
Abstract
Background: The underlying causes of gestational diabetes mellitus (GDM) are important because they are effective for the diagnosis and prevention of this condition. The aim of this study was to identify the risk factors for GDM and the possible etiological agents. Materials and Methods: This case-control study was conducted with 100 women with GDM and 100 healthy pregnant women at a tertiary care hospital, affiliated to Babol University. GDM was identified by impaired oral glucose tolerance test based on the Carpenter and Coustan criteria. Healthy women were randomly selected from the prenatal health care clinic of the same center and were matched to gestational age of 24 to 28 weeks. Descriptive and inferential statistics were used for data analysis via the SPSS software. Results: After adjusting variables, multivariate analysis identified 4 significant risk factors of GDM, including prepregnancy low physical activity (odds ratio [OR] = 2.85, 95% confidence interval [CI]= 0.97-8.34), advanced maternal age (OR = 1.24, 95% CI = 1.13-1.35), body mass index ⩾ 30 kg/m2 (OR = 1.10, 95% CI = 1.02-1.20), and family history of diabetes mellitus (OR = 5.62, 95% CI = 2.26-13.96). Conclusion: We observed significant associations between low prepregnancy physical activity and obesity with GDM risk. Thus the finding of this study can help devise strategies for the prevention of GDM.
‘Hyperglycemia has many consequences in pregnancy and is estimated to influence approximately 16.9% of all pregnancies.’
Gestational diabetes mellitus (GDM) is defined as “carbohydrate intolerance resulting in hyperglycaemia of variable severity with onset or first recognition during pregnancy.” 1 The prevalence of GDM has been reported to be 1% to 20% using various diagnostic methods and indicates a rising trend in recent years. 2
The Asia-Pacific region has the largest number of individuals with GDM. Because Asian populations are more prone to abdominal obesity and low muscle mass with increased insulin resistance compared with their Western counterparts, 3 the Asia-Pacific region has the highest prevalence of GDM. Iran is also a part of Asia. The Middle Eastern (Syrian, Lebanese, Iraqi, Iranian, and Afghanistan) women are the major at-risk groups for GDM. 4 According to systematic review and meta-analysis study in Iran, prevalence of GDM is relatively high, which might be attributed to different factors. 5 The prevalence of gestational diabetes in Tehran is 6.9%. 6 The prevalence of GDM depends on the study population and use of different diagnostic criteria. 7
Hyperglycemia has many consequences in pregnancy and is estimated to influence approximately 16.9% of all pregnancies. The highest prevalence is in the Southeast Asia, where 1 in 7 births is affected by GDM. 8 GDM is associated with some short- and long-term health-related consequences for both women and their children. 9 The clinical recognition of GDM is important, because it often requires diet therapy and drug therapy, such as insulin and antepartum fetal surveillances, to reduce GDM-associated perinatal morbidity and mortality. Hyperglycemia during pregnancy is commonly identified with the oral glucose tolerance test (OGTT). Screening by the use of OGTT is recommended in pregnancy for high-risk woman at their initial prenatal visit and for all pregnant women between the 24th and 28th weeks of pregnancy. 10
The risk factors of GDM are obesity, physical inactivity, 2 advanced maternal age, 8 multiparous, family history of type 2 diabetes mellitus, and certain ethnicities, including Asians, 11 a previous macrocosmic child, GDM in the previous pregnancy, 10 and polycystic ovarian syndrome. 12 These factors increase the risk of GDM among pregnant women.
A sedentary lifestyle is the fourth most important risk factor of mortality in the world. 13 Physical inactivity is a risk factor for a noncommunicable disease and influences women’s overall health.14,15 The International Physical Activity Questionnaire (IPAQ) was administered to allow classifying of pregnant women as active and inactive. The cutoff point of 450 METs (metabolic equivalents) is defined from the multiplication of the minimum consumption of 3 METs of moderate physical activity for 150 minutes weekly that a pregnant woman must meet to be physically active. 16 Physical activity is a reliable strategy to bring about positive changes in human health. Studies have found that physical activity provides major health-related benefits such as improvements in cognitive, 17 cardiovascular, 18 respiratory, 19 and muscle functions 20 and reduces the incidence and severity of type 2 diabetes mellitus and GDM. 21
Since GDM represents a major threat to public health, international health organizations have emphasized the necessity of devising national plans to improve the quality of care. However, the continuous monitoring of the indicators of quality of care remains a challenge in many countries. 22 A meta-analysis of randomized controlled trials on prenatal physical activity showed that physical activity during pregnancy provided a 28% lower risk of GDM compared with those in a control group (relative risk [RR] 0.72, 95% confidence interval [CI 0.58-0.91]. 13 GDM prevention interventions that are started during pregnancy may have less efficacy due to less intensity with concerns about its effects on the fetal growth and biological changes such as craving, nausea, edema, and weight gain in pregnancy as barriers to physical activity and short duration of interventions prior to the diagnosis of GDM. Notably, limited literature, variability in interventions, and lack of adherence to interventions by samples 23 have reduced the generalizability of the findings of previous studies. Therefore, the aim of this study was to identify the risk factors for GDM and the possible etiological agents.
Materials and Methods
This case-control study was performed at Rohani Hospital, a tertiary care hospital affiliated with Babol University, set in the north of Iran from September 2013 to February 2015. This study was carried out on 100 pregnant women with a definite diagnosis of gestational diabetes as a case group and 100 healthy pregnant women as a control group of similar gestational age were selected from the same hospital.
Exclusion criteria included prepregnancy diabetes (type 1 or type 2 or both types of diabetes); recurrent miscarriages; child with congenital abnormalities or neonatal mortality in previous pregnancies; smoking before and during pregnancy; multiple gestation; known chronic illnesses such as hypertension, chronic renal diseases, collagen or vascular diseases, endocrine disorders, chronic hepatic diseases; and current use of corticosteroids. Inclusion criteria for the recruitment of the women were age 18 to 40 years, pregnancy at the gestation age of 24 to 28 weeks, and willingness to take part in this study.
Recruitment
The diagnosis of GDM was made using a 2-step approach. All pregnant women who visit a midwifery clinic for prenatal care are routinely screened for GDM by 50-g 1-hour glucose challenge test (GCT) at 24 to 28 weeks of gestation. The control group consisted of those who had normal GCT. An OGTT was performed on the subset of females whose plasma glucose concentrations exceeded the glucose threshold value (140 mg/dL). The diagnostic criteria for GDM were the Carpenter and Coustan conversion as recommended by the American Diabetes Association. The Carpenter and Coustan’s criteria are as follow: fasting blood glucose 95 mg/dL, 1-hour blood glocuse180 mg/dL, 2-hour blood glucose 155 mg/dL, and 3-hour blood glucose 140 mg/dL. 24
Fasting blood glucose was tested after 12 to 14 hours of fasting. If the pregnant women had a positive GCT test and 2 or more abnormal OGTT readings, they were diagnosed with GDM. The women with an abnormal GCT but a normal OGTT and the women with a single abnormal OGTT were excluded from the study. The laboratory tests were performed at the Rohani hospital laboratory. Measurements were made by using the glucose oxidase method via the Hitachi 704 auto-analyzer.
The women with GDM were enrolled in the study and received required care for the management of GDM. However, the sampling was performed by a trained midwife and continued till the required sample size was reached. The informed written consent form was signed by the participants before starting the study. Ethical approval was obtained from the Ethics Review Committee of Faculty of Medicine, Babol University of Medical Sciences, Iran (project number 746- 8930216).
Data Collection
Anthropometric characteristics, including weight, were measured with the least amount of clothes to the nearest 100 g. Height was measured using a tape measure in the standing position with shoulders in a normal alignment. Prepregnancy body mass index (BMI) was calculated using reported height and pre-pregnancy weight and categorized according to standard cutoffs (underweight <18.5 kg/m2, normal 18.5-24.9 kg/m2, overweight 25-29.9 kg/m2, obese ⩾30 kg/m2). 21 Gestational age was calculated based on the first day of the last menstrual cycle (LMP) for the women with regular menstrual cycles. Also, transabdominal ultrasonography was used for those women with irregular menstrual cycles or those who did not remember their LMP. The family history of diabetes mellitus was defined as the history of type 2 diabetes among the first-degree family members.
Physical activity in the 3 months before pregnancy was assessed at the time of enrollment, from 20th to 28th week of gestation by using the IPAQ. The IPAQ evaluated the women’s participation in 4 domains of activities, including “household/caregiving,” “occupational,” “sports/exercise,” and “transportation.” The frequency, intensity, type, and duration of physical activities were calculated in various domains. 23 The physical activity level scores were assessed to determine whether the woman had a sedentary, moderate, or a vigorously active lifestyle. The IPAQ was modified and validated by a sample of Iranian young individuals. The process of translation and cultural adaptation of the IPAQ was performed in studies by Kelishadi et al. 14 The internal consistency of this questionnaire, using the calculation of Cronbach’s alpha coefficient for the scale, was reported as .7 indicating a satisfactory internal consistency. 13 Prepregnancy physical activity was derived from total MET values. It was estimated for various activities with values 3.3, 4, and 8 for walking, moderate activity, and vigorous activity, respectively, and was categorized as sedentary/low (<600 MET min/wk), moderate (600 to <3000 MET min/wk), and high (3000 MET min/wk). 23
Statistical Analysis
The study’s sample was determined to be 200 women including both the cases and control subjects, based on variables, including 95% confidence interval, 80% power, and 15% difference between the women with GDM and healthy women. The collected data were analyzed using the descriptive mean ± SD, number and percentage, and inferential statistics. The baseline and follow-up characteristics of the women were compared between the GDM and non-GDM groups using the Student’s t test or chi-square test. The logistic regression model was used to assess the association (odds ratio [OR]) between covariates age, prepregnancy physical activity, BMI, family history of diabetes, and GDM.
The data analysis was performed using the SPSS 23.0 software for Windows (IBM Corp, Armonk, NY, USA). The significance level was set at P < .05.
Results
The samples consisted of 100 women with GDM and 100 healthy women. The sociodemographic characteristics of the women are shown in Table 1. No differences were reported in the proportion of illiterate individuals between the groups. Similarly, the women with GDM and the healthy women had almost the same proportion of illiterate husbands. No statistically significant difference was found in the occupation status between the women.
The Sociodemographic and Fertility Characteristics of the Women With Gestational Diabetes Mellitus (GDM) and Healthy Women (N = 200).
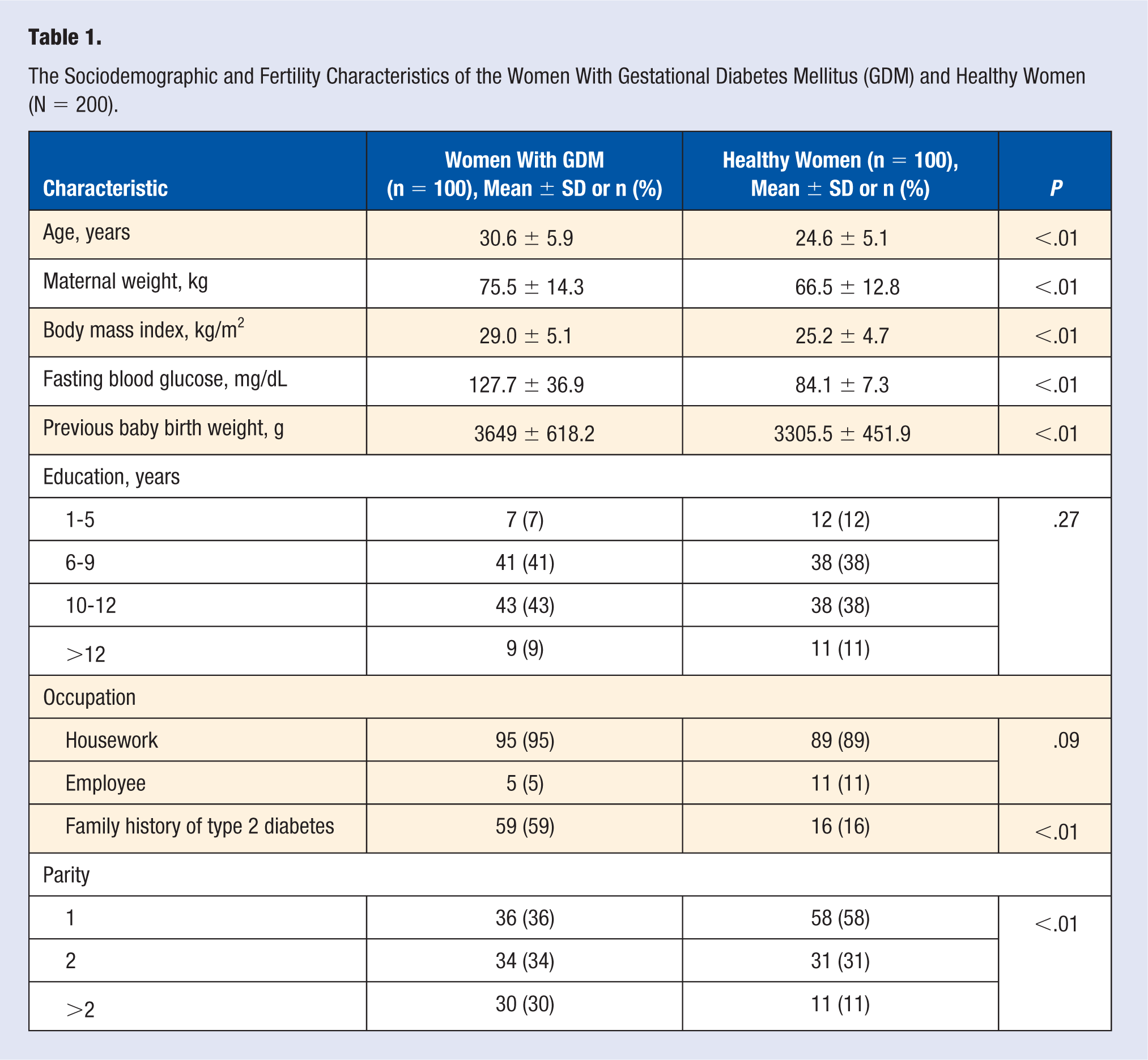
Statistically significant differences were reported between the women with GDM and the healthy women in terms of age, prepregnancy BMI, parity, and family history of diabetes. The physical activity characteristics of the pregnant women is shown in Table 2.
The Mean Prepregnancy Physical Activity in the Women With GDM and Healthy Women.
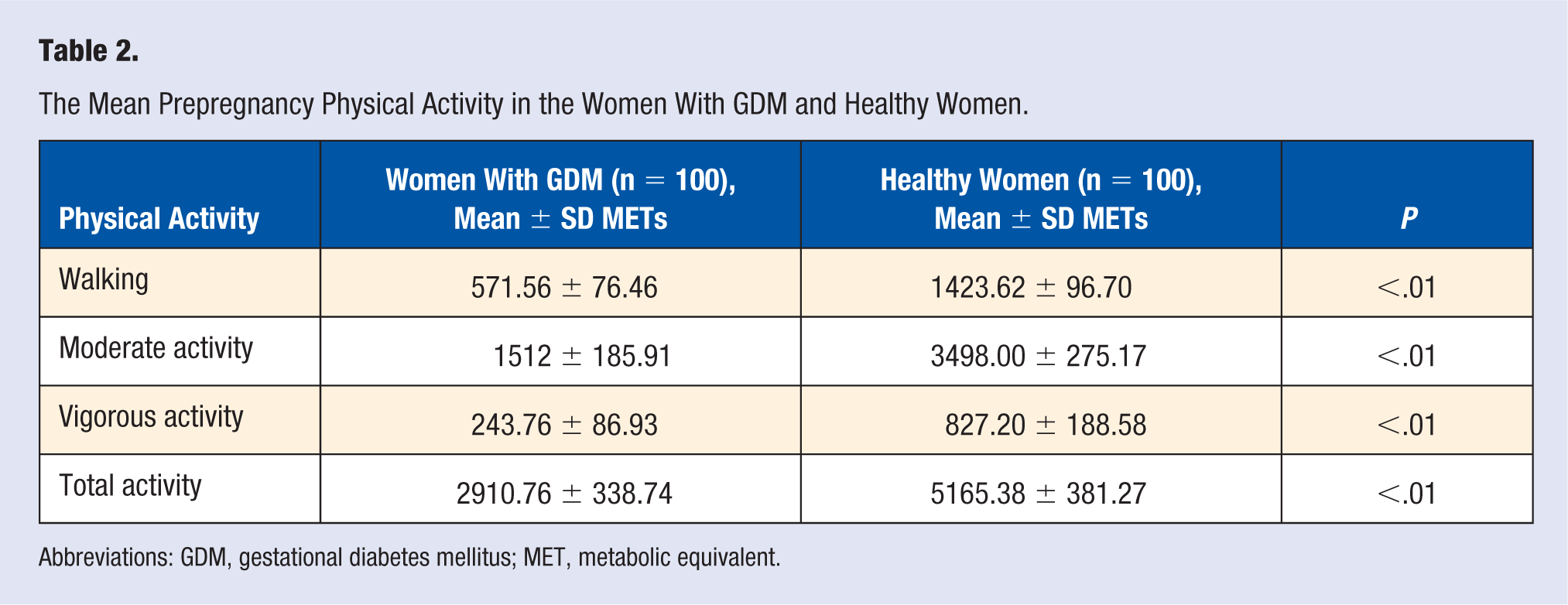
Abbreviations: GDM, gestational diabetes mellitus; MET, metabolic equivalent.
Physical activity for out-of-home work was performed by only 5 women, which did not enter statistical analysis. Total physical activity in the 3 months before pregnancy among women with GDM was significantly lower than among healthy pregnant women (P < .000).
The logistic regression model was used to determine the severity of the relationship between maternal physical activity before pregnancy and GDM. After entering confounding factors such as age, BMI, the family history of diabetes, and parity in the logistic regression model, the number of parity, vigorous physical activity, and walking were excluded from the model, and the rest of the variables remained in the model. The crude and adjusted ORs for GDM are shown in Table 3.
Logistic Regression Model for GDM (N = 200).
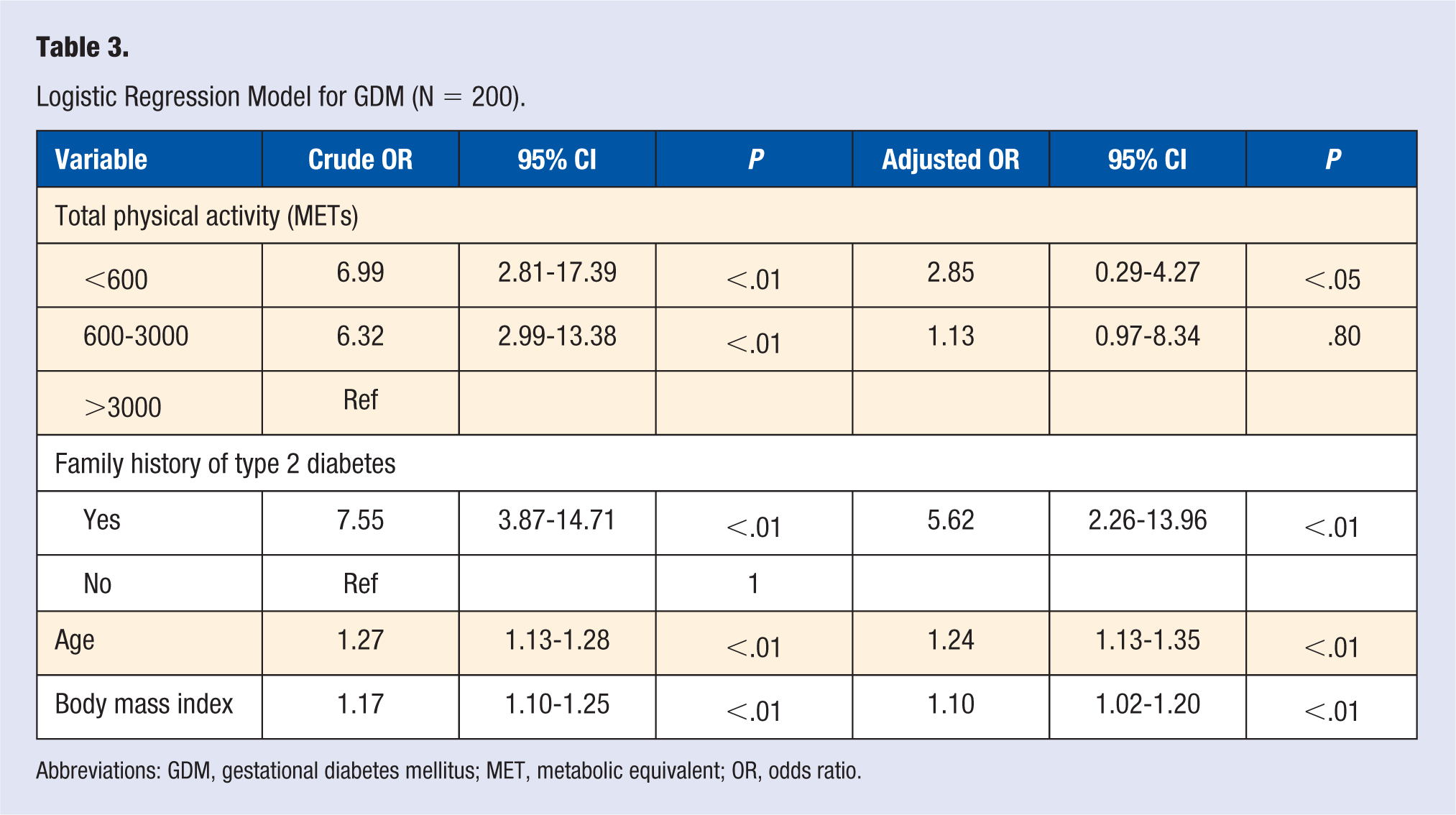
Abbreviations: GDM, gestational diabetes mellitus; MET, metabolic equivalent; OR, odds ratio.
Discussion
This study was conducted to clarify the importance of risk factors for GDM in a study of 100 women with GDM and 100 healthy women. In our study, family history of diabetes mellitus, low physical activity in the 3 months before pregnancy, advanced maternal age, and obesity were significant risk factors of GDM. In the study by Teh et al, 11 the advanced age of the mother was the most important risk factor of GDM, but in this study family history of type 2 diabetes is the most important factor.
In a systematic review and meta-analysis study in Iran, the potential causes of GDM were gestational age, history of gestational diabetes, family history of diabetes, high BMI, abortions, parity, and history of macrosomia. 5 In this study, women in both groups had gestational age between 24 and 28 weeks. Based on the initial univariate analysis, the rate of parity and history of macrosomia was significantly higher among women with GDM. However, after controlling for potential confounders, factors were not the independent factor of GDM. Low physical activity (<600 MET) during prepregnancy tripled the risk of GDM. This held true after the adjustment of a number of possible confounders. This was consistent with the findings of previous studies.22,25,26 Similarly to this study, a systematic review and meta-analysis study by Tobias et al 22 showed that the total physical activity before pregnancy and during early pregnancy was significantly associated with a lower risk of GDM. The value of this association was greatest for prepregnancy physical activity as the women with the highest physical activity experienced a 55% reduction in the risk compared with women with the lowest physical activity. According to Shirazian et al, 27 the increase of age >30 years, BMI >30 kg/m2, and family history of diabetes were independent risk factors of GDM. In this study, the increased prepregnancy BMI, maternal age, and family history of diabetes were independent predictors of developing GDM. Low physical activity during prepregnancy increased the risk of developing GDM (OR = 2.8(. The prevalence of GDM is increasing worldwide in parallel with maternal obesity, sedentary life styles, and the increase in the age of pregnant women.15,16,28 A study in Iran showed that the prevalence of GDM was 3.4%; the highest and lowest prevalence rates were 18.6% and 1.3% in Karaj and Ardebil, respectively. 5
While physical activity is important in all stages of life, it is especially important before and during pregnancy, as it can affect the health of women and their children. The maintenance of adequate physical activity during pregnancy depends on prepregnancy habits. Pereira et al 29 showed that decline in physical activity during pregnancy was accompanied by a near doubling in the prevalence of insufficiently active lifestyle, from 12.6% during prepregnancy to 21.6% during pregnancy. For instance, women with a BMI above the normal range are more likely to remain inactive. 30 Regular physical activity is not contraindicated by the disease, provides pregnant women with better overall fitness, improves cardiovascular and muscular performance, prevents excessive weight gain, improves blood pressure, and protects them against GDM. 17 In a meta-analysis study, the relative risks of GDM were 55% lower for women in the highest prepregnancy physical activity quantiles compared with those in the lowest (pooled OR 0.45, 95% CI 0.28-0.75; P = .002). 22 Prepregnancy BMI was associated with the risk of GDM. These findings are consistent with those reported before.18-20,31 Therefore the American College of Obstetricians and Gynecologists recommended performing at least 30 minutes of moderate daily exercise. 17 Clapp et al 32 and Mata et al 33 conducted review studies and concluded that a personalized physical exercise combining neuromuscular and cardiovascular training is highly recommended in pregnant women if pregnancy period is free of medical contraindications and problems. They emphasized that the uterine blood flow was reduced during exercise, but this does not affect the blood flow to the fetus.
Limitations
The main strength of the study is a comparison group, so that we were able to compare outcomes for women without GDM. But our study had limitations which should be addressed in the future work. Race and ethnicity as a risk factor have been stated in the valid scientific references, but in our study has not addressed the effect of this risk factor in GDM. We conducted this study in Mazandaran province in north of Iran, which lacks different ethnicities. Further research should include women within a heterogeneous society with different ethnicities and races. In our study, assessment of physical activity was performed using a questionnaire, self-reports that were prone to recall bias because the women with GDM remembered physical activity differently than controls. Further research also needs to be done to better understand the mechanisms of the apparent benefits of physical activity in prepregnancy and during pregnancy in prevention of GDM.
Conclusion
According to the findings of this study, low amount of physical activity prior to pregnancy, advanced maternal age, obesity, and family history of diabetes mellitus were significant risk factors of GDM. GDM is one of the major health problems in the world that requires effective prevention and control strategies. Therefore, having accurate and reliable information about the causes of GDM is very helpful in planning the prevention of GDM.
Footnotes
Acknowledgements
The authors thank the pregnant women who sincerely participated in this study and helped with the production of this article. The authors also thank the Health Research Institute for Babol University of Medical Sciences, Iran, for the approval of this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Ethics Review Committee of Faculty of Medicine, Babol University of Medical Sciences, Iran (project number 746- 8930216).
Informed Consent
Informed written consent form was signed by the participants before starting the study.
Trial Registration
Not applicable, because this article does not contain any clinical trials.