
Abstract
Disparities in type 2 diabetes (T2D) care is a global problem across diverse cultures. The Dysglycemia-Based Chronic Disease (DBCD) model promotes early and sustainable interventions along the insulin resistance (stage 1), prediabetes (stage 2), T2D (stage 3), and complications (stage 4) spectrum. In this model, lifestyle medicine is the cornerstone of preventive care to reduce DBCD progression and the socioeconomic/biological burden of disease. A comprehensive literature review, spanning 2000 to 2021, was performed and 55 studies were included examining the effects of lifestyle medicine and their cultural adaptions with different prevention modalities. In stage 1, primordial prevention targets modifiable primary drivers (behavior and environment), unhealthy lifestyles, abnormal adiposity, and insulin resistance with educational and motivational health promotion activities at individual, group, community, and population-based scales. Primary, secondary, and tertiary prevention targets individuals with mild hyperglycemia, severe hyperglycemia, and complications, respectively, using programs that incorporate structured lifestyle interventions. Culturally adapted lifestyle change in primary and secondary prevention improved quality of life and biomarkers, but with a limited impact of tertiary prevention on cardiovascular events. In conclusion, lifestyle medicine with cultural adaptations is an integral part of preventive care in patients with T2D. However, considerable research gaps exist, especially for tertiary prevention.
“From 2020 to 2021, the COVID-19 pandemic signaled that affected patients with T2D were at greater risk for more severe clinical course”
Introduction
Type 2 diabetes (T2D) represents one of the largest public health burdens worldwide, increasing independent of population growth, aging, and income, 1 therefore implicating many complex and ill-defined factors. Culture describes the cluster of shared nonphysical human attributes in a particular population, and when merged with ethnicity, which includes shared physical attributes, produces the more pragmatic “ethno-cultural” descriptor. Lifestyle medicine refers to the nonpharmacological/nonprocedural management of chronic disease and in principle represents the cornerstone of T2D management and portal for cultural adaptions to optimize care. 2
From 2020 to 2021, the COVID-19 pandemic signaled that affected patients with T2D were at greater risk for more severe clinical course. 3 However, preventive strategies to mitigate the adverse effects of pre-existing T2D were challenged by the increased number of patients with abnormal adiposity and insulin resistance, coupled with lack of successful and affordable weight reduction and healthy living strategies.4-6 Moreover, despite consistent evidence across different populations about the effectiveness of T2D preventive programs, many patients with prediabetes remain unaware of their condition and only a few of them adopt evidence-based interventions. 7
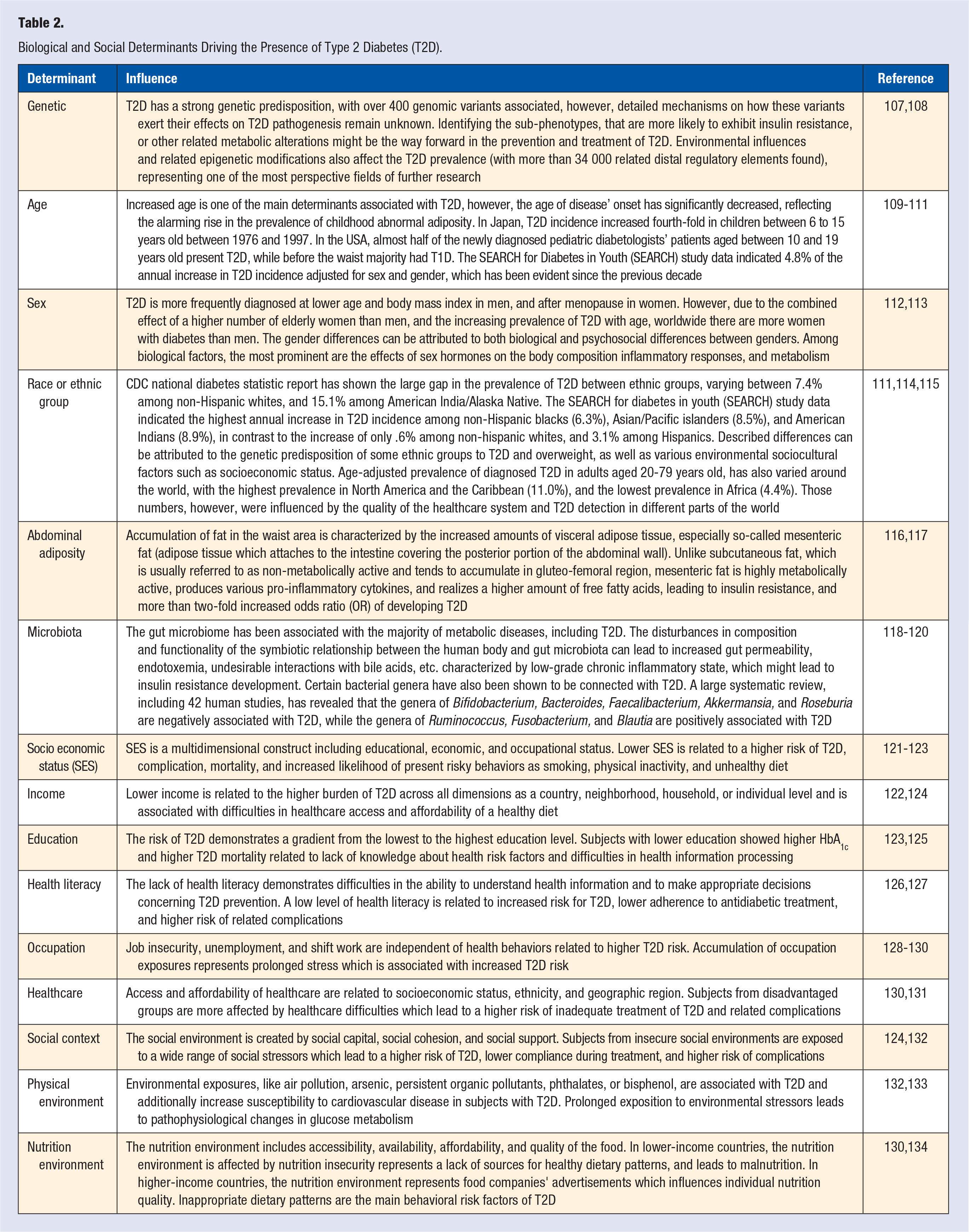
In 2019, the global prevalence of diabetes in adults between 20 to 79 years old was 9.3% (463.0 million), ranging from 4.0% in low-income countries to 9.5% and 10.4% in middle- and high-income countries, respectively (Table 1). 8 The age-comparative prevalence of diabetes varied substantially, from 4.7% in Sub-Saharan African countries to 12.2% in the Middle East and North Africa (MENA) region. 8 A summary of diverse biological and social determinants influencing this variability is presented in Table 2. Whereas culture plays a major role in the development of certain behaviors, risk factors, diseases, recommendations, and changes that should be established to prevent the progression of a chronic disease, acculturation is a process whereby specific cultures change, collide, and/or interact. 9 Specifically, when a person is exposed to a different culture, some aspects of the native culture may still be adopted while others are altered. Unfortunately, may ill-conceived acculturation strategies are related to a higher risk 10 and prevalence of T2D,11,12 worse cardiometabolic profile, 13 and higher microvascular complications. 14 Optimally, scientific evidence from a source culture can be applied to a target culture to improve preventive strategies; this process is termed “transculturation.” 15 Successful lifestyle medicine implementation in diverse cultures requires a transculturalization process. Transculturalization describes the process of adapting evidence-based clinical recommendations from a source culture to another culture using local thought leaders from both source and target cultures in an interactive setting. 16
World-Age Comparative Prevalence of Impaired Glucose Tolerance and Diabetes, Expenditures, and Number of Deaths in Adults.*.
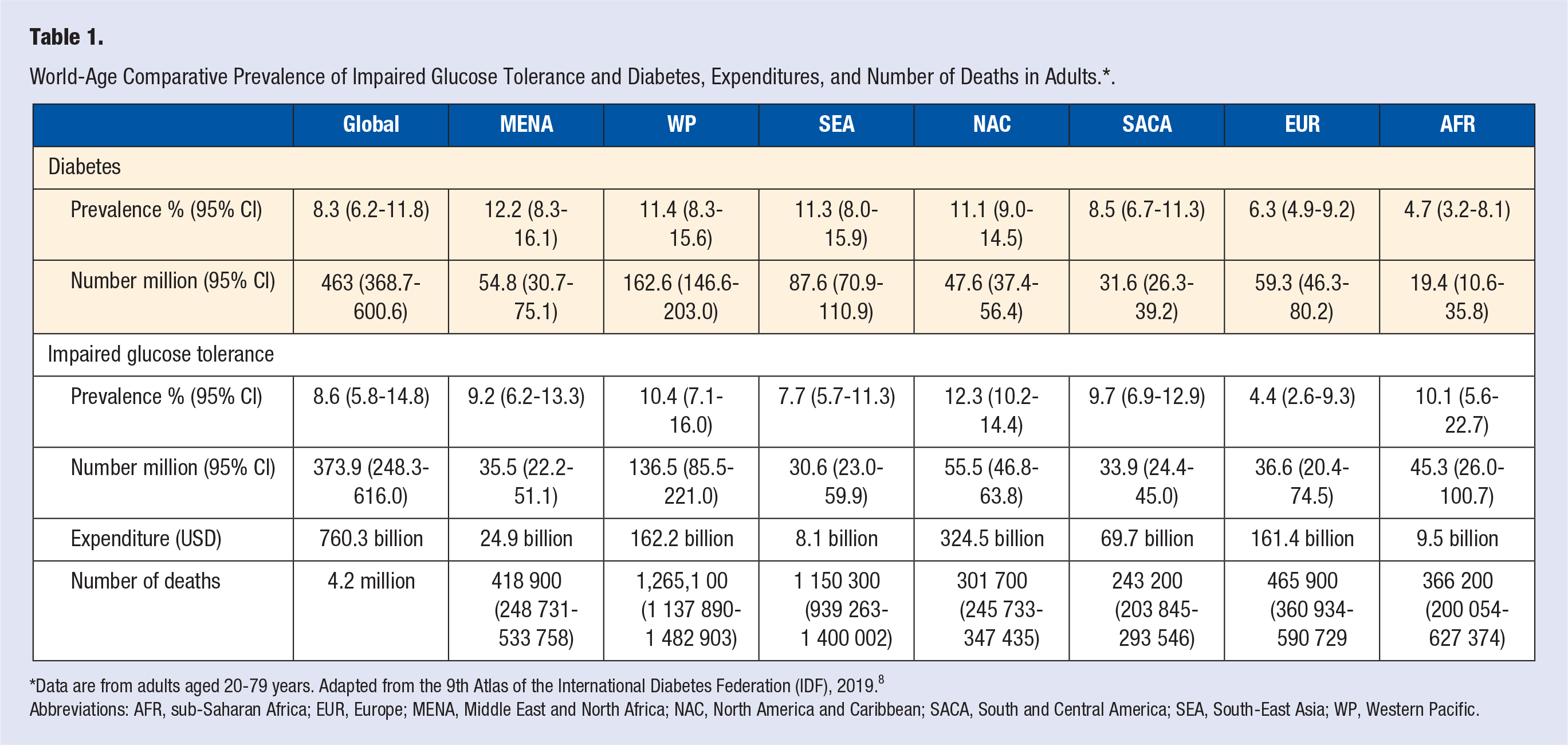
*Data are from adults aged 20-79 years. Adapted from the 9th Atlas of the International Diabetes Federation (IDF), 2019. 8
Abbreviations: AFR, sub-Saharan Africa; EUR, Europe; MENA, Middle East and North Africa; NAC, North America and Caribbean; SACA, South and Central America; SEA, South-East Asia; WP, Western Pacific.
Biological and Social Determinants Driving the Presence of Type 2 Diabetes (T2D).
Effective preventive care strategies need to codify and then systematically address the manifest biological, social, and cultural aspects of health. For this reason, the American Association of Clinical Endocrinology (AACE) proposed a new Dysglycemia-Based Chronic Disease (DBCD) model, consisting of 4 distinct stages along the insulin resistance–prediabetes–T2D–CVD spectrum, encouraging earlier intervention and a complication-centric, rather than a glucocentric approach. 17 Stage 1 DBCD “insulin resistance” reflects the early stage of risk to progress dysglycemia with molecular risk for islet-cell dysfunction under chronic stress of insulin resistance; Stage 2 DBCD “prediabetes” is diagnosed with detectable biochemical elevations in blood glucose and is associate with a high risk of T2D due to the combination of insulin resistance and islet-cell dysfunction and CVD events; Stage 3 DBCD “T2D” is associate with a sustained elevation of blood glucose and a high risk for CVD; Stage 4 DBCD “complications” is defined for the presence of micro and/or macrovascular disease. Specific prevention modalities (primordial, primary, secondary, and tertiary) are mapped to specific DBCD stages, with quaternary prevention (to reduce over-medicalization) applied to all stages through the use of lifestyle medicine. Based on a comprehensive literature review, this chapter will present the scientific basis for a culturally adapted lifestyle medicine approach to DBCD.
Methods
A comprehensive literature review in MEDLINE (PubMed), Web of Science, and Scopus databases, spanning 2000 to 2021 inclusive, was performed by two researchers (I.P. and A.P.) in July to August 2021 using the following keywords: “intervention” OR “lifestyle intervention*” “prevent*” OR “primary prevent*” OR “secondary prevent*” OR “tertiary prevent*” OR “quaternary prevent*”, and terms related to dysglycemia: “diabetes”, OR “prediabetes”, OR “blood glucose”, or “obes*” OR “overweight*” OR “health promotion.” For article searching in MEDLINE (PubMed), the following Medical Subject Headings (MeSH) terminology was used: (prevention) OR (primary prevention) OR (secondary prevention) OR (tertiary prevention) OR (quaternary prevention) OR (lifestyle) OR (lifestyle intervention) OR (risk reduction behavior) OR (obesity) OR (overweight) OR (prediabetes) OR (type 2 diabetes mellitus). Additionally, a hand search using references in identified articles was performed. The inclusion criteria were clinical trials performed on adults 18 years or older, and studies evaluating the implementation of locally adapted strategies as a basis for transculturalization. Exclusion criteria were observational studies (retrospective, cross-sectional, and prospective), case studies, studies that were not performed on humans, studies that included only children and adolescents, and clinical trials assessing the effectiveness of pharmacological treatment regimes. The results were organized as primordial, primary, secondary, and tertiary prevention, and then divided by location according to the International Diabetes Federation (IDF) regions.
Results
A total of 36 788 articles were retrieved from the databases, and 2458 duplicates were excluded. Among the 34 330 unique articles, 34 087 articles were excluded after reading their titles and/or abstracts. Thus, 243 articles were subjected to a full-text review: 57 articles were excluded based on study design; 41 articles excluded based on a focus on pharmacological treatments; and 88 articles that were not aligned with the purpose of the review. Therefore, 57 studies were included: 11 on primordial prevention, 18 on primary prevention, and 28 on secondary prevention.
Primordial Prevention
Primordial prevention of DBCD is population-based and focuses on reducing risks by addressing the pathophysiological events that can lead to insulin resistance and beta cell dysfunction. 18 The target is typically a general population exposed to behavioral or environmental risk factors yet consisting of many metabolically healthy people. 18 The majority of primordial prevention strategies consist of lifestyle medicine and health promotion activities that are educational and motivational. These activities emphasize healthy eating patterns19-21 and plenty of physical activity,22,23 delivered using individual or group face-to-face interactions,23,24,19,21,25 personal calls or messages,26,27 emails, 28 web-based applications, 22 social media and smartphones, 29 community-based activities,19,25 or public mass media 20 strategies (Table 3).
Primordial Prevention Strategies.
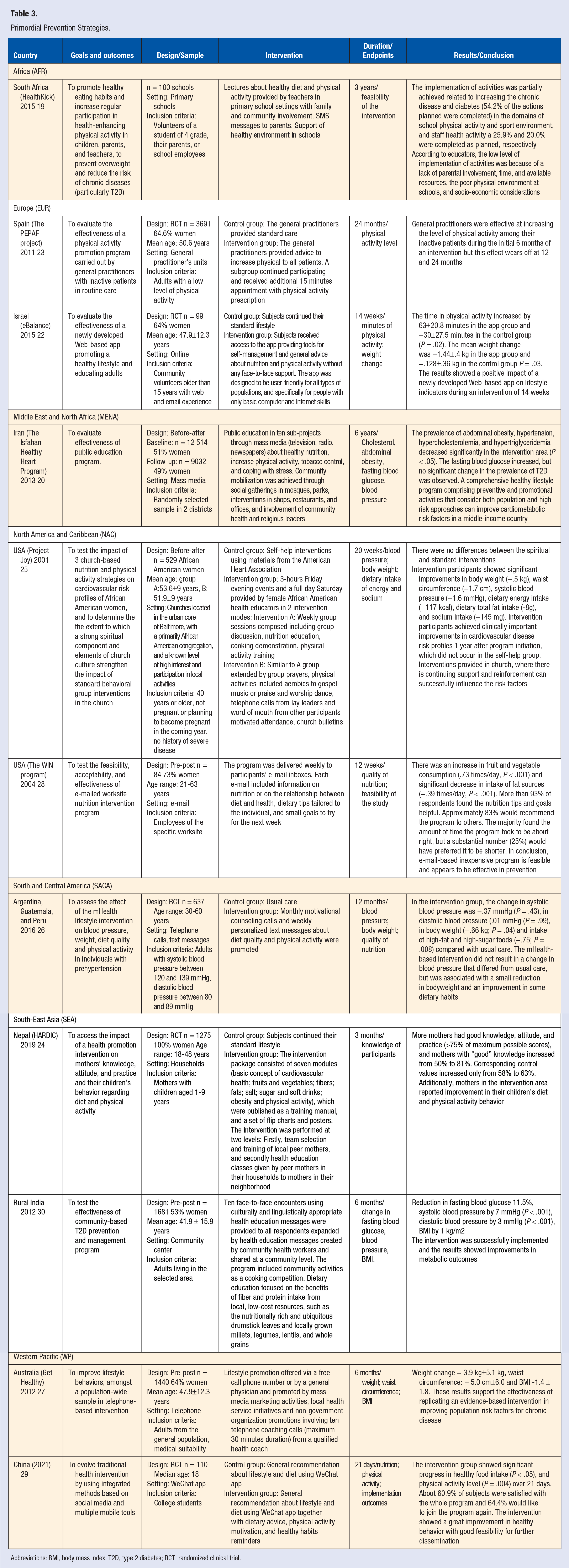
Abbreviations: BMI, body mass index; T2D, type 2 diabetes; RCT, randomized clinical trial.
Diverse cultural components of primordial prevention have been described. For example, in a study of African American women living in the U.S., 25 interventions were implemented in a church, respecting subjects’ religion, and included group prayers and aerobics activities with gospel music or praise-and-worship dance. 25 The important role of religion was also observed in a study from Iran, 20 where the intervention was delivered through mass media but complemented with social gatherings in mosques, parks, shops, restaurants, and offices, with involvement of community health and religious leaders. 20 Other studies24,25,30 described the important role of community involvement and community member healthcare professionals. One study from Africa 19 focused on health promotion in the earlier stages of life with the intervention delivered in schools and including children’ families and teachers. Another study of Nepal 24 targeted mothers of small children, and the intervention was provided in household visits by other trained mothers.
The primary outcomes of primordial prevention strategies for DBCD were behavioural components surrounding food intake (e.g., fruits and vegetables, 28 salt, 25 fat,26,28 and total energy 25 ), levels of physical activity,22,23,29 biological components (e.g., body mass index [BMI], weight,25-27 waist circumference,20,27 fasting blood glucose,20,21 blood lipids, 20 and blood pressure21,25,26), and feasibility of the intervention. 19 In general, most of the interventions were able to improve behavioral risk factors, and cardiometabolic biomarkers with diverse strategies of interventions.
Primary Prevention
Primary prevention in DBCD is applied to patients with predisease in whom insulin resistance has led to β-cell defects and mild hyperglycemia, in order to avoid or delay the progression to sustained, more advanced hyperglycemia and bona fide T2D. 18 The primary prevention educational strategies were usually delivered using contents and tools provided to the patients printed31-37 or virtual,30,38 and implemented using wearable technologies and other devices33,39,40 (Table 4). Active participation was also encouraged as part of diabetes prevention programs, including healthy food preparation21,30,40,41 or physical activity sessions in a group37,40,42 or individually. 33 Notably, the U.S. Diabetes Prevention Program (DPP) was a commonly used framework35,39,42-44 and included a web-based information platform, 40 videos, 40 motivational SMS messages or telephone calls, 36 and asynchronous strategies with pre-recorded video lectures.38,40
Primary Prevention Strategies.

Abbreviations: BMI, body mss index; HDL, high density lipoprotein cholesterol; HR, hazart ratio; IFG, impaired fasting glucose; RCT, randomized clinical trial; RR, relative risk; T2D, type 2 diabetes; OGTT, oral glucose tolerance test.
Various populations routinely included specific cultural characteristics in primary prevention programs.35,45 For example, in Latino women in U.S., 39 the DPP was delivered by community health workers in the target population, referred to as promotoras and promotores. In Africa, 44 DPP content was simplified and contextualized using local examples and visual elements taken by a local photographer in the community. 44 In Saudi Arabia, 35 visual material of the content reflected the Arab culture and environment, using Islamic metaphors, and incorporating local recommendations about routines (For example, increase walking to mosque for prayer, and adjust recipes based on religious and traditional habits of Ramadan). 35 The importance of religion with health was also described in a study from Iran, 21 where the intervention included participation in religious ceremonies and sessions in mosques, particularly during Ramadan. 21
Most of the primary prevention activities were delivered face-to-face in groups21,31,33,35-38,40-42,44,46-50 or individually.41,51,52 In general, interventions were delivered by healthcare professionals in the Western Pacific region,49,50 Europe,31-33,41,52 and South America.36,42 However, in Africa, 44 Middle-East Asia,21,35 and South-East Asia37,43 regions, the interventions were delivered by members of the community. It is important to note that some studies from the U.S.38-40 reported a hybrid approach of healthcare professionals and community members.
The primary outcomes of primary prevention strategies included the assessment of T2D incidence,34,41,43,49,53 the change of biological components, weight and BMI,36,38,50,51 blood pressure,21,30,49 dyslipidemia,20,37,50,51 dysglycaemia,36,38,41,50 and the evaluation of the implementation process.31,44 In general, most of the studies proved to be implementable, improved the presence of biomarkers, and/or reduced the incidence of T2D.
Secondary Prevention
Secondary prevention in DBCD is applied to patients with early, asymptomatic T2D, to prevent the development of symptoms and/or micro-/macro-vascular complications. 18 In addition to pharmacotherapy, lifestyle interventions are core recommendations in patients with T2D and consist of dietary recommendations and physical activity based on local guidelines. 54 In those patients with abnormal adiposity, dietary recommendations often included caloric restrictions (450 kcal/day, 55 825-853 kcal/day, 56 or 1200-1500 kcal/day 57 ) to promote weight loss and a healthy body composition (Table 5). Studies from the U.S.,58-61 Malaysia, 62 and China 63 also incorporated commercial, diabetes-specific nutritional formulas as meal/snack replacements. Physical activity recommendations emphasized performing at least 150 min of moderate-intensity physical activity per week, with some of the interventions also included group-based exercise classes 54 and training sessions on cycloergometer 55 as a part of structured programs. Behavioral interventions included motivational interviewing57,62 to increase self-efficacy, and regularly provided equipment including such as scales for body weight, 64 accelerometers, 64 and educative materials.65,66 A study in Germany 64 included cost liability of 150 Euros for increasing participants’ adherence. The interventions varied in duration, from 3 months 67 to up to 6 years, 68 frequency, and methods of delivery of the educational sessions. Some studies employed specific applications or websites, through which participants reported health-related parameters to the staff.64,69-71 Telemedicine tools included video-conference calls, 69 phone calls,67,72,73 and texts. 70
Secondary Prevention.

Abbreviations: BMI, body mass index; A1c, glycosylated hemoglobin; RCT, randomized clinical trial; T2D, type 2 diabetes.
Various studies have included specific cultural components to facilitate the acceptance and delivery of the study. For example, in faithful communities of Barbados, 74 intervention has been delivered by trusted community health advocates, without medical background. In Malaysia, 62 Thailand, 66 Latin America, 65 and Norway, 54 particular attention has been paid on transcultural adaptation of the educational materials, especially parts related to diet (meal plans, photographs of local foodstuff), and physical activity to fit the cultural patterns of participants. Studies in the U.S.60,75 highlighted the impact of adapting educational content not directly sourced from within various socioeconomic and ethnocultural groups. Studies from South and Central America 65 and North America and Caribbean47,57,58,60,74-77 regions were more likely to deliver the intervention in form of group sessions, emphasizing the importance of peer education, communication, sense of competition, and support. Studies from Europe55,56,64,69,71 and high-income countries in South-East Asia70,78,79 and Western Pacific 73 regions often focused on the implementation of telemedicine tools, as well as delivering interventions in the form of one-to-one sessions, adapted to the needs of a specific subject. Interventions were regularly implemented in traditional medical settings and delivered by healthcare professionals; however, some interventions in the U.S. 75 and Barbados 74 were implemented in churches and faith-based organizations and delivered by trained coaches without a healthcare background.
The primary outcomes of secondary prevention strategies included the assessment of biological outcomes, such as improvement of Hemoglobin A1C (HbA1c),57-59,63-67,69-71,80-87 fasting blood glucose,63-65,70,72,73 BMI,54,57-59,64,65,67,72,82-84,87-89 waist and hip circumferences,63,84 serum lipids,65,70,80,82,83,87 body composition,55,59 and other clinical parameters, as improvement of the quality of life,59,66,87 treatment cost,64,65 decreased incidence of micro- and macrovascular complications, 78 and created T2D remission. 56 In general, lifestyle interventions improved weight, HbA1C levels, quality of life, traditional cardiometabolic biomarkers, and antidiabetic medication use. Substantial weight reduction was associated with T2D remission.
Tertiary Prevention
Tertiary prevention in DBCD is applied to patients already with symptoms and/or afflicted by diabetes complications with the intent to improve quality of life and longevity. Although tertiary prevention accounts for most patient encounters in the modern healthcare system, it is usually related to pharmacological/procedural treatments rather than lifestyle medicine. 18 In this search, there were no results about lifestyle medicine and transculturalization with tertiary prevention in DBCD.
Discussion
Lifestyle medicine is the foundation of preventive care programs to avoid the appearance, progression, and complications related to DBCD. Specific ethnocultural attributes apply to an individual and influence their lifestyle, and by extension, their risk for cardiometabolic disease and the adoption of medical recommendations. Transcultural lifestyle medicine delivers pragmatic lifestyle recommendations, particularly focused on the adoption of healthy eating patterns, regular/sufficient physical activity, sleep hygiene, stress reduction, community engagement, and alcohol, tobacco, and substance cessation. 90 In this review, lifestyle medicine in different stages of DBCD was presented, with specific attention to the strategies implemented and the cultural aspects incorporated. However, most of the studies lacked a description of which were the local components of their intervention. For example, there were common descriptions that dietary recommendations were adapted to local guidelines or available foods, without specification of how this process of adaptation was implemented or how differed from the original recommendations. Most of the cultural aspects described were “immerse” in the intervention.
There is a need for a clear description of the transculturalization process incorporated in the interventions and adaptations of diverse populations. 15 An example of transculturalizing evidence-based recommendations is the Transcultural Diabetes Nutrition Algorithm (tDNA). 16 The tDNA was developed as a tool to facilitate the delivery of lifestyle modifications and nutrition therapy to subjects with prediabetes and T2D in a variety of geographic locations and cultural settings.16,91-97 The tDNA transcultural adaptation process incorporates five steps: (1) Identification of the target population, describing the population where the implementation is going to be delivered; (2) Identification of the clinical question: description of the gap to address; (3) Identification of the appropriate source evidence base: analysis of the scientific evidence addressing the problem; (4) Identification of experts in the source and target populations: experts in the scientific evidence from both the source and target population directly engage to address the cultural differences and adaptations; (5) Synthesis of the transcultural recommendations and algorithm. 98
Primordial, population-based preventive strategies should be implemented to decrease environmental and behavioral risk factors that lead to unhealthy lifestyles, abnormal adiposity, and insulin resistance. 99 Though addressing environmental factors is mainly the concern of government, strategies to change the built (human-made) environment, as well as patient behaviors, can be influenced by healthcare professionals. Unfortunately, abnormal adiposity and many behavioral risk factors are perceived to be under a patient’s control, creating a false association among obesity, “laziness,” and lack of willpower, perpetuating the stigma related to obesity. 99 For this reason, the AACE proposed another framework, referred to as Adiposity-Based Chronic Disease (ABCD) as an effort to address research gaps in abnormal adiposity distribution and function, obesity stigma, and resultant clinical inertia. 100 Insulin resistance may be viewed as the intersection between ABCD and DBCD, which are also associated with inflammation, hypertension, dyslipidemia, residual risks, and CVD, together interpreted as Cardiometabolic-Based Chronic Disease (CMBCD).18,101 The studies found in this review show that lifestyle interventions at early stages could diminish chronic disease burden at later stages on individual, community, and population scales. These interventions have a different delivery modality, from face-to-face to telephone, apps, to massive media campaigns. As a next step, evidence evaluating public health policies and infrastructural changes is needed.
In primary prevention of DBCD, programmatic implementation demonstrates that lifestyle intervention is effective in delaying or reducing the incidence of T2D by around two-thirds compared to standard care. 51 However, subsequent culturally adapted programs in diverse populations show that the effectiveness in daily clinical practice is lower than the original interventions, reflecting the challenges in transculturalization. 102 Most of the T2D preventive programs are based on frameworks of behavioral change that include goal-setting, self-monitoring, stimulus control, motivational interviewing, problem-solving, self-empowering, forming action plans, etc. Furthermore, the delivery of the programs includes synchronous and asynchronous strategies, with content varying substantially according to the region and ethnocultural background. These programs incorporate an aspect of each cultural group, including religion, language, metaphors, and foods available to the programs’ specific content. Despite the overwhelming evidence on the effectiveness of preventive programs to reduce the burden of T2D and the large effort of the transcultural adaptation to different populations, one of the main problems in primary prevention of T2D is the high unawareness of prediabetes, for example, in populations like the U.S. and the Czech Republic, the prevalence of unawareness of prediabetes was 84.7% 103 and 82.4%, 104 respectively. To emphasize the severity of this problem in the U.S., only 4.2% of subjects with prediabetes are referred to prevention programs and only 2.4% participated. 7
In secondary prevention of DBCD, the improvement of lifestyle of subjects with T2D impacts positively on their quality of life, weight, HbA1C, and other cardiometabolic risk factors, but the benefits on cardiovascular events are limited. The Look AHEAD study is one of the largest and longest follow-up evaluations of patients with T2D and obesity that demonstrated, despite a greater weight loss in the intervention group versus the standard care group (8.6% vs .7% at 1 year; 6.0% vs 3.5% at study end, respectively) and 9.6 years of follow up, there was no reduction in cardiovascular events. 58 However, the Japan Diabetes Complications Study demonstrated a 38% reduction of stroke events after 8 years of follow-up for 2033 Japanese subjects with T2D treated with lifestyle medicine versus standard care. 78 Recent studies in subjects with T2D and abnormal adiposity proved that intensive lifestyle interventions aiming at large weight reductions were associated with T2D remission in primary health care centers in the UK, 105 Qatar, 89 and Barbados. 106 However, the main problem at this stage is that the healthcare system is often focused solely on the pharmacological treatment of hyperglycemia, disregarding the benefits of lifestyle medicine by not implementing them on a sufficient scale.
During tertiary prevention, the majority of preventive care for a healthcare system is implemented, because it is the burden of symptoms and disabilities that brings the patient in for evaluation, and unfortunately, there are significant research, knowledge, and practice gaps, as well as funding and reimbursement, for earlier modalities of prevention. A lack of evidence on the implementation of lifestyle medicine at this stage was observed in the analysis of the literature. Because this stage is characterized by pharmacotherapy and procedures, quaternary prevention becomes paramount and should be applied not just at later, but at all DBCD stages
Conclusion
This review summarizes the efforts of implementing transcultural lifestyle medicine across the DBCD spectrum in diverse populations. The results show several strategies to implement lifestyle medicine, from public educative campaigns to individual face-to-face approaches, and the use of technological resources from texts to apps. Primordial prevention targets individual and population DBCD risks, but more information about effective long-term effects and broad reach from cultural adaptation are needed. Primary prevention targets the reduction in T2D incidence with the implementation of diverse transculturalization strategies, but mechanisms to scale up these programs in diverse environments are needed. Secondary prevention targets improved quality of life and halting the progression of early T2D before complications and symptoms arise; many transculturalized biomarkers can be monitored to reflect a beneficial impact on incident cardiovascular events. There was no evidence directly related to culturally adapted lifestyle medicine in tertiary prevention of DBCD highlighting a glaring research gap.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.