
Abstract
Introduction
The relevance of lifestyle medicine in diabetes treatment is now incorporated in clinical practice guidelines but finding an exemplar for the creation of a Lifestyle Medicine Program (LMP) is a difficult task.
Aim
To use Lifedoc Health (LDH) as a LMP exemplar by describing their multidisciplinary team (MDT) approach to diabetes care along with tactics to address sustainability challenges.
Results
The LDH model facilitates early activation of patients with diabetes and other cardiometabolic risk factors, MDT approaches, and protocols/policies that are able to overcome barriers to equitable healthcare in the community. Specific programmatic targets are clinical outcomes, effective dissemination, economic viability, and sustainability. Infrastructure centers on patient-driven problem-based visits, shared medical appointments, telemedicine, and patient tracking. Further discussions on program conceptualization and operationalization are provided.
Conclusion
Even though strategic plans for LMPs that specialize in diabetes care are well represented in the literature, implementation protocols, and performance metrics are lacking. The LDH experience provides a starting point for those healthcare professionals interested in translating ideas into action.
Keywords
“The description of the LDH LMP offers a comprehensive illustration of tactical planning and execution.”
Introduction
The prevalence of diabetes has increased in the U.S. from 7.7% to 13.3% from 1999–2000 to 2015–2016 (90–95% are type 2 diabetes [T2D]) following the same trend as other regions in the Americas. 1 Effective and sustainable actions are required to mitigate the burden and consequences of diabetes. However, successful preventive strategies to reduce T2D incidence and progression, such as the National Diabetes Prevention Program (DPP) 2 and the Diabetes Self-Management Education and Support Program 3 are not easy to implement into practice. Most patients with T2D present with other cardiometabolic risk factors and comorbid conditions, including abnormal adiposity, hypertension, and dyslipidemia. Additionally, T2D progression and management are deeply influenced by social determinants of health (SDOH), as well as ethnocultural and behavioral factors, 4 which are elements that must be taken into consideration for successful implementation of preventive strategies.
In clinical practice guidelines, lifestyle medicine strategies in T2D care focus on the incorporation of nutrition, physical activity, smoking cessation, alcohol moderation, sleep hygiene, and behavioral support, 5 with levels of intensification depending on disease severity. The implementation of these strategies (long-term goals) begins with translation into a tactical plan (short-term actions), which is followed by a materialization process. Conceptualization is the first materialization step, followed by operationalization. These 2 steps define the targeted population, develop diagnostic and management protocols based on the population’s ethnocultural risk profile, and then set realistic financial projections to ensure sustainability and growth.6,7 Lifestyle medicine programs (LMPs; including Centers and Clinical Service Lines) play a critical role in narrowing practice gaps. However, descriptions of this process to enable large scale implementation are scarce. 8
Lifedoc Health (LDH) was designed according to a practice model that can address the glaring barriers compromising care for patients with cardiometabolic-based chronic disease (CMBCD) in the Greater Memphis Area. Since 2005, this translational-research center has been dedicated to building a self-sustained and outcome-oriented resource that detects and manages populations at high risk for T2D, obesity, and associated complications. The key feature of LDH is a primary framework focused on characterization of a particular patient’s cohort in order to better understand the complexity and real-life evolution of cardiometabolic drivers in the population. Data collection platforms and protocols for systematic capture are the central provision of this dynamic model.
The objective of this review is to present the Lifedoc Health model as an exemplar of a LMP for diabetes and cardiometabolic care. A multidisciplinary team (MDT) approach will be described, and the process of implementation outlined. In addition, sustainability challenges especially from the standpoint of ethnocultural factors and SDOH will be discussed.
LDH Care Model
Lifedoc health is a multidisciplinary and data-driven healthcare organization committed to preventing and treating dysglycemia (insulin resistance, prediabetes, and T2D), abnormal adiposity (including overweight/obesity), and their adverse consequences. The LDH programs have received state and National Committee for Quality Assurance (NCQA) recognition and accreditation for over 10 years. 9 Within LDH, there are various clinical service lines that encompass primary and specialty care, acute and chronic conditions, as well as care coordination, pharmacy, patient education, and lifestyle medicine into a unified dynamic approach to patient care. Healthcare professionals (HCPs) undergo protocol training and reinforcement, and primary care providers (PCP) are coached to achieve early activation of patients, with or at risk of cardiometabolic conditions, for co-management by the multidisciplinary team.
The LDH model was designed under the Family-Centered Medical Home (FCMH) model with 3 main aims: MDT approach, validation of outcomes, and building systems based on data collection and analysis to refine the model. The LDH model includes 5 components. The first is risk screening through the LDH’s Diabetes and Cardiovascular Risk Stratification Program, eye exam, cardiology tests, and collecting information about SDOH, ethnocultural factors, lifestyle, and risk behaviors. The second is activation of those patients with at least 1 risk factor to interventions. The third is clinical intervention applying an evidence-based MDT protocol that includes visits provided by nurse practitioners supervised by an endocrinologist, lifestyle medicine, care coordination, shared medical appointments, cardiometabolic-related drug-curriculum, and psychological intervention when needed. The fourth is to reduce inequities by implementing an affiliation program that increases access to healthcare to uninsured patients (e.g., Vida Plus program) via culturally competent services. The bulk of the assigned and referred patients are under some type of governmental healthcare plan (e.g., Medicare or Medicaid) or uninsured. In essence, the LDH model has an inclusive protocol in which any patient could benefit from it regardless of their socio-cultural strata, racial background, or insurance coverage. The last and fifth component of the FCMH model is the inclusion of community-based programs that include nutrition education and healthcare in schools (e.g., Wave for Health Program) and the healthy prepared meal program to reduce food insecurity. Also, within the LDH model is a monthly patient newsletter with educational content about health, lifestyle, nutrition, and exercise. Also, as part of ongoing medical education for HCPs and staff members, an educational meeting (i.e., inservice meeting) is delivered every month. This includes lectures to update the current knowledge about strategic and operational topics. Population characterization, risk stratification and efforts validating interventions has been reported to optimize the LDH model.7,10-22
An analysis of the LDH patient population showed that over 70% of the children, adolescents, and young adults with obesity exhibited 3 or more cardiovascular disease risk factors. Additionally, 13% of patients with overweight or obesity undergoing risk stratification had either prediabetes or unknown T2D, and close to one-third of them have either elevated blood pressure or established hypertension. Data from 2018 showed that 68% of the patients having at least 1 cardiometabolic condition (overweight/obesity, prediabetes/T2D, or hypertension) and 97% of the patients with a glycated hemoglobin A1C (A1C) ≥ 6.5% began the MDT protocol, 23 reflecting the PCP’s awareness regarding the importance of the MDT approach.
The LDH protocol has resulted in a decreased number of cardiovascular disease risk factors among patients and demonstrable financial sustainability, in part because patient activation is associated with those codes and procedures that are covered by insurance companies. The LDH clinics serve between 8000 and 10 000 active patients per year, of which 83% are African American or Hispanic, 44% younger than 21 years of age, and 85% under government insurance or cash coverage, with a 3-year patient retention rate close to 70% and a sustained growth of 11% year over year. 24
LDH Implementation Modalities
Implementation modalities in the LDH model span clinical practice, research, and education. The LDH relies primarily on clinical practice, with research conducted through Lifedoc Research PLLC, a sister company dedicated to clinical trials, investigator-initiated studies, and both translational and population-based research. Evidence generated from research studies can optimize intervention protocols, specify transcultural components, generate novel hypotheses, and lead to publications in peer-review journals. Education to HCPs and staff is an ongoing process. For example, contacts have been established with local universities to formalize a training program in chronic cardiometabolic diseases for nurse practitioners. Lifedoc health members are also involved in continuing medical education, such as lectures, research training programs, and other activities associated with research grants.
Clinical Intervention Protocols
Within the LDH model, there is an emphasis on diabetes and cardiovascular risk stratification that fosters preventive interventions and dynamic insulin algorithms. In this type of protocol, patients are activated through involvement with an MDT when ≥1 cardiometabolic condition (overweight/obesity, prediabetes/diabetes, or hypertension) is detected. Once activated, a visit is scheduled to collect blood samples following a ≥8 h overnight fast for a cardiometabolic laboratory profile, including a 75 g oral glucose tolerance test (OGTT) with serum glucose and insulin samples at 0, 30, 60, 90, and 120 minutes. Lifestyle recommendations are provided by an exercise physiologist. If needed, patients then undergo protocolized pharmacotherapy. Specifically, those with overweight/obesity are treated with topiramate (25 mg po BID) and low dose phentermine (18.5 mg po QD) unless contraindicated or otherwise not tolerated. Those with insulin resistance are treated with metformin (1500 mg po daily in split doses initially and then uptitrated to 2000 mg a day). Patients with T2D are treated with anti-diabetic drugs clinically proven to promote weight loss, primarily metformin and either incretin-based (e.g., glucagon-like peptide 1 receptor agonist [GLP1ra] or dipeptidyl-peptidase 4 inhibitor [DPP4i]) or sodium-glucose cotransporter-2 inhibitor (SGLT2i) therapies. Specific medications are selected according to individual clinical conditions and insurance coverage. Additional follow-up and engagement protocols are tailored according to individual needs (Figure 1). Lifedoc Health clinical intervention protocol. Abbreviations: BID: twice a day, BMI: Body mass index, CVD: Cardiovascular disease, DBP: Diastolic blood pressure, DM: Diabetes, DPP-4: Dipeptidyl-peptidase 4 inhibitors, Echo: Echocardiography, GLP-1: Glucagon-like peptide 1, ICD-10: International Classification of Diseases 10, LDH: Lifedoc Health, OGTT: Oral glucose tolerance test, QD: Once a day, SGLT-2: Sodium-Glucose Cotransporter-2 inhibitors, SBP: Systolic blood pressure, T2D: Type 2 diabetes.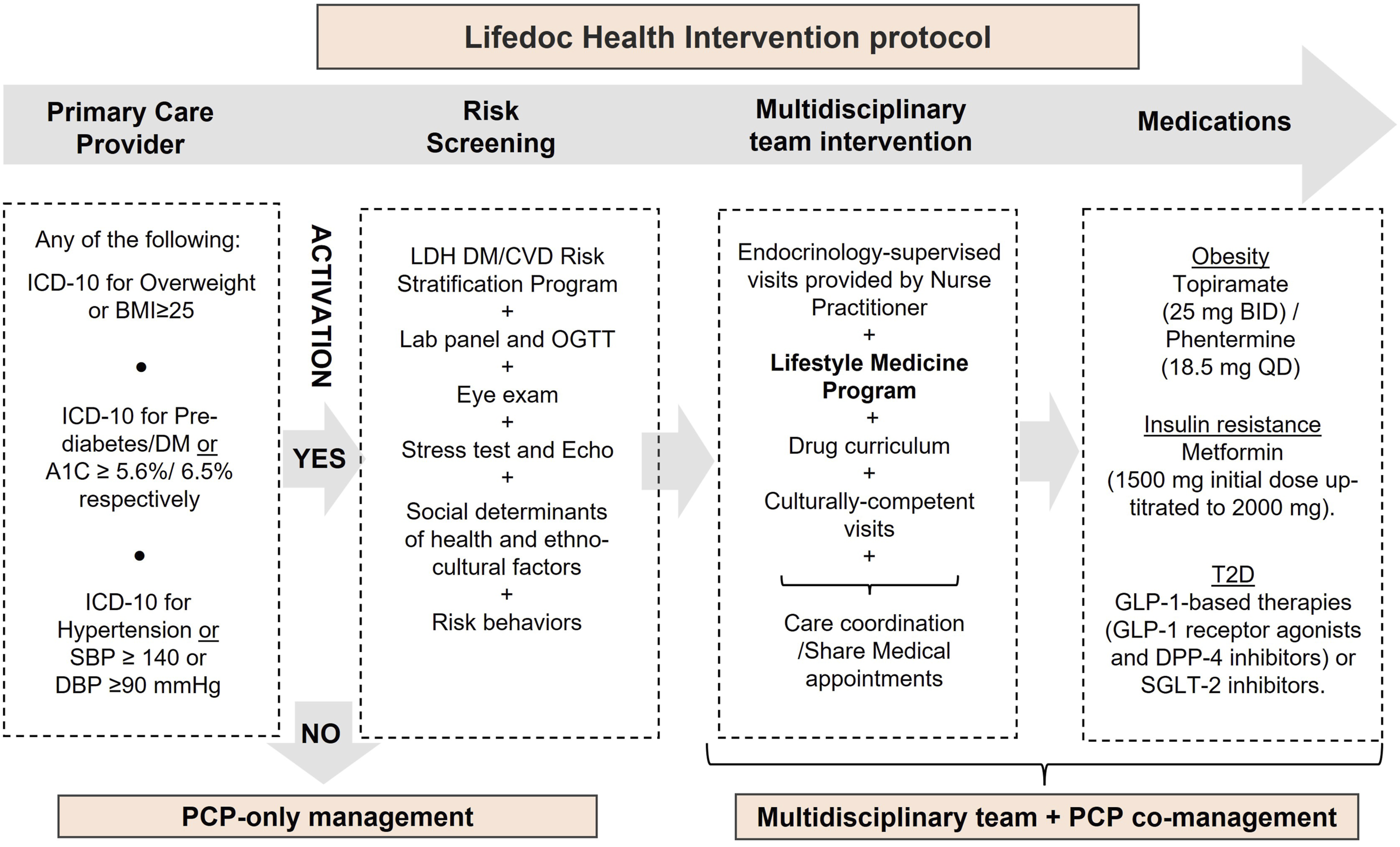
LDH MDT Outcomes
A 1-year retrospective review in 2018 of 598 adults (African American 59%, Hispanic 35%, and Caucasian 6%) with a mean age of 43.8 years ±14.0 was performed. Activated patients (≥1 cardiometabolic risk factors of overweight/obesity, prediabetes/diabetes, or hypertension) who were treated under an MDT protocol were compared to patients who qualified for MDT but instead were treated solely by a PCP. After 1 year of intervention, patients treated by the MDT had a greater reduction (β, 95% CI) in weight (− 4.29 kg, −7.62, −.97), body mass index (−1.43 kg/m2, −2.68, −.18), systolic blood pressure (− 2.18 mmHg, −4.09, −.26), and diastolic blood pressure (− 1.97 mmHg, −3.34, −.60). They also had 77% higher odds of reducing their initial weight by ≥ 5%, 83% higher odds of reducing their body mass index by ≥ 1 point, and 59% higher odds of reducing their diastolic blood pressure by ≥2 mmHg. The number of encounters was an important factor in these positive results. The average number of visits for the total sample was 10.5 but was 2 times higher in the MDT group (12.3) compared to the PCP group (6.6). Among those engaged with the MDT, 30.9% of their visits were for lifestyle intervention. 23
Lifestyle Medicine at LDH
The Implementation Process
For 15 years, the LDH model has provided lifestyle medicine recommendations to patients with obesity and diabetes within an MDT approach. Before the COVID-19 pandemic, group exercise classes, especially in youth, were part of the usual routine of lifestyle interventions. This approach has now been updated by incorporating rigorous standardization to expand the program, replicate outcomes, facilitate personnel training for new satellites centers, and optimize lifestyle interventions. The purpose is to decrease the risk and progression of cardiometabolic chronic diseases in at-risk populations, while investing in new expert leadership and organizational infrastructure. This update of LDH operations adhered with the methodology proposed by Mechanick and Kushner
25
(Figure 2). Conceptual framework for the implementation of the Lifestyle Medicine Program at Lifedoc Health. Adapted from reference 57. Abbreviations: FCMH: Family Center Medical Home; HCPs: Health Care providers; LDH: Lifedoc Health; tCMBCD: Transcultural cardiometabolic-based chronic disease.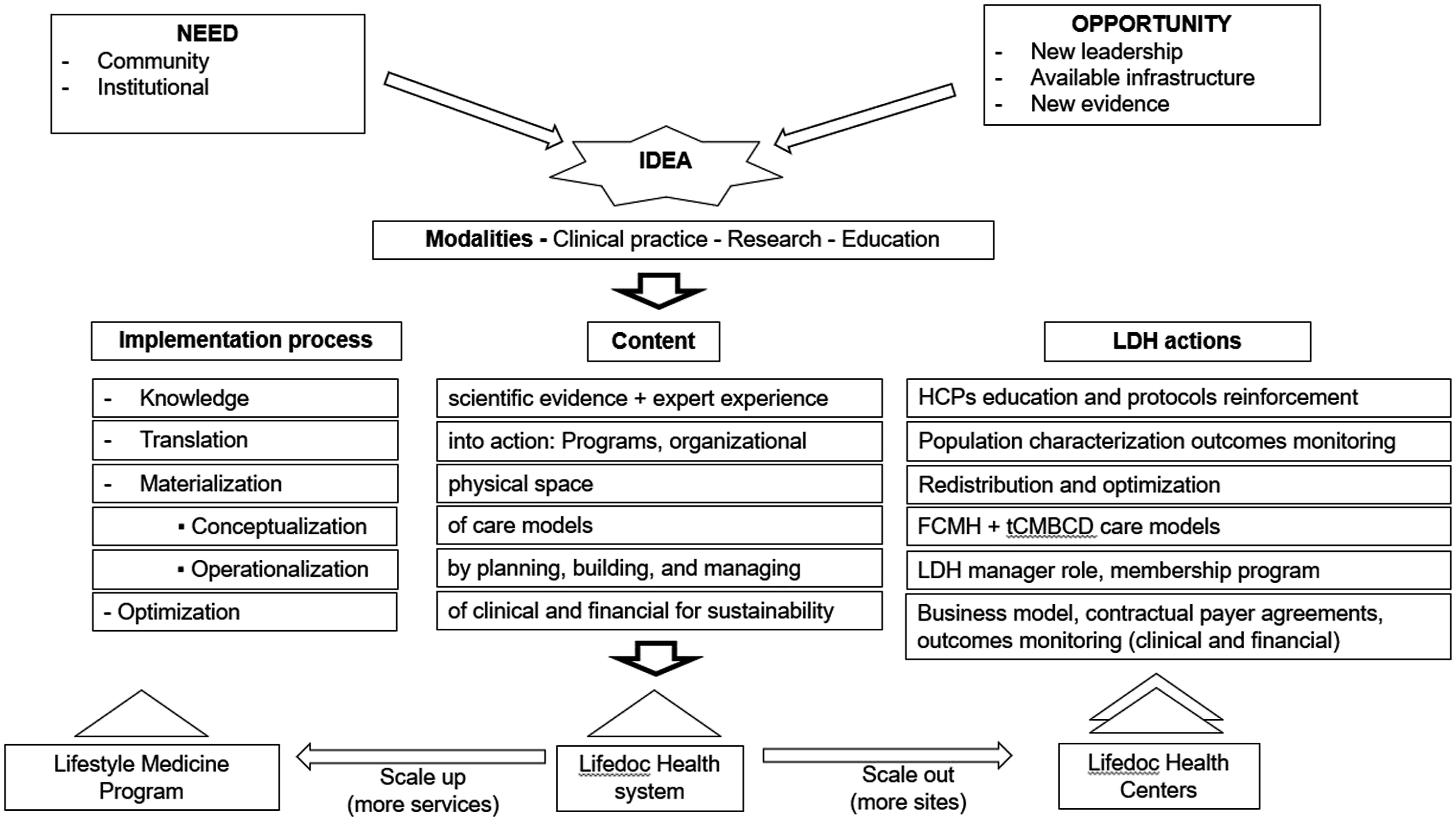
Implementation science involves well-designed multilevel processes that apply evidence-based actions into routine healthcare. 26 However, barriers or “determinants of practice,” including financial and human resources, time constraints, ethnocultural factors, and SDOH, must be used to adapt these interventions to achieve necessary changes. 27 Implementation of the LDH program began with the characterization of the population based on cardiometabolic risk profile, then definition of lifestyle interventional protocols addressing SDOH and transcultural factors, redistribution of existing physical spaces, and eventually “translation” of both evidence-based theoretical frameworks and clinical outcomes expressed in the real-world environment. The subsequent “materialization” process began with “conceptualization” of the care model, followed by “operationalization” (planning, building, and managing), including a process for continuous clinical and financial “optimization” to achieve sustainability. At a later point, the LDH program was scaled up by opening a third location with plans to open 4 more centers in the next 2 years to cover a larger geographic area in Memphis (Figure 2). Codification of these various sequential processes facilitates implementation with the materialization step being the most critical.
The first materialization step is a detailed conceptualization of the idea to be built-out
Interventions to prevent, treat and reverse the progression of diabetes and other cardiometabolic chronic conditions should focus on identifying the most prevalent risk factors in the target population.6,28 The LDH programs are based on overcoming the barriers to access healthcare in the community served and therefore must meet 4 established LDH premises: (1) Can patients be helped? (Clinical outcomes) (2) Can whole populations be helped? (dissemination), (3) Can the program be financially advantageous? (economics), and (4) Can these positive results be sustained? (sustainability). The LDH program leadership continuously adapts to changing environmental pressures optimize resource allocation in this conceptualization process.
Specifically, the LDH programs merged the Family-Centered Medical Home (FCMH) and transcultural CMBCD (tCMBCD) concepts into a structured model. The main objectives of this new model are applicability, actionability, and sustainability for early intervention (e.g., during childhood).29,30 The tCMBCD comprises 3 dimensions: stages, drivers, and SDOH. In the first dimension, the 4 stages are mapped to specific prevention modalities: 1 (Risk—primordial prevention of risk development and progression), 2 (Predisease—primary prevention of disease), 3 (Disease—secondary prevention of complications), and 4 (Complications—tertiary prevention of suffering and mortality); each stage is also subject to quaternary prevention (the avoidance of overmedicalization and unethical behavior).29,31,32 In the second dimension, individual metabolic drivers are considered as progressing along these 4 stages. For example, the dysglycemia-based chronic disease (DBCD) model constitutes a new way to approach diabetes prevention and management: stage 1 is insulin resistance, stage 2 prediabetes, stage 3 T2D, and stage 4 cardiovascular complications. By adopting this paradigm, culturally adapted preventive care is applied at earlier stages .33,34 The DBCD model aims to resolve the controversy around insulin resistance and the diagnosis of prediabetes incorporating them as specific DBCD stages in the progression of dysglycemia and incorporating them as an actionable entity for early prevention. When other metabolic drivers (e.g., abnormal adiposity [adiposity-based chronic disease; ABCD], hypertension [hypertension-based chronic disease; HBCD], and dyslipidemia [lipid-based chronic disease; LBCD] are configured along the 4 stages, a 2 × 2 matrix arises and depicts the 2-dimensional CMBCD framework.29,32 In the third dimension, each stage and driver (represented by each cell of the 2 × 2 CMBCD matrix) is populated by SDOH and other ethnocultural factors to improve precision of preventive actions and optimize outcomes (Figure 3). Implementing this model in the daily routine clinical practice implies the staging of the patient’s individual risk for each biological driver (adiposity, dysglycemia, hypertension, dyslipidemia) and the incorporation of social determinants to specify the lifestyle recommendations. The transcultural Cardiometabolic-Based Chronic Disease (tCMBCD) model. The tCMBCD model describes the natural history of the cardiometabolic disease continuum, its drivers, preventive interventions, and opportunity for transculturalization at each stage. Abbreviations: ABCD: Adiposity-Based Chronic Disease; CMBCD: Cardiometabolic-Based Chronic Disease; DBCD: Dysglycemia-Based Chronic Disease; MetS: Metabolic Syndrome.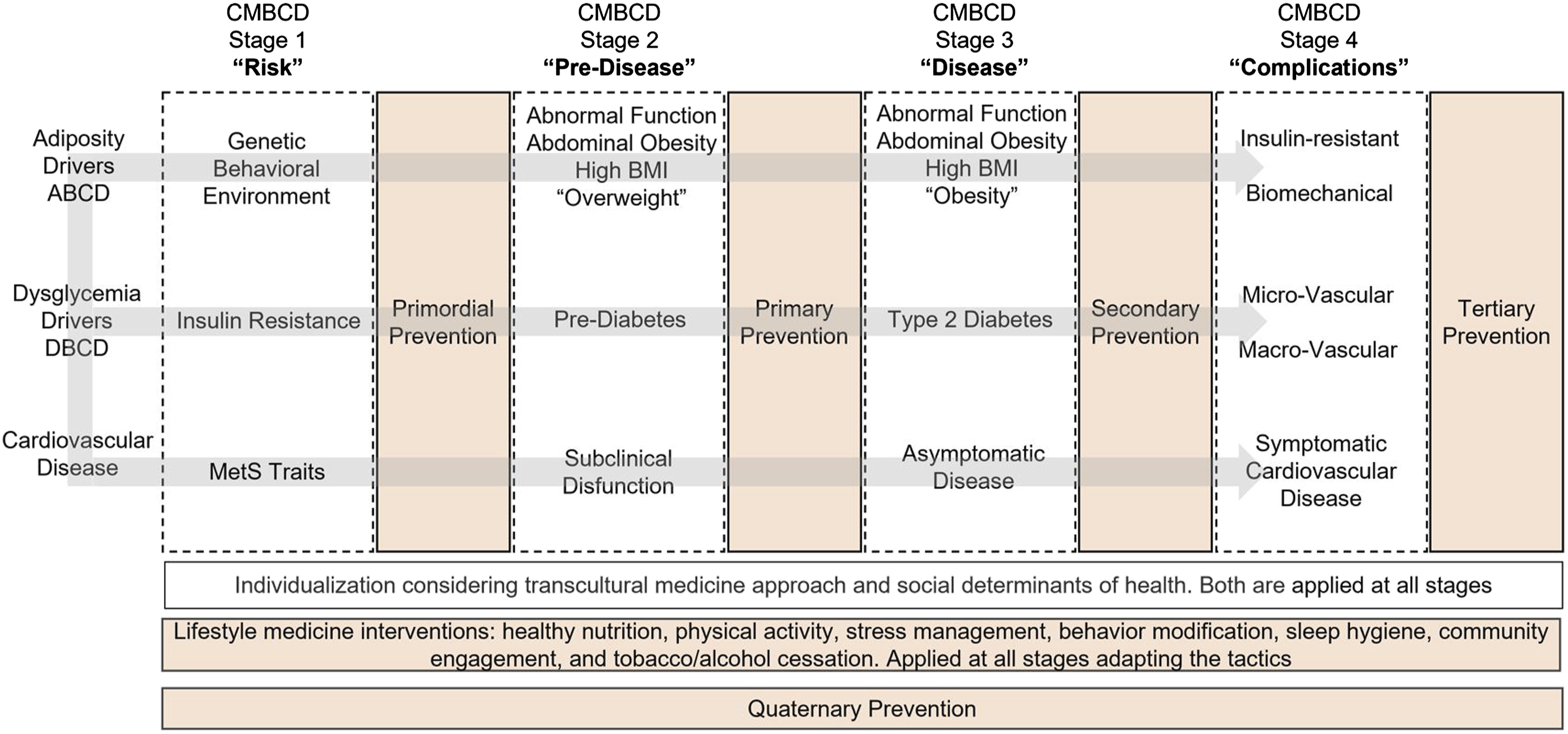
The second materialization step is operationalization of the new LDH programmatic concept
Lifestyle medicine was framed within the mission (To build healthier communities by preventing diabetes and obesity through healthcare and research) and vision (A healthier community with equitable access to healthcare) statement of the institution, followed by a strategic plan are created and included the design of a core academic curriculum consisting of 6 segments, each with specific objectives and actions: CMBCD; lifestyle medicine; translation of strategies into clinical practice; resources management; community expansion; education and research, and business plan. At a more granular level, these segments contain policies and protocols that are audited, vetted, adapted over time, and consequently evolve to allow for success and sustainability.
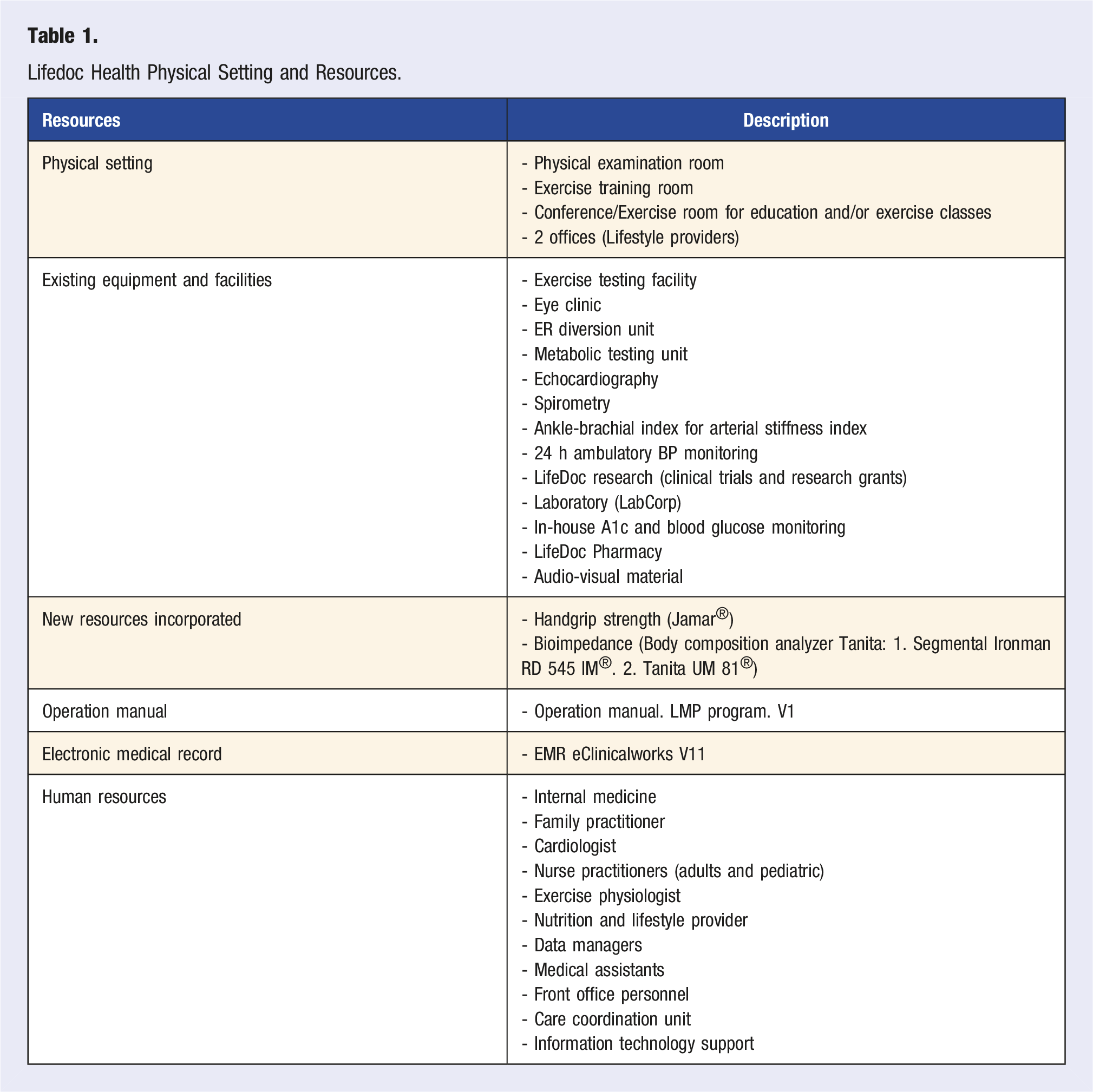
Resources
Lifedoc Health Physical Setting and Resources.
Initial Structure and Subsequent Adaptations
The LDH programs were designed based on analysis of DPP lifestyle recommendations for diabetes prevention and clinical outcomes,
35
American Association of Clinical Endocrinology guidelines for cardiometabolic risk management,
5
various diabetes self-management education and support programs,
3
general reviews of lifestyle medicine in T2D,
36
and guidelines on creating a lifestyle medicine center and/or clinical service line.
37
The initial LDH protocol consisted of establishing a sequence of visits per year based on the patient’s needs and evolution. On average, patients attend 11 flexible-scheduled visits per year (3 for lifestyle education, 4 with providers, and the rest are shared medical appointments). During this process, an interesting opportunity for adaptation emerged: diabetes and obesity were recognized as independent interventions prompting even more structured patient encounters. However, the program had a >50% dropout that could potentially compromise sustainability. Subsequently, compensatory strategies were formulated to integrate more personalized lifestyle medicine infrastructure for those patients with a higher level of complexity. In contrast, less complex cases are referred to group educational sessions (Figure 4). Thus, risk-stratification protocols became part of conceptualization and operationalization steps. These adjustments have produced an increase in the number of visits with better integration among MDT members. Lifestyle Medicine Program at Lifedoc Health: flow chart of visits. Abbreviations: MDT: Multidisciplinary team, MNT: Medical Nutrition Therapy, SDOH: Social determinants of Health, SMA: Share medical appointment.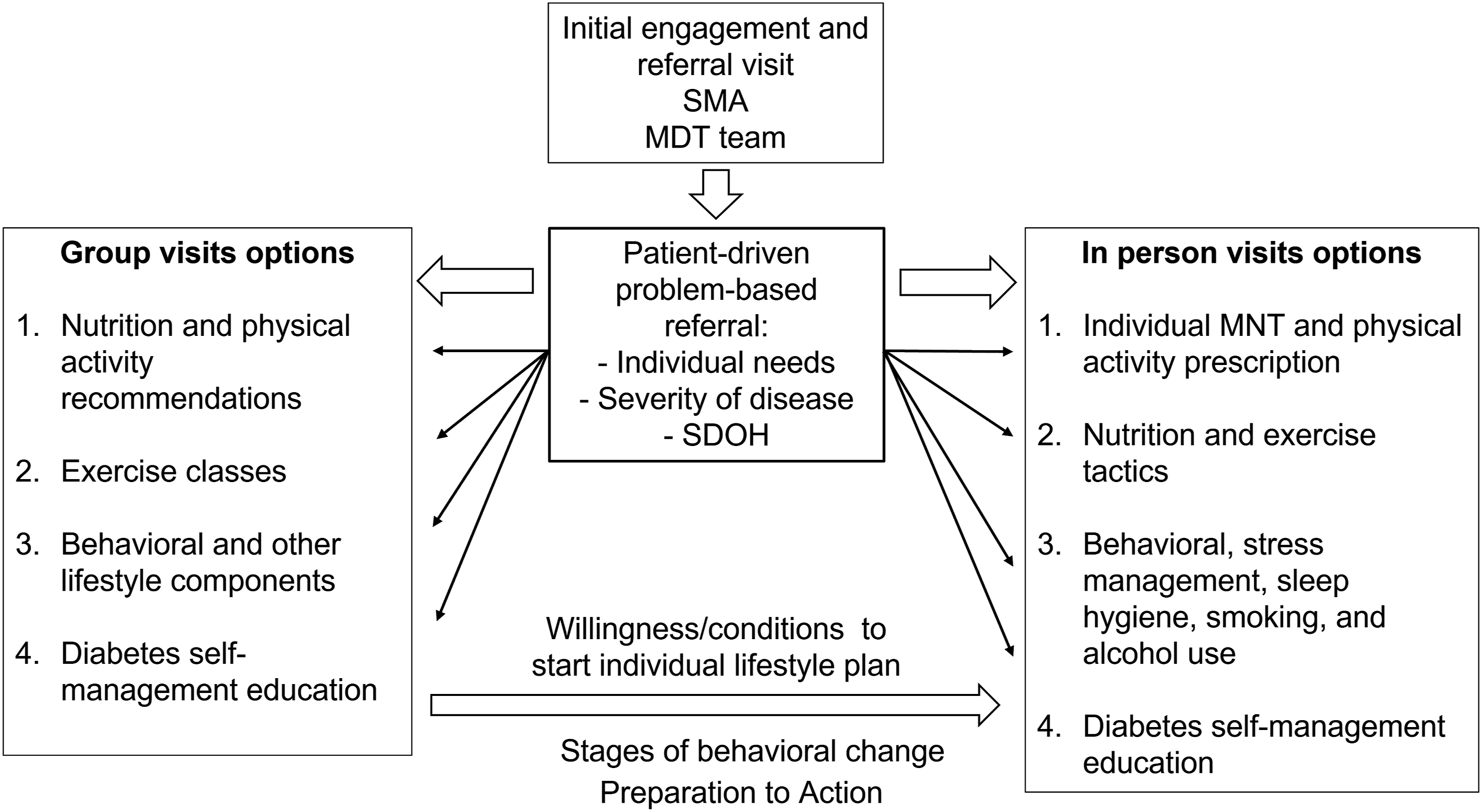
Operationally, the first patient encounter in the LDH program aim to motivate and engage the patient and increased the knowledge-based and understanding of their conditions and potential risks. The next visits include a lifestyle medicine diagnosis and then general recommendations centered on the Mediterranean and low glycemic index dietary patterns. During the in-person visits, patients were given personalized, culturally adapted lifestyle medicine prescriptions adapted to their routines. Tactically, medical nutrition therapy (MNT) was adapted to patients’ preferences and comorbidities offering different strategies. Of the initial 604 MNT prescriptions, 76.6% were healthy culturally adapted meal plans based on Mediterranean diet pattern including low glycemic index options, 16.7% had meal replacements, 4.0% intermittent fasting, 1.5% vegetarian diets, and 1.2% special requirements (hyperlipidemia, athletes, among others). Physical activity prescriptions included exercises for stretching, flexibility, balancing, aerobic conditioning, and muscle strength. For the aerobic component, intensity based on heart rate, duration, and frequency were specified. There were also goals set for the number of steps using pedometers and active pauses at the workplace. Physical activity plans were prescribed according to the patient’s preferences, sports activities that the patient had practiced, and available resources (gym, treadmill, weights, bands, swimming pool, parks, or sports fields nearby). In patients with diabetes, MNT included carbohydrate counting when appropriate, education about insulin adjustments, strategies to overcome the resistance both from patient and provider to initiate insulin treatment, 38 tailored physical activity goals, and education. Most patients with severe hyperglycemia were managed in the protocol-based outpatient emergency room-diversion unit. Those patients demonstrating a willingness for significant lifestyle change, in a behavioral state somewhere between the preparation and action stages, 39 were referred to the in-person visit program. Reinforcement and tracking with telemedicine visits were added when in-person visits were not feasible or as otherwise needed.
Lifestyle Medicine Program Content and Strategies for Cardiometabolic-Based Chronic Disease Management.
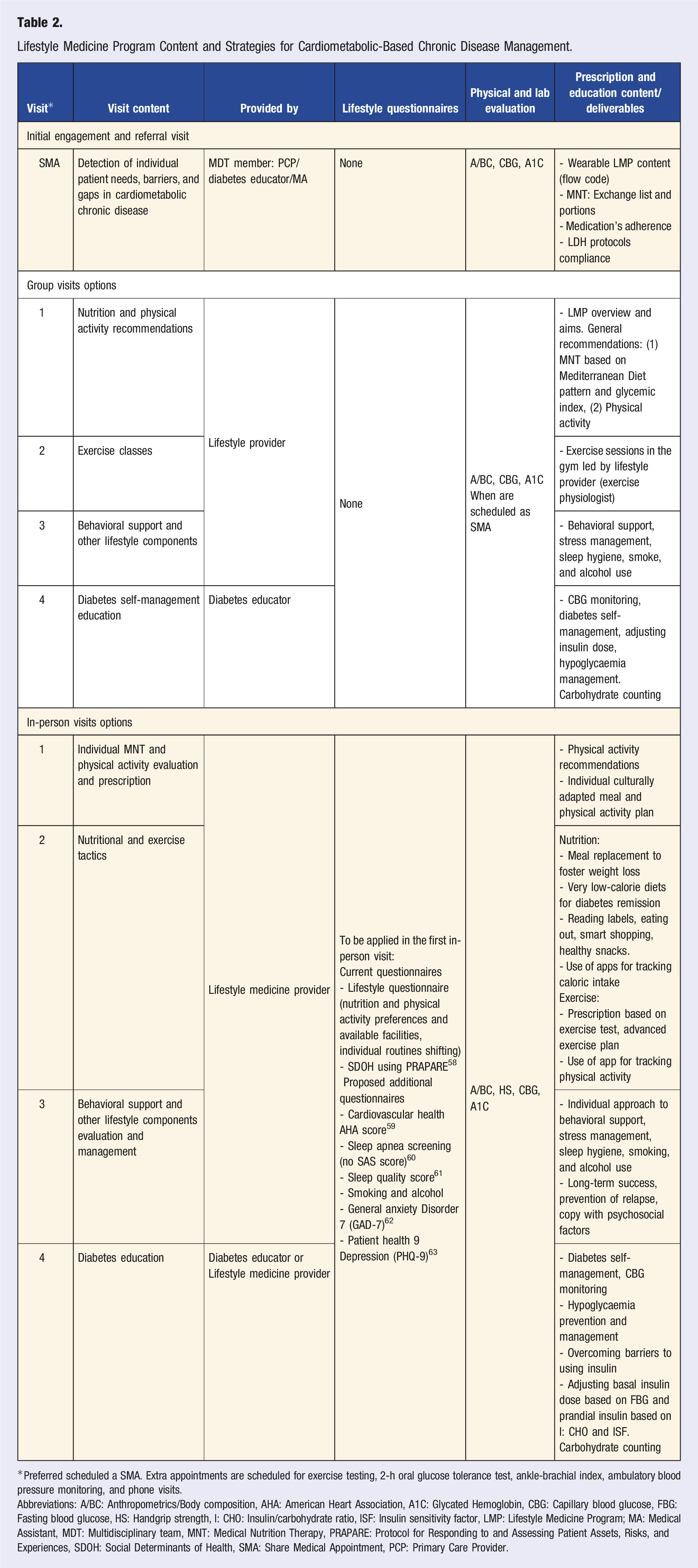
*Preferred scheduled a SMA. Extra appointments are scheduled for exercise testing, 2-h oral glucose tolerance test, ankle-brachial index, ambulatory blood pressure monitoring, and phone visits.
Abbreviations: A/BC: Anthropometrics/Body composition, AHA: American Heart Association, A1C: Glycated Hemoglobin, CBG: Capillary blood glucose, FBG: Fasting blood glucose, HS: Handgrip strength, I: CHO: Insulin/carbohydrate ratio, ISF: Insulin sensitivity factor, LMP: Lifestyle Medicine Program; MA: Medical Assistant, MDT: Multidisciplinary team, MNT: Medical Nutrition Therapy, PRAPARE: Protocol for Responding to and Assessing Patient Assets, Risks, and Experiences, SDOH: Social Determinants of Health, SMA: Share Medical Appointment, PCP: Primary Care Provider.
Transcultural Components
Among African Americans, compared with the general American population, there are disproportionately high morbidity and mortality rates, lower quality and accessibility to health care, less representative randomized controlled study data, more ketosis-prone diabetes, and more associated metabolic syndrome traits.4,42 Among Latino/Hispanics, abdominal obesity, prediabetes, high triglycerides, and fatty liver disease 43 are important drivers, and unhealthy food preferences, physical inactivity, diabetes complications, insulin resistance, 44 and poor adherence to diabetes treatment are more prevalent compared with other U.S. ethnicities. 4 Moreover, language barriers are significant among Latino/Hispanics with 21% not speaking English and only 5% of physicians and 2% of nurses being Latino/Hispanics. 4 In the LDH population, although the majority of their children speak English, more than 80% of their parent adult Hispanic are not fluent in English.
Cultural competency describes a set of behaviors, attitudes, and policies that enable a healthcare system to work more effectively within a transcultural context. 45 In other words, to better incorporate transcultural components so the precision of screening and lifestyle interventions can be maximized. 34 The LDH programs are culturally competent and therefore recognize and include cultural aspects to improve the interactions between patients and HCPs, and consequently the effectiveness of healthcare delivery. 45 Considering that the Hispanic and African American populations represent 83% of adults and 95% of youth patients, 90% of the LDH personnel is bilingual (i.e., English and Spanish speaking). Also, key LDH personnel are trained to improve (1) knowledge about community demographics and the relevant SDOH, (2) attitudes toward ethnocultural diversity, health inequities, and respect for cultural differences, and (3) skills related to transcultural communication and patient-centered healthcare.
One of the major limiting factors for treatment adherence and program engagement is the lack of affordable patient transportation to the Center. At LDH, approximately 35% of scheduled patients are under simultaneous clinical visits including, education, procedures, laboratory, eye clinic, specialty, or primary care; these are arranged based on patients’ needs or gaps in care. In addition, LDH’s pharmacists are part of the MDT approach, and they work in close collaboration with HCPs and patients to educate, synchronize, and consolidate prescriptions. Likewise, LDH’s Medical Treatment Management (MTM) program provides extra support for patient treatment adherence, education, and monitoring. On average, 700 MTM visits a month are implemented and close to 3000 prescriptions every month are delivered to patients during the clinical visits or sent at home without additional charges. These elements enhance the relationship between the patient and healthcare team, overcoming barriers and gaps in the healthcare process, increasing access to care, activating the patient for change, and finally improving outcomes. 45
Food Preferences and Nutrition Behaviors in Lifedoc Health African American Patients (n = 94).
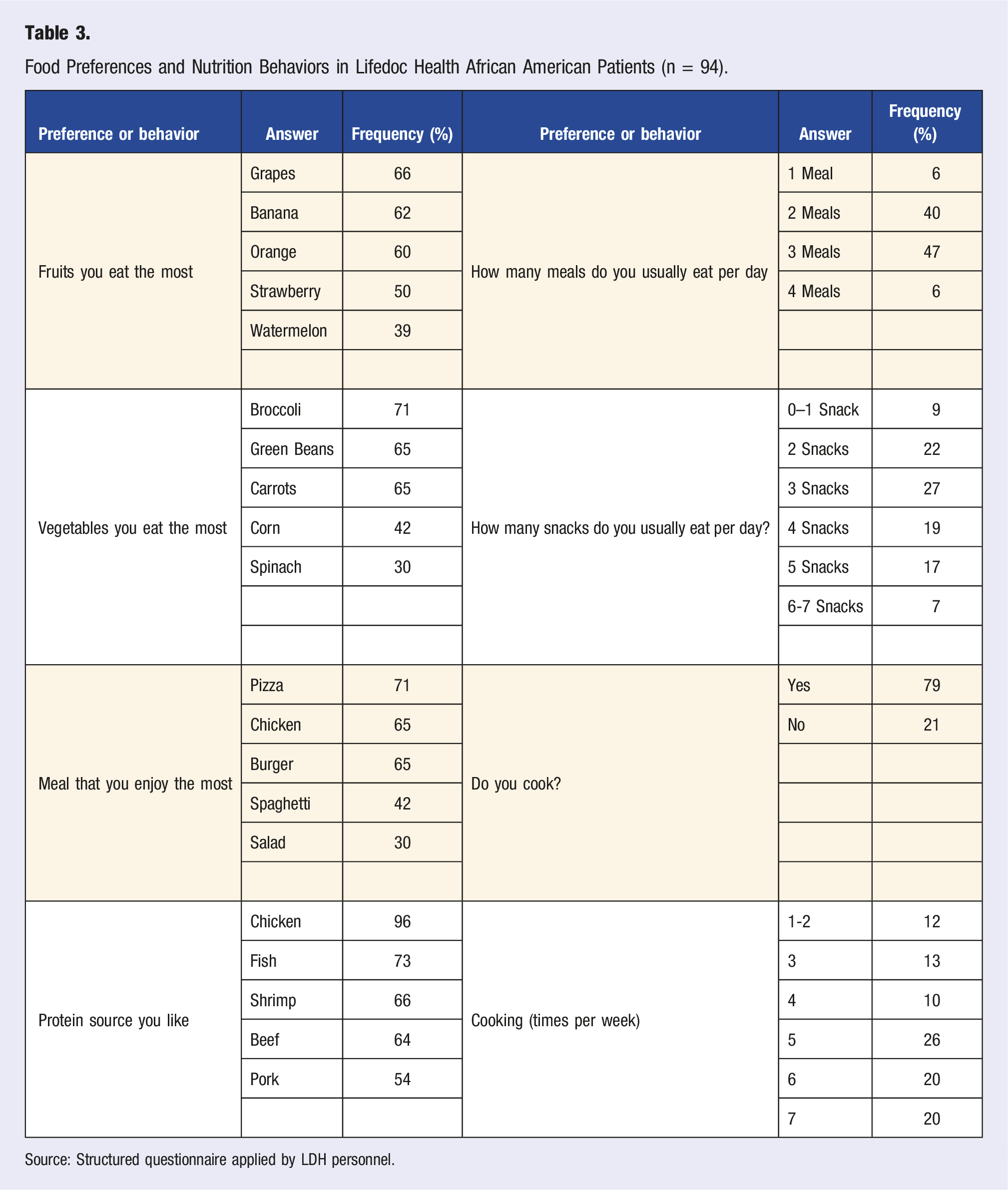
Source: Structured questionnaire applied by LDH personnel.
Outcomes During the LMP Updating Period
Lifestyle Medicine Program Visits and Prescriptions in the first 14 months After the Updating Process.
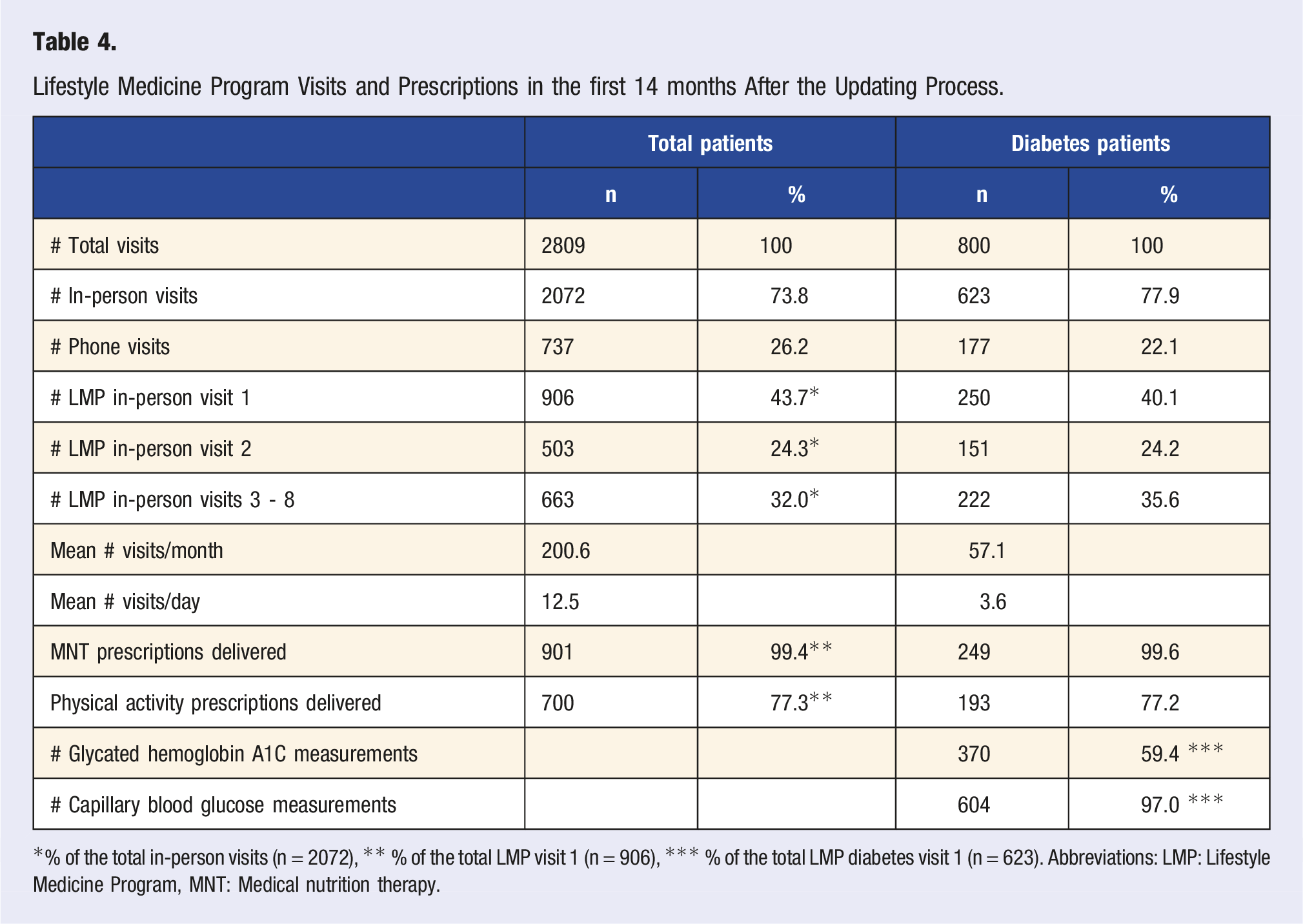
*% of the total in-person visits (n = 2072), ** % of the total LMP visit 1 (n = 906), *** % of the total LMP diabetes visit 1 (n = 623). Abbreviations: LMP: Lifestyle Medicine Program, MNT: Medical nutrition therapy.
Changes in Cardiometabolic Lifestyle Medicine Program Outcomes by Age Groups
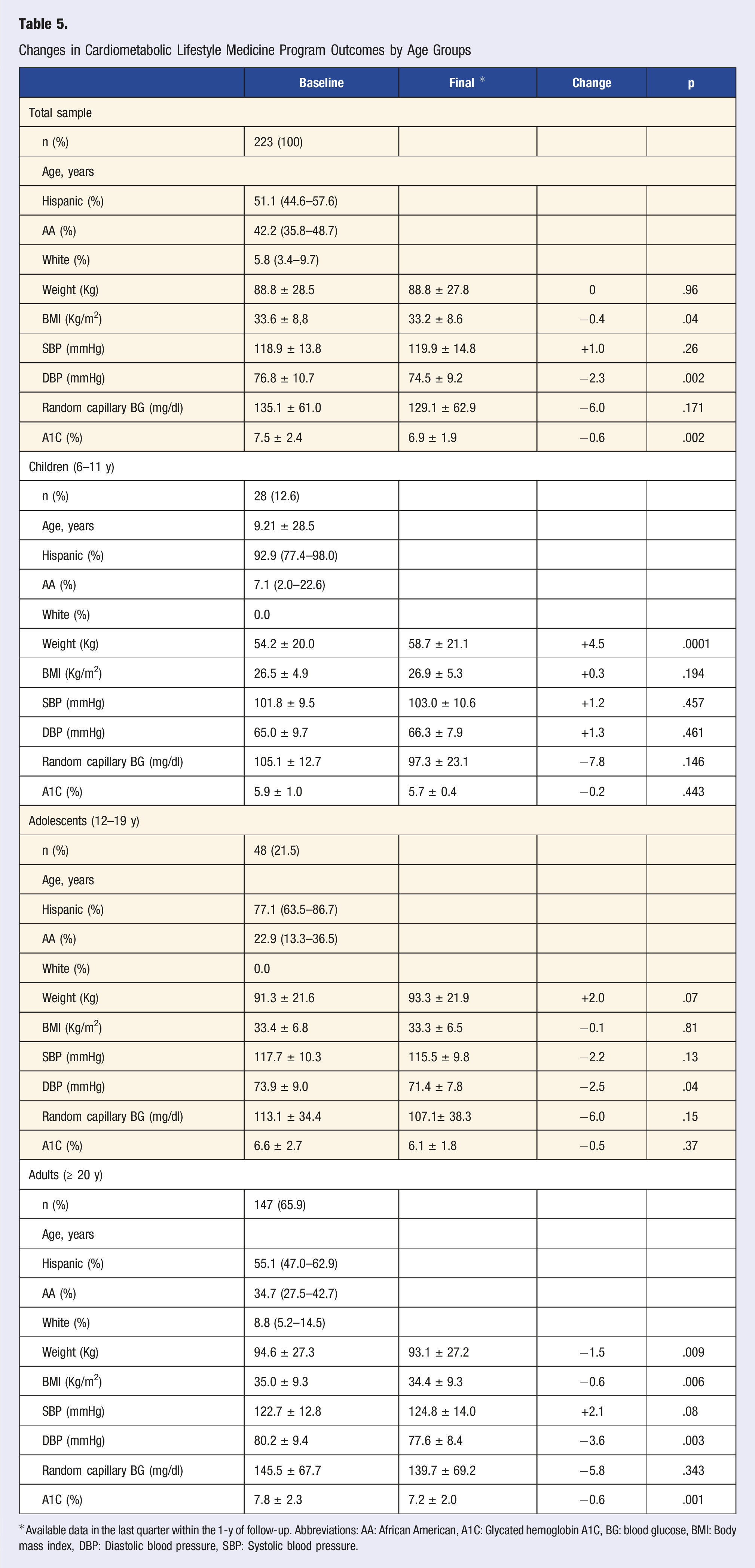
*Available data in the last quarter within the 1-y of follow-up. Abbreviations: AA: African American, A1C: Glycated hemoglobin A1C, BG: blood glucose, BMI: Body mass index, DBP: Diastolic blood pressure, SBP: Systolic blood pressure.
Business Model and Economic Sustainability
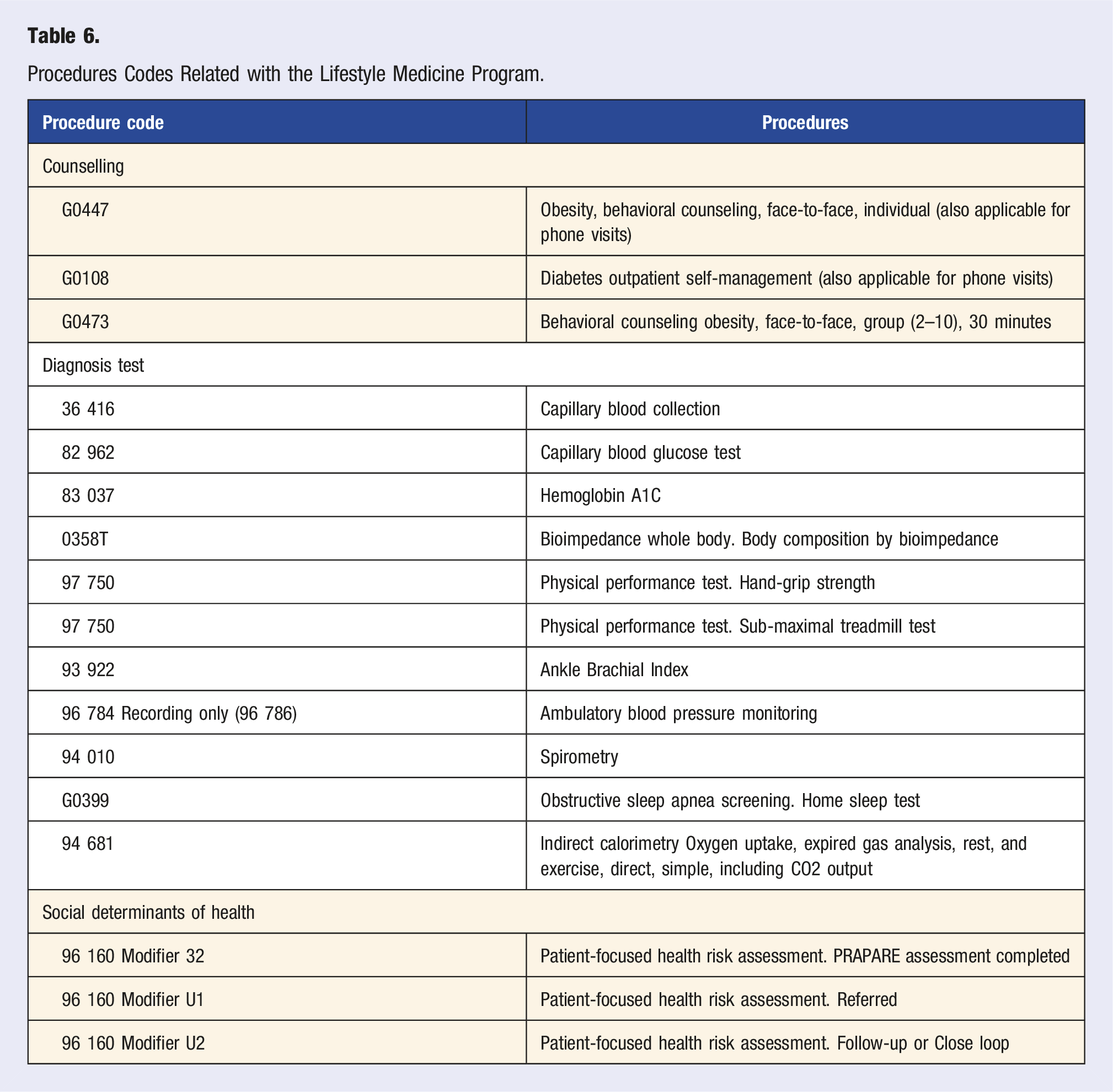
Procedures Codes Related with the Lifestyle Medicine Program.
Long-term sustainability implies both clinical and economic success. In the process of evaluation, LDH programs target all clinical outcomes required for the program to be recognized by the Diabetes Recognition Program of the NCQA. This includes: • having an A1C over 9% in <15% of patients, with A1C <8% in at least 60% and <7% in at least 40%; • having a blood pressure >140/90 mmHg in <35% of patients and <130/80 mmHg in >24% of patients; • having an LDL-cholesterol > 130 mg/dl in <37% of patients and an LDL-cholesterol <100 mg/dl in >36% of patients; • having a documented eye exam in >60% of patients; • having a documented nephropathy assessment in >80% of patients; • having a documented foot examination in >80% of patients; • and having documented smoking status and cessation advice or treatment in >80% of patients.
9
Economic targets to achieve self-sustainability for all LDH programs and their various clinical service lines (clinical practice, LMP, cardiology diagnosis services, education, research, etc.) are considered in aggregate. As new clinical services are proposed during scale-up discussions, they are analyzed using unit economics and reviewed with LDH finance personnel with respect to marketability and sustainability. For example, vibration perception threshold test and arterial stiffness evaluation were useful tools to determine early the end organ impact. However, both were considered experimental procedures and no reimbursable code could be signed. During the LMP update period, an initial financial evaluation of obstructive sleep apnea screening using home sleep testing and indirect calorimetry to assess resting metabolic rate and substrate oxidation for precision MNT counseling did not support self-sustainability when considering third-party reimbursements.
Limitations and Challenges
T2D is a complex disease that must be treated with a combination of personalized lifestyle and medications using advancements in behavioral change technologies, eHealth, health literacy, and personal health data valorization. Lifedoc health is a regional “ecosystem” that combines some of the necessary instruments (education, diagnostics, medication, most of these trying to be personalized and integrated) reducing healthcare costs but is immersed in a healthcare system dominated by industry and insurance companies which only hinders the sustainability of the LMP. 47
Barriers to the LDH LMP’s success include factors from patients, HCPs, health system, and environment. Among patients’ barriers are non-physical contextual factors, such as ethnocultural factors and structural conflict—society’s tendency to change and develop due to perpetual conflict between classes—(e.g., discrimination 48 /oppression) 49 and deterioration (e.g., housing/amenities). 50 Many adverse myths and false beliefs about insulin among African Americans with uncontrolled T2D compromise diabetes care and outcomes and are based on fears, fatalism, self-blame, stigma, frustration, self-care fatigue, and misconceptions among family, friends, co-workers, and HCPs. 4 In the Hispanic population, fears of insulin derive from concerns about hypoglycemia, weight gain, pain, efforts adhering to single or multiple injections, the association of insulin with complications such as amputation and blindness, trust in HCPs, and the positive belief in folk remedies, also compromising treatment adherence and diabetes control. 51 The SDOHs are crucial factors in diabetes management. 52 According to the LDH experience, these SDOHs include lack of transportation or insurance, low income, low health literacy, and work-related constraints for appointments, which contribute to the high proportion of no-shows.
Barriers that are related to HCPs, mainly the PCPs, include clinical inertia and under-recognition of early DBCD and CMBCD stages and obesity stigma. In addition, both time constraints on HCPs and multimorbidities frequently can impose barriers to better outcomes in PCP-driven interventions. Finding qualified HCPs has been a permanent challenge; stiff learning curve about the protocol and outcome-oriented approach, limited understanding of the early risk stratification and the need of intensive intervention, several gaps in their practice skills and evidence-based intervention, poor understanding of the disease mechanism has been significant limitations.
Healthcare system and institutional variables, such as costs, staff turnover, high demand of patients that exceeds the capacity of attention, low third-party reimbursements, and onerous paperwork imposed by payers can influence implementation and effectiveness. Economical aspects also pose challenges since payers generally prefer a fee-for-service reimbursement model, which contributes to the implementation of a volume-driven practice restricting the visit duration and making it difficult for management of patients with multiple competing chronic conditions. The environment is also an important determinant. The LDH LMP began operations during the COVID-19 pandemic and mandated social distancing protocols, which disrupted patients' routines by decreasing the quality of food, reducing physical activity, and adversely affecting other lifestyle behaviors, 53 promoting weight increase, 54 worsening diabetes control, 55 and exacerbating other cardiometabolic risk factors. 56 Moreover, pre-COVID-19 group exercise activities became restricted and in-person appointments were reduced. Lastly, a poorly resolved challenge for any healthcare initiative that has also influenced implementation tactic for LDH programs is striking an optimal balance between massification of lifestyle medicine practices and individualization of recommendations.
From a macro perspective, the mid-term goals of the LDH LMP are to (1) progressively incorporate all lifestyle components; (2) adapt business plans to scale up and out Centers to better serve communities; and (3) continually perform environmental scans to locate realistic funding sources. Under current practice and reimbursement scenarios, an independent, free-standing, self-sustaining LMP is unrealistic. So, for now, the LMP is conceptualized as a clinical service line to support LDH preventive and clinical functions while generating favorable economic outcomes.
Conclusion
Lifestyle medicine is now explicitly part of guidelines in diabetes care. Detailed descriptions of the implementation of lifestyle centers including diabetes care in the U.S. are scarce, so finding a role model for the creation of a Lifestyle Medicine Center, program, or clinical service line is difficult. The description of the LDH LMP offers a comprehensive illustration of tactical planning and execution. Knowledge acquisition, strategics, translation into action, and implementation was accomplished, but LMP has been effective and sustainable only by the integration into LDH clinical model. The creation and optimization of existing formal lifestyle medicine endeavors, especially in cardiometabolic-based chronic disease, is encouraged to foment a transformative healthcare culture that emphasizes prevention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JIM reports receiving honoraria from Abbott Nutrition for lectures and is on Advisory Board of Twin Health.