
Abstract
Introduction: This paper presents a secondary analysis of data from a study of 216 people participating in a trial of program shared medical appointments (PSMA) in weight management. The focus of this paper is the Aboriginal women who participated in this translational research project and who were not reported on specifically in the primary analysis and publication. This paper, therefore, examines the use of PSMA as a culturally safe and responsive procedure to facilitate weight management. Method: Twogroups, totalling 25 Aboriginal women, participated in a 6-session 12-week culturally responsive weight management PSMA. Repeated weight and satisfaction measures at 3, 6 and 12 months were collected. Results: 19 of 25 (76%) Aboriginal women completed the MYU. 16 (84%) lost some weight, and 5 (26%) lost clinically significant weight (> 5%), sustained for 1 year. The participants and providers rated the procedure > 4 on 5-point Likert scales for satisfaction. 95% reported that they preferred MYUs for weight management over 1:1 consultations with their general practitioner. Conclusion: The data indicates that programmed shared medical appointments appear to be a culturally safe and responsive procedure to support the Aboriginal women, in this study, to manage their weight.
Participants and providers received MYUs in weight management well; 84% of completers experienced weight loss, and 26% of these maintained clinically significant weight loss.
Introduction
Shared medical appointments (SMAs, also known as group consultations) are ‘individual medical consultations carried out sequentially in a group of patients with similar concerns, with all listening and contributing’. 1 These have been tested extensively in many countries2-6 and have been adopted as a process in the emerging discipline of lifestyle medicine. 7
Our work with SMAs in primary care centres6,8 has led us to extend this into a form of ‘programmed’ SMA (pSMA), which potentially provides a platform for a range of interventions for chronic diseases and conditions. pSMAs have been defined as ‘a sequence of SMAs in a semi-structured form providing discrete educational input relating to a specific topic’. 9 These allow for a set number of SMAs run in a sequenced ‘active learning’ format coordinated by an SMA facilitator. The SMA facilitator normally is a qualified practice nurse or allied health professional with generic training in conducting SMAs and specific training in the disease topic. The pSMA is generally led by the facilitator but with a doctor providing individual sequential consultations during part of the session and with participation and input of the group.
The authors have undertaken and previously reported, in the Australian Journal of General Practice, on a trial of programmed shared medical appointments, combining data from Aboriginal and non-Aboriginal people in weight management 9 (Southern Cross University HREC. HREC Approval Number = ECN 18-181).
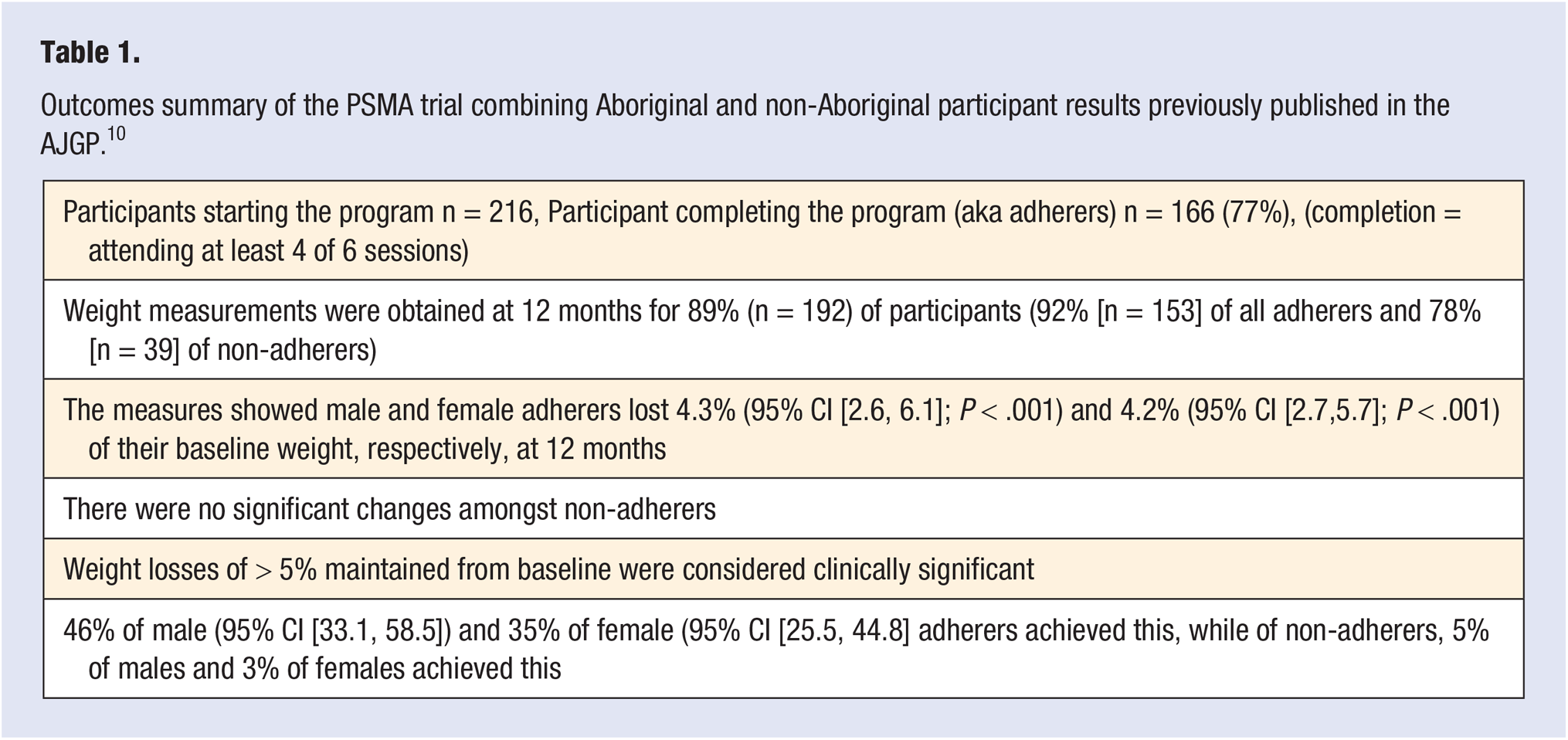
The study found that PSMAs are highly popular amongst both participants and providers with significant; (a) clinical outcomes after 12 months as well as (b) cost- and time-efficiencies, over conventional care. The report showed the findings for all participants (n = 216), combining the results for both Aboriginal and non-Aboriginal peoples’ data, and these are summarised in Table 1.
Outcomes summary of the PSMA trial combining Aboriginal and non-Aboriginal participant results previously published in the AJGP. 10
The programmed shared medical appointments (pSMA) procedure has been renamed by Aboriginal patients as medical yarn ups.10,11 It has been previously theorised that MYUs in weight management would provide a culturally safe and accessible procedure that can help reduce Aboriginal and Torres Strait Islander peoples’ weight by meeting individual patients’ needs in a supportive group setting.10,11
This paper reports on a secondary analysis of data, not previously reported on, obtained specifically from Aboriginal women who participated in the weight management trial previously noted.
The secondary analysis is from data gathered from 2 groups of Aboriginal women who participated in the medical yarn ups program for weight management. Each group was led and coordinated by an Aboriginal medical yarn up–trained facilitator and included individual consultations in the group by their regular general practitioner. The facilitator managed the consultation flow and group dynamics. The facilitator also delivered and added local Aboriginal context to a pre-packaged educational, self-management and behaviour change program in weight management.
Recruitment and Research Process with Aboriginal Women
Participants: The Aboriginal women participants were recruited by GP referral and other staff from Waminda Women’s Health and Welfare Service, located in Nowra and within the South Eastern Primary Health Network of NSW.
Facilitators: 2 facilitators, previously trained in both MYUs for Aboriginal people and in the weight management program, through the Australasian Society of Lifestyle Medicine, were recruited. Only one facilitator was engaged for both groups (the other was on stand-by for back up contingencies and capacity building for the Centre).
Doctor: The participating GP was already working with Waminda but had no specific background in MYUs or weight management. Evidence and experience suggest 5 that whilst it may be beneficial for GPs to attend facilitator and weight management training, this is not essential, as the doctor in a MYU (and other shared medical appointment contexts) ultimately conducts a standard medical consultation.
Program content: The program was designed as an active learning initiative based around evidence-based weight loss information and activities. The program was appropriately ‘Indigenised’ by the facilitator. That is, the facilitator demystified and interpreted some of the medical language and concepts to be more culturally safe and responsive. The full outline of the program, its processes and resources can be found at www.lifestylemedicineprograms.com.
Program structure: The program was conducted over 6 sessions, 2 weeks apart. Each session, lasted 90–120 minutes. The first 20–40 minutes was spent with the facilitator presenting the pre-prepared 10- to 12-minute audio-visual presentation and encouraging discussion on the topic for the session. The GP then joined the MYU for up to 1 hour, and conducted individual, sequential consultations in the presence of the others. A further 10–15 minutes was taken up at the end with the facilitator summing up and answering questions.
Participants were provided a program handbook which helped them set goals and reflect on behaviour. They were also provided access to the audio-visual presentations and other resources for their own review and ongoing learning.
Measures
Participant and provider satisfaction were measured using 5-point Likert scales (1 = very negative; 5 = very positive). Body fat percentage measures were considered by the participants to be too confronting from a cultural perspective and risked confusing them, so it was agreed that the main measure would be weight as measured by simple scales. Weight was measured by facilitators 1, at baseline; 2, after the 12-week intervention; and 3, after 12 months.
Statistical Analyses
For this subset of data, simple frequency analyses are reported (detailed analysis of all data can be found in the original publication). 10
Results
Participants
A total of 25 overweight and obese (BMI < 44 > 24) women aged 35–59 years (mean, 42 years) were recruited and formed 2 groups; one group of 12 and another group of 13.
The Aboriginal women claimed to have been ‘overweight’ for a mean of 16 years. Socio-economic status of most participants was estimated by the facilitator as being predominantly low to middle income.
Of the 25 Aboriginal women, 19 (76%) completed the program (completion was defined by attending at least 4 of the 6 sessions). 16 of the 19 women completers (∼84%) lost some weight. There was a mean weight loss of 3.3 kg or 2.4% within this completing group with big individual differences recorded (for example, one woman lost more than 20 kgs). Five of 19 women completing the program (26%) maintained the clinically significant weight loss of > 5% after 12 months (mean, 11 kg (7.6%); SD = 5.45).
Of the women who did not complete the program, all 6 (24%) reported that they had unfortunate life events which interrupted their attendance. They all asked to be able to attend a future MYU in weight management that was subsequently delivered after the trial was completed.
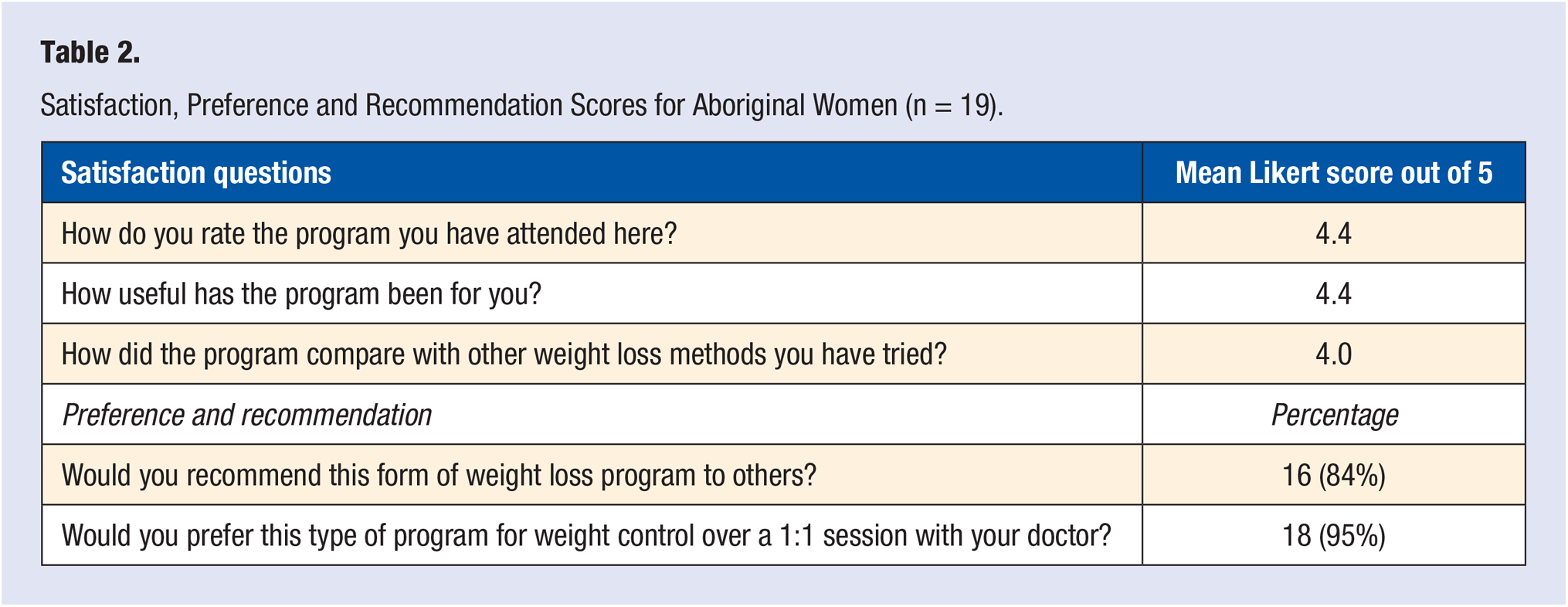
The satisfaction levels for completing participants were 4 or over (on a 5-point Likert scale) for all satisfaction type questions (see Table 2). 16 (84%) of the women completers said that they would prefer the MYU’s approach (with peers in the same room) compared to a conventional 1:1 consultation (alone, in a consulting room) with a doctor.
Satisfaction, Preference and Recommendation Scores for Aboriginal Women (n = 19).
The participating general practitioner (the same GP for all participants) rated the program highly and confirmed that she would prefer medical yarn ups (aka programmed shared medical appointments), over a standard educational program in most circumstances.
In a debriefing session following the last PMYU session, the GP and facilitators collectively also rated the MYU process highly, suggesting that it improved cultural safety and thus accessibility for these women.
Discussion
This secondary analysis of data, though limited in participant numbers and statistical power, further suggests that medical yarn ups may help provide culturally safe and accessible services for Aboriginal people who find current health services confronting, culturally unsafe and unresponsive.
MYUs in weight control (and other chronic disease areas) appear to offer what the Aboriginal and Torres Strait Islander Health Performance Framework has called for 12 : programs that are ‘culturally acceptable, conveniently located and easily incorporated into the daily schedule, with goal attainment that is realistic and appropriate, and led by identifiable Indigenous health services and health care providers’ (p. 1). 12
Further MYU trials are currently in process with Aboriginal people involving smoking cessation, chronic pain self-management and diabetes prevention. The MYUs in smoking cessation and diabetes prevention are also being trialled on-line, as virtual, online medical yarn ups (aka programmed shared medical appointments).
Medical yarn ups for Aboriginal people appear to offer a culturally sustainable model not only for the delivery of health care generally but also for the delivery of specific behavioural change and self-management programs to manage chronic and other lifestyle-related illness.
Key Points
SMAs provide an effective adjunct approach to chronic disease management in primary care.
pSMAs are a series of SMAs that provide an alternative to conventional 1:1 clinical care and can be delivered as telehealth medicine.
Aboriginal people have named programmed shared medical appointments, ‘Medical Yarn Ups (MYUs)’
Medical yarn ups are reported to help develop culturally safe care and accessibility for Aboriginal people
MYUs in weight management were well received by participants and providers and contributed to some weight loss for 16 of 19 (84%) of completers, and 5 of 19 (26%) of these women maintained clinically significant weight loss (> 5% BMI) for 12 months.
Footnotes
Acknowledgements
We wish to acknowledge COORDINARE, South East NSW, Primary Health Network for funding of this project. Ms Hayley Longbottom, Willow Firth, other staff and clients of Waminda Women’s Health and Welfare Service, Nowra NSW Australia
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.