
Abstract
Background. Healthy diet represents one of the largest single modifiable risk factors proven to decrease rates of obesity and associated chronic disease, but practical approaches to improving dietary habits through nutritional intervention are limited. Objective. To evaluate the effectiveness of a medical student–led, 6-week culinary course on participants’ dietary knowledge and behaviors, particularly focusing on the tenets of the Mediterranean diet (MedDiet). Design. This study is a prospective multisite cohort study evaluating the effects of a 6-week, hands-on community culinary education course offered at 3 sites. Participants’ knowledge of cooking skills, eating habits, and adherence to the MedDiet were evaluated using a survey prior to beginning and 6 weeks after the completion of the course. Analysis was conducted using multivariable regression to assess subjects’ diets, associated behaviors, and nutrition beliefs according to the number of classes to which they were exposed (0 to >6). Statistical results were then compared with the machine learning results to check statistical validity after selection of the top-performing algorithm from 43 supervised algorithms using 10-fold cross-validation with performance assessed according to accuracy, root relative square error, and root mean square error. Results. Among the 1381 participants, cooking classes significantly improved patients’ overall 9-point MedDiet adherence (β = 0.62, 95% CI 0.23-1.00, P = .002). Participants were more likely to meet MedDiet point requirements for fruit intake (odds ratio [OR] 2.77, 95% CI 1.46-5.23, P = .002), vegetable intake (OR 4.61, 95% CI 1.85-11.53, P = .001), legume intake (OR 2.48, 95% CI 1.45-4.26, P = .001), and olive oil use (OR 2.87, 95% CI 1.44-5.74, P = .003), and were less likely to believe that cooking takes excessive time (OR 0.31, 95% CI 0.16-0.59, P < .001). Conclusion. Hands-on culinary education courses were associated with increased MedDiet adherence and improved knowledge of healthful eating. Such interventions thus represent a cost-effective option for addressing rates of obesity and obesity-related chronic illness.
‘Extensive research has shown that MedDiet [Mediterranean diet] adherence can decrease rates of cardiovascular disease and a myriad other health conditions.’
Few issues shape our current health care landscape as prominently as obesity. Once an issue predominantly affecting developed countries, recent studies have highlighted increasing rates of obesity and obesity-related disease on a global scale.1,2 The correlation between obesity and chronic disease is well documented, with increased body mass index (BMI) leading to higher rates of diabetes, hypertensive heart disease, and stroke. 3 Obesity-associated health care costs also pose a major challenge for the US health care system, with total costs attributable to overweight and obesity projected to double each decade and amount to over $800 billion by 2030. 4 Healthy diet and positive lifestyle modification have been shown to lower rates of chronic disease, and evidence points to the emerging role of education about healthful cooking in addressing these challenges. 5
The Mediterranean diet (MedDiet) is the most well-studied nutrition-based intervention. Extensive research has shown that MedDiet adherence can decrease rates of cardiovascular disease and a myriad other health conditions.6-8 A case-control study published in 2013 evaluating 2 variants of the MedDiet as a means of primary prevention of cardiovascular disease found a significant reduction in cardiac events in the study groups to 96 and 83 versus 109 in the control group. 9 Extrapolated to a population level, this represents a potential reduction of 1.75 and 3.5 events per 1000 patients, respectively. Another meta-analysis indicates that a 2-point increase in adherence score to the MedDiet can reduce overall mortality by 8% and decrease the risk of developing cardiovascular disease by 10%. 8
The MedDiet has also been shown to improve fasting glucose, postprandial glucose, and hemoglobin A1c levels in patients with type 2 diabetes mellitus. 10 The benefit of adherence to the diet has been shown with regard to cancer mortality, with one analysis demonstrating an inverse relationship between MedDiet adherence and cancer mortality for a variety of different cancers. 11 A relationship has also been observed between the incidence of neurodegenerative diseases and the MedDiet, with data suggesting the diet provides a protective effect against the development of neurological diseases such as Alzheimer’s dementia and Parkinson’s disease as well as overall cognitive decline.12-14
Evidence also points to significant cost saving opportunities offered by the MedDiet. In a study evaluating the effectiveness of the MedDiet versus a traditional Western diet in patients with previous myocardial infarction, the MedDiet resulted in an incremental cost per quality adjusted life year of $703 per person. 15 When considering the reduction in future cardiac events and cost of the MedDiet versus traditional Western diet, the MedDiet was demonstrated to be a highly cost-effective intervention option. Another study considering the national economic burden of cardiovascular disease and potential cost savings from widespread MedDiet adherence estimated that the United States could save between $6.3 and $15.7 billion annually with widespread adoption of this dietary pattern. 15 With the prevalence of obesity and obesity-related illness continuing to rise, nonpharmacologic approaches offering benefit on both an individual and population level warrant further investigation. 16 Given the paucity of practical approaches to implementing the MedDiet, however, adherence remains a major barrier to widespread adoption. 17
Within the medical community, there is significant interest in the importance of dietary counseling and intervention as a means to improve patient health outcomes.18-20 The gap in medical practitioner knowledge, however, limits the ability for significant nutrition counseling. 21 The Cooking for Health Optimization (CHOP) study was developed as means for implementing training for medical students based on the tenets of the Mediterranean diet using the Health Meets Food curriculum, and represents the largest study on nutrition education of medical trainees. This study expands on that premise by utilizing medical students as a force multiplier to disseminate this information further to participants in community-based cooking courses.
Materials and Methods
All procedures in this study were approved by the local and respective site-specific institutional review boards. This trial is a prospective multisite cohort study aimed at evaluating the effects of a 6-week community culinary education course at 3 sites. The Health Meets Food intervention consists of six 2-hour, medical student–led cooking courses conducted weekly over a 6-week period. Courses were conducted at 3 independent sites: Goldring Center for Culinary Medicine at Tulane University School of Medicine, Church Health Center in Memphis, Tennessee, and Spectrum Health in Grand Rapids, Michigan. Participants were administered a survey regarding their knowledge of cooking skills, eating habits, and adherence to the MedDiet prior to starting the first class of the course, and again 6 weeks following the completion of the final class.
The 6-class series focuses on basic nutrition education, practical strategies for healthful cooking, and basic culinary skills participants can use on a regular basis in their own homes. Each 2-hour class consists of 1 hour of hands-on cooking, and 1 hour in which the meal is shared over discussion of nutrition-related topics such as meal planning, identifying healthful foods in the grocery store, strategies for healthful snacking, and the utilization of leftovers for future meals. An emphasis is placed not only on cooking at home with healthy ingredients but also the financial and social benefits of these activities. Time is also spent working to dispel commonly held notions such as “cooking takes too much time” and “buying healthy foods is too expensive.”
The study population consists of local community members, predominantly from Orleans Parish, interested in honing cooking skills and nutrition education to improve dietary habits. The New Orleans population represents a high-risk population primarily from underserved areas with lower health literacy and health care system access. United States census data released in 2018 indicated that the city boasted the highest official poverty rate among the 50 largest metro areas in the country at 18.6%. 22 Similarly, a study published by the New Orleans Department of Health in 2013 indicated that of the 64 parishes of Louisiana evaluated in the study, Orleans Parish ranked 60th in overall health outcomes, with some of the highest rates of heart disease and the lowest life expectancy in Louisiana. 23
Prior to participating in the admininstration of the community cooking courses, medical students were trained on fundamental cooking techniques and education topics. Students completed a variety of online modules covering topics such as cooking measurements and abbreviations, fundamentals of the MedDiet, making stock, safe reheating temperatures, and mindful eating. Competence was evaluated with an online quiz requiring a minimum passing score in order to assist in the community classes. The primary objective was to ensure medical students had the ability to disseminate proper techniques and relevant information to community members.
Study Design and Statistical Methods
This is a prospective cohort study. Study inclusion criteria for consecutively enrolled subjects included age >17 years and indicated ability to complete at least 1 cooking class from Augus 1, 2014 to December 31, 2018. Exclusion criteria were subjects failing to complete the survey response for the number of classes taken. Analysis was conducted according to 2 stages. In the first stage, multivariable regression was conducted to assess subjects’ diets, associated behaviors, and nutrition beliefs according to the number of classes to which they were exposed (0 to >6). Multivariable regression controlled for age, sex, race, special diet, education, provider nutrition counseling, the likelihood of receiving classes (through doubly robust propensity score adjustment), and time-invariant unobserved traits. Statistical results were then compared with the machine learning results after selection of the top-performing algorithm from 43 supervised algorithms using 10-fold cross-validation with performance assessed according to accuracy, root relative square error, and root mean square error. Machine learning was used to check statistical validity in the study. Results are reported at the minimal effective dose or the number of classes, if applicable, required to produce significantly improved outcomes. Statistical significance was set at 2-tailed P < .05. All analyses were performed in STATA 14.2 (STATACorp, College Station, TX, USA) and Java 9 (Oracle) was used for machine-learning analyses. Ethics approval was obtained through the institutional review board of Tulane University.
Results
From fall 2012 to 2018 across 3 sites nationally, 1381 subjects met study criteria and generated 1514 responses to the CHOP evidence-based survey. Subjects were asked to indicate their weekly behaviors with regard to a variety of food-consumption metrics, including each of the 9 tenets of the MedDiet. Weekly behavior incidence was then translated into a MedDiet adherence score using the structure of the well-validated Martínez-González et al study to determine if the frequency met or did not meet the criteria point.24,25 Each point was defined as consumption of: olive oil (≥1 spoon/day), fruit (≥1 serving/day), vegetables (≥1 serving/day), fruit (≥1 serving/day) and vegetables (≥1 serving/day), legumes (≥2 servings/week), seafood (≥3 serving/week), wine (≥1 glass/day), meat (<1 serving/day), and whole-grain bread (>5 servings/week). Behavior most days was defined as completing the given behavior between 5 and 7 days per week.
The cooking classes significantly improved patients’ overall 9-point MedDiet adherence (β 0.62, 95% CI 0.23-1.00, P = .002; Table 1). Diet adherence was further analyzed to sort participants into high-/medium- and low-adherence groups. High adherence was defined as scoring 7 to 9 points, medium 3 to 6 points, and low adherence was defined as 1 to 2 points on the MedDiet scale. Subjects were significantly more likely to have high/medium versus low adherence to the MedDiet following the class series (odds ratio [OR] 2.73, 95% CI 1.42-5.74).
CHOP-Community Machine Learning–Augmented Propensity Score–Adjusted Fixed Effects Multivariable Regression for Causal Inference via Controlling for Selection Bias. a
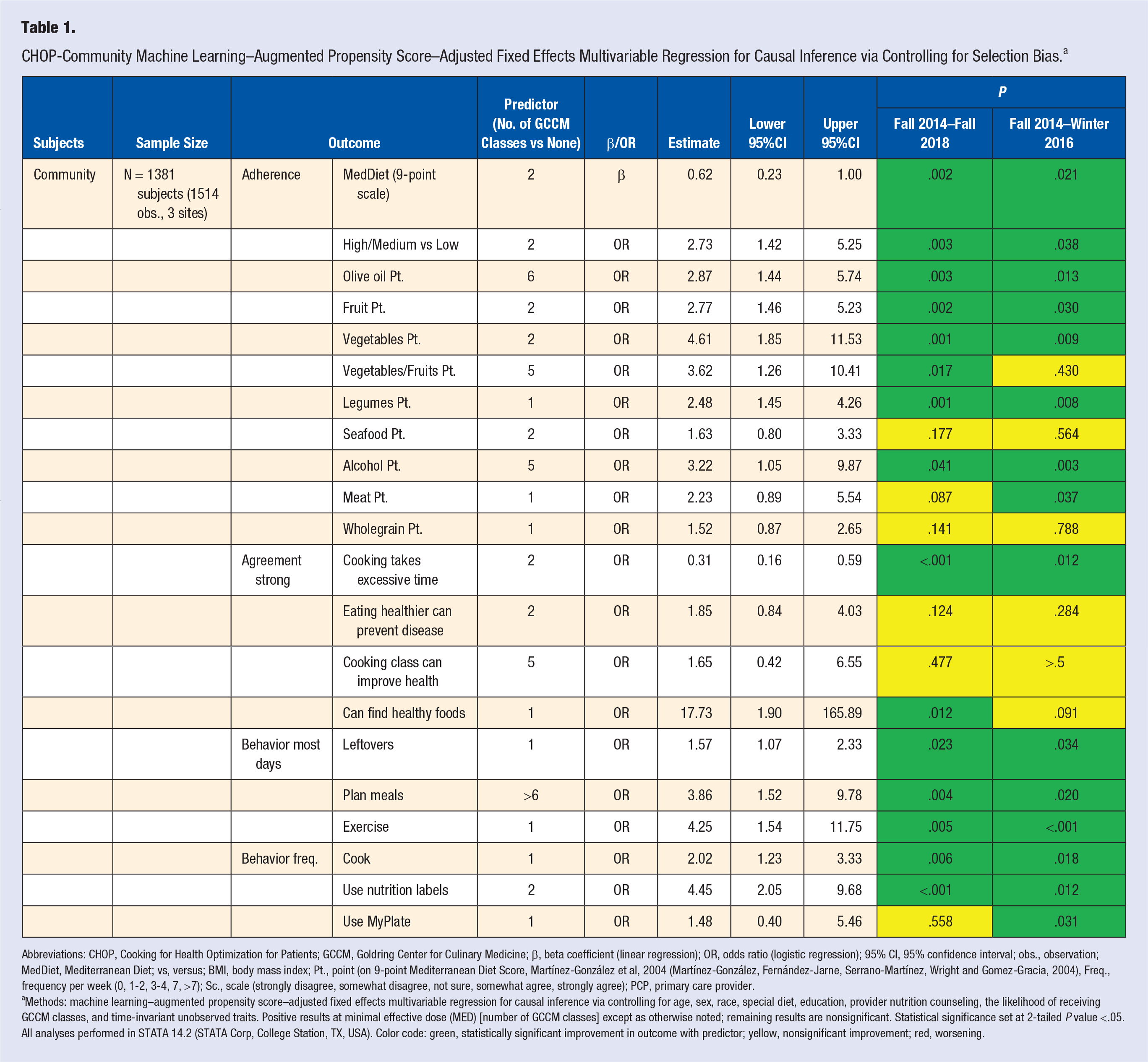
Abbreviations: CHOP, Cooking for Health Optimization for Patients; GCCM, Goldring Center for Culinary Medicine; β, beta coefficient (linear regression); OR, odds ratio (logistic regression); 95% CI, 95% confidence interval; obs., observation; MedDiet, Mediterranean Diet; vs, versus; BMI, body mass index; Pt., point (on 9-point Mediterranean Diet Score, Martínez-González et al, 2004 (Martínez-González, Fernández-Jarne, Serrano-Martínez, Wright and Gomez-Gracia, 2004), Freq., frequency per week (0, 1-2, 3-4, 7, >7); Sc., scale (strongly disagree, somewhat disagree, not sure, somewhat agree, strongly agree); PCP, primary care provider.
Methods: machine learning–augmented propensity score–adjusted fixed effects multivariable regression for causal inference via controlling for age, sex, race, special diet, education, provider nutrition counseling, the likelihood of receiving GCCM classes, and time-invariant unobserved traits. Positive results at minimal effective dose (MED) [number of GCCM classes] except as otherwise noted; remaining results are nonsignificant. Statistical significance set at 2-tailed P value <.05. All analyses performed in STATA 14.2 (STATA Corp, College Station, TX, USA). Color code: green, statistically significant improvement in outcome with predictor; yellow, nonsignificant improvement; red, worsening.
With regard to individual MedDiet points, participants were more likely to meet MedDiet points for fruit intake (OR 2.77, 95% CI 1.46-5.23, P = .002), vegetable intake (OR 4.61, 95% CI 1.85-11.53, P = .001), legume intake (OR 2.48, 95% CI 1.45-4.26, P = .001), and olive oil use (OR 2.87, 95% CI 1.44-5.74, P = .003).
Subjects were less likely to believe that cooking takes excessive time (OR 0.31, 95% CI 0.16-0.59, P < .001), and had higher odds of the following frequent behaviors: cooking (OR 2.02, 95% CI 1.23-3.33, P = .006), using leftovers (OR 1.57, 95% CI 1.07-2.33, P = .023), and planning meals (OR 3.86, 95% CI 1.52-9.78, P = .004). The median number of classes required to produce statistically significant improvements in all outcomes was 2.
Discussion
Identifying strategies for the practical implementation of evidence-based dietary interventions is a significant barrier to the effectiveness of such practices. Diet represents one of the single largest modifiable risk factors for the prevention of the development of cardiovascular disease. 26 Consequently, low-cost interventions addressing nutritional knowledge to positively affect dietary behavior change offer significant value. 27 This study demonstrates the ability of hands-on cooking classes to positively affect patients’ knowledge of nutrition and the MedDiet in 3 different demographic settings.
Notably, participants were more likely to reach MedDiet point thresholds in fruit consumption, vegetable consumption, olive oil use, and alcohol consumption. After participating in programming, they were also significantly less likely to agree with the notion that cooking takes excessive time. As previous studies have demonstrated the health and financial benefits of cooking at home versus outside the home, working to dispel commonly held misconceptions surrounding cooking carries notable importance. 28 Interestingly, the results also highlight the lack of fundamental nutrition knowledge many patients carry. However, after completing the 6-week culinary class series, participants were significantly more likely to strongly agree with the statement “I can find healthy foods.” This demonstrates that even low-dose interventions may produce notable improvements in patient’s diet.
The potential cost-saving opportunities offered by increased adherence to the MedDiet are an important consideration. We estimate the cost of conducting a 6-class course series for 1 individual to be approximately $120. Extrapolated to a population level, the total cost for 1000 patients to take the class series is about $120 000. A study published in 2014 evaluating the onset and costs associated with inpatient versus outpatient ST-elevated myocardial infarction estimates the cost of a single outpatient cardiac event to be $129 000. 29 Utilizing aforementioned data from the Estrutch et al study (Estruch, Ros and Salas-Salvadó, 2013) and assuming a reduction in events of 2.625 per 1000 (the average reduction in events between the 2 case groups) in MedDiet participants, this represents a cost savings of $218 625 per 1000 people.
Furthermore, the novel study highlights the implementation of the MedDiet in 3 communities with varying socioeconomic statuses. Previous studies have found a correlation between socioeconomic status, education, and MedDiet adherence, although these sample sizes are limited in cohort size and geographic distribution.30,31 New Orleans consistently has one of the highest poverty rates in major metropolitan cities in the United States. 32 Yet data from this study demonstrate that significant strides can be made in nutrition education with low-cost, targeted initiatives. Addressing these inadequacies must start with changing the fundamentally held beliefs surrounding healthy eating and cooking.
Several limitations are evident in the study. The study is observational and relies on self-reported behaviors. The frequency with which these behaviors are truly practiced is not assessed. These reported behaviors were also only assessed 6 weeks following the completion of the participant’s final cooking class. Future studies will evaluate the long-term impact to track whether concepts learned in the courses are practiced following the study period. The study also does not incorporate biometric data or health outcomes such as weight loss, which will be addressed in ongoing randomized trials using the Health Meets Food programming.
Footnotes
Acknowledgements
The authors would like to thank all Tulane medical students and faculty for their contributions to the project and in data collection. ZS, ACR, LS, TSH, and DJM have abided by the publication and authorship rules of The American Journal of Lifestyle Medicine.
Author Contributions
ZS, ACR, LS, TSH, and DJM designed and conducted research. DJM analyzed the data. ZS, TSH, and DJM wrote the manuscript. ZS, ACR, LS, TSH, and DJM revised the manuscript. ZS, ACR, LS, TSH, DJM edited and approved the submitted version. TSH had primary responsibility for final content. All individuals named in the acknowledgments section have provided consent to be named in the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TSH is in part supported by the Humana Foundation. ACR is currently supported through a predoctoral institutional training grant funded by the National Institutes of Health under grant number 5TL1TR001418-04. The study is supported by National Institutes of Health and Humana Foundation.
Ethical Approval
All procedures in this study were approved by the local and respective site-specific institutional review boards.
Informed Consent
All participants provided consent.
Trial Registration
Not applicable, because this article does not contain any clinical trials.