
Abstract
As medical schools work to train the next generation of providers, including robust content in nutrition education is paramount. The National Academy of Sciences sets the benchmark for 25 hours of nutrition education in medical schools, though many schools do not meet this requirement. Usually, nutrition lectures in medical schools are given in the pre-clinical years and focus on biochemistry and micronutrients. During the COVID-19 pandemic, there was a unique opportunity to quickly develop and implement an elective course for 3rd and 4th year medical students at the University of North Carolina School of Medicine. A course was created in lifestyle medicine and culinary medicine, and all were delivered remotely through Zoom. This course would be simple to replicate at other institutions and was very well received. This article will describe more of the resources, methods, and reactions to this course.
Keywords
“...complete cessation may not be appropriate for all drivers with glaucoma...”
Background
Lifestyle factors are causal for chronic diseases in the United States. Doctors who exercise are more likely to counsel their patients on exercise. 1 Physicians who are overweight are less likely to counsel their patients on weight management. 2 Research is limited on physician’s personal practices of home meal preparation and what association there may be with counseling of patients. However, the data are clear that cooking at home is healthier and even decreases patients’ risk of diabetes. 3 Unfortunately, citizens in the United States are increasingly eating meals that have not been prepared at home. 4 Incorporating food preparation into group visits with patients has been successfully done and well received. 5
Culinary medicine is the practical application of nutrition theory to the morsels of food that enter patients’ mouths. Increasingly, culinary medicine programs have been adopted at a variety of medical schools in the United States. The Cooking for Health Optimization with Patients curriculum is a hands-on cooking-based nutrition education program, which has been implemented at 32 medical programs across the United States. 6 They noted that students enrolled in this were more likely to agree with regular nutrition counseling for patients. The dearth of kitchen space in medical schools and demand for other content in medical school education has been a limiting factor for this program. Limited kitchen access and inconsistent funding unfortunately halted a successful culinary medicine course at Stanford. 7 The CHEF coaching program 8 does have an aspect of tele-education and is mainly used by residents. Teaching medical students to cook likely increases the odds that these medical students will teach their patients to cook and that they themselves as providers may develop healthier habits.
Methods
Participants in this course included twenty-one 3rd and 4th year students from the University of North Carolina School of Medicine. Students utilized course content through the free online platform NextGenU 9 for self-study and foundational learning. They also completed a free culinary medicine course through the online course provider Coursera from Stanford University. 10 On their own time, students explored a recipe of their own design through the Meal-o-matic functionality on the “Doctor Yum” website. 11
Live lectures covered material on the evidence surrounding a whole-foods plant-based diet, the controversies in nutritional health policy, and best practices in counseling patients regarding diet and nutrition. We discussed different theories behind behavior change and the main principles of motivational interviewing. Via Zoom, students were put into small groups to set their own personal health goals and coach each other. Students stayed with their partner groups throughout the course.
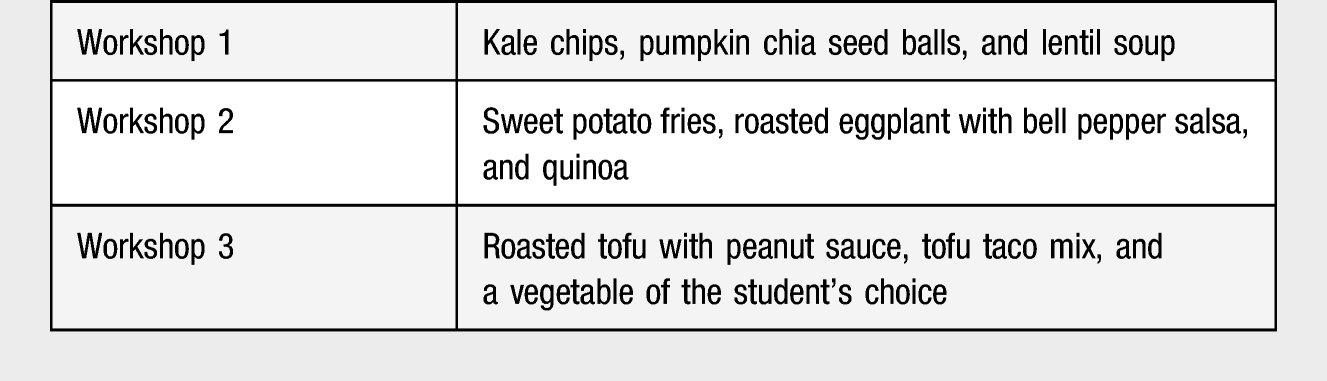
In three separate live group sessions, all participants in the course cooked the same recipe concurrently, each participant in their own kitchen. The recipes were all plant based. Cooking workshops were each approximately 75 minutes in length.
Cooking Workshops
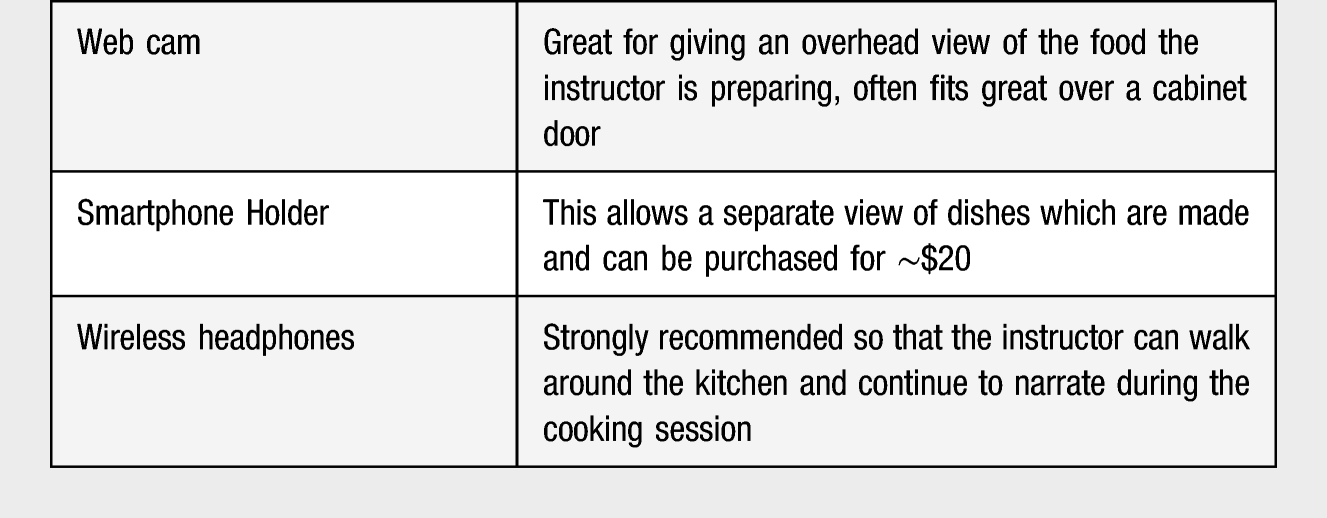
Equipment Needed for Home Cooking Set Up
Results
Students were surveyed before the course on their comfort in counseling patients on a variety of LM topics. Following the course, students were again surveyed to assess their self-reported confidence in these areas and to give feedback on the course. There were 21 students in the course. We received 21 pre-course surveys and 18 surveys following the conclusion of the course. The pre- and post-survey data indicated increased student confidence in comfortability counseling patients on nutrition, knowing credible resources to refer patients for them to learn more about nutrition, shopping for healthy ingredients/meals on a budget, and comfortability counseling patients on the relationship between sexuality and one’s health.
In the post-survey responses, all students agreed or strongly agreed that they would recommend this course to other medical students. All students also felt comfortable that they could foresee writing an exercise prescription for a patient in the future. Pre-survey results indicated only 29% of students agreed that they were comfortable counseling patients on nutrition. Following completion of the course, 95% of students felt comfortable in counseling patients on nutrition. 94% of students felt that cooking together in a virtual setting helped improve their ability to counsel patients on cooking and nutrition.
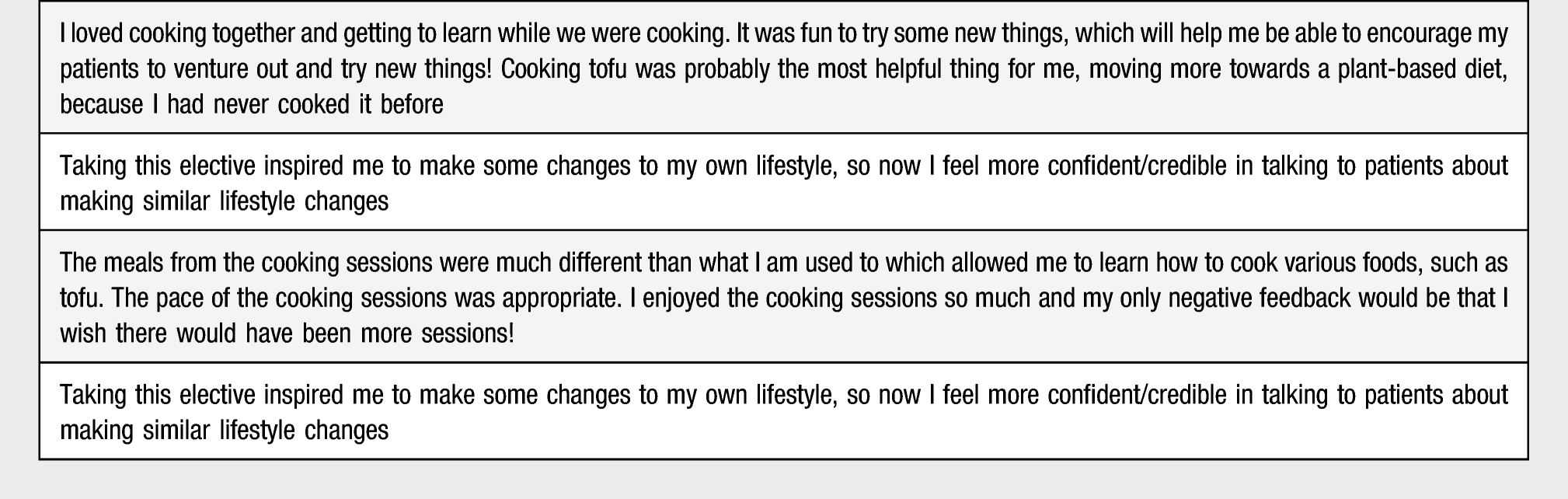
Notable qualitative comments from students are included.
Student Comments on the Course
Discussion
This article describes an innovative way to use virtual classes to help students become more familiar with cooking and counseling patients about lifestyle changes. The students enjoyed the course and their subjective self-assessments indicated significant improvements in the subject matter. One limitation of our course is that we did not objectively assess an improved facility in patient interactions or knowledge of LM subjects. Our preliminary survey results suggest that this is an innovative option that other schools may consider as a trial in their curriculum.
Implementing a course with aspects of culinary medicine offers medical educators a chance to participate in the cutting edge of lifestyle medicine practices and can improve the personal cooking habits of students and educators alike. A survey conducted by Vetter et al 12 indicated an overwhelming 86% of physicians that felt they lacked adequate training to provide nutrition counseling. Considering the correlations between healthy diets and reduced risk of several chronic diseases, 13 there is a need to equip medical students with the confidence and competence required to effectively counsel patients on nutrition. With virtual technology, we are not limited by a lack of a teaching kitchen. In fact, teaching students to cook in their own kitchens may be more powerful because they know they can make meals in the space that is available to them with the tools that they have. It also engages the student in making a trip to the grocery store and procuring ingredients they may not have purchased before. As curricula are increasingly put online, an entirely virtual culinary medicine course is an engaging way to teach students and even allow them to bond with each other and improve their health and clinical skills. As we work to decrease physician burnout, empowering medical students with hands-on methods to improve their own health is critical to their success.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.