
Abstract
Latina and Black/African American (AA) women report disproportionately low levels of muscle-strengthening activities (MSA) and high rates of related chronic health conditions. Despite the health benefits of MSA, physical activity intervention research in these populations has focused mostly on increasing aerobic physical activity. The purpose of this review was to describe the current state of scientific literature on MSA interventions among Latina and Black/AA women. Two electronic databases, CINAHL and PubMed, were searched for studies published during the past 10 years. Studies were included in this review if they reported promotion of MSA, included at least 50% Latina and/or Black/AA women in their samples, and used an interventional design. Search procedures identified 8 unique interventions targeting MSA in Latina (n = 3) and Black/AA women (n = 5). Results revealed there is limited published research on MSA promotion among Latina and Black/AA women, especially on theory-based interventions that address psychosocial and behavioral influences of MSA, as well as assessment of MSA outcomes in these populations. This review highlights a critical need for research on culturally tailored behavioral interventions to reduce the low MSA in Latina and Black/AA women and provides future research directions on this topic.
“MSA components in all studies primarily focused on supervised instruction on MSA via classes and one-on-one sessions.”
Introduction
Physical inactivity is a leading risk factor for global mortality and a critical public health problem in the U.S.1,2 Engaging in physical activity (PA) is a modifiable behavior that helps prevent and manage many chronic health conditions (e.g., type 2 diabetes, heart disease and stroke, obesity, and some cancers), strengthens bones and muscles, and improves mood. 3 To achieve the health benefits associated with regular PA, national PA guidelines 3 recommend that adults engage in 150 minutes/week of aerobic moderate-to-vigorous PA (MVPA) and muscle-strengthening activities (MSA) that work all major muscle groups on two or more days per week. While earlier PA recommendations emphasized primarily aerobic activities, the current guidelines now include MSA recommendations due to the growing body of evidence on the health benefits of MSA. For instance, MSA has been independently associated with reduced risk for cancer-related and all-cause mortality,4,5 improvements in Hemoglobin A1c levels, 6 increases in lean muscle mass, 7 and reduced risk of osteoarthritis, osteoporosis, and osteopenia 8 which is particularly important for women given the increased risk of post-menopausal bone loss.9,10
Despite the health benefits of MSA, most women in the U.S. do not engage in MSA at nationally recommended levels. This is especially evident among Latina and Black/African American (AA) women, who report the lowest levels of MSA engagement compared to other demographic groups. Only 18% of Latina and 13% of Black/AA women meet the full PA guidelines (aerobic PA and MSA) compared to 22% of non-Latina females and 28% of Latino and Black/AA males. 11 Moreover, the disproportionate prevalence of cardiometabolic disease and overweight/obesity in these populations11,12 indicates an urgent need for interventions that help Latinas and Black/AA women achieve the full PA guidelines (aerobic and MSA).
Increasing MSA levels of Latina and Black/AA women will require behavioral interventions that address culturally relevant factors influencing MSA. Such approaches, commonly referred to as culturally tailored interventions, are designed to address the observable characteristics, sociocultural norms, values, beliefs, and behaviors of the study populations in which they are designed and are believed to be more effective at achieving desired behavior changes than non-culturally tailored interventions.13–15 Prior culturally tailored PA interventions for Latina and Black/AA women have predominantly focused on increasing aerobic PA (e.g., walking, dancing, and other moderate-to-vigorous intensity activities), with limited focus on MSA.16–22 While these interventions addressed sociocultural factors influencing PA (e.g., language barriers, body shape preferences, hair care concerns, fear of immigration enforcement, lack of time due to family caretaking), influences of MSA among Latina and Black/AA women may be different than aerobic PA. For example, barriers to MSA in women include the fear of becoming overly muscular or appearing masculine, gender-based stigma, discouragement from family members and others, and the perception that MSA is an activity for men.23,24 Women have also reported feeling deterred from using strength equipment at gyms as they felt intimidated and out of place in spaces dominated by men. 25 Moreover, performing MSA requires specific knowledge and skills that differ from aerobic activities (e.g., knowing what exercises to do, how to do them correctly, number of sets and repetitions, and how to avoid injuries), as well as the inclusion of measures specifically designed to assess MSA outcomes (e.g., changes in muscle strength; self-reported frequency, duration and type of MSA performed).
Given that PA intervention research among Latina and Black/AA women has focused mostly on increasing aerobic PA, further knowledge is needed on how to effectively help Latina and Black/AA women increase MSA levels. Thus, we conducted a search of literature on interventions that promote MSA among these populations. The purpose of this paper is to: (1) describe the current state of scientific literature on behavioral interventions that promote MSA in Latina and Black/AA women, and (2) provide directions for future research on this topic.
Methods
Studies were included if they met the following eligibility criteria: (1) published in a peer-reviewed journal between January 2013 and May 2023; (2) reported promotion of MSA in intervention; (3) included at least 50% Latina and/or Black/AA women ages 18 years and over in the study population, and (4) used an interventional design, including single group, randomized, nonrandomized, and quasi-experimental studies. Studies that focused on PA promotion alone, as well as those targeting multiple health behaviors (e.g., healthy eating, weight loss, smoking) that included PA were eligible for inclusion if MSA was reported as a behavior targeted by the intervention. Studies focused on healthy individuals or populations with existing health conditions (e.g., diabetes, cancer survivors) were also included; however, studies that focused on PA promotion as a rehabilitation treatment for surgery or for an acute health condition were excluded (e.g., rehabilitation after knee surgery or cardiac procedures) as these interventions focus primarily on short-term recovery rather than lifestyle modification. No other inclusion or exclusion criteria were applied.
Two electronic databases were searched, PubMed and CINAHL. The Boolean search strategy was used to identify relevant articles using terms focused on 2 broad topical areas: (1) study population, and (2) behavior targeted by the intervention. Search terms for study population included: Latina or Hispanic, African American or Black, Latinx, and Women. Search terms of behavior targeted by the intervention included physical activity, exercise, muscle-strengthening activity, resistance exercise, resistance training, fitness, weight training, intervention, and program. An example of a search string included: “(Hispanic OR Latin* OR Black Americans OR African Americans), AND (muscle-strengthening OR resistance training OR exercise), AND (intervention OR program).” Appendix 1 includes all search strings used during electronic database searches. To refine the search, articles were sorted using “best match” or “sort by relevance” options, then the 200 most relevant articles in each database were screened (screening stopped at 200 because no more relevant articles were identified).
Search procedures were conducted from May-June 2023 by a single author (NB) following a consultation with an expert research librarian to develop the search strategies for both databases. All articles retrieved during search procedures were imported into EndNote reference management software (NB). Once duplicates were removed, 2 authors (NB, AS) independently screened titles and abstracts and classified them as either “potentially eligible” or “not eligible.” Those identified as “potentially eligible” subsequently received full text review to determine eligibility by 2 additional reviewers (TvA, TB). Any disagreements between the 2 reviewers regarding inclusion or exclusion criteria were resolved by the 2 reviewers reaching consensus. The search procedure and article elimination process is further described in the consort diagram
26
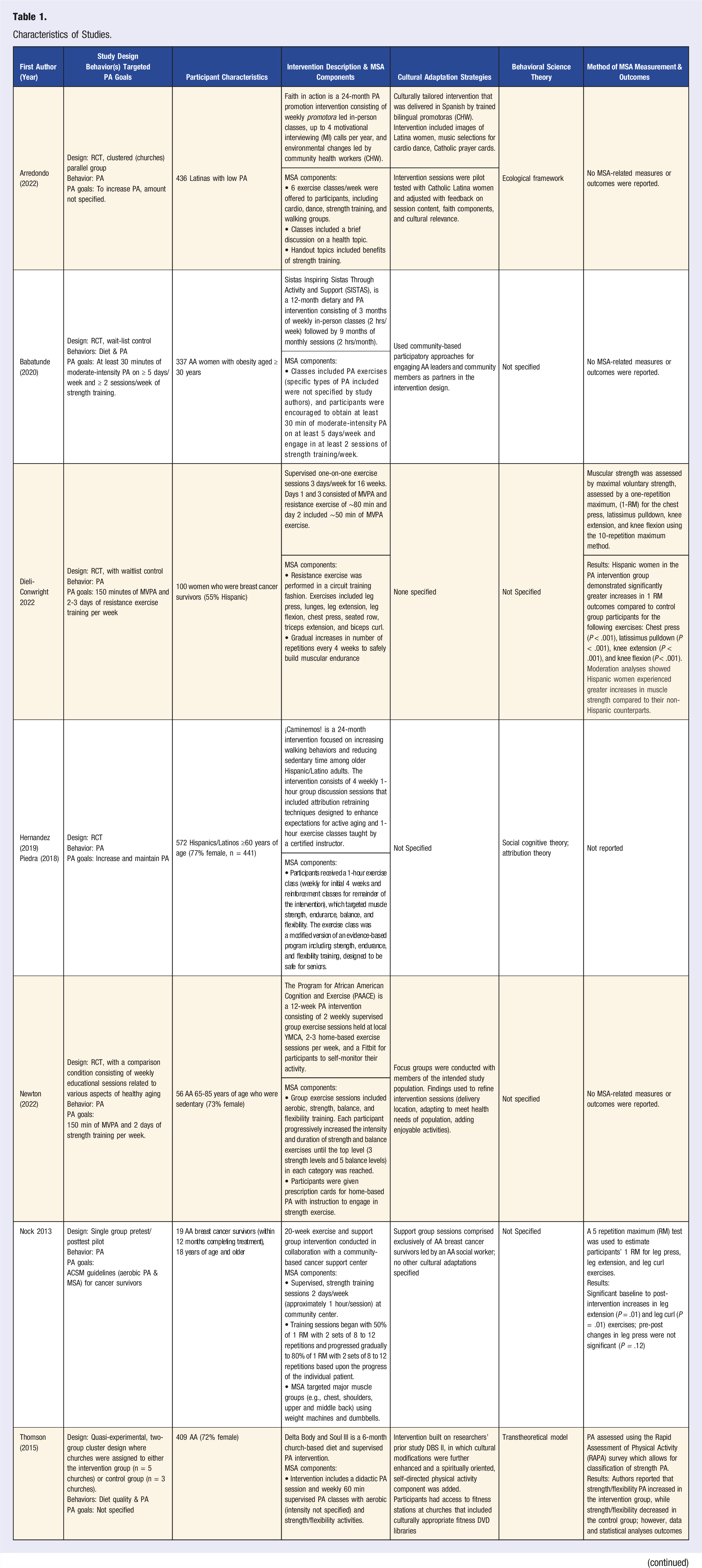
(Figure 1). Data extracted from the study included: (a) publication citation, (b) study design, (c) behaviors targeted by the intervention, (d) inclusion of PA goals, (e) participant characteristics, (f) intervention description, study duration, and MSA components (i.e., intervention activities that were used to promote MSA, such as exercise classes or goal setting sessions on MSA), (g) cultural adaptation strategies (i.e., strategies used to culturally adapt/tailor the intervention for Latina or Black/AA women, such as inclusion of study materials that address concerns about body size ideals or perception of MSA as a masculine activity or avoided topic in culture), (h) application of behavioral science theory, and (i) MSA measurement (i.e., tools used to measure MSA, such as self-reported questionnaires on type and amount of MSA performed, or objective measures of muscle strength) and outcomes (outcomes of MSA measures reported in the study). Literature search and article elimination process.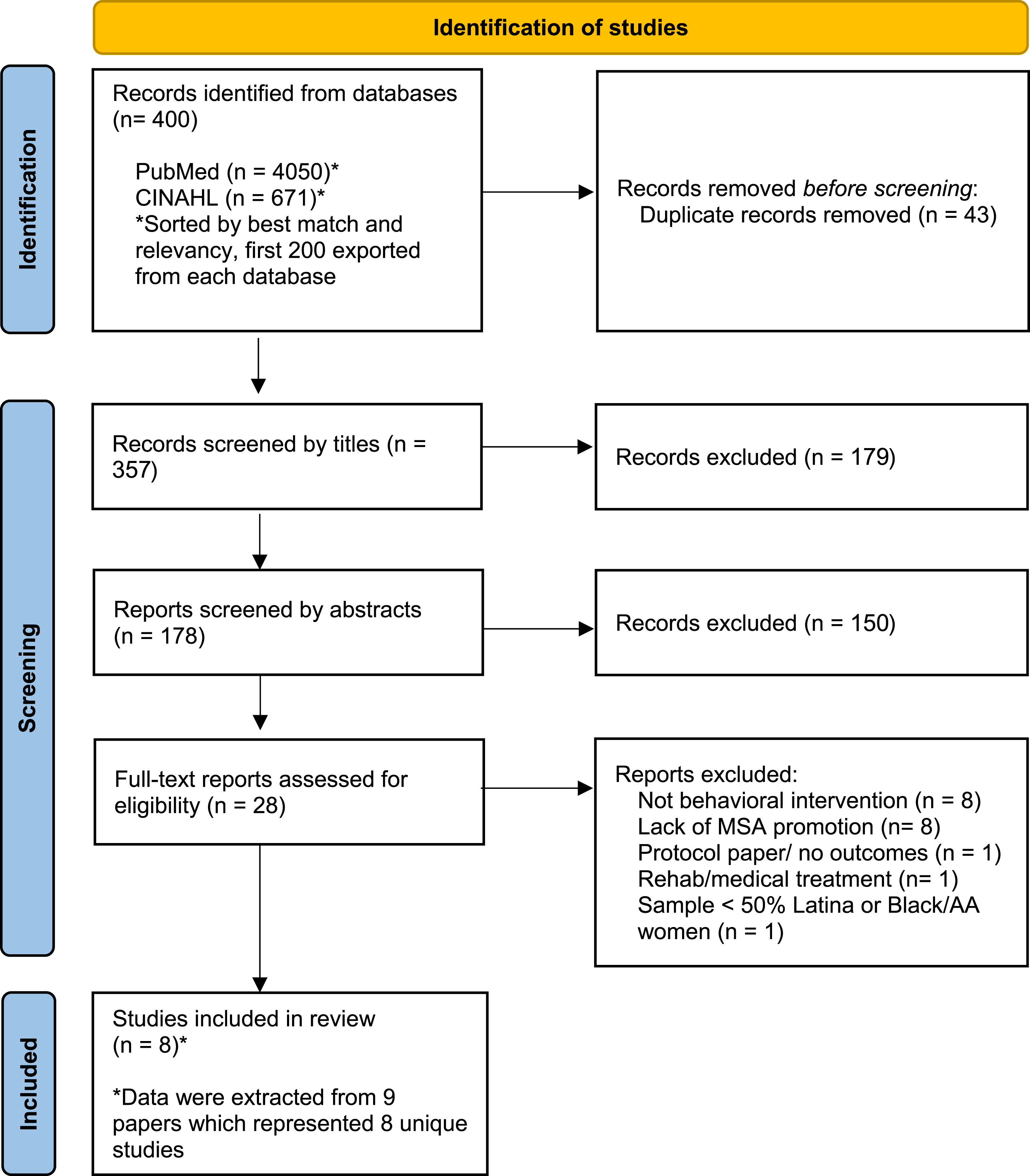
Results
Characteristics of Studies.
Study Population Characteristics
A total of 2128 participants ranging from ages 18-85 years were represented across the 8 studies included in this review, including 1758 Latina and Black/AA women. Study samples were comprised of Black/AA men and women (n = 2), exclusively of Black/AA women (n = 3), Latino men and women (n = 1), exclusively Latina women (n = 1), and 1 study included both Latina and non-Latina women. The majority of studies focused on populations who reported low levels of PA or sedentary behavior,22,27,28 and were overweight or obese.29-31 Two studies focused on breast cancer survivors who were within at least 6 or 12 months of completing treatment.26,32
Study Design, Setting, and Duration
More than half of the studies employed randomized controlled trial designs (n = 5). Two of these studies employed a waist-list control design, 32 one study included a non-PA focused wellness control group, 33 and 1 study utilized a randomized cluster design. 29 Among the remaining 3 studies, 2 utilized a single group pretest/posttest design29,34 and 1 used a quasi-experimental nonrandomized design which assigned churches to either the intervention or control arm. 31 Interventions were delivered at community-based centers,30,34,35 a YMCA, 27 churches,28,31 a Clinical Exercise Research Center at a university, 32 and 1 home-based intervention provided participants with access to community sites with exercise equipment and coaches. 29 Duration of studies ranged from 12 weeks to 24 months.
PA Goal of Studies
The behavioral target of most studies (n = 5) was for participants to achieve national PA guidelines for both aerobic MVPA and MSA. Two studies reported a general goal of increasing PA, but did not specify the target amount of PA,28,35,36 and the other study did not report a PA goal 31 for participants to achieve. Of the 5 studies that recommended achieving national PA guidelines, three27,32,34 did not report meeting MSA guidelines as an outcome (i.e., MSA performed on two or more days/week), rather they included in-person exercise sessions that were designed for participants to achieve national MSA guidelines, and two29,30 included both in-person and home-based interventions recommending PA guidelines, but did not assess meeting guidelines as an outcome.
MSA Promotion Strategies
Nearly all studies (n = 7) included in-person instruction on MSA either through group classes/exercise sessions27,28,30,31,34–36 or one-on-one supervised exercise sessions. 32 One home-based study 29 provided participants with access to community sites that had exercise equipment (e.g., weight machines, free weights) and coaches were available to assist them with performing MSA. Additional MSA intervention components utilized by studies included informational handouts (e.g., benefits of MSA),27–29 providing participants with individualized exercise prescriptions (e.g., prescription cards given to participants; 27 individually tailored exercise prescriptions), 29 and giving participants equipment to perform MSA at home (i.e., resistance bands). 29
Use of Behavioral Theory
Only 3 of the 8 studies reported the use of a behavior change theory or model underpinning intervention content. Arredondo et al, 28 followed an ecological framework to influence potential mediators of PA change at multiple levels of influence, including individual (i.e., in-person PA classes held at or near churches, monthly health flier mailings), interpersonal (i.e., telephone-based motivational interviewing, PA class reminders), organizational (i.e., announcements at mass/ministry meetings, inclusion of PA class schedule in church bulletin, presentations at church fairs, space allocated for PA classes), and environmental (i.e., church and neighborhood improvement projects). Thomson et al, 31 incorporated concepts of the Transtheoretical model to inform decisional balance and increase self-efficacy and social support for PA through the use of didactic educational sessions. These sessions focused on discussing the benefits and recommendations for PA engagement, as well as strategies to overcome PA barriers. Hernandez et al 36 and Piedra et al 35 combined attribution theory and social cognitive theory to develop a curriculum for the ¡Caminemos! intervention. The curriculum (delivered by trained health facilitators) focused on the concept that becoming physically inactive should not be an expected part of aging and included activities such as identification of PA barriers and reframing barriers, establishing action plans to increase PA, logging PA.35,36 Notably, the extent to which the theory-driven activities included in all of these studies focused on MSA behaviors, as opposed to PA in general, was not readily discernible based on the description of the interventions provided by study authors.
Cultural Adaptation
Four studies reported using strategies to adapt their interventions for their target population. These modifications include: (1) focus groups to refine the intervention sessions (inform the delivery location, adapting sessions to meet health needs of population, adding enjoyable activities), 27 (2) engaging AA leaders and community members in the intervention design, 30 (3) intervention sessions that were previously pilot tested and refined for content and cultural relevance, and incorporated images of Latinas, music selections, and Catholic prayer cards, 28 and (4) enhancing a prior intervention with cultural modifications and adding a spiritually orientated, self-directed PA component. 31 One study 29 enhanced the authors’ previous trial with high-risk AA families by delivering the intervention in community sites and adding personal exercise coaches, easy access to community sites, and social support (via observing others exercising). The remaining 3 interventions for Latina and non-Latina women, 32 Latino adults,35,36 and AA breast cancer survivors 34 did not report cultural adaptation strategies (although the Nock et al intervention was delivered in a community center because AA may prefer community-based programs).
Method of MSA Assessments and MSA Outcomes
Although all studies included in this review had a focus on promoting MSA, only 3 reported MSA-related study assessment measures and associated outcomes. MSA outcomes for 2 studies included maximum voluntary strength, as assessed by either a single repetition maximum (RM) 32 or a 5 RM. 34 One study 31 assessed self-reported MSA outcomes via the Rapid Assessment of Physical Activity (RAPA) survey which contains a single question asking whether participant performed MSA on 1 or more days during the week. 37 Results for the 2 studies assessing maximum voluntary strength reported significant increases in muscle strength for 1 or more of the muscle groups targeted (see Table 1). Authors of the study using the RAPA to assess self-reported MSA engagement reported that strength/flexibility activities increased in the intervention group and decreased in the control group; however, no data were reported to support this conclusion.
Assessment of Participants’ MSA Experience
One of the 8 studies in this review reported assessment of participants’ experience with MSA components. While the authors of this study did not provide explicit experiences about the strength training component of the physical activity group (PAG), participant satisfaction scores were high and most PAG participants (70%) reported that the intervention helped them increase engagement in exercise or motivated them for regular exercise. Suggestions (primarily from 1 participant) for improving the intervention consisted of including more variation of exercises and upper body exercises, removing a particular exercise (i.e., squats), providing more instruction, and adding cognitive and nutrition intervention components.
Discussion
Despite the low MSA levels and related health disparities in Latina and Black/AA women, our findings revealed that there is limited published literature on behavioral interventions that promote MSA in these populations. While Latina and Black/AA women have expressed interest in learning how to increase their MSA,24,38 few interventions were identified in this review that targeted or were culturally tailored exclusively to Latinas or Black/AA women.
Interventions that are developed or adapted exclusively for Latina or Black/AA women are important for addressing sociocultural factors influencing engagement in MSA and can increase relevance, appeal and salience compared to non-culturally tailored interventions. 13 Nearly all studies in this review included cultural adaptations for their target population; however, the extent of cultural adaptations reported varied. Interventions commonly included “surface level” adaptations, referring to observable characteristics of a target population that are incorporated into the intervention, 13 including delivering at community-based locations,27-31,34 providing the intervention in Spanish, 28 incorporating images of women from the target population, and using community health workers. 28 A select few studies also reported the use of “deep structure” adaptations, which involve a more in-depth understanding of sociocultural, environmental, psychological factors that influence a behavior, 13 such as incorporating religion/faith-based components into the intervention. 28 Future investigation should focus on identifying individual, social, and environmental influences of MSA, particularly “deep structure” factors that limit participation in MSA (e.g., MSA is an avoided topic in social circles, perceived as an activity for men 24 ) and addressing these in MSA interventions.
While previous theory-driven aerobic PA interventions have shown success in increasing aerobic PA among Latina and Black/AA women,19,20,22,39 the majority of studies in this review did not specify the use of a theoretical framework. Among the 3 studies that included a theoretical framework, theory-driven activities were focused on general PA promotion rather than MSA promotion. For instance, 1 study in the review included the Transtheoretical Model 40 —a theory used to promote individual behavior change that has been commonly used in MVPA research,41-44 and another intervention followed an ecological framework—which focuses on the dynamic interrelationships between social and environmental factors, but does not include theoretical constructs of behavior change. Another study35,36 combined attribution theory with social cognitive theory to develop a curriculum for reducing sedentary time and enhancing expectations for active aging in older adults. Behavioral theory provides a framework for designing, implementing, and evaluating public health interventions. 45 Interventions that are grounded in behavior change theory are essential for understanding the mechanisms in which change occurs and may be more effective at changing behavior than nontheory-based interventions.46,47 Thus, findings from this review suggest that further research is necessary to develop theory-based interventions promoting MSA in Latina and Black/AA women; these studies should provide a description of how theoretical concepts were applied to MSA activities. Given the limited research on MSA in these populations, there is a need for formative research to identify potential theory-based mediators of MSA (e.g., social support, self-efficacy, knowledge, environmental factors influencing behavior) that can be leveraged in behavioral interventions. Moreover, future research on theory-based MSA promotion should also focus on survivors of various types of cancer. Despite the benefits of MSA for cancer prevention and control,4,5,48 only 2 studies in this review focused on cancer survivors, and both were specific to breast cancer.26,32
MSA components in all studies primarily focused on supervised instruction on MSA via classes and one-on-one sessions. However, two studies also included informational handouts (i.e., prescription cards with MSA instructions, handouts with MSA information) to complement these in-person sessions. All interventions were delivered in community settings, except for 1 home-based study which also provided participants with access to exercise equipment and coaches at a community site. Although it was clear that all studies reviewed included components for enhancing knowledge and skill related to MSA, few studies reported intervention content focused on addressing underlying psychosocial and behavioral processes (i.e., sociocultural beliefs regarding MSA, evidence-based behavior change techniques) associated long-term PA behavior change. Thus, further research is needed to explore the psychosocial and behavioral processes influencing MSA behaviors among Latina and Black/AA women. Such work is necessary to inform development of interventions focused on the long-term adoption of MSA behaviors among these populations. Future research should also examine the efficacy of different intervention delivery modes (e.g., home-based, fully remote/telehealth, or combination of both in-person and remote), especially given that home-based PA interventions among Latinas and Black/AA have shown success at increasing aerobic PA17,20,39,49 and help overcome common barriers to in-person programs (e.g., lack of transportation, language barriers, lack of time due to family responsibilities). Additionally, all studies included in the review promoted both aerobic and MSA together; however, it is not known whether increases in MSA typically occur simultaneously with aerobic PA or sequentially (i.e., increase aerobic PA first then increase MSA, or vice-versa). Future research should examine the efficacy of interventions that promote MSA and aerobic PA sequentially vs simultaneously, and should evaluate potential moderating factors for MSA change (e.g., baseline PA levels, age).
Lastly, although all studies included in the review included a stated focus on MSA, only 3 reported assessment measures and outcomes related to MSA. Two interventions included objective measures of muscle-strength (e.g., 1 repetition max test) and 1 study used a self-reported measure that contained a single question asking whether the participant performed MSA on 1 or more days during the past week. The lack of consistent assessment of MSA among studies in this review underscores the need for researchers to incorporate both objective and subjective measures of MSA engagement. Similarly, future research should focus on: (1) development/adaptation of comprehensive measures of MSA that are consistent with national guidelines for MSA (i.e., assess activities that work each major muscle groups on two or more days/week); (2) establishing validity and reliability of objective and subjective MSA measures among Latina and Black/AA women; (3) inclusion of measures that accurately assess activities that count as both MSA and aerobic exercise (e.g., High Intensity Interval Training (HIIT) with dumbbells or circuit training); and (4) measures that can be conducted remotely (e.g., video or telehealth assessments). In addition, there is a need for measurement of potential psychosocial/theoretical mediators of MSA in interventions for Latina and Black/AA women. While existing measures are commonly used in aerobic PA interventions (e.g., social support for PA, efficacy for PA, PA enjoyment), further research on psychosocial/theoretical mediators of MSA is necessary to: (1) understand whether such factors influence aerobic PA in the same way as MSA, and (2) identify psychosocial/theoretical factors that can be targeted to increase MSA in behavioral interventions.
While participant input can be valuable for informing the development and refinement of behavioral interventions, only one of the eight studies in this review reported information about the MSA experience of participants. Future studies promoting MSA in Latina and Black/AA women should also incorporate assessment of participants’ experience with the intervention (e.g., satisfaction questionnaires, interviews) to elicit feedback on MSA components.
Strengths and Limitations
The purpose of this review was to describe the current state of scientific research on MSA promotion among Latina and Black/AA women; accordingly, the review included only studies published in the past 10 years. It is possible that articles published more than 10 years ago may have included MSA promotion content that was not represented in this review. Additionally, our search strategy was limited to 2 electronic databases and included filtering strategies to enhance the relevance of articles retrieved during search procedures. Including additional databases in our search and not using filters may have resulted in the identification of additional articles for inclusion in our review. A strength of our review is that it is the first to examine the state of the literature on the use of behavioral interventions that promote MSA among Latina and Black/AA women. Results provide a comprehensive synthesis of intervention efforts focused on promoting MSA among these study populations and highlight key areas for researchers to explore in future research.
Conclusions
There is a critical need for research on behavioral interventions to reduce the low MSA levels and related health conditions among Latina and Black/AA women. Findings from this literature review provide future research directions in a critical and understudied area of PA promotion in 2 at-risk populations.
Footnotes
Acknowledgments
We thank the librarian, Allison Howard, for providing guidance on the search strategy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Heart, Lung, And Blood Institute of the National Institutes of Health under Award Number (K01HL159044; PI: Benitez) and the National Cancer Institute of the National Institutes of Health Award Number (R03CA252500; PI: Benitez). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Dr Nashira Brown’s work was funded by the National Cancer Institute while a postdoctoral fellow at H. Lee Moffitt Cancer Center and Research Institute (T32CA090314; MPIs: S. T. Vadaparampil and V.N. Simmons).