
Abstract
Background: Approximately 40% of college/university students have overweight/obesity; physical activity and sleep play a role. To address these interrelated behaviors, Canada recently released 24-Hour Movement Guidelines. This study aimed to determine (1) the percent of students with overweight/obesity meeting Canadian 24-Hour Movement Guidelines, (2) whether health behaviors differ by demographics, and (3) whether meeting guidelines is associated with BMI. Methods: University students 18–35 years (n = 459) enrolled in a randomized controlled weight management trial completed 1 week of ActiGraph measured activity, self-reported sleep duration, researcher-measured height/weight, and demographics at baseline. ANOVA and t-tests determined differences in student demographics and BMI among those meeting vs not meeting each guideline. Results: Of the analytic sample (n = 403), 341 (84.6%) met the MVPA guideline, 284 (70.5%) met the LIPA guideline, 236 (58.6%) met the sleep guideline, 62 (15.4%) met the sedentary time guideline, and 34 (8.4%) met all guidelines. Students meeting MVPA (30.8±4.3 vs 32.5±4.5, P = .008) or sleep (30.7±4.4 vs 31.6±4.3, P = .04) guidelines had significantly lower BMIs compared to those not meeting each guideline. Percent of students meeting sleep (P = .039) or all guidelines (P = .012) differed by race/ethnicity. Conclusion: Meeting MVPA/sleep guidelines is associated with lower BMI; these behaviors are important targets for future weight management programs.
Among university students who have overweight or obesity, lower body mass index was associated with meeting MVPA and sleep guidelines.
Background
Sufficient physical activity, minimal sedentary behavior, and adequate sleep are independently protective against leading causes of morbidity and mortality in the US, 1 including cardiovascular disease, obesity, and cancer.2-5 These behaviors are also time-codependent movement behaviors, meaning that a reduction in one must increase one or more other movement behaviors within a 24-hour period. For example, reducing sedentary time equates to an increase in either physical activity or sleep, and this exchange is associated with a reduction in cardiovascular disease risk. 6 Consequently, understanding the interplay among movement behaviors and their relationship to health in various populations is a growing public health priority. 7
Led by Canada, 8 several countries9-11 and the World Health Organization 12 have released 24-hour movement guidelines for children. Building on this paradigm shift, Canada recently released their 24-Hour Movement Guidelines for Adults 18–64 years, 13 continuing the trend toward assessment of movement behaviors within the 24-hour day. Specifically, Canadian 24-Hour Movement Guidelines for Adults include the following recommendations: (1) ≥ 150 minutes of moderate-to-vigorous physical activity (MVPA) per week, (2) several (operationalized as ≥ 3) hours of light-intensity physical activity (LIPA) per day, (3) limiting sedentary time to ≤ 8 hours per day, and (4) 7–9 hours of good-quality sleep nightly. 13 These guidelines have been used as a framework for examining associations between health behaviors and health outcomes in various populations (e.g., stress in adults 14 and body weight in children 15 ).
One understudied population at-risk for chronic disease and long-term health complications are the 40% of college/university students with overweight/obesity in the US. 16 The university years (roughly 18–35 years) are developmentally important; during this time, students can engage in self-exploration and identity formation with generally few responsibilities to others. 17 It has been posited that during this time, health behaviors (e.g., regular physical activity and sleep) may become solidified habits that continue into later adulthood, impacting long-term health. 18 However, less than 50% of college/university students meet US physical activity recommendations and only 25% report getting enough sleep on 5 or more nights per week. 16 Furthermore, disparities in health behaviors exist across demographic characteristics. For example, it is well established that males are more physically active than females at all ages, 19 including university age. 16 These trends are concerning given the independent associations that physical activity, sleep, and weight status each have with increased risk of chronic diseases, particularly among individuals who already have obesity.2-5 Furthermore, obesity is difficult to treat in this population 20 and exhibits strong tracking into later adulthood, 21 making elevated BMI an issue that is important to address early in life prior to adverse changes in health status.
The 24-hour movement paradigm is a useful framework for measuring, synthesizing, and disseminating evidence for relationships among movement behaviors; however, it has not yet been applied to studying the behaviors and health indicators of at-risk university students with overweight/obesity. Understanding whether university student characteristics are associated with meeting specific 24-Hour Movement Guidelines can inform future interventions tailored to promote health behaviors in this population. Therefore, this study aimed to (1) describe 24-hour movement behaviors in a sample of university students with overweight/obesity, (2) determine the percent of university students with overweight/obesity meeting Canadian 24-Hour Movement Guidelines, and (3) test whether meeting 24-Hour Movement Guidelines is associated with student demographic characteristics or BMI.
Methods
Sample
The Healthy Body Healthy U (HBHU) three-arm randomized controlled trial tested the effect of tailored or targeted technology-based weight loss interventions vs contact control. 22 Eligibility criteria included individuals ages 18 to 35, body mass index (BMI) of 25–45 kg/m2, enrolled in a university in the greater Washington, DC, or Boston areas, regular Facebook user, fluent in English, and access to regular text messaging. Exclusions included major medical conditions and current participation in other weight loss or physical activity programs. See Napolitano et al. 22 for full inclusion/exclusion criteria. The HBHU trial enrolled 459 students. Baseline data were collected between May 2015 and January 2018. Participants were included in this secondary cross-sectional analysis if they had baseline data for accelerometer-measured physical activity (n = 408), self-reported sleep duration (n = 453), researcher-measured height/weight (n = 459), and demographic characteristics (n = 459), resulting in an analytic sample size of n = 403 participants.
Measures
Physical activity. Physical activities (i.e., moderate-to-vigorous physical activity [MVPA], low-intensity physical activity [LIPA], and sedentary time) were objectively measured at baseline via 1 week of ActiGraph accelerometer wear-time. Participants wore an ActiGraph (wGT3X-BT) for at least 4 days of 10 or more hours. Due to variability in days of accelerometer wear data, weekly MVPA, LIPA, and sedentary time were calculated as the daily average multiplied by 7. See Napolitano et al. for more details. 22
Sleep. Self-reported sleep duration was assessed using one question from the Medical Outcomes Study (MOS) Sleep Scale. 23 Participants responded to the following prompt: “On the average, how many hours did you sleep each night during the past 4 weeks?”
Demographics. Baseline demographics collected from participants included age, sex, and race/ethnicity (i.e., Black, non-Hispanic White, Asian/Pacific Islander, Hispanic, and multi-racial/other).
Body mass index. Participants’ height (to the nearest .1 cm) and weight (to the nearest .2 kg) were measured by study staff in duplicate using a standard portable stadiometer and a digital scale (Seca Model 769). Participants were asked to remove bulky outerwear and shoes prior to measurement. Average values were used to calculate BMI (kg/m2).
Statistical Analyses
Descriptive statistics were generated to describe average physical activity and sleep behaviors, as well as the number of participants meeting each 24-Hour Movement Guideline. T-tests and ANOVA were used to determine differences in student physical activity and sleep behaviors by demographics (age, sex, BMI, and race/ethnicity), as well as differences in BMI and race/ethnicity among those meeting vs not meeting each guideline. Fisher’s exact tests were employed where the number of observations per cell was 10 or fewer. RStudio 24 Version 1.3.1056 was used for all statistical tests; a significance level of < .05 was determined a priori.
Results
The final analytic sample included n = 403 participants with baseline ActiGraph and self-reported sleep. On average, participants engaged in 311.33 (166.73) minutes of MVPA per week, 3.66 (1.02) hours of LIPA per day, 9.16 (1.27) hours of sedentary time per day, and 6.81 (1.24) hours of sleep per night. In terms of meeting guidelines, 341 participants (85%) met the MVPA guideline, 284 (70%) met the LIPA guideline, 62 (15%) met the sedentary time guideline, and 236 (59%) met the sleep guideline. Further, 185 (46%) met any 2 guidelines, 118 (29%) met any 3 guidelines, and 34 (8%) met all 4 guidelines (see Table 1).
Descriptive statistics for the full sample (N = 403).
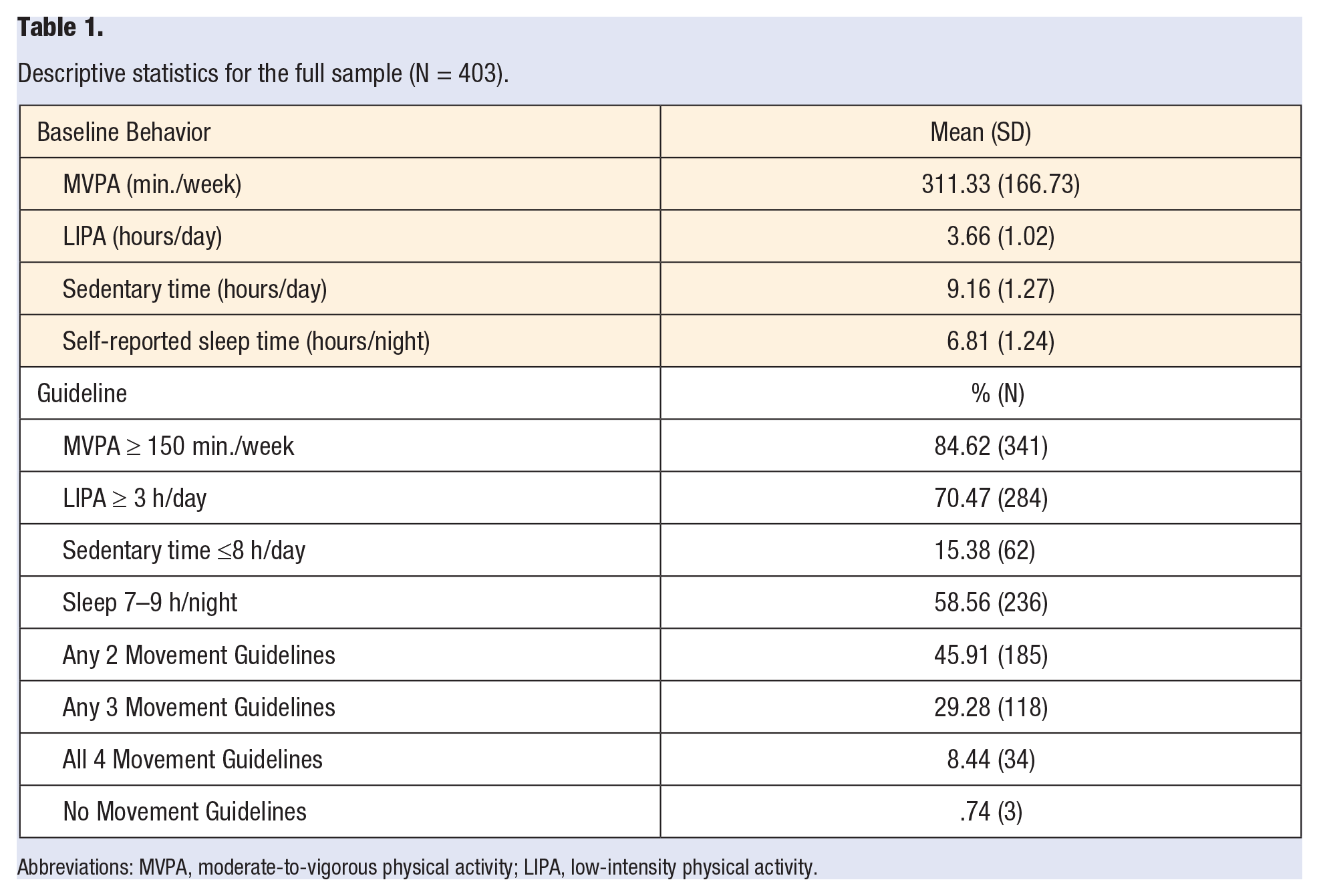
Abbreviations: MVPA, moderate-to-vigorous physical activity; LIPA, low-intensity physical activity.
24-Hour Movement Behaviors
University students ages 18–25 years exhibited fewer sedentary hours per day compared to students ages 26–35 years (9.08 [1.31] vs 9.36 [1.13], P = .037). Differences in MVPA were identified by sex and BMI, with males reporting more MVPA per week than females (363.00 [170.36] vs 297.11 [163.14], P = .002), and individuals with overweight reporting more MVPA per week than individuals with obesity (337.78 [181.14] vs 285.28 [147.05], P = .002). Finally, students with overweight exhibited fewer hours per day of LIPA compared to students with obesity (3.53 [.99] vs 3.78 [1.04], P = .012) (see Table 2). Differences in sleep duration were found by race/ethnicity with African American/Black students reporting the shortest sleep duration (P = .025) (see Table 3).
Behaviors among the sample by age category, sex, and BMI status.
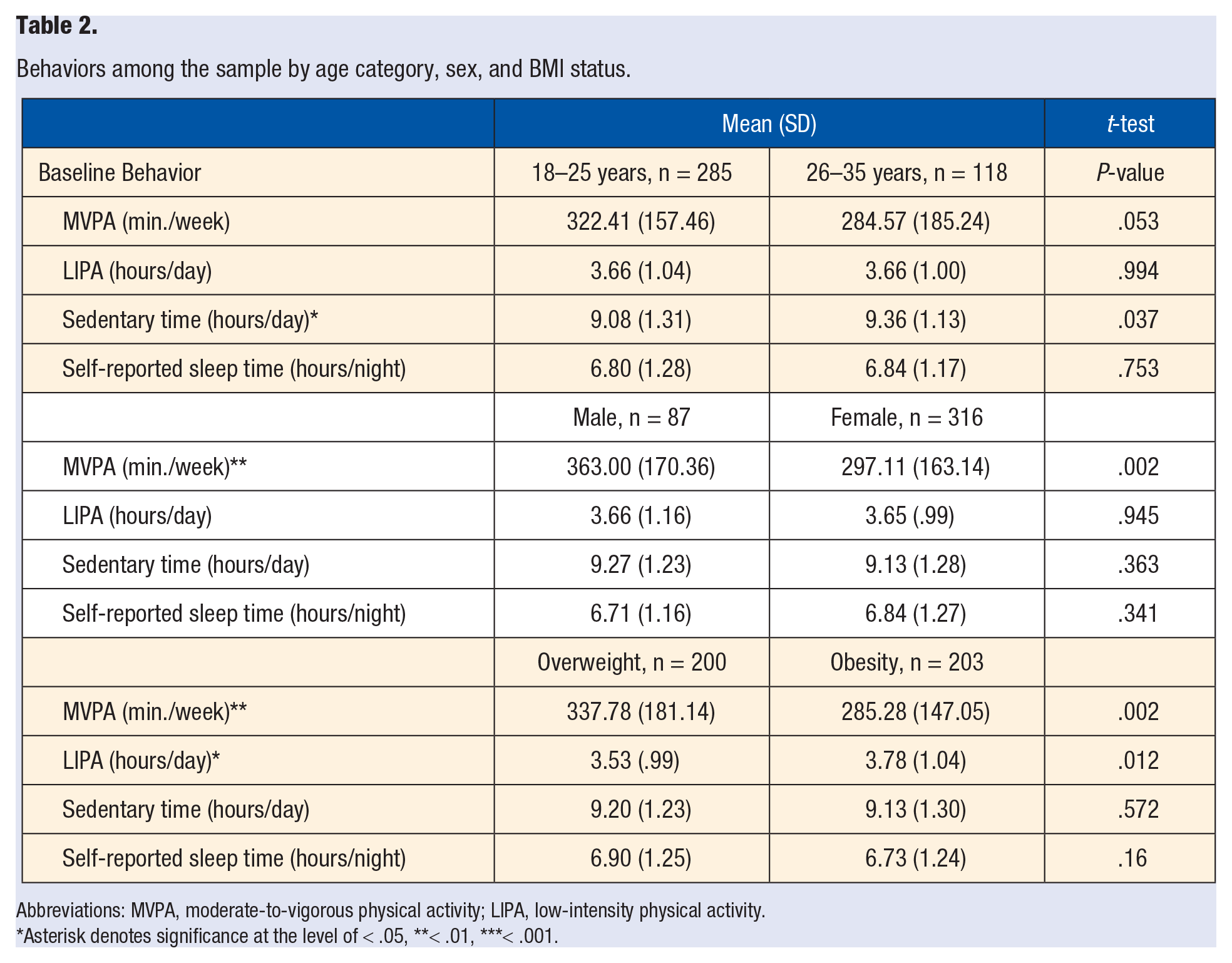
Abbreviations: MVPA, moderate-to-vigorous physical activity; LIPA, low-intensity physical activity.
Asterisk denotes significance at the level of < .05, **< .01, ***< .001.
Behaviors among the sample by race/ethnicity.
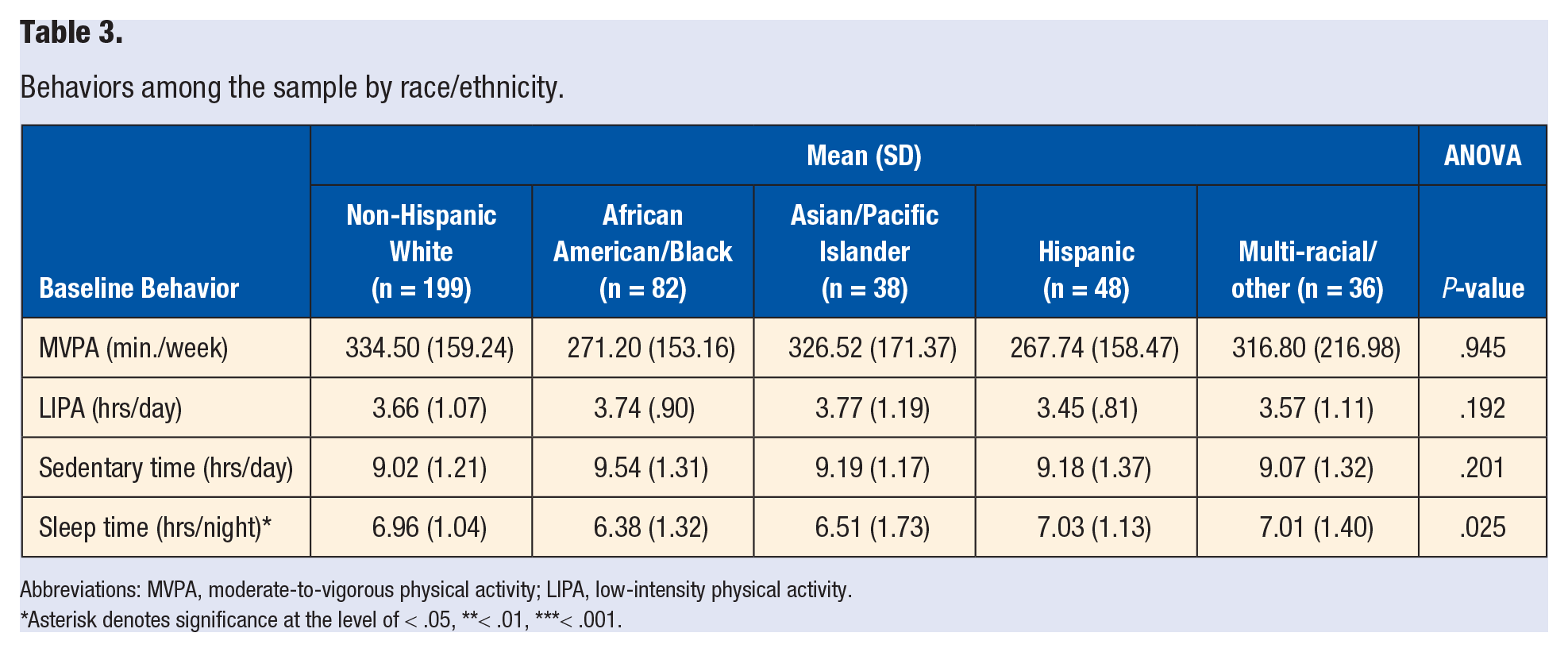
Abbreviations: MVPA, moderate-to-vigorous physical activity; LIPA, low-intensity physical activity.
Asterisk denotes significance at the level of < .05, **< .01, ***< .001.
Guidelines and Demographic Characteristics
There were no differences in the percent of individuals meeting guidelines by age category (18–25 vs 26–35 years). Similar to the continuous variable results above, a significantly greater percentage of males vs females (94% vs 82%, P = .005) and students with overweight vs obesity (89% vs 80%, P = .015) met the MVPA guideline (see Table 4). Additionally, the percentage of individuals meeting the sleep guideline was significantly different across racial/ethnic groups, with African American/Black students reporting the lowest percent (Non-Hispanic White: 64%, African American/Black: 41%, Asian/Pacific Islander: 50%, Hispanic: 67%, Multi-racial/other: 64%, P = .039). African American/Black participants also reported the lowest percent meeting all 4 guidelines (Non-Hispanic White: 12%, African American/Black: 0%, Asian/Pacific Islander: 3%, Hispanic: 10%, Multi-racial/other: 1%, P = .001) (see Table 5).
Associations between meeting 24-Hour Movement Guidelines with age category, sex, and BMI status at baseline.
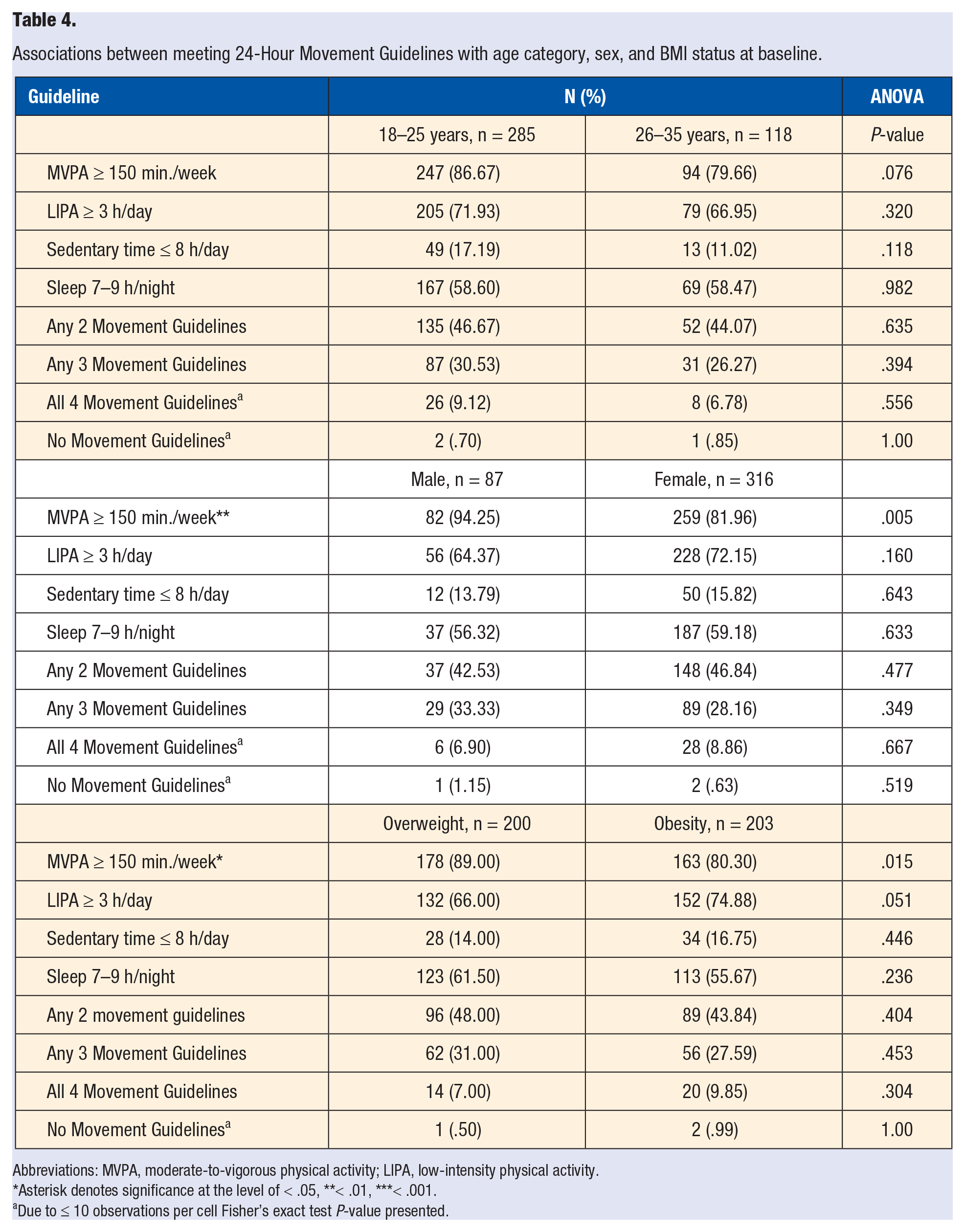
Abbreviations: MVPA, moderate-to-vigorous physical activity; LIPA, low-intensity physical activity.
Asterisk denotes significance at the level of < .05, **< .01, ***< .001.
Due to ≤ 10 observations per cell Fisher’s exact test P-value presented.
Associations between meeting 24-Hour Movement Guidelines and race/ethnicity at baseline.
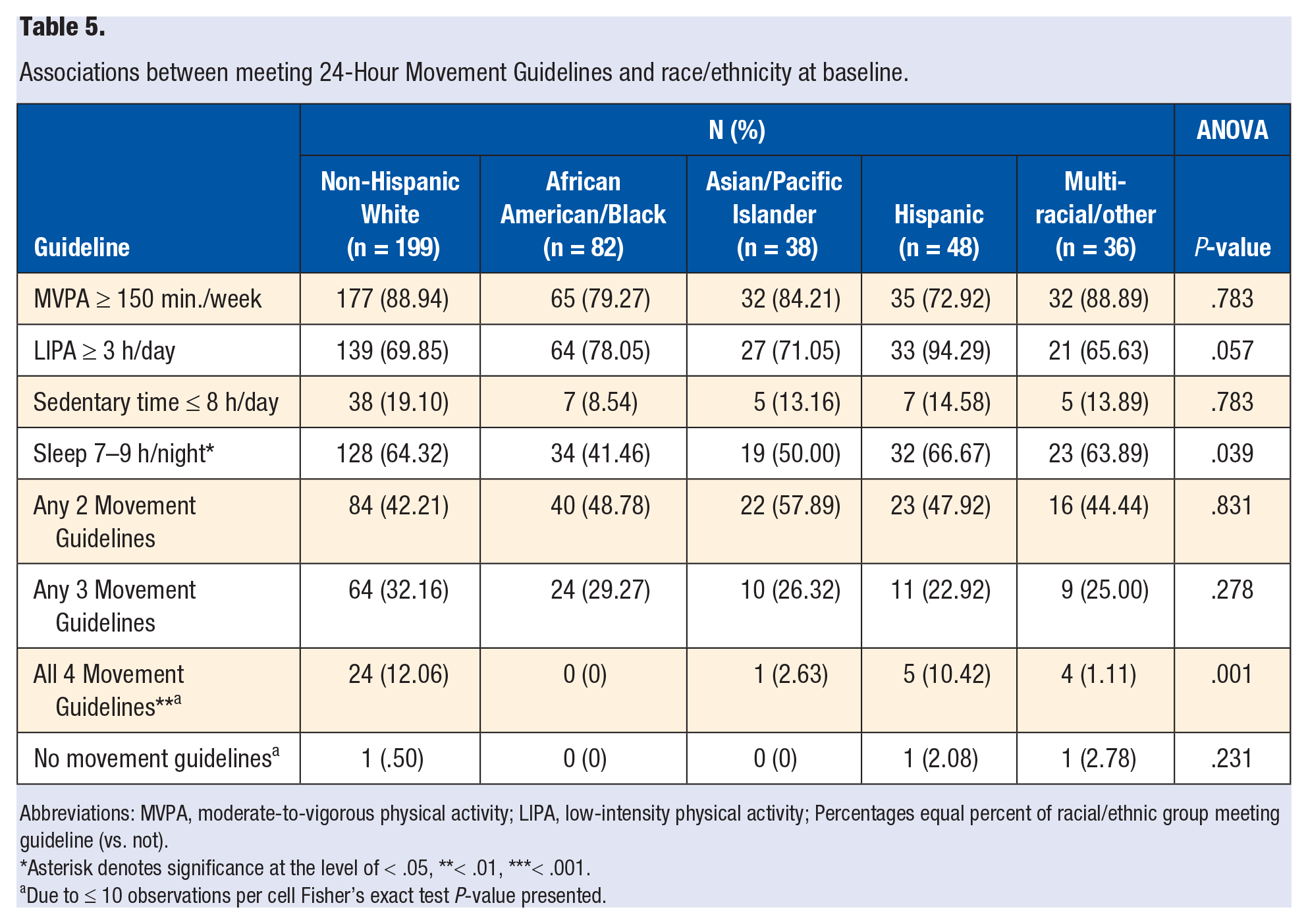
Abbreviations: MVPA, moderate-to-vigorous physical activity; LIPA, low-intensity physical activity; Percentages equal percent of racial/ethnic group meeting guideline (vs. not).
Asterisk denotes significance at the level of < .05, **< .01, ***< .001.
Due to ≤ 10 observations per cell Fisher’s exact test P-value presented.
Guidelines and BMI
Students meeting the MVPA guideline had significantly lower BMIs compared to those not meeting the MVPA guideline (30.83 [4.31] vs 32.50 [4.45], P = .008). Similarly, students meeting the sleep guideline had significantly lower BMIs compared to those not meeting the sleep guideline (30.71 [4.36] vs 31.63 [4.33], P = .038). Finally, students meeting the LIPA guideline had significantly higher BMIs compared to those not meeting the LIPA guideline (31.37 [4.31] vs 30.41 [4.44], P = .047) (see Table 6).
Associations between meeting 24-Hour Movement Guidelines and BMI at baseline.
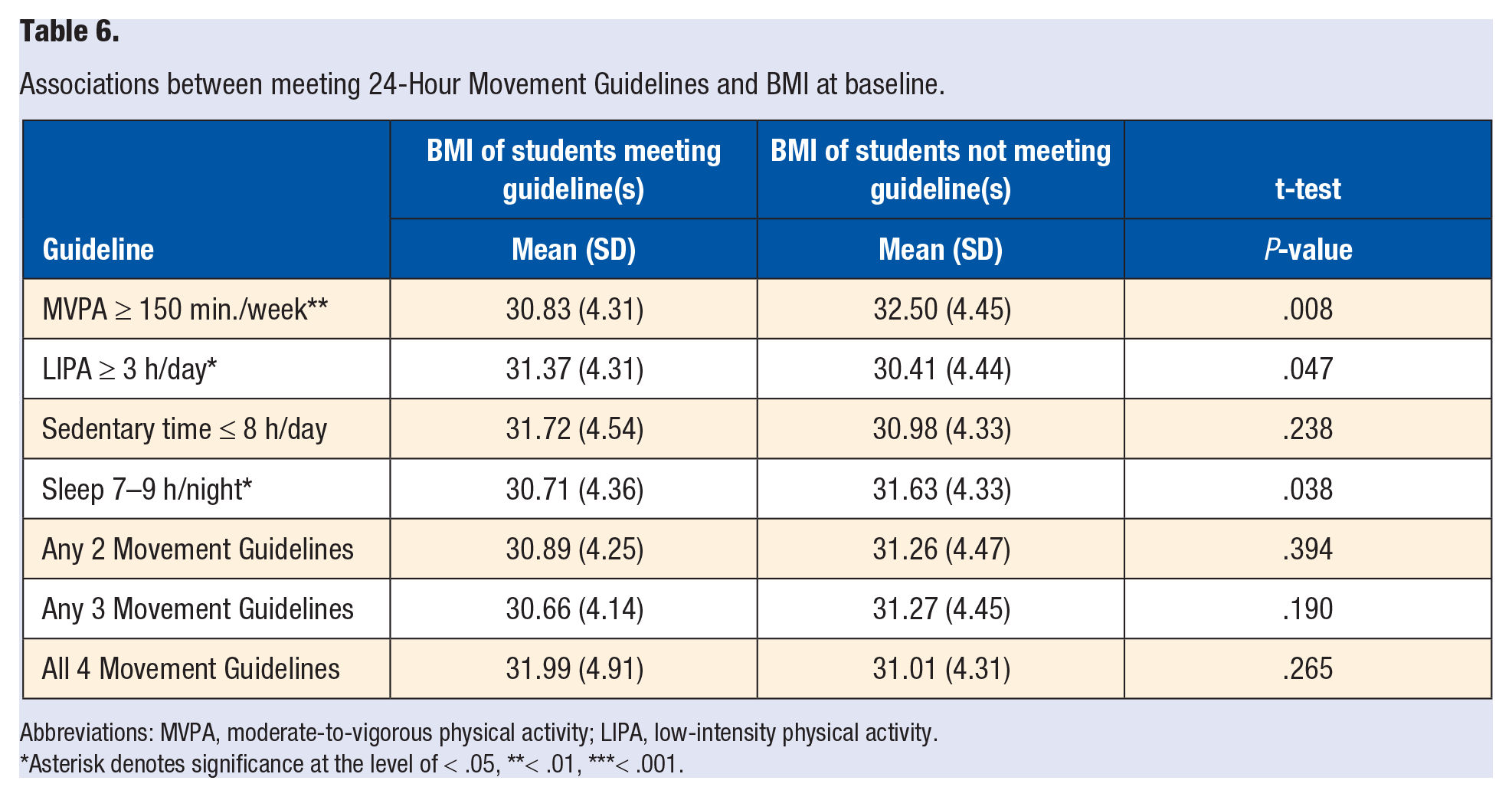
Abbreviations: MVPA, moderate-to-vigorous physical activity; LIPA, low-intensity physical activity.
Asterisk denotes significance at the level of < .05, **< .01, ***< .001.
Discussion
In our sample, the majority of university students with overweight/obesity met MVPA (85%), LIPA (70%), and sleep guidelines (59%), while few (15%) met the sedentary time guideline. Older students (26–35 years) exhibited significantly more sedentary hours per day compared to younger students (18–25 years) (9.36 [1.13] vs 9.08 [1.31], P < .05), indicating that older students with overweight/obesity are more likely to experience excessive sedentary behavior and related health concerns. Additionally, fewer than 50% of all students met two or more guidelines and very few (< 10%) met all 4.
Males and students with overweight reported more weekly MVPA than females (363 [170] vs 297 [163], P < .01) and students with obesity (338 [181] vs 285 [147], P < .01), respectively. Males (94% vs 82%, P < .01) and students with overweight (89% vs 80%, P < .05) were also significantly more likely to meet the guideline of 150 minutes or more of MVPA per week. This is in line with previous research which has reported that female college/university students and those with obesity are less likely to meet guidelines compared to male and overweight counterparts, even on university campuses with curricular policies designed to promote student physical activity. 25 Interestingly, students with obesity recorded significantly more hours per day of LIPA compared to students with overweight (3.78 [1.04] vs 3.53 [.99], P < .05). This may indicate that individuals with obesity replace what would otherwise be MVPA time with LIPA. Future studies can examine students’ perceptions in relation to 24-hour movement behaviors to elucidate whether differences in LIPA among students of varying BMIs is related to their perceived level of activity and/or exertion. The exchange of movement behaviors within a 24-hour day is of growing interest to behavioral scientists, 6 and our results highlight the need to explore such questions in relation to BMI and other indicators of health risk.
When examining behaviors by racial/ethnic status, African American/Black students reported the shortest sleep durations, with an average of 6.38 hours. Furthermore, only 41% of African American/Black students met the sleep guideline, compared to 50% or greater for all other racial/ethnic groups (P < .05). African American/Black participants were also least likely to meet all 4 guidelines (0%), followed closely by multi-racial/other (1.1%), and Asian/Pacific Islanders (2.6%, P < .01). Racial/ethnic sleep disparities have been previously reported in adults: specifically, shorter sleep duration and lower sleep efficiency has been described among African Americans in comparison to White/European Americans, and these disparities explain 41–58% of racial differences in cardiometabolic disease risk. 26 Additionally, Black adolescents have reported significantly shorter school night sleep durations and more social jetlag (discrepancy between biological rhythms and sleep/wake behaviors) compared to White or Hispanic peers, 27 and social jetlag is a known risk factor for cardiometabolic disease risk. 28 Taken together, these results suggest that lack of sleep may be a key contributor to disease risk among already at-risk university students and that culturally tailored sleep promotion programs are needed on college campuses to address sleep and health disparities.
Finally, we found an association between three 24-Hour Movement Guidelines and student BMI. First, meeting MVPA or sleep guidelines was associated with lower student BMI, indicating that these behaviors are important targets for weight management programs. Furthermore, meeting the LIPA guideline was associated with higher student BMI, indicating that students with obesity may replace MVPA time with LIPA. Interventions aiming to promote physical activity and/or sleep on college/university campuses may benefit from tailoring such interventions according to the demographic differences identified in this sample: MVPA disparities exist by sex and weight status, and sleep/overall movement guideline disparities exist by racial/ethnic status. Our findings may be particularly useful given that weight management interventions among university students report more success among students with overweight vs obesity. 20 Sleep, in particular, may be an important missing behavioral component to address when providing weight loss/maintenance guidance to college students and merits future research.
Our findings support the importance of promoting 24-hour movement behaviors among university students with overweight/obesity. Future work should explore university students’ awareness of 24-hour movement guidelines, as well as demographically tailored interventions to promote these 4 movement behaviors. In particular, African American/Black students may be at increased risk for short sleep durations, social jetlag, and other sleep disruptions that ultimately impact health, indicating need for targeted interventions. Finally, researchers should consider the time of day that 24-hour movement behaviors occur within a 24-hour day to uncover how timing may affect health.29,30 Objective measurement tools, such as accelerometers, and self-report tools, such as the National Cancer Institute’s ACT-24, 31 are growing in popularity and availability, allowing researchers to test ever more granular questions regarding relationships between time of day of health behaviors and health outcomes.
Limitations
Limitations of this work include the cross-sectional design. Future studies should build upon these analyses by testing associations between meeting 24-Hour Movement Guidelines and BMI over time to discern whether meeting specific guidelines may have a causal influence upon BMI. The present sample includes only individuals with overweight/obesity and may not be representative of college/university students more broadly. Finally, although physical activity behaviors were measured objectively via accelerometer, sleep duration was based on a self-report measure. Future investigations should consider objective assessment of sleep, such as accelerometer algorithms designed to differentiate sleep from sedentary behavior.
Conclusion
Among university students with overweight/obesity, lower BMI was associated with meeting MVPA and sleep guidelines. Females and students with obesity were less likely to meet the MVPA guideline compared to males and students with overweight, respectively. African American/Black students were least likely to meet the sleep guideline, and all 4 guidelines, compared to other racial/ethnic groups. Results indicate that demographically tailored interventions may help promote MVPA, sleep, and weight management among students with overweight/obesity. Future research is needed to test these associations longitudinally.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by National Institute of Diabetes and Digestive and Kidney Diseases (R01DK100916).