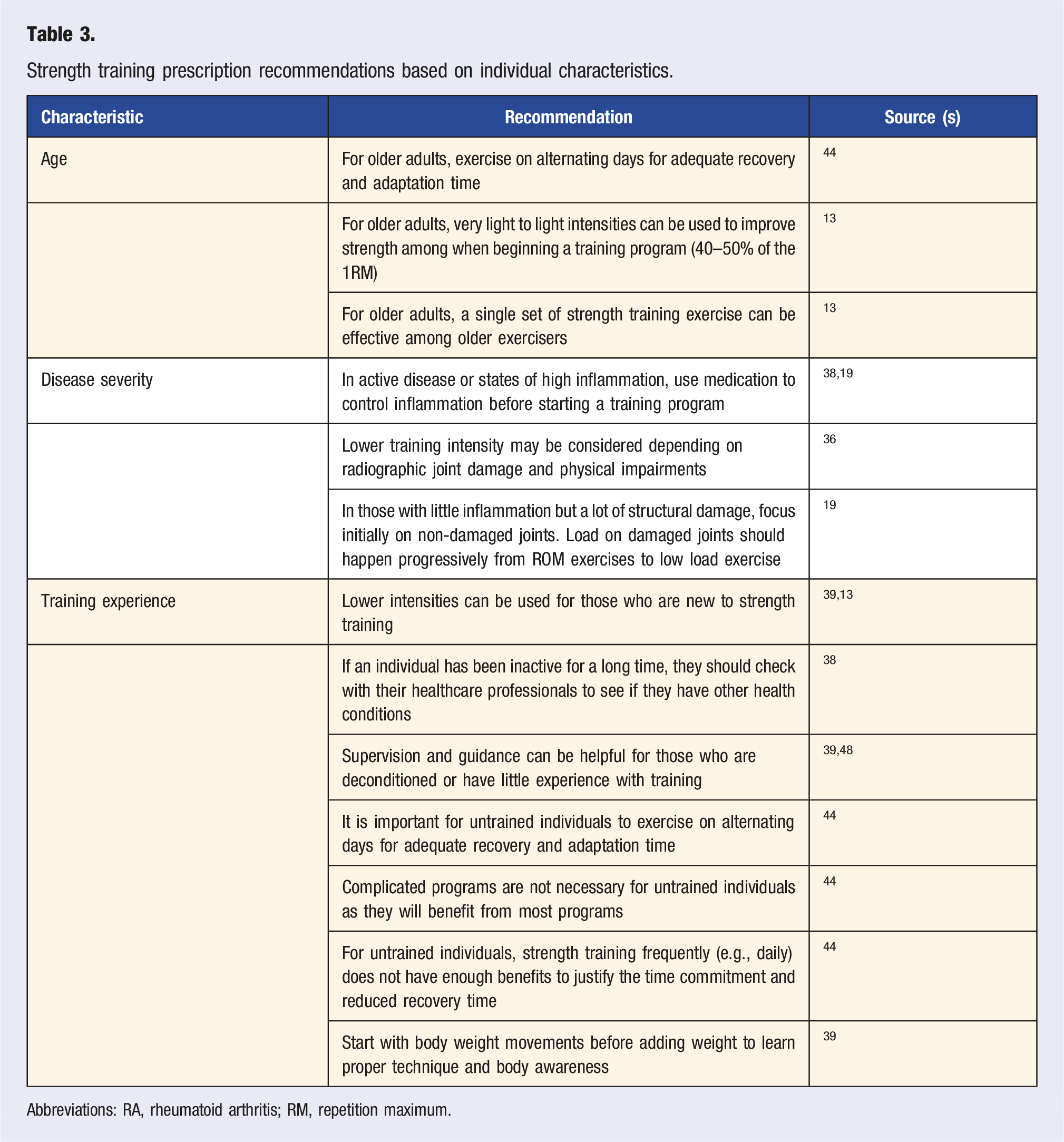
Abbreviations: RA, rheumatoid arthritis; RM, repetition maximum.
Box1. Summary of recommendations for tailoring strength training prescriptions for clients with rheumatoid arthritis
1. Provide education and resources to support clients’ knowledge of the disease and benefits of strength training. 2. Clear and documented instructions for the exercise prescription should be provided in case the client is experiencing symptoms that cause memory loss or “brain fog.” 3. Screen for co-morbidities and ensure contraindications and cautions to specific co-morbidities are incorporated into the program. For example, avoid the Valsalva maneuver among individuals with high blood pressure. 4. Use adaptive or protective devices such as padded gloves, splints, or adapted shoes to help the client exercise move comfortably, especially with joint deformities. 5. Schedule sessions around peak effectiveness of medication or when symptoms (e.g., pain) are least severe. 6. Strength training can be continued at a lower intensity during a flare, and focus on exercises that involve the least symptomatic joints. Therefore, high intensity exercise testing (e.g., 1 repetition maximum) should be avoided. It may be helpful to have a plan for flare and non-flare days. 7. Ask or assess how the client is feeling (e.g., joint symptoms, pain, stiffness) at the beginning and throughout the session to determine if the program needs to be adapted. 8. Offer variety/adaptability in type of equipment and exercises, range of motion, volume, progression, and frequency in the strength training program. 9. Include a warm-up that increases blood flow to the working muscles and improves safe range of motion. The warm-up can be used to help the client gauge the current disease status that day and to mitigate existing pain and stiffness. 10. Monitor symptoms for a few days after the session to inform whether intensity needs to be decreased in the next session. 11. Pain location (i.e., in the muscle) may be used to help distinguish normal delayed onset muscle soreness pain from potentially harmful joint pain. 12. To help maintain the program, progress slowly to help overcome fear of being active, incorporate activities that the client enjoys, are convenient, and provide variety. Suggest exercising with a friend or joining a group class, and use behavior change techniques such as goal setting and action planning to help your client stick to their goals. 13. If the client’s needs for strength training exceed the clinician’s scope and experience, the client should be referred to a more appropriate exercise professional.
Quality Appraisal
Guidelines
Mean AGREE II Domain Scores for Guidelines a
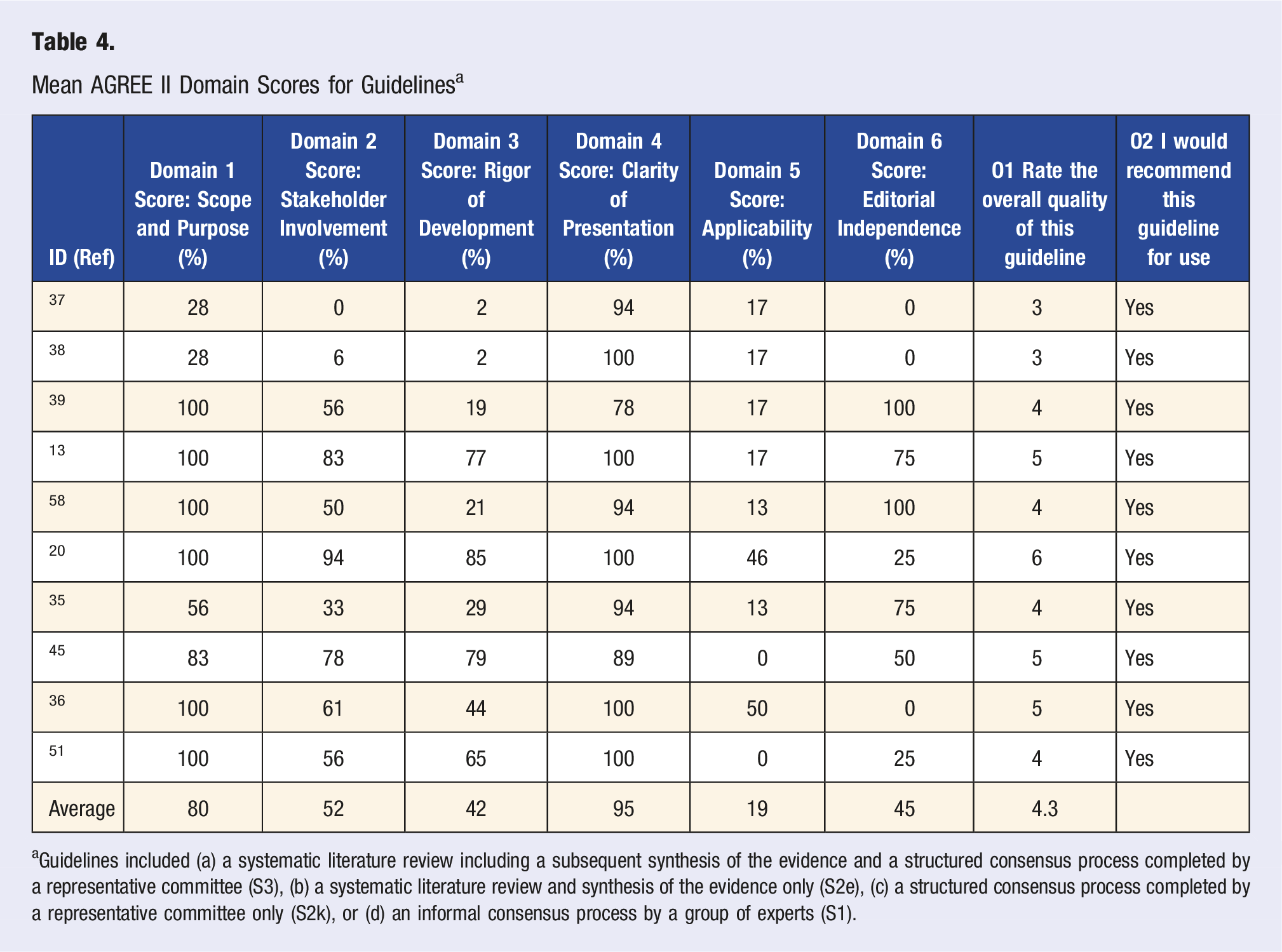
aGuidelines included (a) a systematic literature review including a subsequent synthesis of the evidence and a structured consensus process completed by a representative committee (S3), (b) a systematic literature review and synthesis of the evidence only (S2e), (c) a structured consensus process completed by a representative committee only (S2k), or (d) an informal consensus process by a group of experts (S1).
Systematic Reviews
AMSTAR-2 Assessment of Systematic Reviews According to Critical Domains.
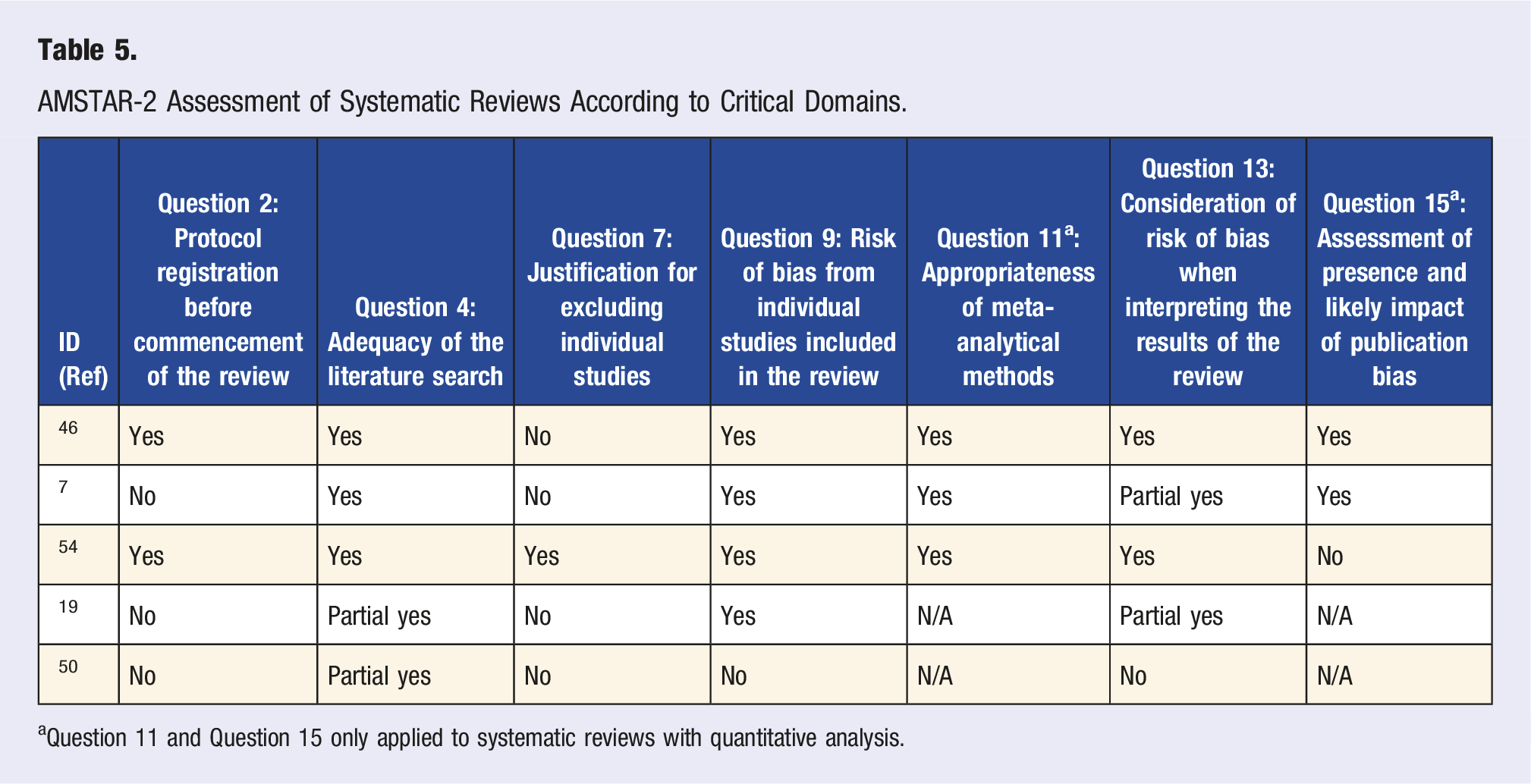
aQuestion 11 and Question 15 only applied to systematic reviews with quantitative analysis.
Discussion
Recommendations for Tailoring Strength Training Prescriptions for People with RA
This review highlights available recommendations for tailoring strength training prescriptions for people with RA. Findings span recommendations that address an individuals’ capability, opportunity, and motivation to participate in strength training. 56 While the scope of recommendations to address participation factors (e.g., barriers and facilitators) was diverse, no single article addresses the full range of factors that affect strength training participation among people with RA. This is supported by the finding that “applicability” of the reviewed literature, which considers the extent that articles provide tools for application and discuss practical considerations such as barriers to implementation, was the lowest-scored AGREE II domain. 33 Furthermore, many participation factors (e.g., sleep, fatigue, medication side effects, mental health status) lack evidence for recommendations that adequately target these in the context of strength training.
Clarifying Pain Recommendations
Recommendations regarding pain monitoring were at times conflicting. Pain duration was recommended to be monitored with both 2 hours42,43 and 24 hours suggested as a threshold for when to be concerned about pain.13,40 Of note, the 24-hour threshold is supported by a guideline 13 that scored high on the AGREE-II rigor of development domain, while other sources were non-systematic reviews. However, neither recommendation was grounded in empirical evidence. Not only is the range of recommendations for acceptable pain duration post strength training confusing and untested, these recommendations conflict with evidence on delayed onset muscle soreness (DOMS). DOMS is a type of pain that appears 12 to 48 hours after exercise but is considered to be normal, self-limited, and not necessarily a reflection of undesirable damage.57–60 This means that timelines for potentially harmful pain and normal DOMS-related pain overlap, potentially creating confusion if pain duration recommendations are not paired with further indicators to distinguish acceptable vs harmful pain. For example, to distinguish harmful pain from typical post strength training pain, recommendations included the use of pain location to distinguish joint pain from expected strength training muscle soreness such as DOMS.39,44 Therefore, clarity is needed to contextualize pain monitoring recommendations to prevent confusion or fear amongst people with RA participating in strength training.
Using Assessment to Guide Safe and Appropriate Prescription
Many of the included recommendations suggested using symptoms to guide strength training prescription, but specifics on how to use findings from symptom assessment to inform prescriptions were lacking. For example, it was recommended to assess joint symptoms, pain, and stiffness to determine whether the program needs adaptation on a given day.37,39,43 Using the warm-up was also recommended to assess how the patient is feeling. 39 Disease activity and symptom fluctuation is a common experience amongst individuals with RA 61 and a challenge for prescribing strength training, although little evidence is available to guide practice. 30 Assessment of other factors beyond disease activity and symptoms may also be important for supporting clients in strength training participation. Recommendations from the European League Against Rheumatism (EULAR) advise comprehensive assessments of physical, social, and psychological factors to adapt programs. 13 Likewise, evidence on which factors to assess and how to assess them in the context of strength training has not been described to date. This practice is still in its infancy and further research is needed on what assessments can be used to individualize and adapt strength training prescriptions. In the interim, this process will require ongoing trial and error and collaboration between professionals and their patients.
Patient-Level Factors Remaining to be Addressed
Strength training research and recommendations would benefit from exploring how factors such as sleep, mental health status, fatigue, and medication side effects can be managed to facilitate participation in strength training. The broader literature acknowledges these RA-specific participation factors and their interconnected relationship.36,62–67 Fatigue has been shown to be associated with mental well-being and sleep disturbance in patients with RA. 68 Also, medications such as methotrexate and prednisone can be associated with side effects including fatigue and sleep disturbance, as well as weight gain, respectively.64,69 Many of the included articles in this scoping review noted strength training’s positive effects on mental health and emotional status.39,50,51 However, previous work on general physical activity has acknowledged the potential role of addressing mental health early in the program so that patients with RA can experience these mental health benefits. 18 Overall, these participation factors have complex relationships amongst themselves and with strength training. Future research should explore how to optimally prescribe strength training in the face of these complex participation factors while considering the unique interconnected relationships at play.
Strengths/Limitations
A few limitations must be acknowledged. First, the inclusion criteria of guidelines, recommendations, and reviews precludes the ability to examine the evidence of relationships between the prescription recommendations and strength training participation. In other words, it is unclear whether applying these recommendations for strength training prescription leads to increases in strength training participation. This may be an area for future research. Second, the broad nature of the research question required including articles of variable quality. This resulted in some conflicting statements in Table 2 which summarizes prescription recommendations made in each article. To address this issue, the summary of recommendations has been contextualized within the quality of their sources in the discussion where appropriate and the use of the AGREE II or other guidelines are encouraged to promote higher methodological quality in future research or guidelines. Third, only articles with full text written in English were included meaning articles in other languages may have been excluded. A strength of this scoping review was the use of an integrated knowledge translation approach, engaging both patient and healthcare professionals throughout the review process, helping improve the relevance to patients with rheumatologic conditions and their healthcare professionals.
Conclusion
This review summarizes recommendations for practitioners to tailor RA-specific strength training prescriptions. The physical, psychological, and social factors that affect strength training participation in individuals with RA makes prescribing strength training a complex and multi-faceted endeavor. Indeed, providing information on strength training prescription parameters needs to be paired with how to deliver strength training in the face of these multi-faceted participation factors. Addressing the identified areas for future research may better equip healthcare professionals to usefully prescribe and support patients with RA to experience the many benefits of strength training.
Supplemental Material
Supplemental Material - Tailoring Strength Training Prescriptions for People with Rheumatoid Arthritis: A Scoping Review
Supplemental Material for Tailoring Strength Training Prescriptions for People with Rheumatoid Arthritis: A Scoping Review by Michael L. Wu, B.Kin, Jasmin K. Ma, PhD, B.Kin, Karen Tsui, BSc(PT), Alison M. Hoens, MSc, BSc(PT), and Linda C. Li, PhD, BSc(PT) in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental Material - Tailoring Strength Training Prescriptions for People with Rheumatoid Arthritis: A Scoping Review
Supplemental Material for Tailoring Strength Training Prescriptions for People with Rheumatoid Arthritis: A Scoping Review by Michael L. Wu, B.Kin, Jasmin K. Ma, PhD, B.Kin, Karen Tsui, BSc(PT), Alison M. Hoens, MSc, BSc(PT), and Linda C. Li, PhD, BSc(PT) in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
We would like to thank Jon Collins, Eileen Davidson, Sadiq Jiwa, Shanon McQuitty, and Louella Sequeira for their considerable time and expertise in review question conceptualization, developing the review methodology, and interpretation of the results.
Author’s Contributions
MW was responsible for developing the review methodology, data screening and extraction, interpretation of the results, and writing and review of the manuscript. JM was responsible for review question conceptualization, developing the review methodology, data screening and extraction, interpretation of the results, and writing and review of the manuscript. KT and AH were responsible for review question conceptualization, developing the review methodology, interpretation of the results, and review of the manuscript. LL was responsible for review question conceptualization, developing the review methodology, interpretation of the results, and writing and review of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jasmin Ma is supported by the Michael Smith Foundation for Health Research Trainee Award (#17936), the Arthritis Society Post-Doctoral Fellowship (TPF-18-0209), and the Canadian Institute of Health Research Post-Doctoral Fellowship (201910MFE-430114-231890). Linda Li is supported by the Harold Robinson/Arthritis Society Chair in Arthritic Diseases award, the Canada Research Chair Program, and the Michael Smith Foundation for Health Research Scholar Award. Funding bodies did not play a role in the study collection, analysis, interpretation of the data, or writing of the manuscript.
Availability of Data and Material
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.