
Abstract
Physical inactivity is an underrecognized and undertreated lifestyle behavior among patients with chronic obstructive pulmonary disease and is independently associated with a number of adverse health-related outcomes. Pulmonary rehabilitation with exercise training provides an efficacious intervention with short-term improvements, but it is an infrequently used modality and does not consistently result in longer term increases in physical activity. Similarly, pedometer self-monitoring with coaching has demonstrated short-term increases in physical activity. However, further research is needed to determine the optimal method to support long-term behavior change that will have the greatest benefit. While available evidence suggests that reversing physical inactivity is an essential component of self-management to optimize health, it is only one component of a complex set of interventions needed to support patients in adapting to their chronic condition. In the future, this support will ideally start with identification of specific patient phenotypes, which describes their adaptation to the condition based on patients’ knowledge, skills, confidence, symptoms, and impairments. This information will then be used to tailor education and behavior change strategies over the long term to promote sustainable physical activity and other healthy lifestyles.
‘Patients with COPD [chronic obstructive pulmonary disease] often have other comorbid conditions.’
In this issue are 2 articles relevant to lung health. Seguel et al 1 provides an overview of indoor exposures to toxic agents, and O’Reilly 2 reviews the diagnosis and management of chronic obstructive pulmonary disease (COPD). Both articles emphasize the need to eliminate chronic exposures to active tobacco smoking, secondhand smoke, biomass combustion products, and occupational particulate exposures to protect lung health, and prevent COPD and other chronic respiratory conditions.
While primary prevention of chronic conditions is the ideal through promotion of healthy lifestyles (eg, smoking cessation, physical activity, and weight control), for patients with established disease, interventions are also required to help patients “live well” and to minimize the burden on individuals and society. 3 As highlighted by O’Reilly, 2 patients with COPD often have other comorbid conditions. Worldwide, patients with multiple chronic conditions comprise one of the greatest public health and clinical challenges, which are a major driver of health care costs. 4 However, health care solutions alone will be insufficient because health status is determined by many factors outside of the health care realm (eg, social, environmental, health literacy, patient activation), 5 and because optimal management will require complex, integrated interventions at multiple levels including community, health care system, health care team, and individual. 3
While “living well” with a chronic condition may have different meanings for individuals, in general, patients’ goals are to maintain independence and control symptoms associated with their conditions (eg, dyspnea, fatigue, pain). 6 For patients with COPD, inhaled medications are the most common method used to control symptoms, and the priority of research and development efforts for future interventions. 7 However, technological solutions such as medications may be necessary, but alone will be insufficient to help patients optimally adapt to their condition.
Adaptation to “live well” with COPD or any other chronic condition is a process that all patients experience. 3 The process involves learning what to expect of their illness, accepting and coping with it, and ultimately learning to self-manage their condition (Table 1). 8 When patients first develop symptoms of dyspnea and/or fatigue, they often unwittingly adapt by doing less physical activity and may incorrectly attribute their symptoms to ageing and/or minimize their importance. 9 This maladaptive lifestyle change may go on for years before they seek medical attention and are diagnosed with COPD. Moreover, initially they may reject the diagnosis, 10 which may compromise adherence to recommendations. As symptoms worsen, patients experience progressive loss of exertional physical capacity, 11 compromising their ability to work or participate in pleasurable leisure-time activities. 12 These losses are associated with uncertainty about their prognosis that may result in fear about the future. 12 Unfortunately, in the current health care environment there is little or no support for self-management to assist patients to better understand their illness and to make necessary adaptations to “live well” with their condition. 3 Among these adaptive changes medication adherence and smoking cessation are commonly recognized and managed. In contrast, the clinical relevance of physical inactivity is underrecognized and addressed.
Definition of COPD Self-management.
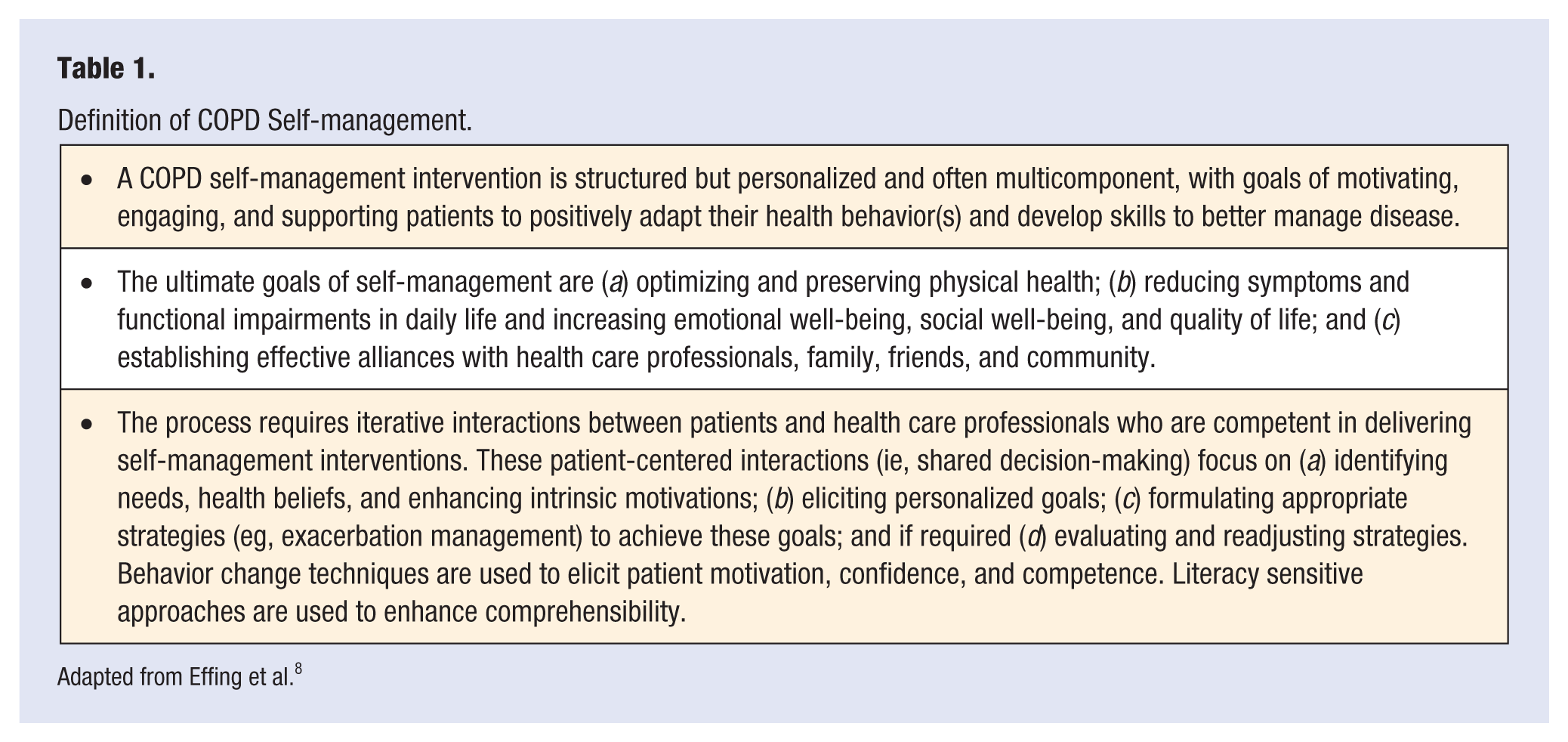
Adapted from Effing et al. 8
Physical inactivity among patients with COPD occurs early in the course of the condition, 13 and with more advanced impairment has consistently been associated with excess morbidity and mortality.14,15 Specific adverse health-related outcomes have included disability, 16 poorer health-related quality of life, 16 depletion of muscle mass, 16 comorbid conditions, 16 higher rates of hospitalizations,17-19 and mortality. 18 On average, COPD has been associated with an annual decline of about 400 steps per day, which is 2 to 4 times greater than healthy elderly. 16 Moreover, sustained physical inactivity over approximately 3 years is associated with depletion of muscle mass and clinically significant declines in functional capacity measured by 6-minute walk distance. 16
Pulmonary rehabilitation is an efficacious intervention to address many of the adverse outcomes associated with physical inactivity among patients with COPD. 20 This complex intervention composed of patient education and exercise training conducted over 8 to 12 weeks improves health-related quality of life, functional capacity, and reduces hospitalizations over 12 months. 20 However, few patients have access to these programs and the results are not consistently sustained long-term. 21 The lack of sustained benefit from pulmonary rehabilitation may be partly explained by a progressive decline in physical activity. 16 And interventions to increase physical activity using coaching and/or pedometers with feedback postrehabilitation have been inconsistent.21-23 However, even small increases in daily physical activity are associated with improved health outcomes. For example, the minimal important difference associated with reduced risk for hospitalization after pulmonary rehabilitation among patients with COPD is an improvement of only 600 steps per day. 24
Other interventions intended to increase physical activity have included physical activity advice/counseling, bronchodilator treatment, long-term oxygen, nutritional supplementation, nocturnal noninvasive ventilation, and neuromuscular electrical stimulation. 21 Of these interventions only physical activity advice/counseling and bronchodilator treatment are generalizable to all patients with COPD. However, the overall quality of these studies is considered very low. 21 Despite these limitations, the available evidence suggests that on average using objective measures of physical activity, coaching to increase physical activity, longer duration pulmonary rehabilitation programs, and bronchodilators all increase levels of physical activity by about 15% to 25% compared to usual care, which otherwise is associated with progressive decline in physical activity. However, in studies that have measured step counts,25-28 improvement has been documented in the short-term (≤4 months), but may not be sustained over longer periods. 28
In contrast to physical activity as an outcome, relatively few randomized controlled trials have examined the effectiveness of interventions intended to increase physical activity on specific health-related outcomes.25-31 And except for an Internet-mediated intervention using pedometer monitoring and feedback, 27 the interventions have primarily comprised providing patient education, self-monitoring with pedometers, and physical activity coaching. However, results have been inconsistent because these studies have been very heterogeneous with different target populations (primary vs specialty care); sample sizes (n = 35-305); behavior change strategies; intensity and duration of the coaching (4 weeks to 5 months); duration of follow-up (3 months to 18 months); and health outcomes measured (eg, health-related quality of life, functional capacity, health care utilization). For example, in the short-term (≤4 months) most have found improvements in health-related quality of life, but not with longer-term follow-up ranging from 6 to 18 months.28,29,31 Similarly, Mitchell and coworkers 29 found an improvement in functional capacity at 6 months measured by endurance shuttle walk test, but in 3 studies using the 6-minute walk test there has been no improvement at 3 to 18 months.26,30,31 Finally, the occurrence of hospitalizations has been inconsistent in 2 studies.29,31 Further research is needed to overcome the methodological heterogeneity of these studies in order to determine whether interventions intended to increase physical activity are effective for improving health-related outcomes.
In summary, physical inactivity is an underrecognized and undertreated lifestyle behavior among patients with COPD that is independently associated with a number of adverse health-related outcomes that compromise patients’ ability to “live well.” Pulmonary rehabilitation with exercise training provides an efficacious intervention with short-term improvements, but it is an infrequently used modality and does not consistently result in longer-term increases in physical activity. Similarly, pedometer self-monitoring with coaching may result in short-term increases in physical activity, but further research is needed 9 to determine the optimal method to support long-term behavior change that will have the greatest reach, effectiveness, adoption, implementation, and maintenance. 32 Moreover, while available evidence suggests that reversing physical inactivity is an essential component of self-management, it is only one component of a complex set of interventions needed to support patients in adapting to their chronic condition (Table 1). 8 In the future, this support will ideally start with identification of specific patient phenotypes, which describes their adaptation to the condition based on patients’ knowledge, skills, confidence, symptoms, and impairments. 33 This information will then be used to tailor education and behavior change strategies over the long-term to promote sustainable physical activity and other healthy lifestyles among patients with COPD.11,14,15,21
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.