
Abstract
Over 80% of chronic disease is caused by lifestyle practices, including an unhealthy diet. Despite this, most medical students in the United States graduate having received minimal nutrition education, guidance towards improving their nutrition, or skills needed to coach patients to adopt a healthier diet. This study aimed to educate fourth-year medical students in evidence-based knowledge regarding a delicious, whole-food plant-based diet while introducing practical culinary skills and patient coaching skills. We adapted an open-source culinary medicine curriculum designed for in-person teaching of pre-clinical medical students to provide a novel 1-month online elective to fourth-year medical students. We used a 26-item pre/post questionnaire to assess change in evidence-based knowledge regarding nutrition, culinary skills, patient coaching skills, and attitudes toward a whole-food plant-based diet. In addition, we reviewed narrative comments by the student participants, course directors, and medical-school administrators. Scores in all 4 domains were tested, and for all individual questions, they showed statistically significant improvement following the course. Most narrative responses were positive, and areas for improvement were also identified. We successfully adapted an open-source whole-food plant-based culinary medicine curriculum for advanced medical students into a 1-month elective taught on a virtual platform. This course filled a need for training in nutrition and counseling for these students as they start their professional careers.
An open-source whole-food plant-based culinary medicine curriculum adapted into an elective demonstrated improvement in nutrition knowledge, coaching confidence, culinary skills, and desired attitudes and behaviors.
Introduction
Unhealthy lifestyles underlie 80% of chronic illness. 1 Physicians’ nutritional behaviors may strongly affect how their patients nourish themselves 2 . Despite this, most medical students graduate with minimal nutrition education to protect their own health, prevent chronic disease, or the skills needed to coach their patients to adopt a better diet.3,4 Indeed, physicians often have unhealthy lifestyles, leading to a high prevalence of chronic medical and mental illness.5,6 An additional barrier to adopting a better diet is a common misperception that healthy food is not enjoyable. 7 Healthcare professionals, at all levels of training from pre-medical to postgraduate, are now recognizing this critical gap in their education and requesting or demanding nutritional education, and even designing their own programs.5,8
Culinary medicine is a “simulation-based medical education with deliberate practice” (SBMP-DP) approach to teaching nutrition skills that can take many forms. 9 It has been shown to be more effective than traditional methods in teaching healthy nutrition to medical students.4,10 Nutrition is minimally taught in the medical school core curriculum at the Keck School of Medicine (KSOM); however, students can participate in nutrition education electives. An opportunity to introduce a culinary medicine elective into the KSOM curriculum arose in early 2020 due to 2 key factors. Firstly, the COVID-19 pandemic created a sudden need for interactive virtual learning programs for medical students.11,12 Secondly, in December 2019, the American College of Lifestyle Medicine (ACLM) made available a comprehensive, open-source culinary medicine curriculum (CMC) to health professionals at no cost. The initiative aimed to support CM implementation at academic institutions worldwide. 13 The hunger for such a curriculum was evidenced by the fact that in the first 2 months after it was made available, it was downloaded over 2000 times in 83 countries, with 58% of viewers being physicians. 13 This curriculum was developed by Michelle Hauser, MD and Chef, and colleagues at Stanford University over several years and used in in-person teaching of pre-clinical students.13-15 The CMC was designed to expose the students to the fundamentals of cooking interactively in a kitchen as a tool to learn more about nutrition, improve the personal health of enrolled students, and teach more effective patient counseling techniques towards healthier nutrition. It expressly aims to provide experiential training in fundamental culinary skills that allow students to master preparing an appetizing whole-food plant-based diet.
This paper describes how we expanded the newly released ACLM CMC into a novel 1-month virtual elective program. We discuss our findings from three 1-month teaching courses provided to 24 fourth-year medical students.
Methods
Administrative Approval
Shortly after the COVID-19 pandemic required KSOM medical students to receive instruction remotely, the course directors proposed an online culinary medicine course to the KSOM Medicine Education Curriculum Committee. The proposal was approved as a 40-hour/week elective of either 2 or 4 weeks’ duration for fourth-year students. We also sought and obtained approval from the CMC lead author, Dr Hauser, and the CMC distributor, the ACLM, to use the CMC in this program.
The Teaching Team
The course was designed and led by 3 physicians, each with a passion for delicious and healthy nutrition. One had prior experience teaching culinary medicine as a member of the Teaching Kitchen Collaborative, 16 2 are diplomats of the American Board of Lifestyle Medicine, and, in addition, one is a trained chef. The course was structured to fit into the directors' existing schedules, with each participating in 3 three-hour live cooking sessions/week. Administrative support was provided by a pre-medical student and staff from the KSOM Department of Medical Education, with IT support available when needed. Many highly qualified medical professionals from within and outside the university participated in the program as guest lecturers or invited guests during the culinary skills sessions.
Students
A 2-week course was piloted with five third-year students. Subsequently, all participants were fourth-year students. Students were required to have access to a quiet kitchen for the online culinary skills sessions and basic kitchen equipment. They were also required to buy all ingredients for the recipes and the course textbook (Beth Frates’ “Lifestyle Medicine Handbook”). 17 To allow for personal attention to each student, each course was limited to 8 students. Students with all levels of nutrition and cooking experience were encouraged to enroll.
Overview of Course
We defined 4 main learning objectives for the course: to deliver evidence-based knowledge regarding the role of nutrition and health, to teach practical culinary skills, to enable students to apply this learning to personal cooking, and to coach patients toward healthy nutrition utilizing motivational interviewing techniques. An overview of a typical weekly schedule is shown in Table 1. We included one live session/day and scheduled time for students to work on their weekly assignments. Weekly assignments were based on the week’s learning. We utilized a “flipped classroom” model, with students watching videos and reading materials before the online teaching sessions and teaching their peers.
Overview of Weekly Schedule Culinary Medicine Curriculum.
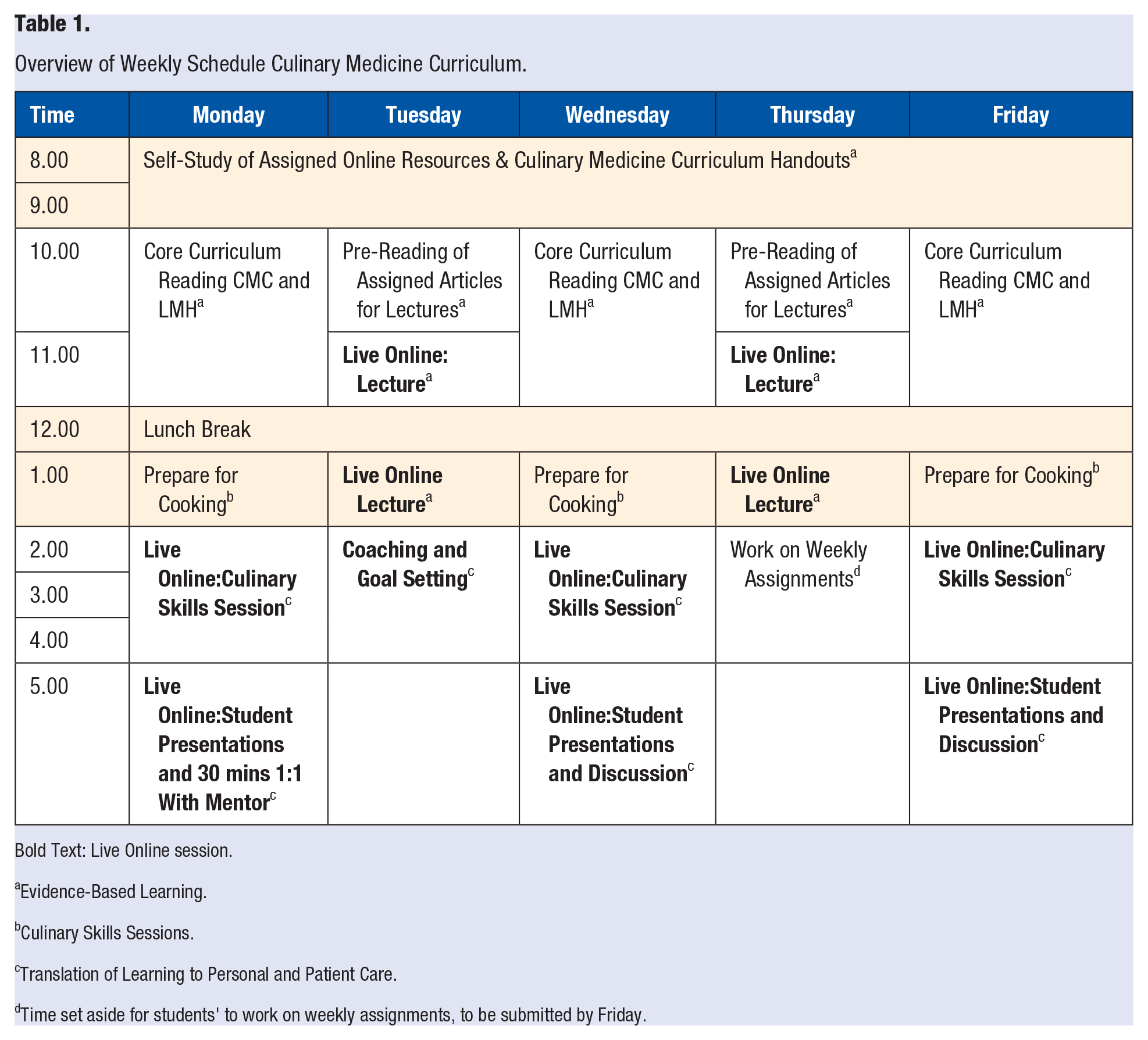
Bold Text: Live Online session.
Evidence-Based Learning.
Culinary Skills Sessions.
Translation of Learning to Personal and Patient Care.
Time set aside for students' to work on weekly assignments, to be submitted by Friday.
Technical Aspects
Live sessions were conducted through the professional ZOOM service through an institutional license to the KSOM. 18 Students and directors placed their smartphone and/or computer camera to display their kitchen workspace during the culinary skills sessions. Course materials were posted on a common password-protected Google Drive file. In addition, each student had a personal Google Drive folder where they could submit their assignments for review by the course directors.
Culinary Skills
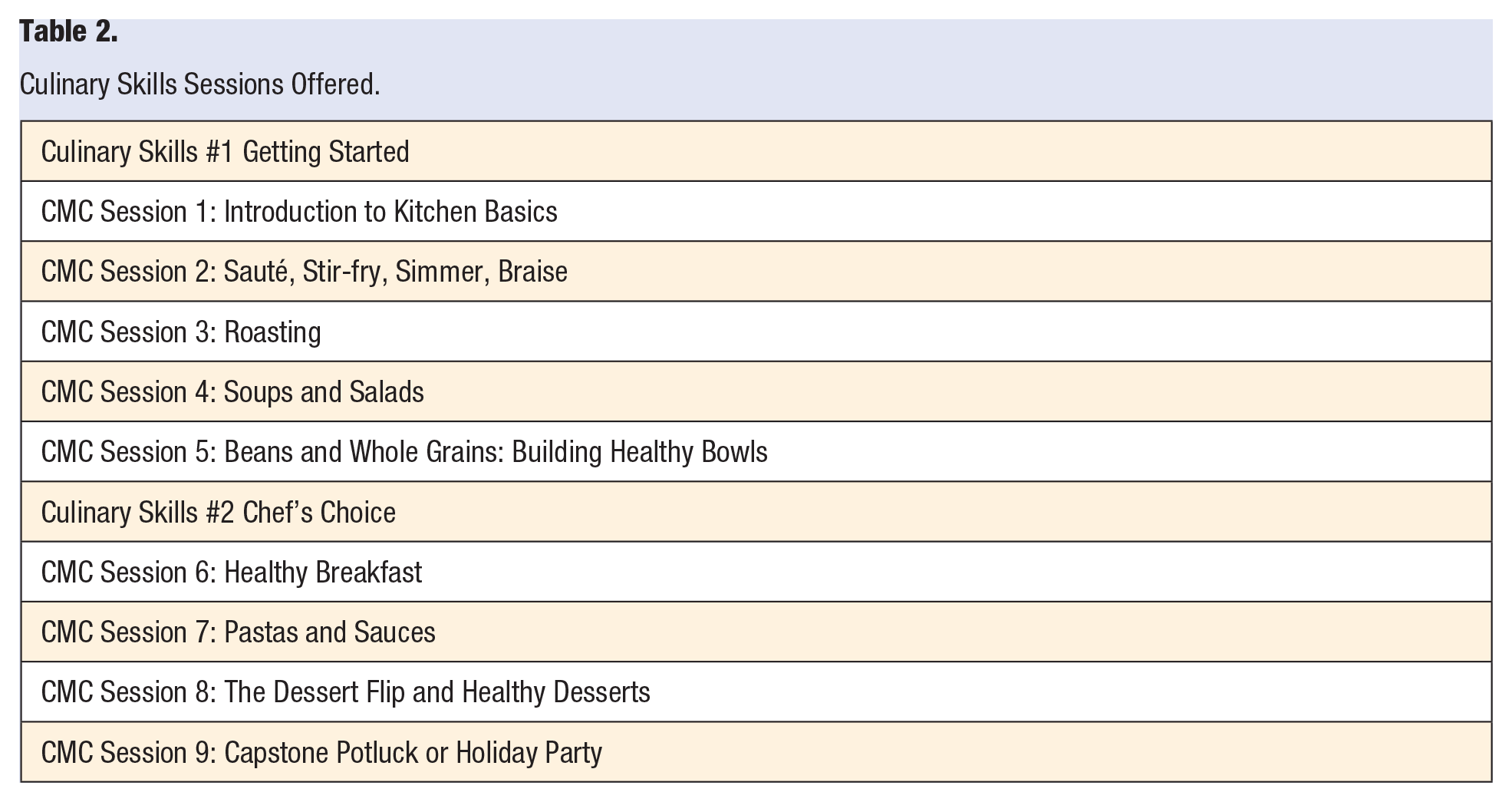
The foundation of the program was the 9 culinary medicine sessions in the CMC 14 (see Table 2). These comprehensive sessions provide detailed information on preparing for and conducting each session. Background reading and recipes are included. Each session focuses on a different culinary technique, and a wide variety of plant-based whole foods is used. The virtual sessions were predominantly hands-on and interactive. The course directors monitored the student’s techniques and provided suggestions in real-time. The course chef, who cooked with the students most often, used 2 cameras and felt successful in demonstrating techniques to the students virtually. In addition to the 9 sessions in the CMC, the course chef provided 2 additional sessions to teach further culinary skills using whole-food plant-based recipes of his choice. Rather than the final session being a group potluck (as described in the original curriculum where each student contributes a unique dish), the course directors and students all prepared similar seasonal party recipes in their kitchens.
Culinary Skills Sessions Offered.
Initially, we were apprehensive about teaching culinary skills virtually, thinking that hands-on instruction was irreplicable. In our virtual class, we were unable to critique and correct culinary techniques as well as we could in person. Additionally, we missed out on sharing olfactory, tactile, and tasting skills. However, the upside of virtual classes was that the students could gain culinary skills in the comfort of their kitchens and take ownership of their newfound abilities. The students would frequently comment on how they repurposed leftovers and felt comfortably creative in their personal kitchens. In the future, we will most likely utilize both in-person and virtual classes to reap the benefits of both modalities.
Evidence-Based Learning
Reading, online videos, and lectures enabled students to learn some of the science behind culinary medicine. Students were assigned to read the Introduction to the Culinary Medicine Curriculum, 14 and five chapters from Beth Frates’ “Lifestyle Medicine Handbook” (viz, Understanding Lifestyle Medicine, Empowering People to Change, Collaborating, Motivating, Goal Setting and Tracking, and The Nutrition-Health Connection). 17 Experts from within and outside KSOM presented one-hour lectures with discussions. Relevant journal articles were assigned to be read before the lecture. Lecture topics included an overview of lifestyle medicine, an introduction to culinary medicine, separate lectures on nutrition as it relates to diabetes, cardiology, and Alzheimer’s Disease, the “Blue Zones,” motivational interviewing, health coaching, batch cooking, working with an outpatient dietitian, food sustainability and insecurity, and the consequences of high intake of refined sugar. Finally, students were encouraged to research and discuss relevant topics of personal or professional interest.
Translation of Learning to Personal Care and Effective Patient Coaching
Reading, lectures, and individual mentoring provided the background to this component of the course. In addition, experienced dieticians discussed strategies for coaching patients in dietary change. Each student received personal mentoring every week from one of the course directors and was first asked to review their own diet and set a “SMART” goal for change. Each student mirrored the mentoring session by practicing their skills by coaching a family member or friend in a weekly session. Finally, role-play coaching sessions were included in the discussion period that followed the culinary skills sessions.
Assignments
Each student was assigned to lead one of the culinary skills sessions with the assistance of the course directors. Students previewed the session’s description in the CMC, described the purpose of the session to their classmates, and presented a 15-minute slideshow on a relevant topic of their choice. We allowed some student creativity in this regard. Students added information regarding their cultural heritage to their presentations and discussed their relationships with that particular food topic.
Assigned work was also submitted each week for review by the director mentor and feedback discussion with the student the following week. Assignments were designed to reinforce learning in the 3 main areas of the course and stimulate individual exploration of culinary medicine. Core curriculum reading was assessed by preparing a lecture to present to peers or patients and answering questions at the end of each textbook chapter. Students submitted weekly coaching reflections and photos of their “mise-en-place” and plated food for each culinary skills session. Finally, students submitted one-minute videos of different knife skills and the preparation of one complete recipe. A collection of student-curated recipes with photos from the course was provided to each student on completion.
Student Performance Assessment
The student-mentor graded weekly projects, and performance was assessed for effort, proficiency, and behavior. The mentor evaluated the individual students and summarized the overall performance at the end of the elective student evaluation form. The pass/fail course was graded based on attendance, class participation, and submission of weekly projects.
Student Assessment and Course Evaluations
A 26-item self-made questionnaire covering 4 areas (nutrition knowledge, culinary skills, coaching confidence, and attitudes and behaviors toward a whole-food plant-based approach to nutrition) was completed by each student by the first day of the course. The same questionnaire was completed on the last day of each section. Two-tailed paired t-tests were used to compare pre- and post-scores for categories of questions and individual questions. In addition, students completed qualitative confidential course assessments as is standard practice at KSOM.
Ethical Considerations
Publication of findings from this course was deemed exempt from IRB review by the USC Social Behavioral IRB. The KSOM Medical Education Curriculum Committee approved the elective, and the Assistant Dean for Research and Scholarship at KSOM supported this submission. Still, they did not provide financial or other resources to run it other than technical support, which may dissuade future students from participating. Each student was reimbursed $40 for food they bought through “A Taste of Lifestyle Medicine” microgrants awarded by the American College of Lifestyle Medicine to the course directors. None of the course directors had any conflict of interest related to this work.
Results
Enrollment
Twenty-four students enrolled for the 3 elective offerings, the target enrollment. Of the 24 students, 20 enrolled for 4 weeks and 4 for 2 weeks. The objective of the course offerings remained the same, and results were not significantly different across (1) individuals that completed the full vs reduced course or (2) individuals in each of the 3 iterations of the course. There was a waitlist for all 3 elective offerings. By gender, there were 14 female and 10 male students. The students have since been accepted into the following postgraduate residency courses (23 of 24 students): Internal Medicine: 7; Pediatrics: 3; Medicine-Pediatrics: 1; Family Medicine: 3; Psychiatry: 2; Emergency Medicine: 3; Anesthesiology: 2; Dermatology: 1; and Diagnostic Radiology: 1.
Quantitative Analysis of Learning Objectives
After inputting data from our four-point scale questionnaire into Microsoft Excel, it became evident there was a statistically significant increase in the average pre- to post-test scores for the 26 questions, consistent with increased knowledge, coaching confidence, culinary skills, and desired attitudes and behaviors. The average total (SD) pre-test raw score was 73.1 (11.1) out of a maximum of 104, and the average post-test score was 100 (3.7), that is, a change from pre to post of 70.3% to 96.2% (P < .0001). Scores were higher for each of the 26 questions on the post-test compared with the pre-test. The average (SD) score for each question pre-test was 2.8 (.62) and post-test 3.8 (.2). (P < .0001).
Figure 1 shows a comparison between the pre- and post-responses by categories of question. For questions testing knowledge, the pre-test average was 2.3 (out of 4), and the post-test average was 4 (out of 4), for a change from 57.5% to 100%. As for student coaching confidence levels, the pre-test average was 2.4 and the post-test average was 3.8, increasing from 60% to 95%. At the start of the course, the students reported a 2.4 (70%) average for culinary skills and ended the course with a 3.9 (97.5%). Lastly, as for attitudes and behaviors, the pre-test average was 3.4 and the post-test average was 3.8, for a change from 85% to 95%. Figures 2–5 indicate the change in score for each question. Some questions had a low average pre-test score with an opportunity for a significant increase, while others had a high average pre-test score with little room for improvement.
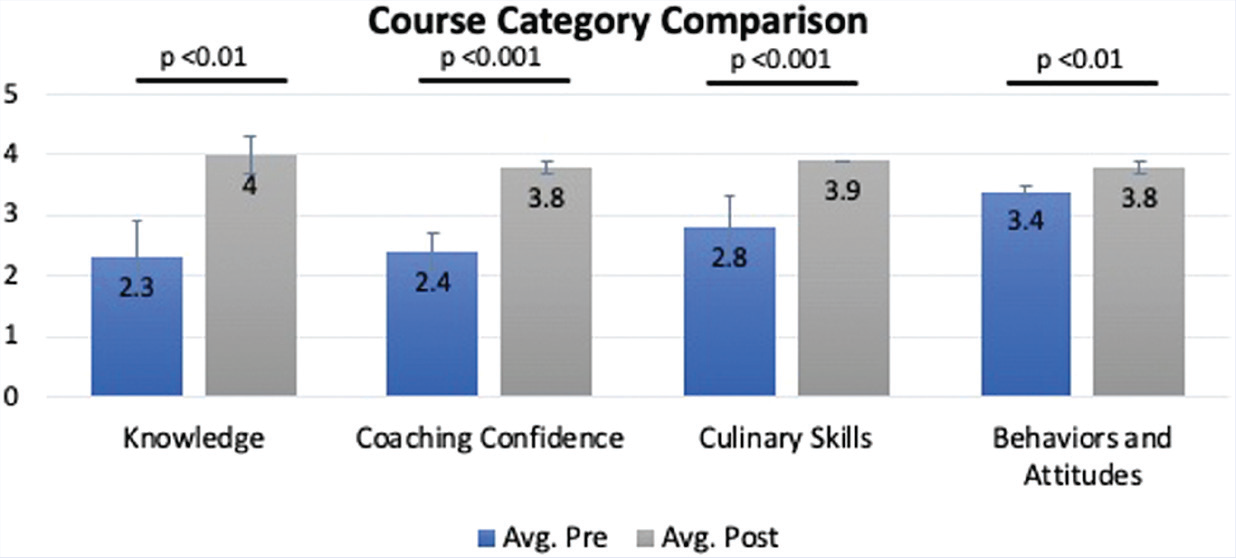
Comparison of pre- and post-test score by category of question (n = 24 students).
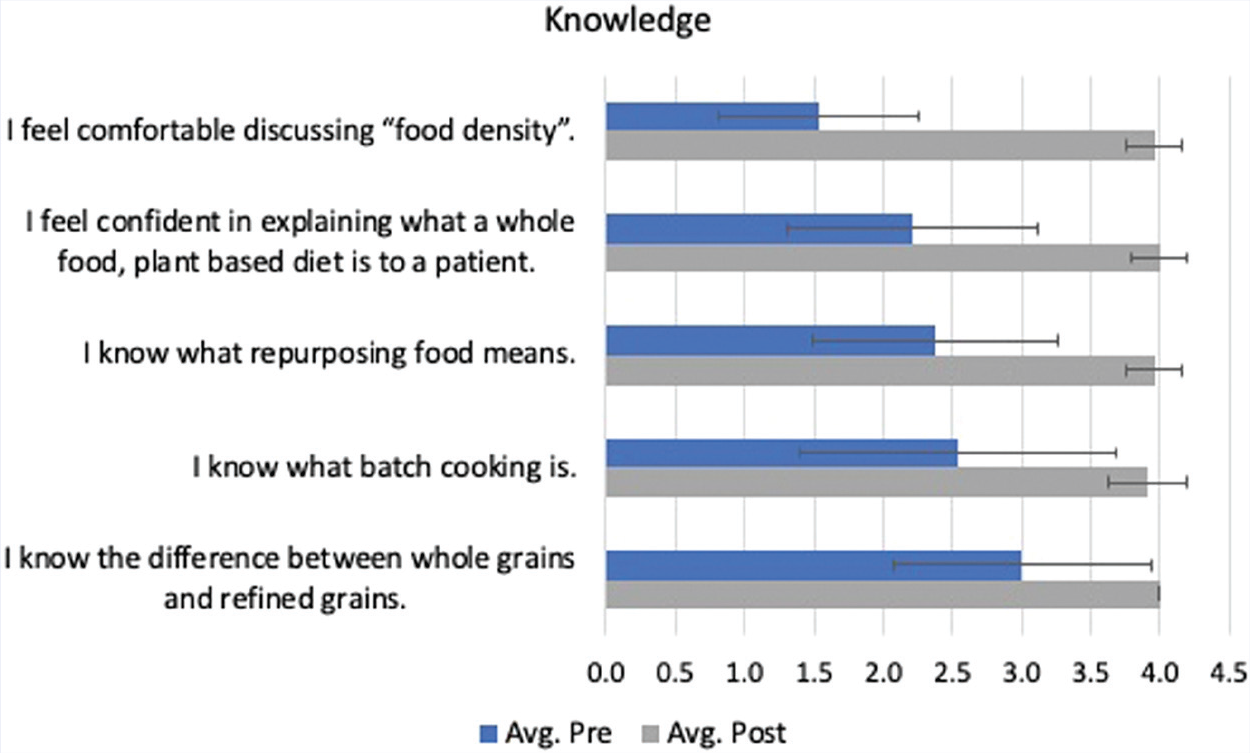
Culinary knowledge pre- and post-test scores (n = 24).
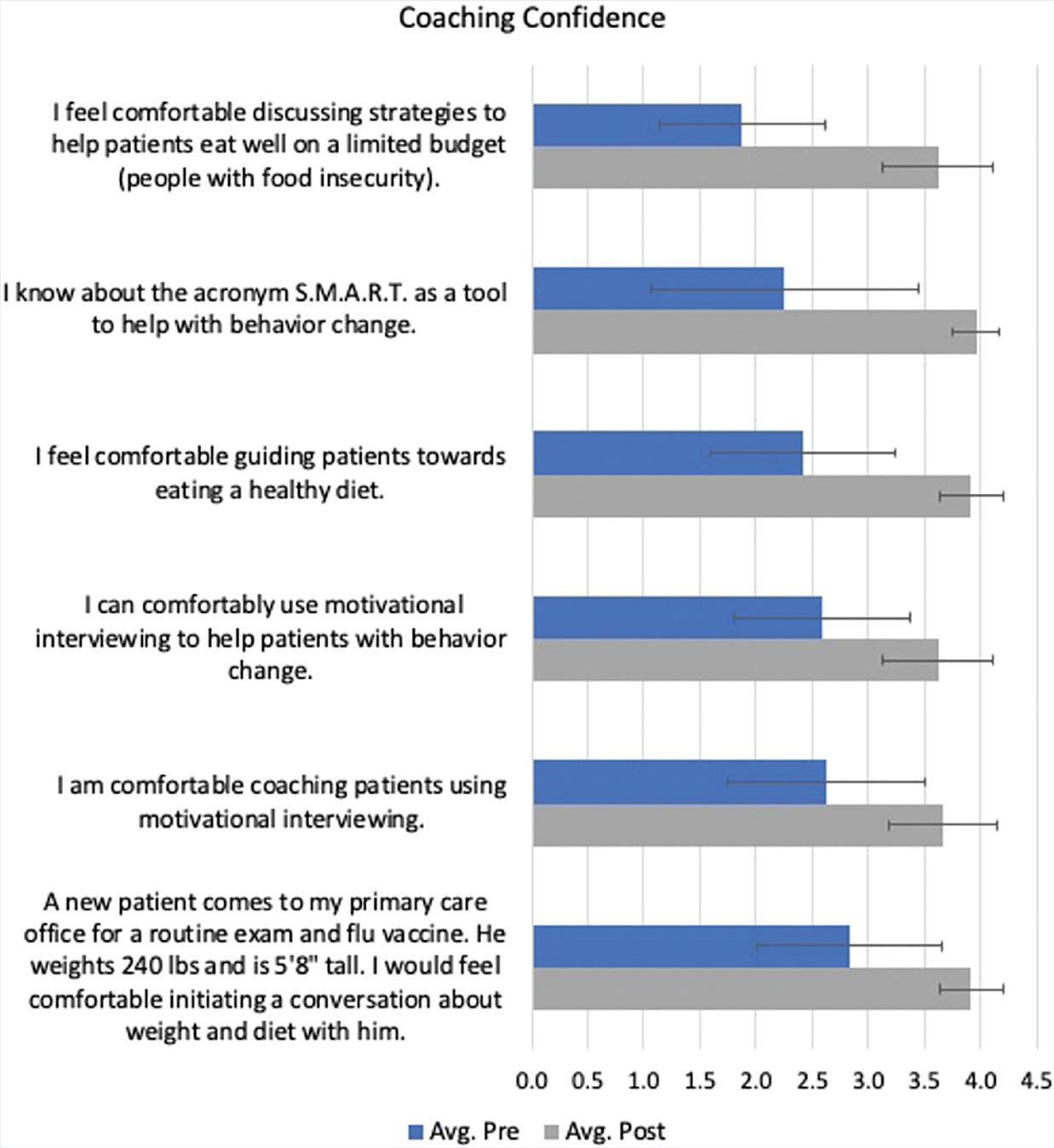
Coaching confidence pre- and post-test scores (n = 24).
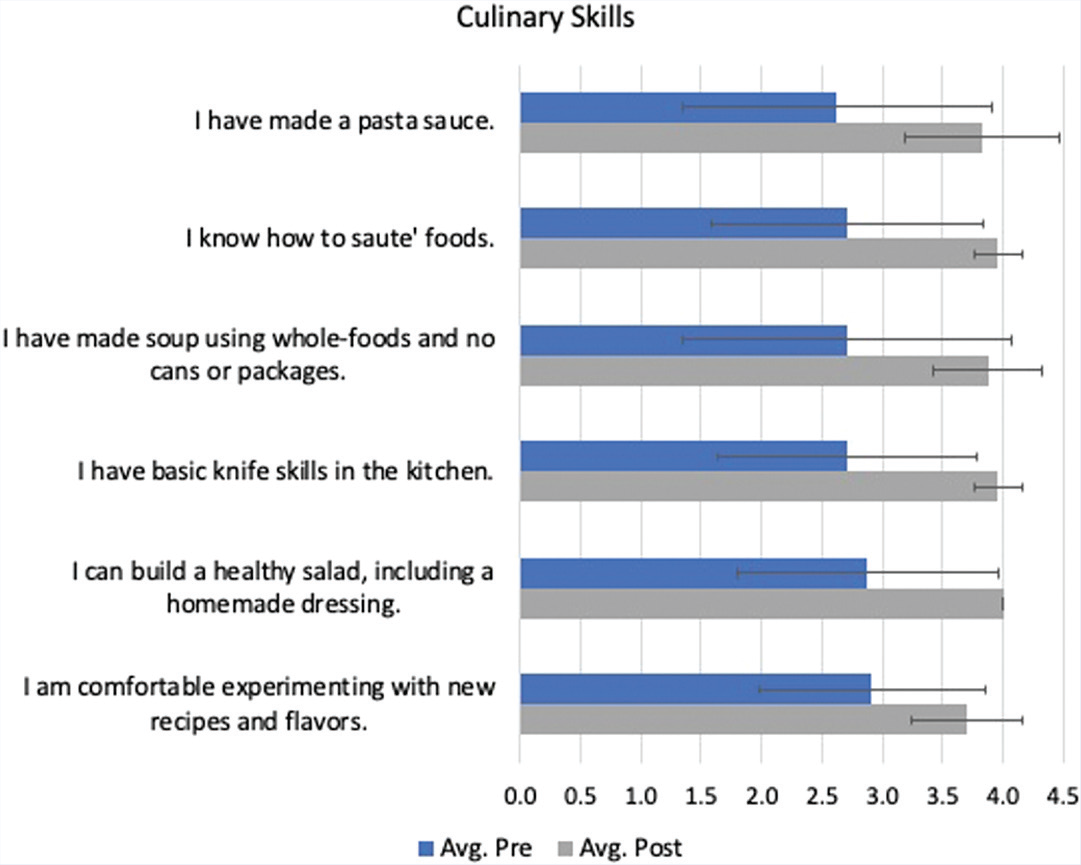
Culinary skills pre- and post-test scores (n = 24).
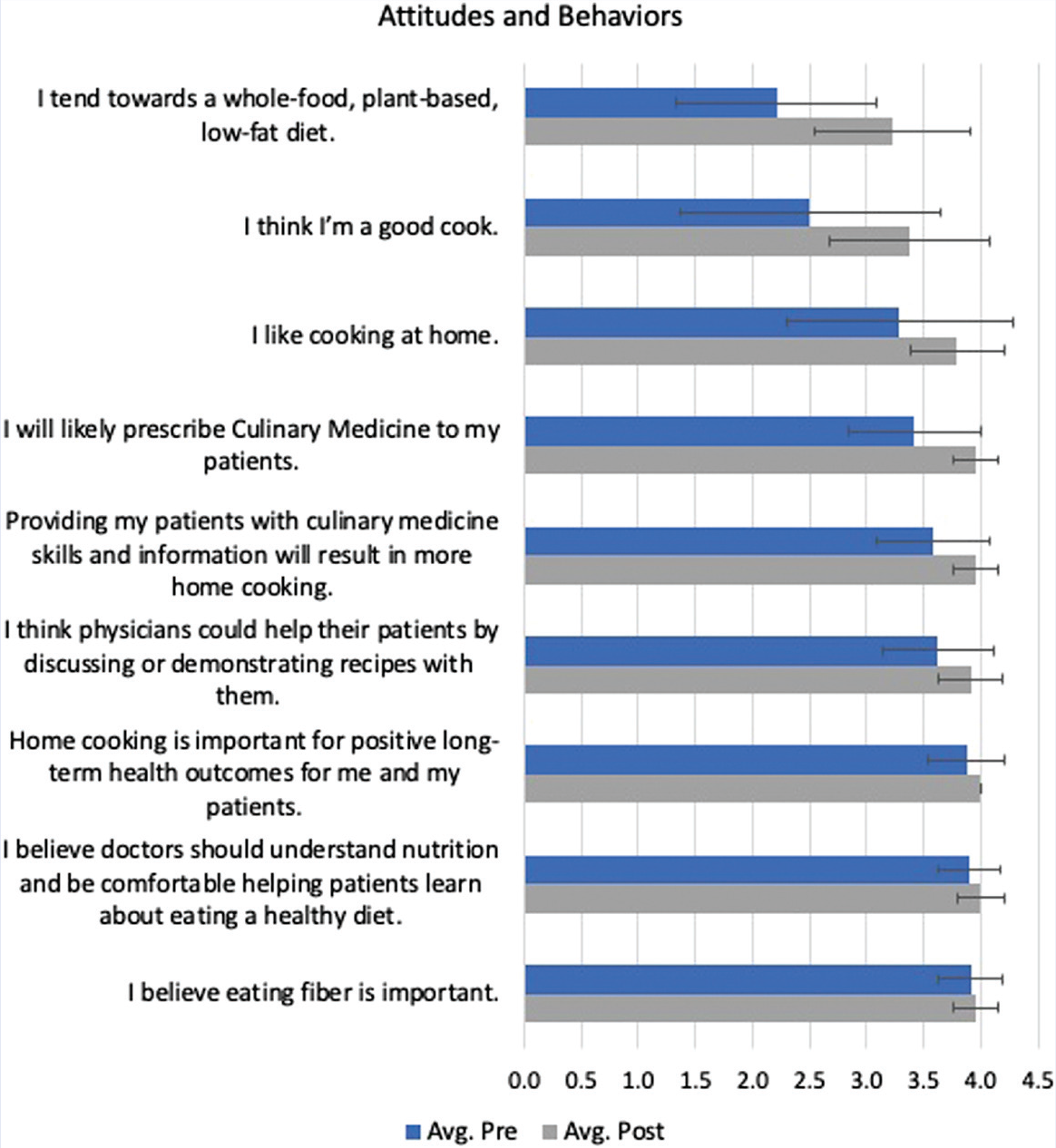
Attitudes and behaviors pre- and post-test scores (n = 24).
On the pre-test, 5/26 (19%) of answers had an average score ≥ 3.5/4 with 0/26 (0%) achieving a score of 4/4, whereas on the post-test, 24/26 (92%) of questions had an average score of ≥ 3.5/4 with 13/26 (50%) achieving a 4/4 score (P < .0001 for both). The only 2 post-test responses with an average score of < 3.5/4 were “I think I’m a good cook” and “I tend towards a whole-food, plant-based, low-fat diet.” Both responses, however, showed a significant increase in the desired personal attitude and behavior, namely, pre: 2.5; post: 3.4 and pre: 2.2; post 3.2, respectively. (P < .0001)
We found no significant difference in responses over the 3 different elective offerings or the 2-week course vs the 4-week course; however, there were only 4 students in the 2-week group, therefore, further research should be done to verify the effectiveness of the condensed elective offering.
Key Qualitative Observations of the Online Program
Course Directors
As course directors, we found the presentation of the course personally rewarding due to our perception of the urgent need for such a program and the overwhelmingly positive response of the students. Our main concerns were finding time to develop a novel 1-month virtual course and then lead and coordinate the sessions. We aimed to present the course in a positive and personal manner that incorporated not only nutrition as part of a healthy lifestyle but incorporated other aspects of a healthy lifestyle, that is, minimizing stress and increasing social connections and mindfulness. We felt these aspects were fundamental given the stress and social isolation experienced by many students during the COVID-19 pandemic and the stress related to their final year at medical school and preparations for residency. We also wanted to present a wide variety of remote learning experiences to the students, given their inability to participate in normal daily activities. This led to a rich but complex schedule that required frequent modifications due to unanticipated scheduling changes or efforts to improve aspects of the program. We considered that the chosen number of 8 students allowed for the desired individual teaching and support.
We determined the CMC to be an excellent foundation for the course, providing detailed practical culinary skills sessions appropriate for medical students and integrating our other course objectives of evidence-based learning and coaching. We also found an abundance of materials in the curriculum, online, and in the course textbook that could be used to expand the information and experienced and enthusiastic experts to assist with presentations. We were concerned that the cost of food, materials, and a textbook for the students was unexpected and challenging for some, despite support from the ACLM microgrants.
Concerning the technical aspects of the course, the ZOOM platform generally worked well for group discussions and cooking demonstrations. However, during the interactive cooking sessions, the students muted their microphones, so conversation was difficult. The single camera most students used on their phone or laptop showed the cutting board or stove-top well but generally did not allow for viewing beyond this. Our chef used a double-camera setup, one displaying the cutting board and one over the stove.
Students
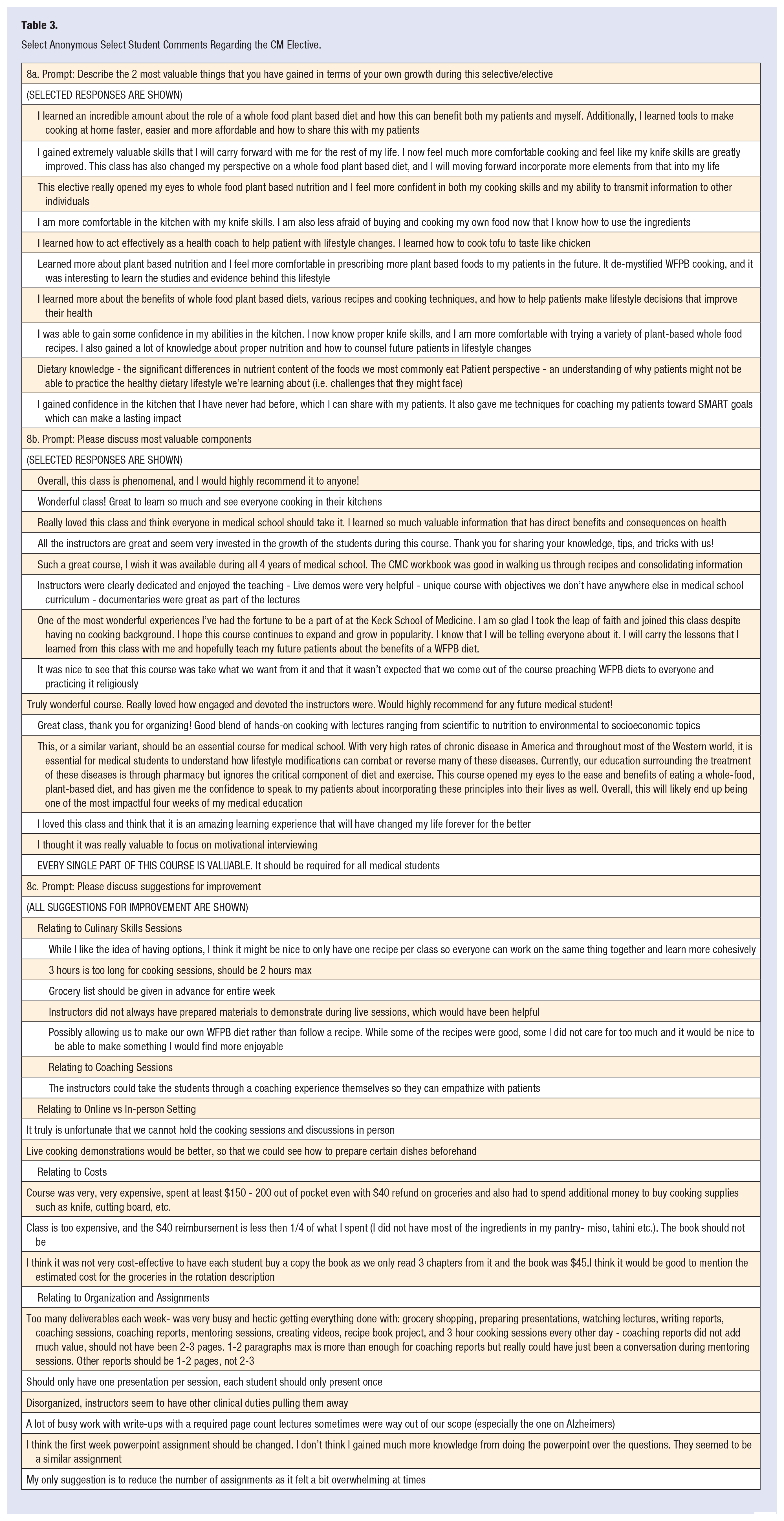
In confidential medical-school–mandated evaluations of the course by the students, the responses were overall very positive. Students particularly highlighted improved skills, knowledge, and patient coaching strategies as critical benefits. Suggestions for improvement related primarily to requests for better organization of the course material and assignments. Additionally, a few commented that the cost of food and the required textbook was unexpectedly high. Select positive comments are included, and all suggestions for improvement are given in Table 3.
Select Anonymous Select Student Comments Regarding the CM Elective.
Administration
The KSOM Associate Dean for Curriculum noted the overall success of the elective. The directors were invited to continue offering the course to fourth-year students and prepare a proposal to offer sessions in Lifestyle and Culinary Medicine to incoming first-year medical students.
Discussion
This manuscript describes the rationale and method for establishing a novel 1-month online elective culinary medicine program for fourth-year medical students. The program used a whole-food plant-based approach to nutrition and was based on teaching materials available to all healthcare professionals through the ACLM. We determined that the project was feasible and achieved our objectives of improving nutrition knowledge, coaching confidence, culinary skills, and desired attitudes and behaviors.
Culinary medicine courses for medical students vary in the stage of training at which they are offered to students, the duration of the training, and the course classification as either “required” or “elective.” Our course was offered to fourth-year students as a 1-month elective. Most students had received minimal prior training in nutrition or other components of a healthy lifestyle. Yet, most were about to enter primary care residencies where management of lifestyle-induced chronic disease would be a large part of their work. Typically, nutrition courses are taken by pre-med students and are not a prerequisite for entering medical school. 19 Of the peer-review reports of culinary medicine courses offered to medical students, most have been elective courses for pre-clinical students of concise duration and involved only a small proportion of the class.16,20-23 Rothman 24 has reported a culinary medicine elective course for fourth-year medical students comprising eight 2-hour sessions. The students requested the locally developed course, most of whom said receiving minimal prior education in nutrition. The “Health Meets Food” curriculum was developed at Tulane University in 2013, and components of this course are designed for all stages of medical training. Access to this program is by license, and currently, it is used in over 55 medical schools. 25 Our course provided a relatively intensive program for graduating medical students about to enter a primary care residency but who had received little, if any, formal training in nutrition during medical school. At this stage in medical school, the students appeared to be particularly receptive to learning the course content. They recognized its immediate relevance not only to their patients but also to themselves, their family members, and their friends. They were able to make informed comparisons to the more typical approach to chronic disease management, namely, tertiary care for established disease. We consider it of particular value to provide these graduating students with practical and long-lasting tools for self-care. As is well-recognized, medical residency is typically associated with an overall unhealthy lifestyle and an increased risk of developing a chronic physical and mental disease. 5
Curriculum content also varies between courses. The core of our curriculum was 2 publications from the ACLM: the CMC14,17, and selected chapters from the LMH. 15 These curricula promote a whole-food plant-based approach to nutrition and patient coaching techniques, and we emphasized the health and environmental aspects of this approach to eating. We expanded the core texts to take advantage of local experts and topics of particular interest to the students. Currently, the most widely used curriculum for teaching culinary medicine in medical schools is “Health Meets Food,” which teaches a Mediterranean diet. 25 At other medical schools, curricula have been locally developed by healthcare professionals and students themselves.19,24,26,27
The use of telemedicine to teach medical students significantly increased in 2020 due to the COVID-19 pandemic. We found the benefits and disadvantages of using this approach for teaching culinary medicine. Advantages included providing students the ability to work at different “paces and places” with the opportunities to shop for ingredients, use their own kitchen tools, keep their kitchen workspace clean and organized, and learn from their own mistakes. We also believe that working in one’s kitchen allows a mental immersion into the work at hand or “mindfulness,” which is a natural stress reduction. Students were always pleased to have an interactive faculty-driven kitchen teaching event.
Disadvantages were the need for students to each buy the supplies for each session, our inability to do hands-on culinary instruction in the kitchen, and the inability to taste and smell the food as a group. We are not aware of any prior telemedicine teaching of culinary medicine to medical students. Polak et al, however, have successfully pioneered teaching evidence-based culinary coaching online to healthcare professionals virtually with a “CHEF” course (Culinary Health Education Fundamentals), which is led by health coaches trained in the program.28,29 The trained healthcare professionals use the knowledge gained in direct patient care. While we realize that hands-on teaching of culinary techniques has its benefits, we also now appreciate the benefits of distance learning. The live lectures and mentoring sessions were convenient for the speakers and students and allowed personal connection and social support. Students with other commitments such as residency interviews could join or leave a session more conveniently than in-person sessions. By contrast, direct patient interaction and counseling and community service programs were difficult to organize for this particular course, although they are desirable components. As might be expected with the rapid adoption of new technology, technical difficulties included difficulty logging in to a session and an unstable internet connection for some of the participants. However, these were manageable issues. We anticipate that a hybrid remote and in-person approach to teaching culinary medicine will offer a suitable format for future courses.
There is a groundswell of medical schools offering culinary medicine courses, yet qualitative assessment of the efficacy of these approaches remains limited. Findings to date, however, are consistently positive. We found that fourth-year students improved all 4 domains evaluated, with generally positive narrative responses from students, course directors, and administrators. Our findings are similar to preliminary data by the CMC developers in pre-clinical students. 15 Monlezun et al 30 have reported that a multisite cohort study of hands-on cooking and nutrition education using the “Health Meets Food” curriculum vs a traditional curriculum for medical students was associated with improved patient counseling competencies on nutrition while improving students’ diets. This large study involved 3248 unique medical trainees from 20 medical schools and was conducted from 2012 to 2017. A single-site independent assessment of the same program in 60 first-year students reported that the course was associated with increased counseling confidence, familiarity with evidence-based nutrition interventions, and understanding of the role of interprofessional engagement to address lifestyle-related disease. 31 We propose a future study recording patients’ progress over time as a direct result from coaching received by students taking this elective.
Significant limitations of our course design were the relatively high proportion of non-standardized material. While this allowed us to incorporate live speakers and a wide variety of topics, it was time-consuming for the course directors to develop and monitor this design, potentially confusing the students. We became increasingly aware that the cost of equipment, ingredients, and the textbook were financially challenging for some students. Additionally, some students found it challenging to coach their family members, a problem familiar to many healthcare professionals. We hope to incorporate primary care practices into our program in future sessions to allow students to have direct patient interactions about nutrition and practice their coaching skills. Significant limitations of our data analysis are the relatively small number of students involved and the short duration of follow-up.
We recommend telemedicine CM courses, such as the one described here, continue to be offered and refined, given the strong positive outcomes of even these early sessions. To reduce the cost to students working remotely, we will prepare and distribute a “care package” at the start of class that will include basic kitchen utensils (chef’s knife, cutting board, and measuring spoons) and small amounts of bulk purchases of some products (e.g., nutritional yeast, dried spices, and herbs). We recommend that frequent live interactive kitchen skills sessions be incorporated into the course and that more standardized coursework be provided for self-study, preferably at low or no cost to the student. Cooking demonstrations for patients should be used to teach nutrition counseling and social determinants of health. 32
We are currently exploring alternate methods of assessment for future course offerings. One such option is the Cooking with a Chef Survey, 33 validated by various research studies. This survey consists of 8 sections, 6 scales, and one knowledge test that evaluates the following: availability and accessibility of fruits and vegetables, cooking attitudes, cooking behaviors, self-efficacy of produce consumption, cooking self-efficacy, self-efficacy for using basic cooking techniques, self-efficacy for fruits, vegetables, seasonings, and knowledge of cooking terms and techniques. In addition, the pre- and post-questionnaires will be modified to overarching group themes and may be expanded to assess additional topics.
Summary
We successfully adapted an open-source whole-food plant-based culinary medicine curriculum into a 1-month online elective for advanced medical students. We demonstrated statistically significant improvement in nutrition knowledge, coaching confidence, culinary skills, and desired attitudes and behaviors. This course filled a need for further training in nutrition for both self-care and patient care for students as they start their professional careers. We propose developing a more standardized open-source version of this initial course.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.