
Abstract
Many parents still hesitate to encourage their children to participate in resistance training programs. This is unfortunate since recent research shows that resistance training can positively affect children’s health. This narrative review aims to present an overview of the health-associated effects resistance training can provide particularly in children and adolescents with disabilities by describing its effects on muscle strength, physical function, mental health, self-concept, obesity, and injury prevention. To illustrate the variety of possible fields of application, the effects of resistance training in children and adolescents suffering from Charcot-Marie-Tooth disease, cerebral palsy, Down syndrome, Ehlers-Danlos syndrome, joint hypermobility, juvenile idiopathic arthritis, obesity, and spina bifida are discussed. Although randomized controlled trials with a sufficiently large sample size are rare, the research presented in this review indicates that this mode of training might be a potent tool to improve mental and physical health by improving muscle strength, body composition, self-concept or functionality, reducing pain or injury risk, and strengthening bone or tendons even in the most vulnerable groups of children with physical or mental disability. Furthermore, it has to be emphasized that compared with other types of treatment resistance training is considered to be without adverse effects.
‘. . . resistance training is just as beneficial for children and adolescents with disabilities as it is for young athletes.’
It is a persistent misperception that resistance training is harmful for children and adolescents. For many years it has been believed that high forces produced by resistance training will cause damage when being imposed on the immature skeleton. 1 It has been speculated that the immature skeleton is not able to cope with resistance training–induced loading, which would lead to growth plate injuries, thereby inhibiting growth of the long bones at the respective site.2,3 However, there is no evidence supporting this while the current literature indicates that neither adult height nor body segment length is compromised in children regularly exposed to high forces during training as, for example, in elite gymnastics. 4 While resistance training has been a component of many elite sports training programs and its positive effects on performance are well documented, 5 this review will focus on the other end of the spectrum, the less or not at all physically active. It will show that resistance training is just as beneficial for children and adolescents with disabilities as it is for young athletes.
However, nearly a third of parents still fear that resistance exercises are bad for their child’s health, causing injuries and impairing physical development. 1 While 96% of parents had no objections to their child engaging in aerobic exercises, a recent survey reported that 29.6% of parents would not allow their child to participate in exercises with an emphasis on strength. 1 While parents may still hesitate to encourage their children to participate in strength training programs, recent research shows that their worries are uncalled for. On the contrary, many studies have described beneficial effects of resistance training, positively affecting children’s health, while not detecting adverse events as this review will show. Those effects range from direct physiological changes such as enhanced muscle strength, increased bone density, or improved cardiovascular function, to indirect changes in mobility, pain reduction, injury prevention, or self-concept (Figure 1). This narrative review aims to illustrate the variety of health-associated effects resistance training can provide with a specific focus on children and adolescents with disabilities. While the application of strength training programs as a mean to improve health has been investigated thoroughly in some populations, such as obese children and adolescents, other groups of children with disabilities have been neglected. At the same time, it is particularly those groups as, for example, the ones suffering from disorders accompanied by reduced physical fitness and function, where even a small increase in muscle strength, followed by a little change in mobility or self-concept, could potentially have a big impact on their quality of life. To illustrate the variety of possible fields of application for specific populations potentially profiting from resistance training interventions, a range of disabilities is described in this review (Table 1). These are representative of certain impairments that have been selected as they might provoke opposition when resistance training is suggested as a treatment modality. Even though not supported by the current literature, both parents and physicians might still raise the following concerns: one might, for example, argue that resistance training should not be used in children suffering from hereditary muscular disorders as the muscle might not have the capability to adapt (e.g., Charcot-Marie-Tooth disease and Ehlers-Danlos syndrome); one might hesitate to apply resistance training in children suffering from muscle spasticity, as stronger muscles might worsen the spastic muscle contractions (e.g., cerebral palsy); one might worry that it is not feasible to do weight training with children with cognitive impairments, as they might not understand the instructions and might injure themselves (e.g., Down syndrome); one might also argue that resistance training is not viable below a certain level of physical fitness and in children who cannot walk (e.g., spina bifida); one might hesitate to apply resistance training in children suffering from painful joints as the high forces occurring in resistance training might cause even more pain (e.g., joint hypermobility and juvenile idiopathic arthritis); and one might argue that children with obesity should rather do aerobic training to burn calories than to engage in a form of exercise that might make them even bigger.
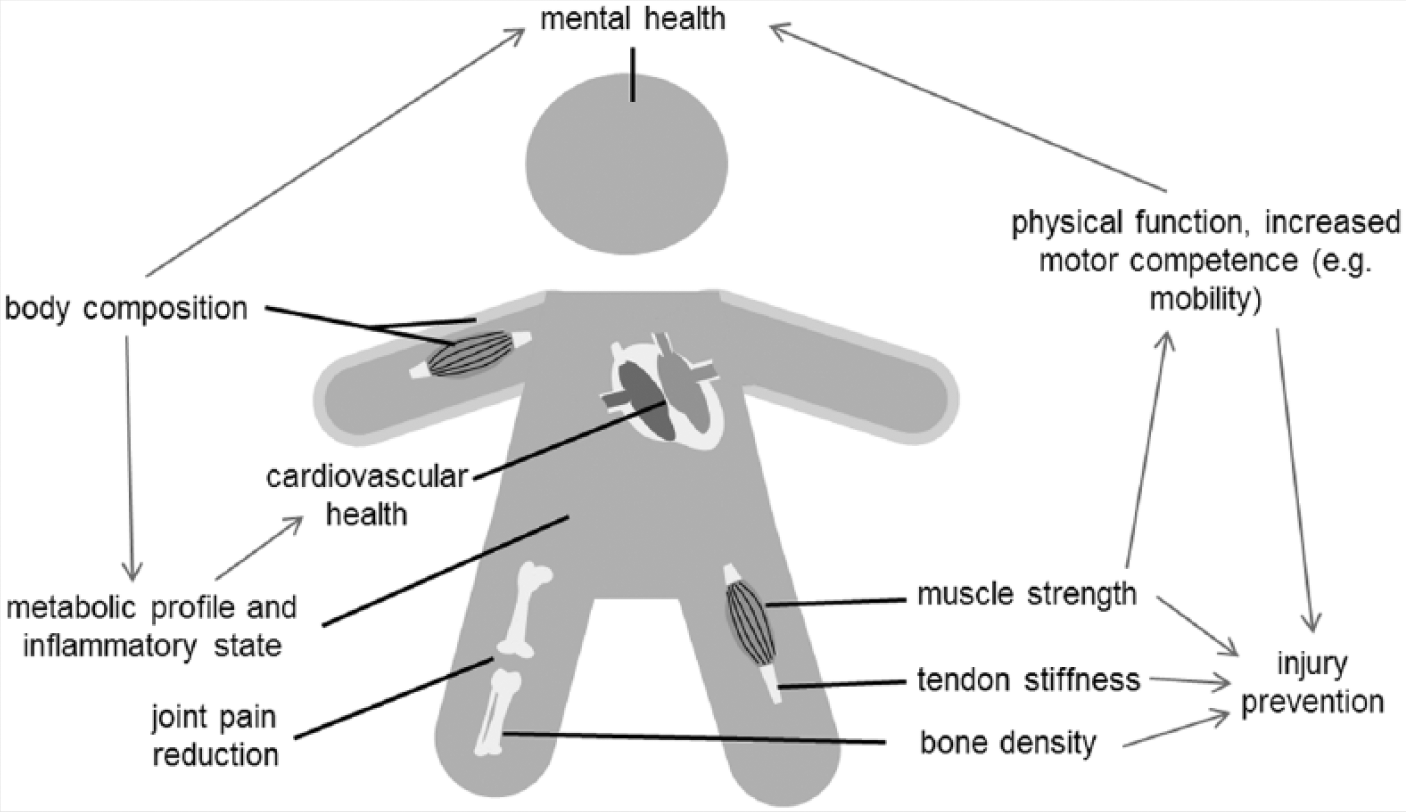
Illustration of resistance training–associated health benefits in children and adolescents. Arrows indicate potential relationships between specific variables directly or indirectly affected by resistance training.
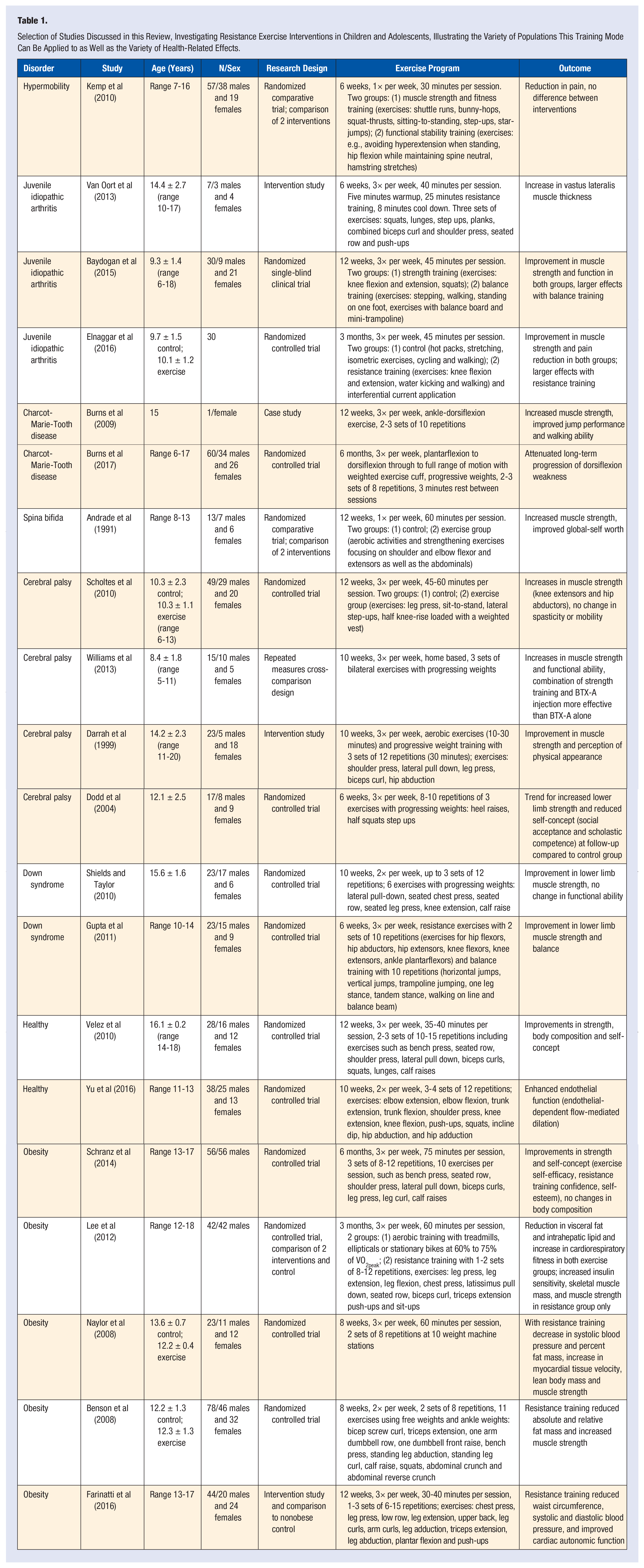
Selection of Studies Discussed in this Review, Investigating Resistance Exercise Interventions in Children and Adolescents, Illustrating the Variety of Populations This Training Mode Can Be Applied to as Well as the Variety of Health-Related Effects.
It is not possible to cover the entire spectrum of disabilities. However, irrespective of the specific disability or syndrome, the synthesis of the presented literature illustrates that resistance training is feasible and can be beneficial for children and adolescents suffering from impairments such as muscle weakness, muscle spasticity, joint pain, or low self-esteem or being at risk to suffer from injury and metabolic or cardiovascular disorders. In the subsequent sections, this narrative review will present an overview of the health-associated effects resistance training can provide in those children by describing its effects on muscle strength, physical function, mental health, self-concept, obesity, and injury prevention. An improvement in one or some of these areas might have a positive impact on the quality of life particularly in children and adolescents with disabilities.
Methods
A literature search was performed using the electronic bibliographic databases ISI Web of Science and PubMed as well as manually screening the reference lists of eligible articles. The eligibility criteria were (1) a publication in English as a full-text paper, considering original articles, case reports, and reviews; (2) publications reporting on children and adolescents aged up to 18 years; (3) publications reporting on the effects of exercise interventions consisting purely of resistance exercises or containing strength training elements; and (4) publications reporting health-associated factors such as muscle strength, cardiovascular parameters, self-esteem, fracture risk, pain, or body mass reduction. The database search was performed in June 2017. No limitations were placed on publication date or study design. The search syntax included combined sets of terms related to resistance training and health combing 4 semantic groups. The first 3 groups identified youth (child* OR adol* OR youth* OR pubes* OR young*), the type of training (resistance OR strength OR weight*), and the training itself (training OR exercise* OR intervention* OR program), concatenated by the Boolean AND. The last group identified (1) obesity (obes* OR overweight OR adipos*), (2) orthopedic issues (hypermobi* OR injury prevention OR rupture OR fracture), (3) cardiovascular parameters (cardi* OR heart OR blood pressure OR HRV OR BP), (4) psychological parameters (self esteem OR self concept OR self efficacy), or (5) cerebral palsy. For the group identifying obesity, the search field was limited to the title, due to the high number of original papers and reviews in this field. For all other groups all search fields (abstract, title, keyword, text) were considered, as a very limited number of papers has been published in those areas of research. The initial database search yielded 81 articles for group 1, 5 articles for group 2, 14 articles for group 3, 12 articles for group 4, and 49 articles for group 5. Since it was the intent of this article to present an overview of possible fields of application of resistance training in children and adolescents with certain impairments by providing a synthesis of the available literature on the effects of resistance training on health, not all studies available have been presented. Instead, it was referred to reviews and meta-analyses wherever possible, to depict current views on the application of resistance training and its effects, while presenting some experimental studies as examples.
Muscle Strength and Physical Function
There are numerous diseases or disabilities that are associated with reduced physical fitness and function in affected children compared to their normally developing peers. Muscle strength is in this context a key determinant as it effects the ability to walk or to perform daily tasks. The reduction in muscle strength might be a consequence of the disability or injury itself. However, it might also be the result of pain, whereby as secondary effect the avoidance of certain movements, tasks, or exercises leads to muscle atrophy. In addition, this will be made worse by adopting a predominantly sedentary lifestyle, which many of these children do. 6
Even with neuromuscular disorders the capacity of the muscle to adapt to physical loading is usually maintained. Although the extent of muscle hypertrophy might differ from normal developing controls, resistance training can improve muscle strength and function in children with a disability. An example is the Charcot-Marie-Tooth disease, a hereditary degenerative slowly progressing neuromuscular disorder characterized by motor and sensory impairments. In those patients, muscle weakness, which particularly affects the foot muscles, has a great impact on their quality of life, as it impedes everyday activities such as walking or stair climbing. The loss in functionality may then also lead to injuries resulting from trips and falls. 7 However, the adaptive processes of the muscles are not affected and thus muscle adaptation is still possible in spite of the disease. Although the evidence is still limited due to the small number of studies, it appears that resistance exercise may be beneficial to maintain muscle strength and function in these patients. 8 Studies suggest that resistance training is also feasible and safe in childhood Charcot-Marie-Tooth disease, counteracting foot weakness.9,10 A case study reported an increased ankle dorsiflexion and plantarflexion strength, being accompanied by improved jump performance and walking ability in a 15-year-old girl after 12 weeks of resistance training. 9 The first randomized controlled trial on the effects of resistance training in pediatric patients with Charcot-Marie-Tooth disease confirmed this positive outcome. It reported that 6 months of targeted progressive resistance exercise attenuated long-term progression of dorsiflexion weakness without detrimental effects on muscle morphology or other signs of overwork weakness. 10
Another population that might benefit from resistance training is children with cerebral palsy. Cerebral palsy is a nonprogressive neurological disorder, which is often accompanied by muscle weakness, muscle stiffness, and decreased range of motion, spasticity, and difficulty walking.11,12 In children suffering from this condition, resistance exercise has been avoided for many years due to concerns that exercise might negatively affect muscle spasticity, flexibility, or movement patterns. However, growing evidence suggests that these fears are uncalled for, that there are no serious adverse effects, 13 and that children with cerebral palsy may benefit from exercise. 14 Resistance training does considerably increase muscle strength in children with cerebral palsy without adverse effects on spasticity or a reduction in range of motion.15,16 However, an increase in muscle strength does not necessarily translate into improved mobility or walking ability.15,16 A recent Cochrane review therefore concluded that resistance training does not improve gait speed and gross motor function in children with cerebral palsy, 13 while another review stated that muscle strengthening interventions are neither effective nor worthwhile. 17 It needs to be considered though that the Cochrane review also stated that the quality of evidence for these conclusions is low to very low, due to small sample sizes of most trials. 13 In addition, a resistance training program can be composed of very different exercises that can be executed in different ways, affecting the efficacy of the training program. Thus, resistance training should not be disqualified yet until there is better evidence on its efficacy, possibly in combination with other exercise or treatment modalities. Indeed, the combination of resistance training with botulinum toxin type-A did not only increase muscle strength but significantly improved the functional ability of children with cerebral palsy. 12 The study furthermore demonstrated that the concurrent treatment was more successful than the botulinum toxin type-A injections alone. 12 This also highlights that even partially paralyzed muscles, as those injected with botulinum toxin type-A, can be successfully strength trained.
However, in some children with cerebral palsy and in children with other disabilities, the muscle weakness in the lower body may be too pronounced to allow resistance training of the lower limb muscles. Still, wheelchair-bound children may be able to train the muscles of the upper body, benefiting from increased strength in the core and upper limb muscles. As an example, a 10-week exercise program with 8- to 13-year-old children with spina bifida, half of them wheelchair users, led to significant improvements in elbow flexion strength compared to a nonexercising control. 18
Muscle weakness is also a symptom of Down syndrome,19,20 a genetic disorder attributed to the triple occurrence of the chromosome 21. Other symptoms include cardiovascular and cognitive impairment, as well as weak gross motor and fine motor skills. 21 The ability to walk independently, to perform daily activities and workplace-related tasks depend on a sufficient level of muscle strength. This emphasizes the need to enhance and preserve muscle strength from childhood on. Resistance training has been shown to increase muscle strength both in children21,22 and adults 23 with Down syndrome. These studies furthermore indicate that resistance training is both safe and feasible even with mentally disabled people as those with Down syndrome.21-23 However, similar to other disabilities with associated muscle weakness, an increase in muscle strength does not necessarily improve function directly. A study that subjected 11 adolescents with Down syndrome (15.6 ± 1.6 years of age) to a 10-week-long progressive resistance training program with 2 sessions per week led to a 42% increase in lower limb strength, while the timed up and down stairs test, a measure for physical function, did not change compared to the control group. 22 However, while muscle strength is easily quantifiable, it is more challenging to verify a clinically relevant improvement in physical function and performance such as the ability to complete daily tasks, particularly if small sample sizes are investigated.
Another field of application is the management of disorders leading to joint pain, such as hypermobility or juvenile idiopathic arthritis. Joint hypermobility, defined as greater than normal joint laxity across multiple joints and a Beighton score of ≥6, is common in children with prevalence rates of 11% and 26% in boys and girls. 24 Although joint hypermobility does not necessarily cause musculoskeletal pain, a significant association between generalized joint hypermobility and pain experienced in 2 or more areas has been described for 14-year-old boys and girls. 24 While sport in general can make this pain worse, 24 physiotherapy approaches aiming to improve muscle strength and motion control are an important tool in the management of hypermobility.25,26 Indeed, a 6-week exercise program aiming to improve muscle strength and fitness, containing resistance training elements such as squat-thrusts and step-ups, led to a significant reduction in pain in 7- to 16-year-old children. 25 Even children suffering from the Ehlers-Danlos syndrome, who present with severe hypermobility, skin extensibility, and tissue fragility caused by a collagen type V defect, might benefit from resistance training. A small pilot study on adults with genetically verified Ehlers-Danlos syndrome could show that heavy resistance training in those patients was both feasible and safe, leading to increased tendon stiffness, increased muscle strength, and improved balance, represented by a smaller sway-area. 27
Similar to the hypermobility syndrome, pain is a common and frequent symptom of juvenile idiopathic arthritis. The high intensity of pain in juvenile arthritis limits and disrupts functional activities, which in the long term leads to muscle weakness.28,29 Exercise treatment has been recognized as a clinically relevant strategy in the management of juvenile idiopathic arthritis30,31 to maintain or restore function and to reduce pain. A 6-week home-based resistance program has been shown to be both safe and feasible in 10- to 17-year-old children, with no adverse effects and no increase in pain during the intervention period. The 40-minute program, which had to be executed 3 times per week, contained squats, lunges, step-ups, planks, combined biceps curl and shoulder press, seated row and push-ups, and led to a significant increase in the vastus lateralis muscle thickness. 32 Another resistance training program equally led to muscular improvements, by increasing muscle strength of the knee flexors and extensors, while also reducing pain at rest and during exercise. 28 Particularly in populations suffering from painful joints or musculoskeletal injuries, resistance training can also be performed in water. Muscular training in water uses the resistance provided by the water while at the same time taking advantage of the buoyancy effect leading to reduced forces acting on the joint. Furthermore, water might provide an environment in which the hydrostatic pressure helps to alleviate swelling and to improve circulation. 29 Underwater resistance training has been reported to be feasible and effective even in children. This form of training applied for 3 months improved muscle strength of both quadriceps and hamstrings in 10-year-old children suffering from juvenile idiopathic arthritis. 29 In conclusion, resistance training has been shown to improve muscle strength in a variety of disorders and disabilities, while an improvement in muscle strength did not necessarily lead to improved physical function. Resistance training has been reported to be safe and feasible even in children suffering from severe musculoskeletal disorders, painful joints, muscle spasticity, or mental disability.
Mental Health and Self-Concept
While it is intuitive to associate resistance training with physical changes in the musculoskeletal system and particularly with muscle strength, resistance training can also affect mental health. Several studies have shown that a resistance training intervention can provoke positive effects such as a higher self-concept.18,33,34 There may be several reasons for the psychological benefits of resistance training. Among the most relevant reasons is most likely the relationship between self-concept and competence. Adolescents with low motor competence have been reported to have low physical self-perceptions compared to their well-coordinated or physically fit peers. 35 If motor competence is increased, for example, by an exercise intervention, this can have a positive impact on adolescent physical self-perceptions, particularly in males. 35 In this context, resistance training may be particularly suitable and also practical in children with lower motor competence, such as children with disabilities, musculoskeletal disorders, or obesity, who may have difficulties to participate in other forms of physical activities. Children with obesity might even outperform their lean counterparts, as a higher fat mass often goes along with a higher fat-free mass. 36 The higher body mass, which they have to carry with every single movement, acts as a continuous stimulus inducing muscle hypertrophy. The larger muscle mass can then lead to a better performance in strength exercises such as the medicine ball throw. 37 Indeed, a 6-month resistance training with obese adolescents aged 13 to 17 years not only significantly increased muscle strength, as illustrated by better bench press and leg press performance, it also positively affected exercise self-efficacy, training confidence, and global self-esteem. 33 The effect of resistance training on psychological outcomes is not limited to children or adolescents with obesity. Also in adolescents with cerebral palsy (aged 14.2 ± 2.3 years), a 10-week exercise training program, which included resistance training elements leading to a significant improvement in muscle strength, was associated with a dramatic change in the perception of physical appearance. 11 That such changes in perception might substantially affect the quality of life in those children was indicated by anecdotal evidence reporting that a participating boy was wearing shorts for the first time, and that 3 girls, who took part in the study, were feeling confident enough at the end of the exercise program to attend a regular aerobics program. 11 Similarly in children with spina bifida, global self-worth increased together with elbow flexor strength after a 10-week exercise program. 18 While the psychological well-being of children with musculoskeletal disorders or severe obesity may be more at risk, healthy adolescents also benefit from resistance training. A 12-week resistance training program with healthy Hispanic adolescents between 14 and 18 years of age also led to significant improvements in their self-concept including attractive body adequacy and global self-worth. 34 This might encourage the adolescents to keep exercising, which in turn might prevent them from developing diseases associated with a sedentary lifestyle. The setting in which the exercise program takes place might in this context have a decisive impact on the effectiveness of the program in terms of mental health. A group of children with cerebral palsy, who participated in a 6-week-long home-based resistance training program, unexpectedly showed a decreased self-concept in the domain of scholastic competence and social acceptance at the follow-up 12 weeks after finishing the program. The authors of that study suggested that the children might have felt that they had less time to do their homework and to interact with their peers, since they had to spend time on doing the resistance exercises at home. 38 A home-based intervention has certainly advantages, such as it requires less time spend on travelling from and to the training venue and less effort from the parents driving their children. However, a group training might be perceived as more sociable and enjoyable, which might also promote exercise adherence. 29 In conclusion, resistance training has the potential to positively influence the self-concept of children and adolescents, while there appears to be no direct relationship between the increase in muscle strength and the self-concept. The mechanism by which resistance training improves mental health needs to be elucidated.
Obesity Management
There has been a recent shift in obesity management, away from focusing on a reduction in fat mass toward an improvement in body composition through increasing the percentage of lean body mass. 39 While this at first sight seems a marginal change in perspective, it allows the establishment of resistance training programs in obesity management instead of aerobic exercise programs that children with obesity might be less inclined to follow due to their lower endurance competence. 39 An overwhelming number of studies have now shown that resistance training indeed leads to an improvement in body composition.40-45 As a result, a recent meta-analysis confirmed that there is compelling evidence that resistance training positively affects body composition in children and adolescents, although the effects were very small to small. Furthermore, the authors concluded that aerobic training alone was not better, similarly producing small to very small effects on body composition, with resistance training having the advantage of also resulting in moderate to large improvements in muscle strength. 46 Significant improvements in children’s body composition can already be seen after just 8 weeks of resistance training, given a training frequency of 3 times per week. 47 On cessation of the training program the benefits can be maintained for several months.47,48 However, further improvements are realized with longer duration training programs,47,48 and long-term health benefits will only be achieved when the children and adolescents continue to engage in physical activities on cessation of the controlled study program. 49 Improving the body composition through increasing the fat-free mass furthermore affects the energy balance and the metabolic profile. Several studies found that resistance training improved insulin sensitivity in obese adolescents.45,50,51 As insulin resistance is suggested to be a key factor contributing to the development of obesity-related chronic diseases such as type 2 diabetes, the improved insulin sensitivity may reduce the risk to develop obesity-related comorbidities. Systemic inflammation has similarly been linked to comorbidities in obese individuals. And again, a resistance training intervention has been shown to reduce levels of pro-inflammatory cytokines such as interleukin-6 and tumor necrosis factor-α. 52 Other studies have shown that the combination of aerobics with resistance training was more effective in positively influencing the inflammatory state in obese adolescents, as reflected by an increase in serum adiponectin concentrations, than aerobic training alone.53,54 Moreover, childhood obesity increases the risk to develop cardiovascular disorders such as hypertension. Already in 13- to 17-year-old adolescents systolic and diastolic blood pressure have been shown to be increased compared to nonobese controls. 55 Their cardiovascular health was significantly improved by a 12-week resistance training program, reducing blood pressure and increasing parasympathetic activity. 55 Myocardial function has also been shown to be improved by an 8-week-long resistance training program in children with obesity, as represented by an increased diastolic myocardial tissue velocity. 56 The positive effects of resistance training on cardiovascular health are at the same time not restricted to children and adolescents with obesity. Even in lean and active boys and girls aged 11 to 13 years a 10-week-long resistance training program improved vascular function, illustrated by an increase in endothelium dependent flow-mediated dilation, 57 while an 8-week resistance training program reduced systolic and diastolic blood pressure in young (aged 21 ± 0.3 years) normotensive subjects. 58 In conclusion, resistance training with obese and nonobese children and adolescents can have positive effects on their body composition, metabolic profile, inflammatory state, and cardiovascular health.
Injury Prevention
Functional impairments, habitual inactivity, and medication may increase the injury risk in children with disabilities compared to regularly active, healthy children. Particularly bone fractures are a common problem in children with disabilities such as cerebral palsy, 65 spina bifida, 66 or Duchenne muscular dystrophy. 67 As described in a recent review, immobilization or conditions of weightlessness, poor nutrition, and the use of potentially bone toxic medications may adversely affect bone health in children with chronic neuromuscular diseases, thus leading to an increased risk of fractures. 68 In addition, joint contractures in the lower limbs or hips make it more difficult to adequately react to perturbations, leading to falls in situations of unstable balance and also increasing fracture risk. 68 Not all studies found a higher fracture rate in children with cerebral palsy compared to normally developing peers.69,70 However, the injury mechanism particularly in children with severe cerebral palsy is different: children with severe cerebral palsy are far more likely to suffer from fractures after minimal or no trauma.69,70
There are two main reasons why resistance training could potentially prevent fractures, particularly in children and adolescents with disabilities. First, an increased muscle strength might allow more control over joint movements in unexpected situations while increasing the amount of possible movement patterns, leading, for example, to successful balance recovery following perturbation. Thus, movements imposing nonphysiologically high loads on the musculoskeletal system are avoided. This might be particularly important for children suffering from disabilities accompanied by a pronounced reduction in muscle strength. Second, resistance training might change the structure of the musculoskeletal system. Thus, potentially injury-provoking movements might not lead to the fracture of the well-adapted, stronger bone, respectively, the rupture of the well adapted, stiffer tendon.
Indeed, low muscle strength has been found to be associated with an increased risk of fracture, as a large cross-sectional study on 1590 children aged 13.9 ± 1.5 years has shown. Interestingly, the greatest risk of fractures among the children with low muscle strength was seen in those with the highest aerobic fitness. 71 While aerobic fitness per se could be related to the amount of physical activity, thereby increasing injury risk as a consequence of exposure time, it highlights the importance of a balanced physical education. Endurance training has undoubtedly many beneficial effects on the cardiovascular system, including aerobic fitness. However, it does not protect from musculoskeletal injuries. Furthermore, if exercises that improve muscle strength are included in an exercise program, an increase in the amount of physical activity does not necessarily lead to an increase in the fracture incidence. This is supported by a 5-year school-based exercise intervention study, which increased the physical education curriculum from 60 minutes to 200 minutes per week, while the control group continued with the regular physical education of 60 minutes. The exercise program significantly improved the gain in lower limb muscle strength, and although the amount of physical activity was 3 times higher in the intervention group, fracture risk was not elevated. 72
While there is evidence for the effect of resistance training on injury rate in adults and the elderly,59-61 there is little known on the effect of resistance training on injury rate in children and adolescents with disabilities. However, the regular participation in resistance training sessions or the incorporation of strength training elements in the regular training regime is strongly recommended in recent publications and position statements as strategy to prevent injuries in healthy children and adolescents.62-64 It seems reasonable to assume that resistance training may similarly be used as a strategy to prevent injuries in children with disabilities. Apart from increased muscle strength, compositional and architectural changes in bone and tendon could reduce the injury risk particularly in children with disabilities. Low bone mass in children with cerebral palsy, spina bifida, or Duchenne muscular dystrophy causes increased bone fragility, leading to fractures after even slight trauma. 68 Increasing bone mass by regular loading in form of weight-bearing, using standing devices or practicing resistance training, may decrease the risk of fractures.
It is well established that vigorous physical activity affects bone properties even in children. Several studies have described an increased bone mineral content and bone strength index (noninvasive indicator of bone strength, calculated from the product of cortical bone mineral density and cross-sectional moment of inertia) of the radius in trained female gymnasts, aged 6 to 12 years, resulting in a reduced estimated fracture risk.73-75 A structured resistance training program can similarly lead to changes in bone properties. Fifteen months of resistance training with 3 sessions per week, consisting of 2 to 3 sets of 15 exercises, increased, for example, femoral neck density in the resistance trained compared to the control group in 14- to 17-year-old girls. 76 Even a much shorter intervention of only 6 weeks resistance training (75 minutes 3 times per week) with children with obesity aged 8 to 11 years led to significantly larger increases in bone mineral content compared to a control group. 40 However, not all studies have detected changes in bone properties following resistance training. While a resistance training, consisting of 4 sets of 13 exercises performed 3 times per week with progressive intensity performed over 26 weeks, led to significant increases in muscle strength, bone mineral density and content did not change significantly in 14- to 18-year-old girls. 77 While there are no studies on the effect of resistance training on bone properties or fracture risk in children with disabilities, beneficial effects of weight-bearing on bone have been observed. In children with severe cerebral palsy the fracture risk was reduced 4-fold in those using standing devices on a regular basis compared to children who lacked weight-bearing as part of their everyday routine. 70 In children with spina bifida bone mineral density was found to differ significantly according to the ambulatory status, with lower values in children who were wheelchair-dependent.78,79 Independent of the ambulatory status, higher values were found in those who practiced sports activities. 79 This indicates that resistance training may be an appropriate tool to increase bone mass or bone mineral density and decrease fracture risk in children with disabilities. Similar to bone, the adolescent tendon responds to long-term loading with changes in structure and composition. This is illustrated by significantly larger tendon thickness being observed in young competing athletes compared to age-matched nonactive controls.80,81 Resistance training has the capacity to improve mechanical and material properties by increasing stiffness and Young’s modulus, as a 10-week program in prepubertal children (aged 8.9 ± 0.3 years), consisting of 2 to 3 sets of 8 to 15 plantar flexions twice a week, has shown. 82 By enhancing the tissue loading capacity, nonphysiological levels of stress and strain, potentially leading to tendon pathologies such as tendinopathies, can be avoided. 83 In conclusion, resistance training in children and adolescents can lead to physiologically relevant changes in bone and tendon properties. Together with an improved muscular control this can reduce the injury risk.
Conclusion
The reported positive effects of resistance training are manifold (Figure 1), while it has been shown again and again that this form of training is feasible and safe even in the most vulnerable groups of children with disabilities. Although randomized controlled trials with a sufficiently large sample size are rare, the overall large number of small studies reports a range of positive effects following resistance training. This indicates that this mode of training might be a potent tool to improve mental and physical health of children and adolescents. Furthermore, it has to be emphasized that, in contrast to other types of treatment particularly children and adolescents suffering from diseases or disabilities are subjected to, resistance training is more or less free from adverse effects. Given that some safety rules are followed and that instructions are given by qualified professionals, it can be concluded that strength training is a relatively safe and healthy practice for children and adolescents. 84
Admittedly, there is still room for improvement in terms of the effectiveness of the resistance training programs. To be able to tailor an exercise prescription to the needs of a specific population, achieving exactly the form and extend of adaptation one is aiming for, the mechanobiological mechanisms behind the effects of resistance training need to be better understood. While we know that resistance training causes physiological adaptations such as muscle hypertrophy, we do not know exactly which mechanobiological stimulus leads to what molecular/cellular response and how this relates to structural or metabolic changes. 85 To tackle this problem, which is not restricted to studies in children or adolescents and similarly applies to studies in the adult or elderly, two requirements need to be fulfilled. First, the applied loading stimulus would need to be described in great detail, which rarely is the case in the past and present literature. This should allow the association of a specific loading condition with a specific physiological adaptation. Most studies provide information on the load magnitude, the number of sets, and the number of repetitions (Table 1). However, to fully understand quantitative and/or qualitative effects on skeletal muscle with respect to resistance exercise, a set of not less than 13 mechanobiological determinants has been proposed, adding information, for example, on the time under tension, rest in-between repetitions, or range of motion. 85 Second, more information on the change of physiological parameters as a result of resistance training in children and adolescents are needed, to be able to link the training stimulus to a physiological adaptation and the physiological adaptation to a functional outcome. 86 To date we do not fully understand the relationships between single variables influenced by resistance training such as muscle morphology, muscle strength, and mobility or injury prevention. If, for example, muscle strength is reported as an outcome parameter following resistance training, we do not know if a measured improvement in muscle strength is a result from changed muscle morphology, changed muscle activation, better intramuscular coordination, or better motivation. If we then try to link an increase in muscle strength to an indirect functional outcome, it will be difficult to identify and specifically target the variable responsible for an improvement in functionality.
While we are still beginning to understand the mechanisms with which physical training, such as resistance training, affects the health of children and adolescents, we do know that it can potentially result in a variety of health benefits. Furthermore, we know that it is safe and feasible to apply in even the most vulnerable groups of children, presuming that appropriate supervision and instruction is given. So instead of asking ourselves why children should engage in resistance training, we should ask why they are not doing it already. Further improving our understanding of the mechanisms behind adaptation to resistance training should help to make exercise interventions more effective and convince both children and their parents to invest their time in participating in a resistance training program.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.