
Abstract
“The WAI-SR Bond domain refers to the positive relationship between the patient and HC that facilitates engagement with the program.”
Introduction
Living with chronic obstructive pulmonary disease (COPD) can be challenging, and several patients are unable to achieve and maintain a healthy lifestyle and a positive quality of life.1–3 Many COPD patients strive to maintain their independence and live well within the context of the physical limitations and psychological implications of COPD and its treatments. 4 Health coaching and remote monitoring represent an opportunity for behavior change in a home-based setting, which is particularly relevant in the current COVID-19 pandemic. 5
Telephonic health coaching is an innovative way of delivering health care in a home setting to comprehensively improve the Self-Management (SM) of patients with COPD.5–7 Health Coaching includes practices and strategies that follow principles of patient-centered communication (motivational interviewing), setting goals, strength-based discussion, patient self-discovery, self-monitored patient behaviors, and accountability provided by the Health Coach (HC) to help mobilize patient behavior change. 8
It is plausible that the degree of engagement between the patient and the health coach can have an impact on SM abilities: a critical outcome in behavior-change interventions. 9 Positive therapeutic engagement between provider and patient has been shown to improve patient health outcomes.10–12 Building a working relationship and rapport is considered fundamental for effective patient care. 13 From a patient’s perspective, support with chronic disease management, rapport-building, and shared decision-making are highly appreciated and valued. 14
We hypothesized that patient engagement, a foundational aspect of health coaching, is positively associated with SM abilities, in patients diagnosed with COPD. The latter has never been tested and may have profound implications for patients and providers given that SM is associated with quality of life and effective healthcare utilization.15,16
The purpose of this project was to investigate the association of health coach-patient engagement with SM abilities in an 8-week remote monitoring intervention with health coaching for patients with COPD.
Methods
Intervention
The 8-week intervention consisted of weekly health coaching calls and a system that include video-guided exercises using a computer tablet, a pulse oximeter, the measurement of daily steps through a wearable fitness tracker, and daily self-report of symptoms (figure 1). The results of the intervention have been previously reported.
5
Remote monitoring with health coaching intervention.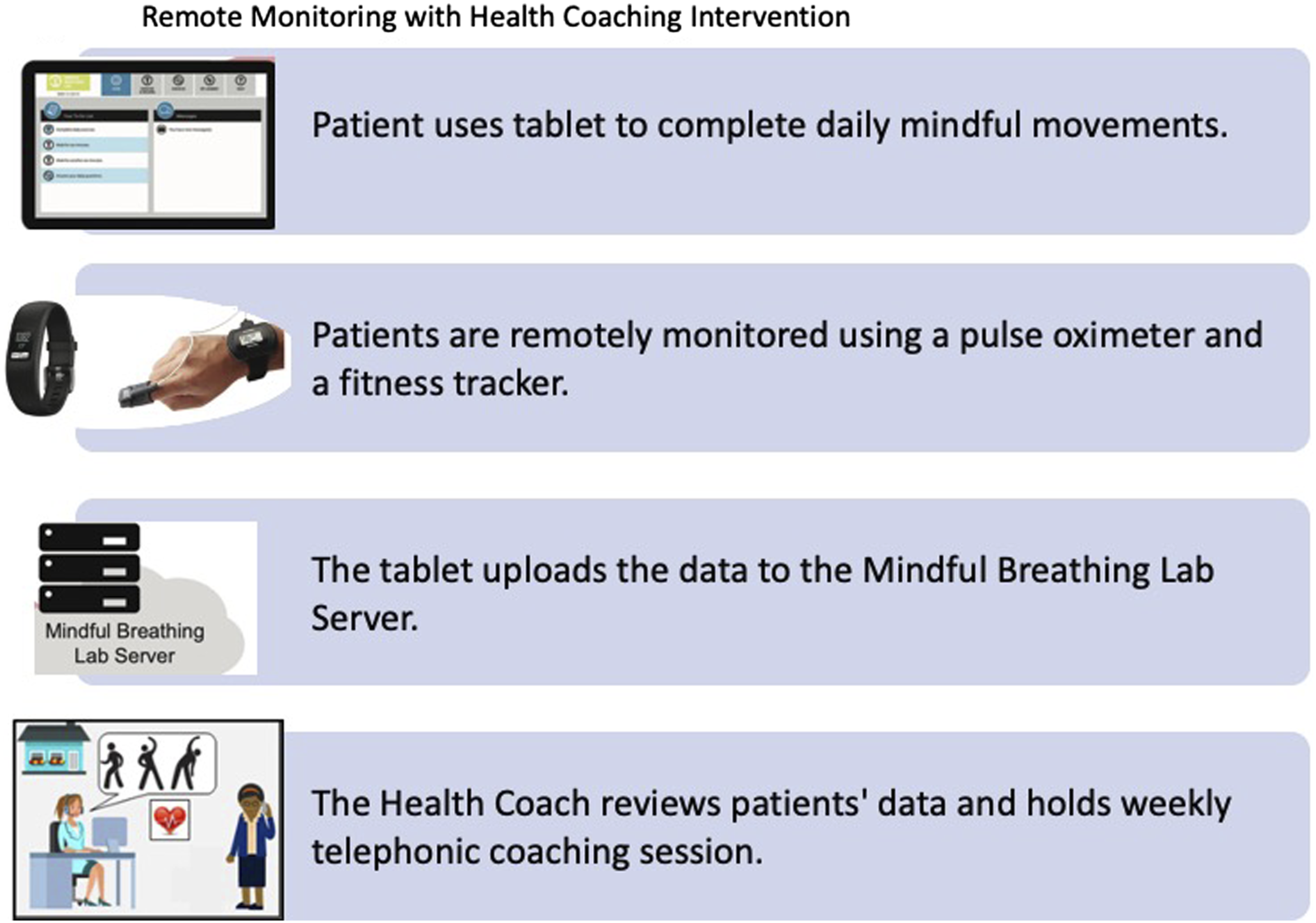
Health Coach Training
The training of the non-accredited HCs for the tested eight-week health coaching with technology intervention was based on Motivation Interviewing (MI). The HCs had diverse educational backgrounds (nurse, master’s in public health, and bachelor’s degrees). The Mindful Breathing Laboratory provided the training for the HC to be proficient in the skills to engage with patients. MI is an effective communication technique that focuses on a collaborative, person-centered approach to elicit and strengthen motivation for change.17 MI focuses on communication skills that explore and resolve ambivalence while centering on motivational processes within the individual to facilitate change.
The MI training of the health coaches consisted of 2 key components. The first component was reading the book “Building Motivational Interviewing Skills: A Practitioner Workbook” by David Rosengren. 17 The health coach read each chapter and completed the assignments at the end of the chapter, and the trainer would review these.
The second component of the training was the use of a commercially available interactive software that the health coach could roleplay with called “SIMmersion” (www.simmersion.com). SIMmersion is a software developed to train motivational interviewing and communication skills in realistic simulations. SIMmersion required ten completed sessions of 80% or higher for the certificate of completion to be issued; however, the Mindful Breathing Lab required 90% scores to fully allow the health coach to engage with real-life patients. Once a certificate was obtained, the health coach continued to complete a monthly session with a score of 90%, as a marker of fidelity.
The same HC was assigned to the patient for the 8-week intervention. Weekly required meetings between the health coaches and Pulmonologist (principal investigator) provided a review of patient outcomes and discussion of specific pulmonary issues beyond the education and knowledge base of the health coach. The team reviewed the HC portal and each HC reported on their patients. The main points that were covered were patient engagement with the exercise videos, daily step counts, oxygen saturation during exercise, and daily check-in questions. Additionally, HCs reported if the patient had an exacerbation of symptoms, had to use an emergency medication plan or used health care services, or any other clinically significant event. HCs were instructed to facilitate patients’ self-efficacy in self-management abilities and avoid the righting reflect of trying to fix their problems.
This approach allowed the health coach to engage with the patients fully and feel confident to effectively coach while having the clinical support of the Pulmonologist. The health coaches had the training provided by the Mindful Breathing Laboratory but were not accredited.
Health Coaching Intervention
Health coaching was provided weekly throughout the 8-weeks of the intervention. The HC can facilitate patient motivation and empowerment to achieve desired goals.
The weekly topic was chosen by the patient. The HC had the intent to empower patients to address what was important to them. There was not an educational component besides the information given on how to use the system. The coach’s informative support helps patients in becoming more effective in their technology use, so they could fully engage with the program. If the patient asked for information, the HC was able to give general information with an elicit-provide-elicit framework. The HC would ask the patient what they know about the topic, offer additional information or ideas, and ask the patient again what they take away from the conversation. The HCs marked the topic discussed on the call log database and added a brief description of the call, this allowed us to investigate patients’ main topics of interest. Our approach challenges the “one size fits all” interventions by tailoring programs to the individual field.18,19 Increased patient mastery of disease, addressing facilitators and barriers to the success of self-management interventions can facilitate tailoring of interventions based on patient’s needs. 20 Previous reports suggest that personalizing and adapting health messages have been found to increase the engagement of the patients. 21
Measures
The Self-Management-Ability-Scale-30 (SMAS-30) is a 30-item questionnaire designed to measure SM abilities in chronic disease. It asks patients to rate on a Likert scale how often they engage in or how much they agree with various facets of self-management. The questionnaire reports a total score (main outcome) and has 6 subscales: taking initiative, investment behavior, variety, positive frame of mind, self-efficacy, and multifunctionality. The questionnaire is valid in the COPD, elderly, and frail populations, 9 has good internal consistency, and reliability, and has demonstrated validity in COPD outcome research. SMAS-30 subscales scores range from 5 to 30, with higher scores indicating higher SM. The self-management of wellbeing theory that supports this instrument poses that successful aging is a lifelong process of proactively sustaining wellbeing, even in the face of declining resources and chronic conditions. 9
The Working Alliance Inventory Short Revised (WAI-SR) was the validated questionnaire used to investigate the degree of working alliance/engagement between the patient and the health coach during the eight-week health coaching intervention. The WAI-SR is a 12-item questionnaire that provides a total score and is categorized in domain scores for Bond (engagement with the health coach), Task (agreement with a specific activity), and Goal (alliance on the weekly endpoint). 22 The responses are rated on a seven-point Likert scale, ranging from 1 (never) to 7 (always). The total score ranges from 12 to 84, and domain scores range from 1 to 7.
The Medical Research Council Dyspnea (mMRC) is a 5-question questionnaire used to establish functional impairment of respiratoration caused by dyspnea. The items on the 5-point scale (0–4) rate the severity of dyspnea. 23 Lower scores (0–1) indicate less shortness of breath, and higher scores (2–4) indicate high perceived dyspnea.
The Patient Health Questionnaire (PHQ-2) was used to screen for depression symptoms. The PHQ-2 score ranges from 0–6. A scoring of 3 or greater indicates a higher likelihood of a clinically significant depression. 24
The Generalized Anxiety Disorder 2-item (GAD-2) is a very brief and easy to perform initial screening tool for the assessment of symptoms of a generalized anxiety disorder. A scoring of 3 or greater indicates a higher likelihood of a GAD. 25
Statistical Analysis of Health Coaching Intervention Database
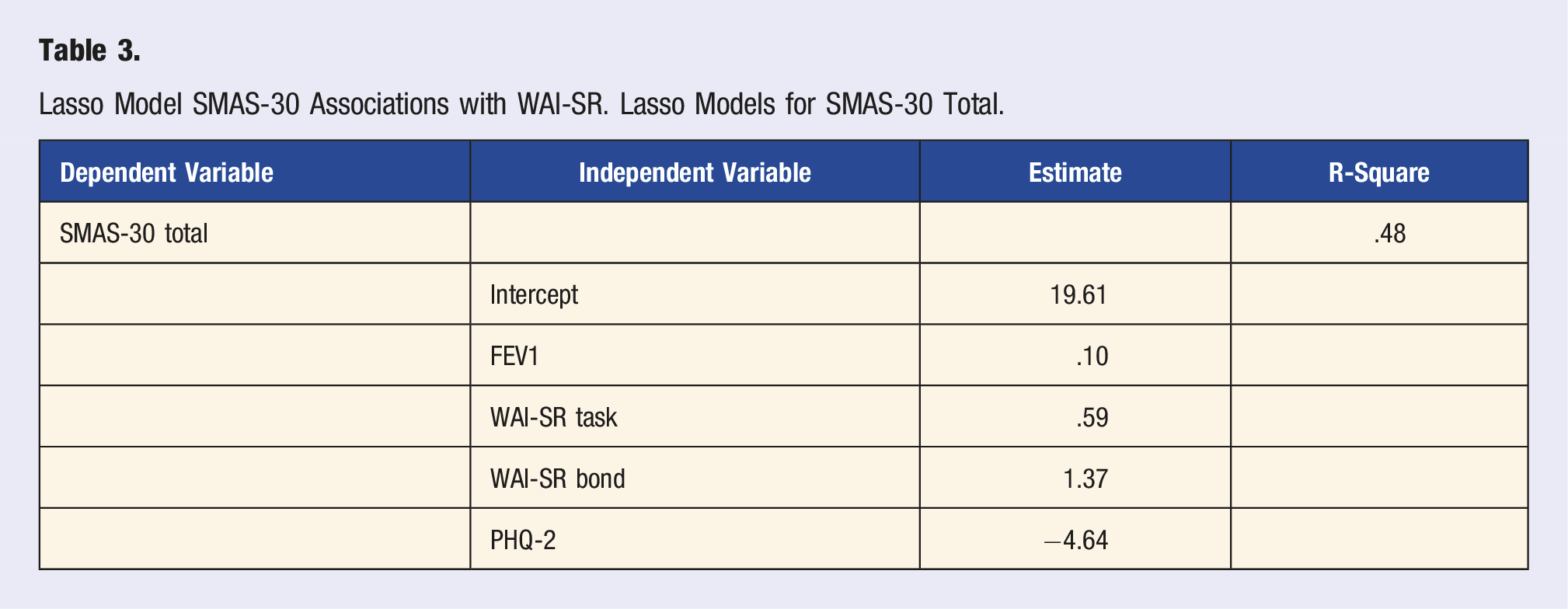
Linear regression models were used to define the association between WAI-SR domain scores (independent variable) and SMAS-30 totals score (dependent variable), other independent predictors (identified by the model) included age, lung function (FEV1%), mMRC, gender, and PHQ-2. Model selection was done using lasso shrinkage methods. The dependent variable was modeled separately by starting with all the independent predictors in the model and allowing the lasso method to select the best predictors of the dependent variable. Model assumptions were validated by looking at residual plots. All analyses were done using SAS software, Version 9.4.
Results
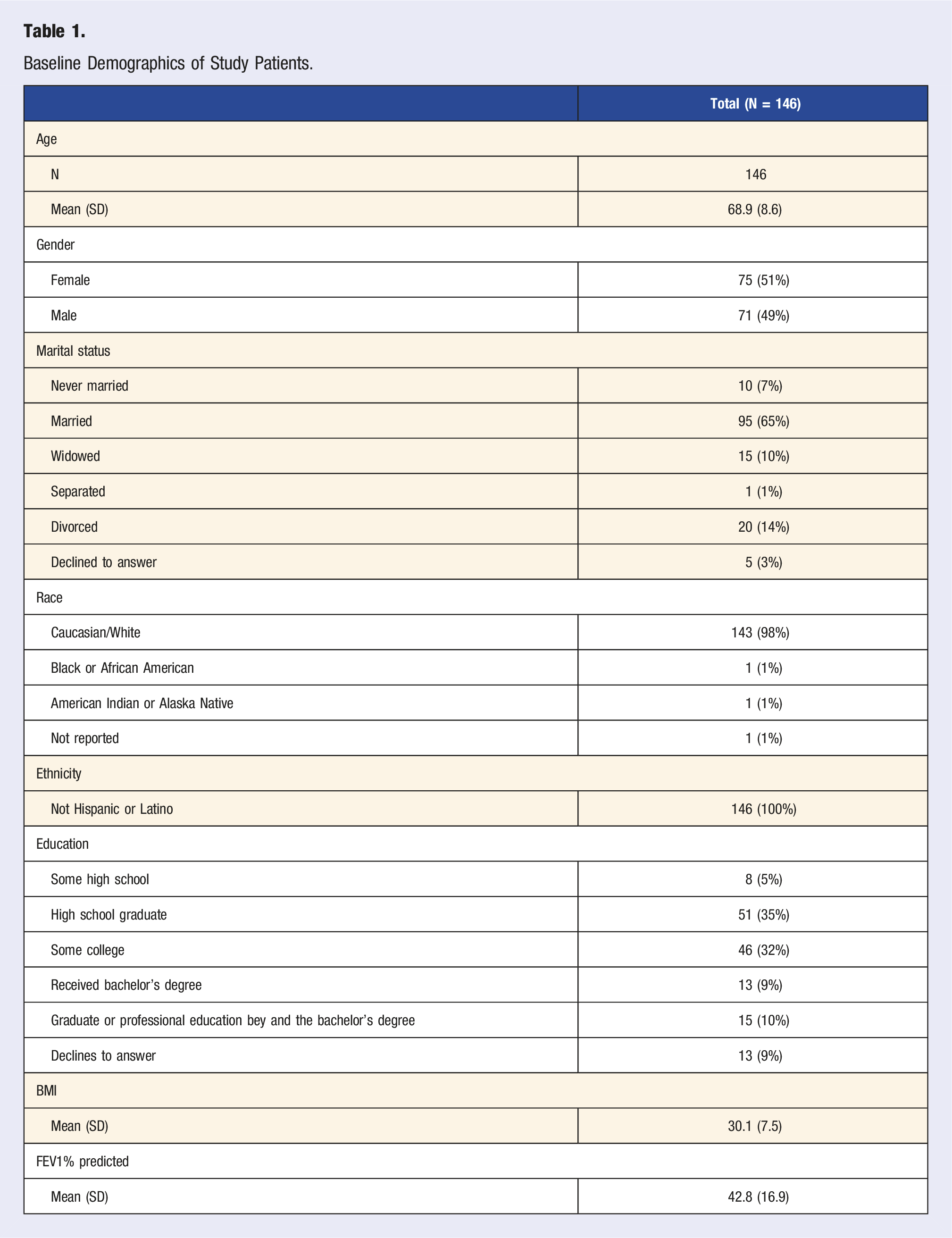
Baseline Demographics of Study Patients.
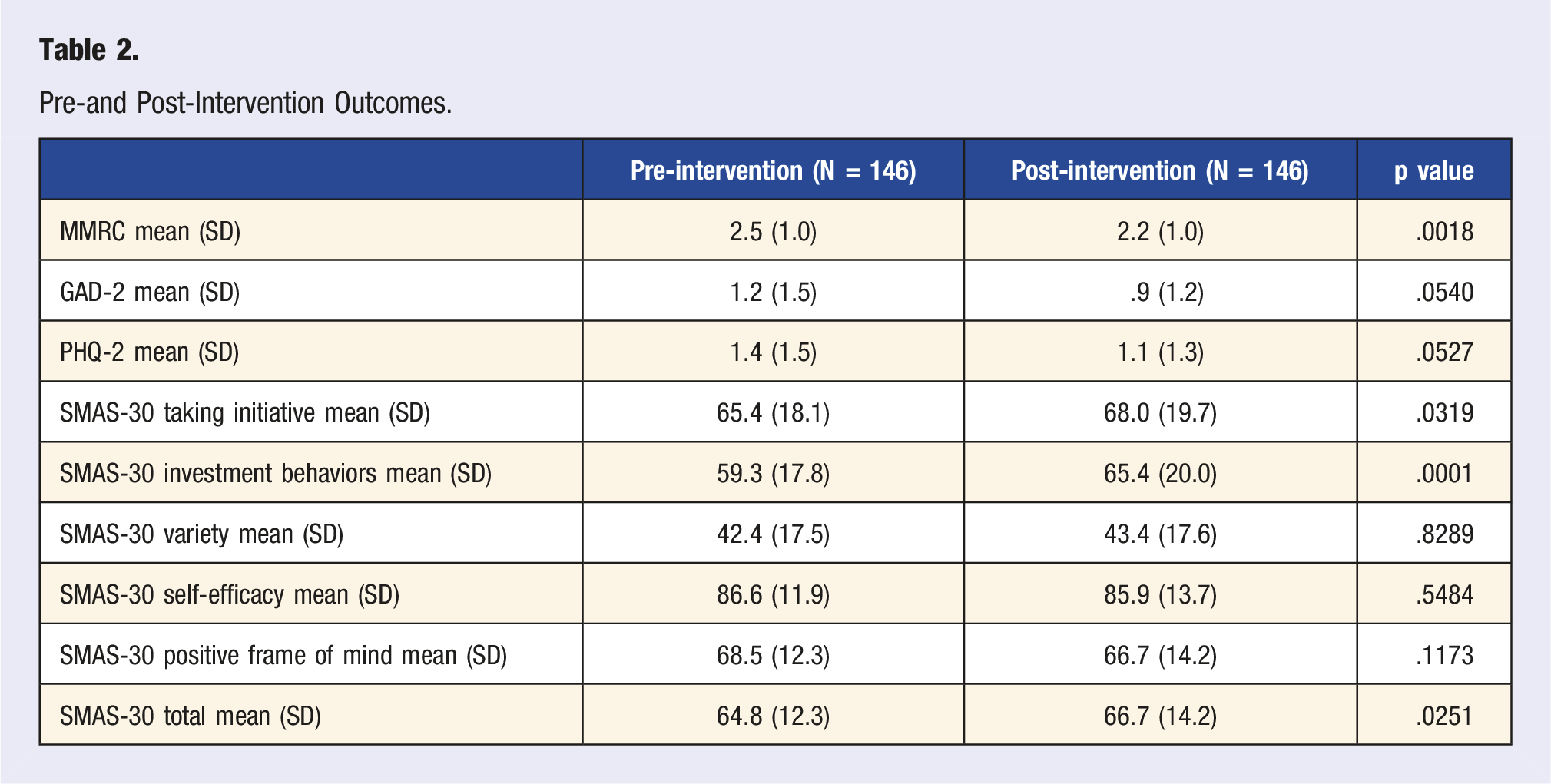
Pre-and Post-Intervention Outcomes.
The specifics of the health coaching telephone calls are as follows: 787 telephone calls were completed, and the mean (SD) call length was 13.2 (8.6) minutes. Goals were set on 52% of the telephone calls. The adherence to the telephone calls is shown in Figure 2: 63% of the patients took at least 6 of the 8 planned telephone calls. Only age was associated with adherence: older subjects were associated with having more intervention calls. Adherence to telephone calls.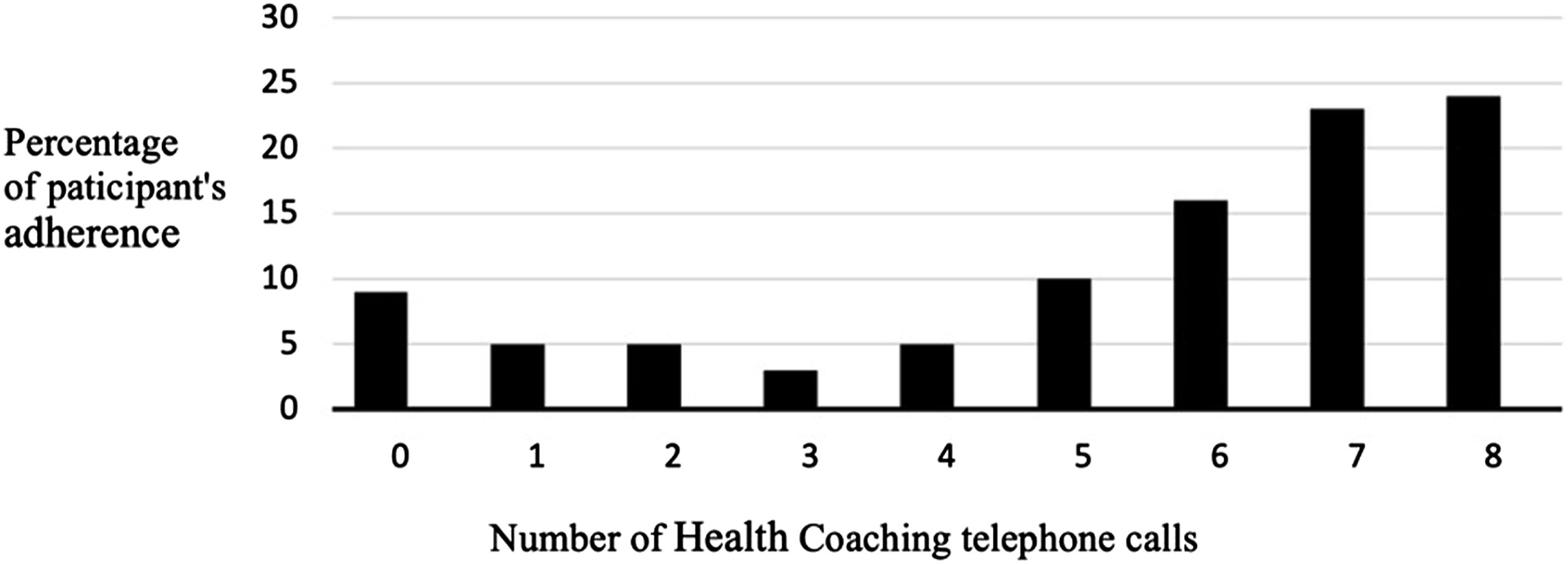
The health coaching topics discussed during the calls varied by week. Figure 3 shows that the two main topics elected by patients over the course of the 8-week intervention to be discussed were “Increasing physical activity,” and “Breathing more effectively.” Main topics of health coaching telephone calls throughout the 8 weeks.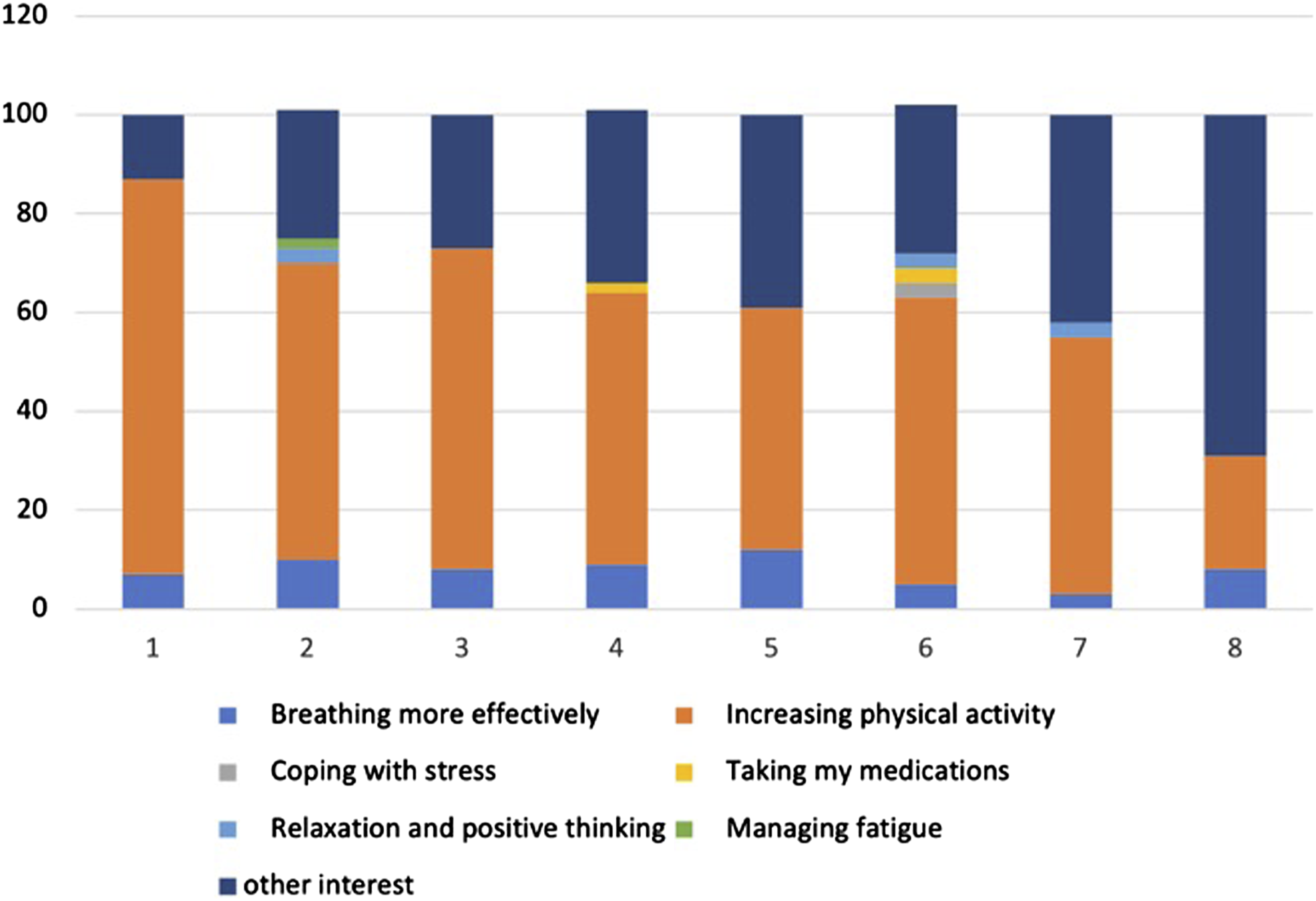
The working alliance inventory total score was 72 which is 85% of the maximum scores indicating a high degree of engagement between the HC and the patients. The Task, the Bond, and the Goal domain were 24, 25, 23, and which represent 80% of the maximum possible scores.
Lasso Model SMAS-30 Associations with WAI-SR. Lasso Models for SMAS-30 Total.
Discussion and Conclusion
We found a positive association between patient-HC engagement and COPD self-management abilities in this 8-week intervention. These results are novel for COPD health coaching interventions.
Our results also provide a mechanistic understanding of HC-patient engagement: We found that the WAI-SR Task and Bond were significantly associated with the measure of SM, but the WAI-SR Goal was not.
The WAI-SR Task domain refers to the agreement of what task is the focus of the health coaching session and the specific activity that the patient is interested in. Our findings further confirm previous work that indicates that discussing patient’s wishes and ambitions can lead to an agreement on the task and this leads to greater treatment satisfaction.26,27 One of the core features of the MI approach is the patient and HC collaboratively identify the overall focus and plan for each session. This process aligns with the task agreement domain of the WAI-SR, which was also recognized as important to COPD self-management.
The WAI-SR Bond domain refers to the positive relationship between the patient and HC that facilitates engagement with the program. It was expected that the therapeutic bond was identified as helpful in facilitating behavior change and COPD self-management given that the relationship between the coach and the patient is heavily encouraged in MI.27,28 Establishing a collaborative working relationship characterized by acceptance and empathic understanding is foundational in MI. 29 Often described as the “spirit of MI,” this skill was heavily emphasized throughout the health coaching training and ongoing fidelity monitoring.
The WAI-SR Goal domain of the working alliance inventory did not show association with self-management, which is thought-provoking. The latter agrees with MI theory: planning and goal-setting process are often not explicit in MI, distinguishing it from other expert-driven treatment approaches. 30 MI conceptualizes the patient as the expert in what will work for them. While the provider may elicit the patient’s ideas or goals, they generally participate minimally in the planning process. Health coaching with an MI approach allows the patient and HC to collaboratively identify the overall focus and plan for each session. Our findings contrast with other research that supports the working alliance is positively related to goal setting. 27 Additionally, the agreement on treatment goals, along with the trust and the bond, have been associated with better treatment outcomes in physical rehabilitation of low back pain and health coaching interventions for weight loss.10,31 Importantly, while goal setting was a planned component of health coaching intervention, it was only accomplished in 50% of the telephone calls in this study which may have impacted the WAI-SR bond score.
Our findings about the association of engagement (therapeutic alliance) with SM abilities are supported by previously published work by our research team:32–34 Patients with chronic conditions benefit from a positive wellness coaching relationship and could change their attitudes and approach to wellness.32–34 Other studies that have conducted regression analysis on anxiety treatments show that alliance predicts both outcome and dropout from treatment. 35 Positive therapeutic alliance has also been reported as beneficial in distant self-management programs for arthritis pain using an internet-based program and non-certified HCs. 12 In this research study, the health coaching relationship provided patients with a range of emotional or psychological benefits, including a sense of encouragement, reassurance, and understanding. 5 The health coaching was focused on being empathetic and supportive to enhance accountability in the SM process. We also found that screening positive for depression symptoms was associated to lower SM abilities. The latter suggests the need for additional efforts in those patients to personalize their SM programs.
Our results are novel for COPD but extend the previous finding from chronic disease research: Positive therapeutic engagement between provider and patient has been shown to improve patient health outcomes like pain reduction, adherence to treatments, physical rehabilitation, and weight management.10-12 We confirm that a strong engagement can improve adherence to healthy behaviors, providing the basis for positive treatment outcomes.11,12,36
The implementation and effectiveness of a telephonic health coaching intervention in medical patients warrant future research in specific patient populations. Other published studies show that one-to-one phone-based health coaching using motivational interviewing (MI) skills, mindful listening, and goal setting support, has been associated with improved self-management abilities, self-efficacy, health status, and medication adherence in a variety of chronic conditions including pain, diabetes, hypertension and hyperlipidemia and COPD.37-39 The working alliance can predict patient adherence to treatment, in this case, coaching calls.40,41 Learning engagement/communication skills like health coaching may be beneficial and synergistic to other interventions like pulmonary rehabilitation.
We have robust models based on an R2 of .48. R-square values can be between 0 and 1, with higher values being associated with better fitting models. Models for a social science study as low as 10% are generally accepted because human behavior cannot be accurately predicted. The R2, or the coefficient that shows the proportion of variance in the dependent variable that can be explained by the independent variables, informs how well the data fit the regression model was very high for a social science model.
We previously reported the feasibility and acceptability of this intervention: 42 In this publication, we further analyzed the adherence to the health coaching component. The maximum number of HC call that patients were expected to complete was eight, one per week. We were able to determine that 63% of the patients took at least six of the eight planned telephone calls. Regarding the acceptability, the high engagement shown by the WAI-SR results post-intervention shows that patients found the health coaching acceptable. We previously reported that health coaching can also be integrated into a primary care team approach to managing prediabetes43,44 and into breast cancer survivorship. 45
This study had limitations. The patients were primarily Caucasians, so how these results apply to diverse or underserved populations is unknown. We only measured the degree of engagement at one time point. Future studies should consider multiple measures of the patient-health coach relationship. Our results may benefit from further validation in other cohorts.
Practice Implications
The practical implication of these findings suggests that patient engagement matters: Our results highlight the importance of the relationship between the HC and the patient as it can positively influence self-management abilities in patients diagnosed with COPD. We provide mechanistic understating of the patient engagement as it relates to SM abilities in patients with COPD.
Footnotes
Acknowledgments
The authors thank Nyanjok Lam, Benjamin Thomas, and Allison Spradley for their work as health coaches.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Grant K24 HL138150 from the National Heart Lung and Blood Institute, National Institutes of Health, USA (Principal Investigator: Roberto Benzo).