
Abstract
This study aims to determine the impact of 2 (low vs high volume) high-intensity interval training (HIIT) programs with Mediterranean diet (MedDiet) recommendations on health-related quality of life (HRQoL) and lifestyle modification, and to examine the relationships between the changes in anxiety and depression with HRQoL and lifestyle variables after myocardial infarction (MI). Participants (n = 80) were randomized to attention control or one of the two supervised HIIT groups (2 d/weeks). Surveys before and after intervention (16 weeks): HRQoL (SF-36), anxiety and depression (HADS), MedDiet adherence (MEDAS), and physical activity (PA) and sedentary behavior (SB) levels. After intervention, there were improvements (P < .05) in HRQoL, HADS scores, and MedDiet adherence, with higher PA level in both HIIT groups with no between-HIIT group differences. The HADS score decline correlated (P < .05) with both the increase in physical component of SF-36 (r = .42), the overall metabolic expenditure (r = .26), and adherence to the MedDiet (r = .24), and the reduction in the SB (r = .35). HIIT exercise intervention with MedDiet recommendations improved HRQoL, along with reduced anxiety and depression symptoms, and a healthier lifestyle after MI. Better mental health was related to higher values of PA and MedDiet adherence.
Better emotional health is related to lower sedentary behavior rates and higher values of HRQoL's physical component, metabolic expenditure, vigorous PA, and MedDiet adherence.
An update of the practical recommendations on the core components of secondary prevention programs establishes the growing evidence for greater effectiveness of aerobic high-intensity interval training (HIIT, series of high-intensity workouts interspersed with light-to-moderate periods) compared to moderate-intensity continuous training in improving cardiorespiratory fitness. 1 Research has confirmed the multiple benefits of HIIT programs, including in health-related quality of life (HRQoL), as well as anxiety and depression states;2-4 additionally, it is presented as a safe, effective, and pleasant method. 5 Further, low-volume HIIT protocol (i.e., 10 minutes or less of accumulated work at high intensity) has been shown to be a time-efficient treatment for increasing cardiorespiratory fitness.6-8 In addition, many prospective observational studies reinforce the beneficial effects associated with higher adherence to the Mediterranean diet (MedDiet) in reference to the management of cardiovascular diseases and to establish a healthy way of living.9,10 Accordingly, there appears to be an association between the attainment of a healthy lifestyle with better mental function.
People who have suffered an acute myocardial infarction (MI) are more likely to perceive a poor HRQoL. 11 Hence, HRQoL questionnaires are considered important tools in prevention for monitoring increased risk of adverse health events. 12 In this sense, a lower HRQoL is associated with higher anxiety and depressive states, even 10 years later from post-MI. 13 This association increases the risk of MI incident 14 and doubles the risk of re-infarction and mortality compared to those without depression.15,16 Further, patients with depression tend to have a worse lifestyle with poorer diets, reduced physical activity (PA) level, and more stress.15,17 Therefore, it seems that healthy lifestyle behaviors are necessary to lessen the cardiovascular disease. 1 Previous reviews evaluating the literature on HRQoL outcomes for exercise-based secondary prevention programs are controversial. While some have reported important clinical improvements in physical performance and general health, 18 including a reduction in anxiety and depressive symptoms, 19 others show some evidence of a short-term benefit on HRQoL but with insufficient support. 20
While previous systematic reviews have reported the association between exercise and HRQoL in patients with cardiovascular disease,17-21 much less attention has been given to the rest of the core components in response to aerobic HIIT intervention with MedDiet recommendation. Therefore, the objectives of the present study in patients after MI were (1) to determine the effects of different aerobic HIIT programs (low volume vs high volume) with MedDiet recommendations on HRQoL, and lifestyle modification, and compared to an attention control (AC) group; (2) to examine the relationships between the changes in depression and anxiety with HRQoL and lifestyle variables; and (3) to determine predictors of mental health.
Material and Methods
Study Design
The protocol (ClinicalTrials.gov ID: NCT02876952) and informed consent procedures of the INTERFARCT study were approved by the university (UPV/EHU, CEISH, 2016) and hospital committee (CEIC 1462). The design and selection criteria have been previously detailed.
22
The measurements for the study were taken before (T1) and after (T2) the intervention period (16 weeks) (Figure 1). After baseline measurements, participants were enrolled in the study and were randomly assigned to one of the three intervention groups through randomization software using the stratified randomization technique by etiology and age: AC and exercise groups (low-volume HIIT and high-volume HIIT). The characteristics of the recruitment process, randomization, follow-up, and posterior analysis are described in the flow chart diagram following CONSORT statement criteria.
23
Flow diagram of the INTERFARCT study from recruitment to the end of the intervention.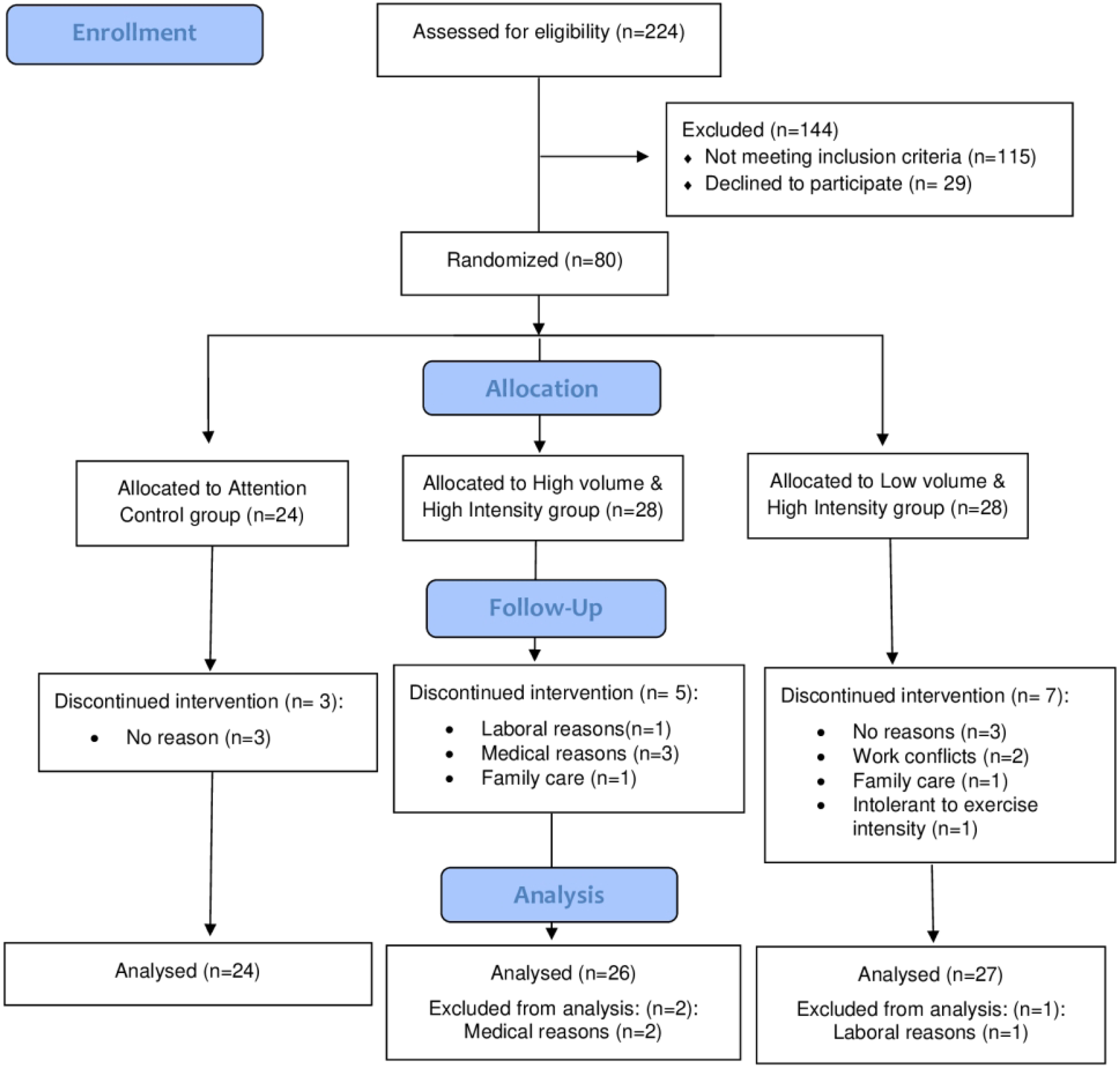
Participants
Baseline Demographic and Clinical Characteristics of the Participants. a
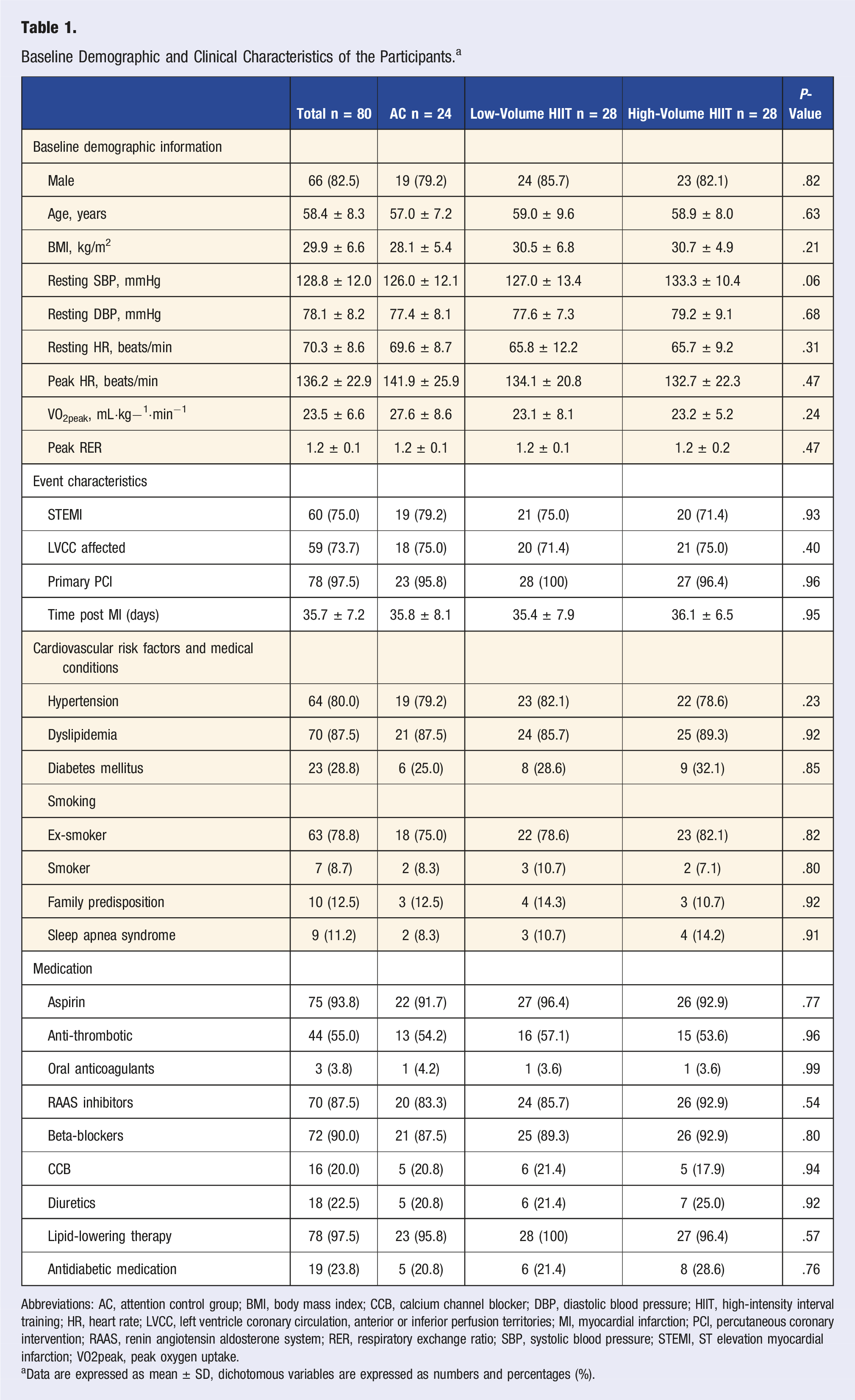
Abbreviations: AC, attention control group; BMI, body mass index; CCB, calcium channel blocker; DBP, diastolic blood pressure; HIIT, high-intensity interval training; HR, heart rate; LVCC, left ventricle coronary circulation, anterior or inferior perfusion territories; MI, myocardial infarction; PCI, percutaneous coronary intervention; RAAS, renin angiotensin aldosterone system; RER, respiratory exchange ratio; SBP, systolic blood pressure; STEMI, ST elevation myocardial infarction; VO2peak, peak oxygen uptake.
aData are expressed as mean ± SD, dichotomous variables are expressed as numbers and percentages (%).
Baseline Physical and Psychological Characteristics, Dietary Patterns, and Levels of Physical Activity and Sedentary Behavior of Participants.
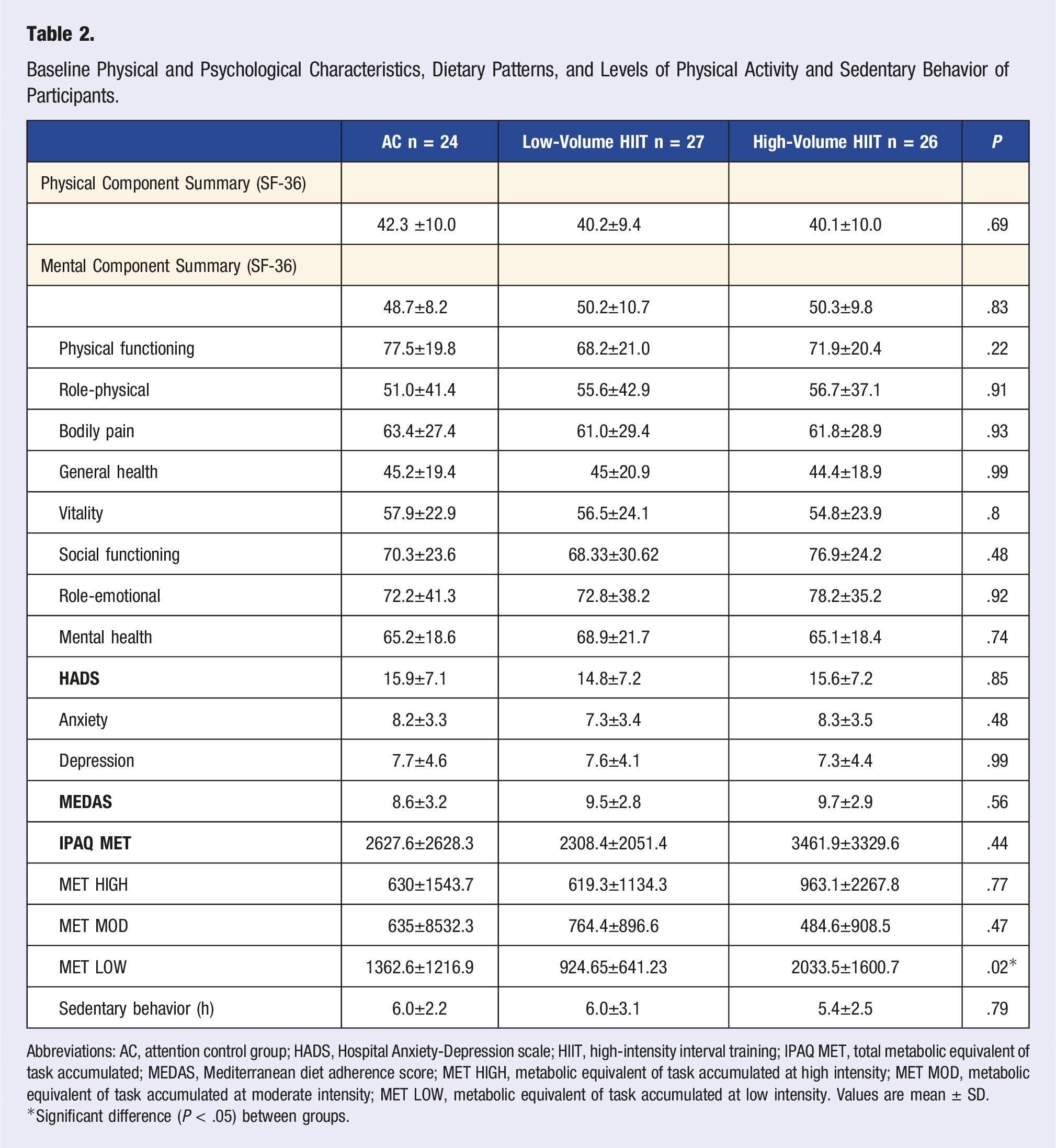
Abbreviations: AC, attention control group; HADS, Hospital Anxiety-Depression scale; HIIT, high-intensity interval training; IPAQ MET, total metabolic equivalent of task accumulated; MEDAS, Mediterranean diet adherence score; MET HIGH, metabolic equivalent of task accumulated at high intensity; MET MOD, metabolic equivalent of task accumulated at moderate intensity; MET LOW, metabolic equivalent of task accumulated at low intensity. Values are mean ± SD.
*Significant difference (P < .05) between groups.
Surveys
The standardized 36-item Short-Form Health Survey (SF-36) questionnaire was administered to assess the HRQoL. 25 The 36 items of the instrument cover the following scales: physical function, physical role, body pain, general health, vitality, social function, emotional role, and mental health; they also allow for the calculation of 2 summary scores, the physical component summary and the mental component summary, by combining the scores of each dimension. For each dimension of the SF-36, the items are coded, added, and transformed into a scale with a path from 0 to 100 (higher scores indicating higher levels of HRQoL) using the algorithms and indications that the scoring and interpretation manual of the questionnaire offers. 25 This instrument has been validated in Spain. 26
The Hospital Anxiety and Depression Scale (HADS) questionnaire assessed emotional stress (14 items) and specialists commonly use it to determine the levels of anxiety (7 items) and/or depression (7 items) that a person is experiencing. 27 Each item was scored from 0 to 3, and subscores are on scales of 0–21. Scores ≤ 7 on each subscale indicate no anxiety or depression, scores 8–10 indicate possible anxiety and depression cases, and scores ≥ 11 indicate high likelihood of anxiety and depression. The questionnaire was validated into the Spanish version of HADS. 28
Adherence to the MedDiet was measured by the 14-item Mediterranean Diet Adherence Screener (MEDAS) self-reported questionnaire 29 from the Spanish PREDIMED study. 30 Adherence was stratified based on the score as low (≤ 7 points), medium (8–9 points), and high (≥ 10 points). 29 To analyze the activity type or intensity of PA (walking, moderate, and vigorous activities) and estimated time spent sitting per week (sedentary behavior), participants completed the short form of the International PA Questionnaire (IPAQ). 31 Data were used to estimate total weekly PA in mLO2·kg−1·min−1 expressed as metabolic equivalent (MET) within each activity category by an estimated energy expenditure (i.e., 1 MET = 3.5 mLO2·kg−1·min−1). 31 The minutes and frequencies of physical activities are encoded in METs by an algorithm based on the following reference values: walking or slow PA, 3.3 MET; moderate PA, 4 MET; and vigorous or high PA, 8 MET. 31
Intervention
After evaluating dietary habits, all participants received Mediterranean diet recommendations with nutritional counseling every 2 weeks. 22
The AC group was advised to practice regular PA to keep ethical procedures regarding health with no supervision. 32 The exercise training groups (aerobic low- and high-volume HIIT) trained 2 non-consecutive days per week for 16 weeks under the supervision of an exercise specialist. Procedures and design have already been published. 22 In short, the training volume was kept constant in low-volume HIIT (always 20 minutes and less than 10 minutes at high intensity), whereas it was progressively increased in high-volume HIIT (i.e., from 20 to 40 minutes, with more than 10 minutes at high intensity). The intensity was individually tailored to heart rate at moderate or high intensities according to ventilatory thresholds from the cardiopulmonary exercise test.
Statistical Analysis
Statistical analyses were carried out with the SPSS statistical software package (22nd edition). Descriptive statistics were calculated for all independent variables and data are expressed as the mean ± standard deviation (SD), or frequency and percentage.
One-way analysis of variance was used to determine if there were significant pre-intervention differences among groups. The comparison of frequencies in categorical variables among groups was performed using the Chi2 test.
Data were analyzed according to the intention to treat principle. The paired-sample t-test was used to compare the baseline and follow-up values of all the independent variables. Analysis of covariance was used to examine training effects across intervention groups; post-intervention outcomes were selected as dependent variables, and analysis was adjusted for the pre-intervention outcome of each dependent variable. Bonferroni post-hoc comparisons and Helmert contrasts were performed to analyze the differences between all groups or the 2 exercise training groups pooled together vs the AC group, respectively. Statistical significance (P-value) was set at 95% (α < .05). It was identified that adequate power (.80) to evaluate differences in our design consisting of 3 experimental groups would be achieved with 177 people (59 each group, α = .05, effect size f = .23). 22 Therefore, as the sample size was too small to have adequate power for statistical significance for anything smaller than large effects, the current report takes special consideration of effect sizes for each outcome variable. 33 Hedges’ g (g) was used as the index of effect size for within and between comparisons of the 2 groups (i.e., T1 vs T2; after-intervention change in AC vs HIIT). A g index of .2 was considered a small effect; .5, medium; and .8, large. 34 Cohen’s f (f) was used to assess training effects across the different intervention groups (AC, low-volume HIIT, and high-volume HIIT). An f index of .1 was considered a small effect; .25, medium; and .4, large. 35
Pearson’s coefficient assessed the correlation between changes in markers of physical health behaviors and mental health markers. Forward stepwise linear regression was performed to test the effects of physical health behaviors on HADS and to determine which variables are the strongest predictors of improvement in mental health.
Results
All participants were under pharmacological treatment. No significant between-group differences were observed (P > .05) in anthropometrics, physical, physiological, psychological, and pharmacological treatment after random assignment (Tables 1 and 2). Three participants (n = 1 low-volume HIIT, n = 2 high-volume HIIT) did not complete the 16-week intervention due to causes unrelated to the study (Figure 1).
Physical and Psychological Characteristics, Dietary Patterns, and Levels of Physical Activity and Sedentary Behavior Before (T1) and After (T2) Intervention Period.
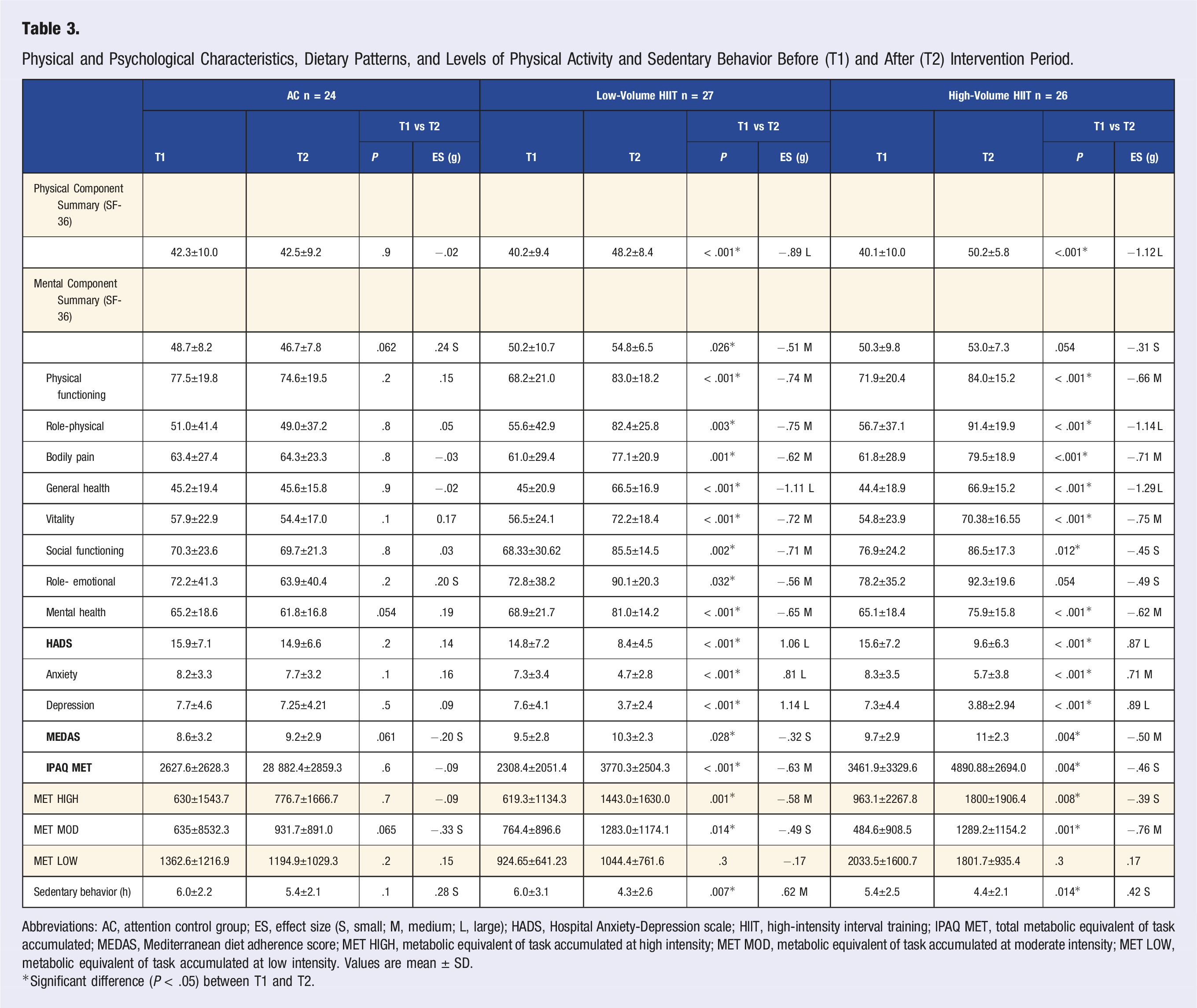
Abbreviations: AC, attention control group; ES, effect size (S, small; M, medium; L, large); HADS, Hospital Anxiety-Depression scale; HIIT, high-intensity interval training; IPAQ MET, total metabolic equivalent of task accumulated; MEDAS, Mediterranean diet adherence score; MET HIGH, metabolic equivalent of task accumulated at high intensity; MET MOD, metabolic equivalent of task accumulated at moderate intensity; MET LOW, metabolic equivalent of task accumulated at low intensity. Values are mean ± SD.
Significant difference (P < .05) between T1 and T2.
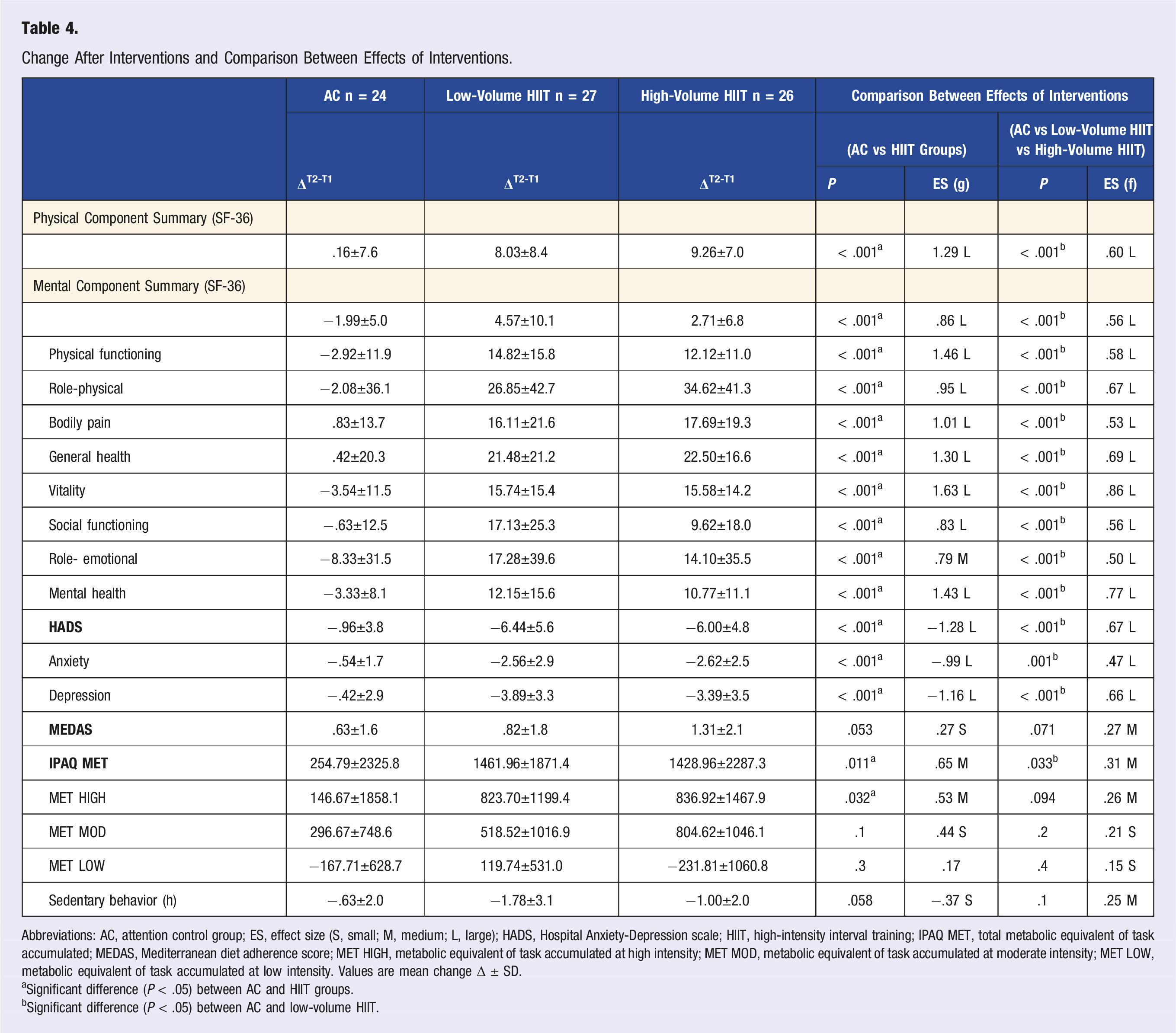
Change After Interventions and Comparison Between Effects of Interventions.
Abbreviations: AC, attention control group; ES, effect size (S, small; M, medium; L, large); HADS, Hospital Anxiety-Depression scale; HIIT, high-intensity interval training; IPAQ MET, total metabolic equivalent of task accumulated; MEDAS, Mediterranean diet adherence score; MET HIGH, metabolic equivalent of task accumulated at high intensity; MET MOD, metabolic equivalent of task accumulated at moderate intensity; MET LOW, metabolic equivalent of task accumulated at low intensity. Values are mean change Δ ± SD.
aSignificant difference (P < .05) between AC and HIIT groups.
bSignificant difference (P < .05) between AC and low-volume HIIT.
Only HIIT groups reported significantly better anxiety (low volume, g = .81; high volume, g = .71) and depression (low volume, g = 1.14; high volume, g = .89) scores at T2 with significant lowering effects (P < .001), and the changes in AC were not significant. Low-volume HIIT resulted in a bigger change of anxiety scores than high-volume HIIT (P < .001, g = .8 and P < .001, g = .7, respectively). There were no significant differences between HIIT groups observed in any of the studied variables at T2 (P > .05), but the differences between HIIT and AC effects were large and significant in all variables (P < .001, g > .9) (Table 4).
Regarding the frequencies of the categorized anxiety and depression HADS scores (Figure 2), in AC, low-volume HIIT, and high-volume HIIT, the participants (a) without anxiety symptoms increased at T2 16.7%, 22.2%, and 30.8%, respectively; (b) with possible anxiety decreased −8.4%, −7.4%, and −11.6%, respectively; and (c) with a high likelihood of anxiety decreased −8.3%, −14.8%, and −19.2%, respectively. Frequencies of anxiety and depression categories at T1 (before) and T2 (after intervention) for the Hospital Anxiety and Depression Scale questionnaire assessed in each group of the INTERFARCT study (AC, attention control; LV HIIT, low-volume and high-intensity interval training; HV HIIT, high-volume and high-intensity interval training).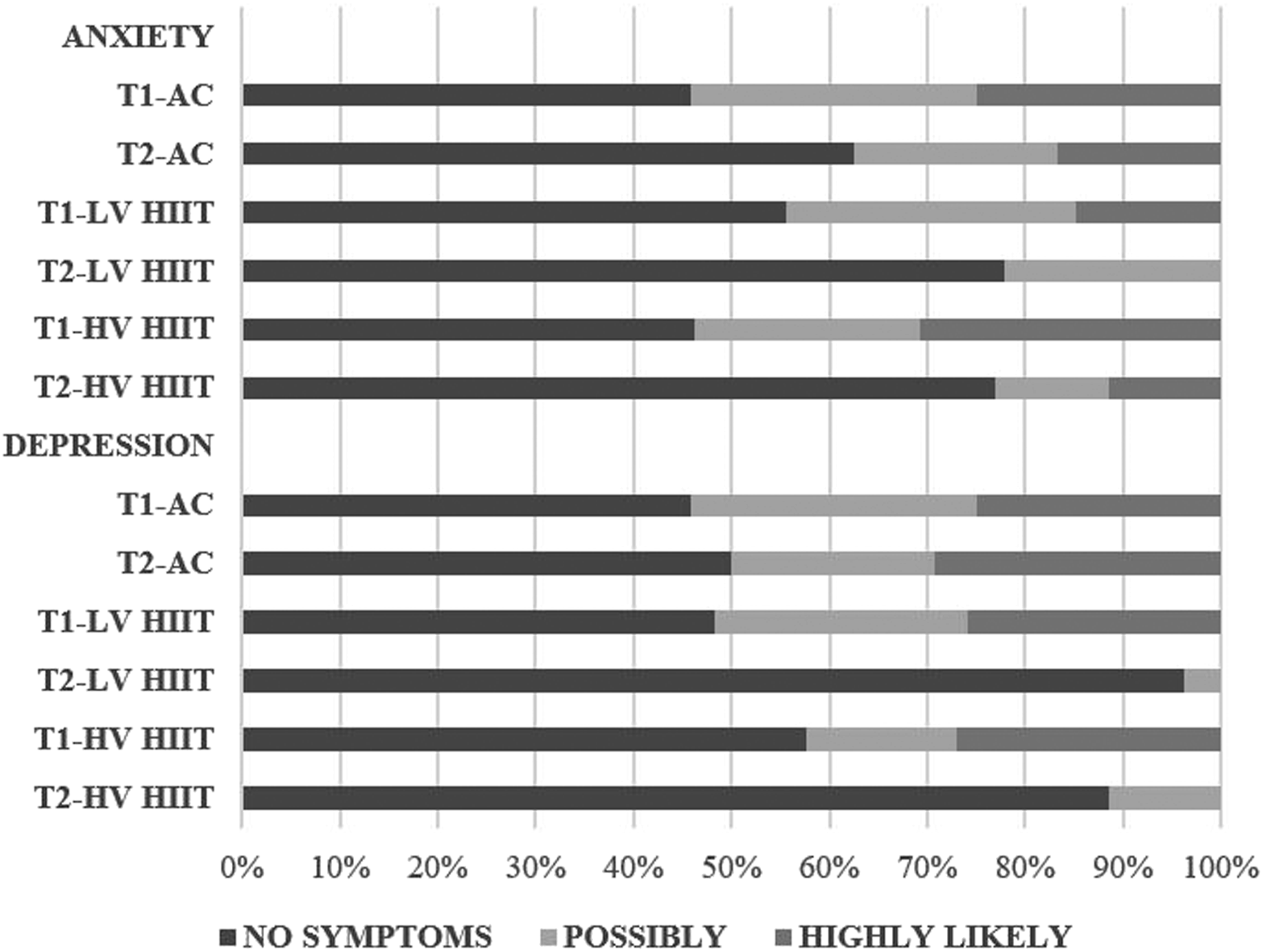
Concerning the depression component (Figure 2), at T2, the number of participants identified as (a) not having symptoms in AC, low-volume HIIT, and high-volume HIIT was increased by 4,2%, 48.1%, and 30.8%, respectively; (b) with possible depression decreased −8.4%, −22.2%, and −3.9%, respectively; and (c) with a high likelihood of depression increased 4.2% in the AC, and decreased −25.9% and −26.9%, in HIIT groups.
Regarding adherence to the MedDiet (Table 3), there was no significant change in AC (P = .061). Significant but small in low-volume HIIT (P = .03, g = .3) and medium in high-volume HIIT (P = .004, g = .5). No significant changes between intervention-differences were observed (Table 3). After intervention, the IPAQ results indicated that energy expenditure rose in general and at different intensities (low, moderate, and high), showing significant effects after HIIT interventions. The most interesting being after low-volume HIIT in total MET and high-intensity PA (P < .001, g = .6), and after high-volume HIIT in moderate-intensity PA (P < .001, g = .76). Moreover, HIIT interventions were demonstrated to produce medium-sized significant effects in vigorous and general PA rates compared to AC (P < .05, g > .5). Low-volume HIIT was the intervention that reduced sedentary behavior the most, producing a medium significant effect (P < .01, g = .6), followed by the small significant effect of high-volume HIIT (P = .01, g = .4); the small differences observed between AC and HIIT were not significant (P > .05, g = .37).
Correlations between the changes in different variables were observed. Thus, the decrease of HADS and depression score correlated with the increase of physical component summary (r = .42, P < .001 and r = .41, P < .001, respectively), the reduction of sedentary behavior (r = .35, P = .002 and r = .33, P = .004, respectively), the increase of IPAQ rated general metabolic expenditure (r = .26, P = .02 and r = .30, P = .007, respectively) and vigorous PA metabolic expenditure (r = .24, P = .03 and r = .27, P = .02, respectively), and with the rise in adherence to MedDiet (r = .24, P = .03 and r = .29, P = .01, respectively).
Linear regression analysis pointed out that (1) a decrease in sedentary behavior (i.e., spending less time sitting), along with an increase in physical component summary, could lead to a reduction in anxiety and depression (r = .47, r 2 = .22, P = .001) and (2) an increase in physical component summary and IPAQ rated general metabolic expenditure could lead to a reduction in the depression component alone (r = .45, r 2 = .20, P = .003). Other variables (i.e., higher values in MEDAS or vigorous PA) also correlated negatively with HADS’ components and could lead to a lower depression score, but those changes did not seem to report greater relations than those previously cited.
Discussion
This research was carried out in patients after MI to determine the impact of 2 different HIIT programs (low-volume vs high-volume) with MedDiet recommendations after the 16-week intervention compared to an AC group on HRQoL, anxiety and depression symptoms, and lifestyle. Thus, greater and significant improvements in most of the domains of SF-36 (physical and mental), HADS (anxiety and depression), MEDAS (adherence to Mediterranean diet), and IPAQ (PA and sedentary behavior) surveys were observed in both HIIT groups, with no significant differences between HIIT groups, but large and significant differences between AC vs HIIT groups. Further, changes with higher values of physical component summary, general metabolic expenditure, and vigorous PA, rise in adherence to the MedDiet, along with lower sedentary behavior were related to a decrease in HADS and depression score, showing a clear association between a healthy lifestyle (PA and healthy diet) and better emotional health (Figure 3). Main outcomes of the study.
Recent investigation has reported significant improvements in depression severity and HRQoL after HIIT, Nordic walking, and moderate-to-vigorous intensity continuous training. 4 Less is known regarding the different impacts of low-volume HIIT and high-volume HIIT. In this sense, both HIIT exercise programs carried out in the current research also demonstrated their effectiveness in improving the HRQoL and lowering the anxiety and depression symptoms. Therefore, the time efficiency of the low-volume HIIT is particularly remarkable, since the same effects are achieved with half the volume of time compared with the high-volume HIIT. These results confirm previous analyses in this research comparing both HIIT volumes on other variables.6,36
The relationship between emotional health, assessed by symptoms of anxiety and depression, and cardiovascular disease is complex and bidirectional. 13 In our sample of participants after MI, around 25% of them presented highly likely symptoms of anxiety and depression before the intervention. We shall emphasize that aerobic exercise HIIT program with nutritional recommendations reduced the symptoms in the whole group, and specifically by 15–19% in the HIIT groups. Therefore, it is worth noting the increase in patients without depressive symptoms after both HIIT programs, resulting in 96.3% and 88.5% of participants in low-volume and high-volume, respectively (Figure 2). The mechanisms through which PA in general, and aerobic HIIT exercise in particular, might facilitate a better physical, emotional, and social perception might be related to the endocrine crosstalk between skeletal muscle and the brain, representing one of the most effective strategies to reduce the prevalence of depression and to improve brain functions.37,38
Increasing exercise levels and adopting a healthier diet, such as adherence to the MedDiet, are considered the main modifiable factors in cardiovascular disease prevention and treatment.39,40 In the present study, adherence to the MedDiet was significantly augmented by the 2 HIIT groups, improving, consequently, cardio-healthy eating patterns and greater protection against new cardiovascular events. 30 Further, recent investigations have demonstrated that adherence to the MedDiet may protect neurocognition and play a vital role in the maintenance of cognitive health, 41 and is positively associated with the general health subscale of HRQoL. 42
Furthermore, the recommended core components for secondary prevention programs include PA counseling to increase PA throughout the week,1,32 since the structured exercise program usually generates an insufficient total amount of PA. 43 In the present study, both HIIT exercise groups significantly decreased the amount of time spent on sedentary behavior and increased moderate-to-vigorous PA. These results are highly relevant because of the association between higher levels of moderate-vigorous PA and improvements in cardiorespiratory fitness with a lower prevalence of cardiovascular disease and risk factors. 44 However, once again, the efficiency of the low-volume HIIT program should be highlighted, being the most favorable in achieving better results reducing sedentary behaviors compared to high-volume HIIT. Previous investigations have already mentioned the compensatory effect of a high-volume exercise program with a reduction/increase of PA/sedentary behavior, respectively; promoting, therefore, low-volume exercise programs to improve health-related outcomes. 45
Finally, the present study confirms, as former investigations,4,46-48 the close and beneficial relationships among changes in physical and mental components of HRQoL and a healthier lifestyle with better emotional health (less depressive and anxiety symptoms) after 16-weeks of HIIT exercise and MedDiet recommendation-based program. Therefore, including not only exercise but also diet/nutritional counseling will encourage preventive health behaviors (Figure 3).
Some limitations of the present study need to be recognized. First, the small sample (n = 80), not reaching a priori statistical power for the study, and predominately male (82%) and white non-Hispanic population limit the generalizability of the findings. Secondly, there was no long-term follow-up after the 16-week exercise training intervention with MedDiet recommendations to observe the adherence to the program and the relationship between changes in the outcomes. Finally, total MET levels and MET at moderate- and high-intensity activities obtained by the IPAQ questionnaire and not through more objective methods, could overestimate real PA levels performed, assuming that cardiac patients may have a reduced physical capacity. 43
Conclusion
This study showed the beneficial effects of 16-week aerobic HIIT interventions with MedDiet recommendations on most of the domains of HRQoL, along with reduced anxiety and depression symptoms and a healthier lifestyle in patients after MI. Low-volume HIIT is a time-efficient adjuvant program for improving physical and mental health. Better emotional health is related to lower rates of sedentary behavior, and higher values of the physical component of HRQoL, metabolic expenditure, vigorous PA, and adherence to the MedDiet.
Footnotes
Acknowledgments
The authors thank the participants for their commitment. Our special thanks to Rodrigo Gallardo and Tatiana Matajira as cardiologists of the project. This paper is in memoriam of Dr Juan Jose Goiriena, a brilliant person and researcher who supported the research and the project from the beginning.
Author Contributions
All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The trial was supported by the Santiago Apostol Hospital (Miranda de Ebro, Burgos, Spain) and the Department of Physical Education and Sport (University of the Basque Country, UPV/EHU).