
Abstract
‘The good news is that primary care physicians and internal medicine residents show a high interest in receiving nutrition training.’
Poor sleep, poor stress management, sedentary behavior, and a low-nutrient-density diet contribute substantially to the most common chronic diseases of the Western world.1,2 The benefits of following a Mediterranean dietary pattern are well documented, and adherence to this diet can be quantified using a “Mediterranean diet score.”3-5 Improvements in the Mediterranean diet score are associated with a reduced risk of heart disease and stroke,3,5-9 diabetes,2,10 some cancers, 11 Parkinsonism, 12 and overall mortality.2,5 In contrast, higher intake of fast food and processed food has been associated with higher mortality.13,14
Despite the burden of chronic disease attributable to lifestyle and the rising associated health care costs, nutrition education in medical training is declining.15-17 Even in the face of strong recommendations from bodies such as the American Heart Association, 18 a minority of medical schools have a course dedicated to nutrition 19 and a minority of internal medicine residents report adequate training in nutrition.20-23 This is unfortunate as studies consistently show that the more confidence a physician feels in knowledge of nutrition, the more likely they are to counsel their patients.22,24-26 Conversely, lack of knowledge and confidence in nutrition counseling stand as significant barriers to patient counseling.24,27 The good news is that primary care physicians and internal medicine residents show a high interest in receiving nutrition training.23,28,29
In residency programs where food is provided to the residents there is also an opportunity to emphasize the importance of nutrition for physicians. Many residency programs offer snacks and meals that have low nutritional value. Only about half of internal medicine residents thought their program provided healthy meal options, 21 and studies show that residents tend to gain weight during training.30,31 Improving resident diet is a way to support the well-being of trainees, while also improving attitudes toward patient counseling. Studies have shown that trainees who follow a healthy lifestyle are more likely to counsel their patients about the benefits of a healthy lifestyle.21,32,33
We developed a curriculum for internal medicine residents to address this gap in education, which included a workshop, longitudinal didactics, case discussions, and incremental changes to the food provided at conferences. We hypothesized that residents would feel more confident in counseling patients and feel more strongly that nutrition is important in patient care after our intervention.
Methods
Setting and Participants
Our curriculum was enacted at the University of Washington—Boise Internal Medicine Residency Program (UW Boise IM) during the 2018-2019 academic year. We had a total of 30 residents and all participated in the curriculum (9 Cat R1, 4 Prelim R1, 9 R2, 8 R3).
Intervention and Implementation
Workshop
All residents attended a 90-minute interactive workshop during the annual fall resident retreat. This session focused on the benefits and principles of the Mediterranean diet. The residents practiced (with each other) taking a 24-hour dietary history, giving it a Mediterranean diet score, and then working with a hypothetical patient to recommend incremental dietary changes. The association between incremental change in Mediterranean diet score and cardiovascular disease risk was emphasized.
Conference Food
We made incremental changes to food provided at conferences. Morning report cookies, candy, and chips were replaced by apple slices, fresh vegetables, nuts, and chips and salsa purchased and prepared by chief residents (the cost was reimbursed). Lunch conference catered meals were adjusted after discussions with the residents and program leadership (see Table 3). The improvement in the Mediterranean diet score with these changes was discussed with the residents and verbal feedback solicited. The culmination of changes to the provided food, as measured by the Mediterranean diet score, was roughly associated with a reduction in cardiovascular disease risk and overall mortality by around to 30% and 25%, respectively.2,4,5
Pre-Conference “Teasers”
Brief, interactive didactic sessions focused on culinary medicine and the Mediterranean diet were used about once every other week as “teasers” prior to morning report or lunch conference. Some focused on the clinical implications of dietary modifications on chronic diseases such as hypertension, type 2 diabetes, heart failure, and hyperlipidemia. Others focused on giving a Mediterranean diet score to published diets of celebrities and then recommending incremental changes. And others discussed broader lifestyle pearls such as exercise and other diets.
Continuity Clinic
A refresher on dietary history taking and the Mediterranean diet score was presented at pre-clinic conference on Monday for 4 weeks (in order to catch every resident given our 3 + 1 scheduling). Residents were encouraged to choose one patient coming in that week, and based on their dietary history help them make incremental changes. Some residents were concerned about the time commitment so we collaborated with nurses who were willing to take the 24-hour dietary history from the patient. A poster with basic Mediterranean diet principles was posted in resident workspaces.
Grand Rounds
There were 2 grand rounds sessions devoted to culinary medicine and the Mediterranean diet during the intervention period. These focused on the association between diet and chronic disease, and small- and large-scale interventions to help patients improve their diet.
Data Collection and Analyses
We used a voluntary, anonymous survey administered both prior to the curriculum (September 2018) and then at the culmination of the curriculum (March 2019). The survey included the Nutrition Competence Questionnaire (NUTCOMP), a validated instrument aimed at measuring self-perceived competence in providing nutrition care to patients with chronic disease. 34 We modified this slightly to focus on the Mediterranean diet. The survey also included questions about the food served at conferences and basic demographic information.
The primary outcome was the NUTCOMP total score. Secondary outcomes were individual NUTCOMP questions and lunch conference preferences. The individual questions had a Likert-type scale with items from 1 to 5 (1 was the lowest and 5 the highest score). To examine the change from baseline for the total score a t test was used. Because of the ordinal nature of the individual questions, they were examined using a Mann-Whitney U test.
This study was reviewed by the IRB and determined to be QI/Program Evaluation exempt.
Results
Of 30 residents, 26 (87%) submitted the pre-intervention survey, and 26 (87%) submitted the post-intervention survey (not necessarily the same 26). The demographics information on the participants is provided in Table 1.
Demographics of Study Participants.
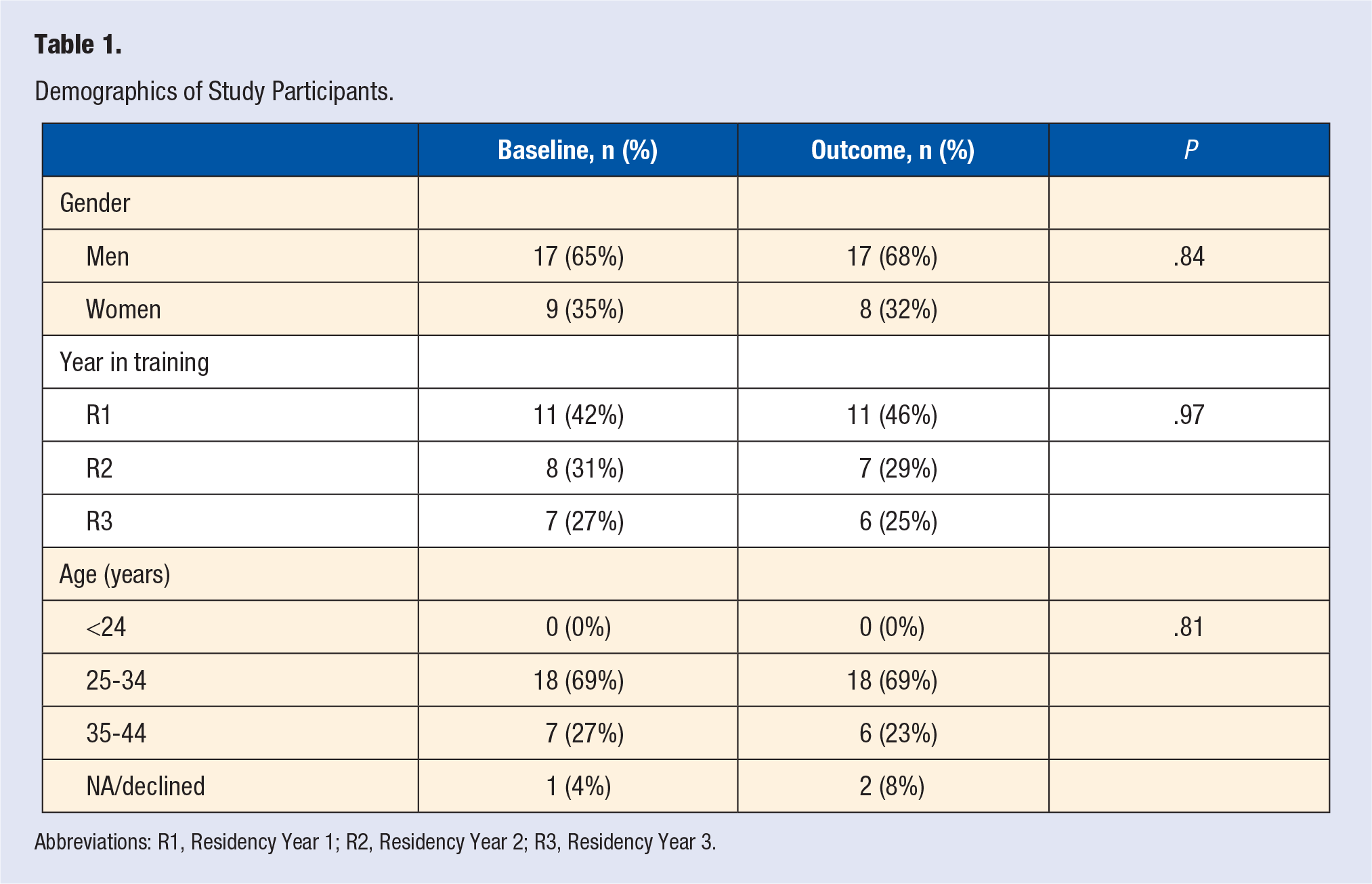
Abbreviations: R1, Residency Year 1; R2, Residency Year 2; R3, Residency Year 3.
Comparing pre to post intervention, there was a significant increase in mean NUTCOMP total score from 3.5 (95% confidence interval [CI] 3.4-3.6) to 4.0 (95% CI 3.9-4.2), P < .0001, indicating that our residents’ self-perceived competence providing nutrition care to patients with chronic disease improved. Looking at individual NUTCOMP domains, we saw significant improvement in confidence in describing the Mediterranean diet and in using it to evaluate an individual’s diet and propose changes (see Table 2). Our residents thought that attention to nutrition was important and worth their clinical time both before and after our intervention, without significant change between the 2 time periods.
NUTCOMP Survey Results a .
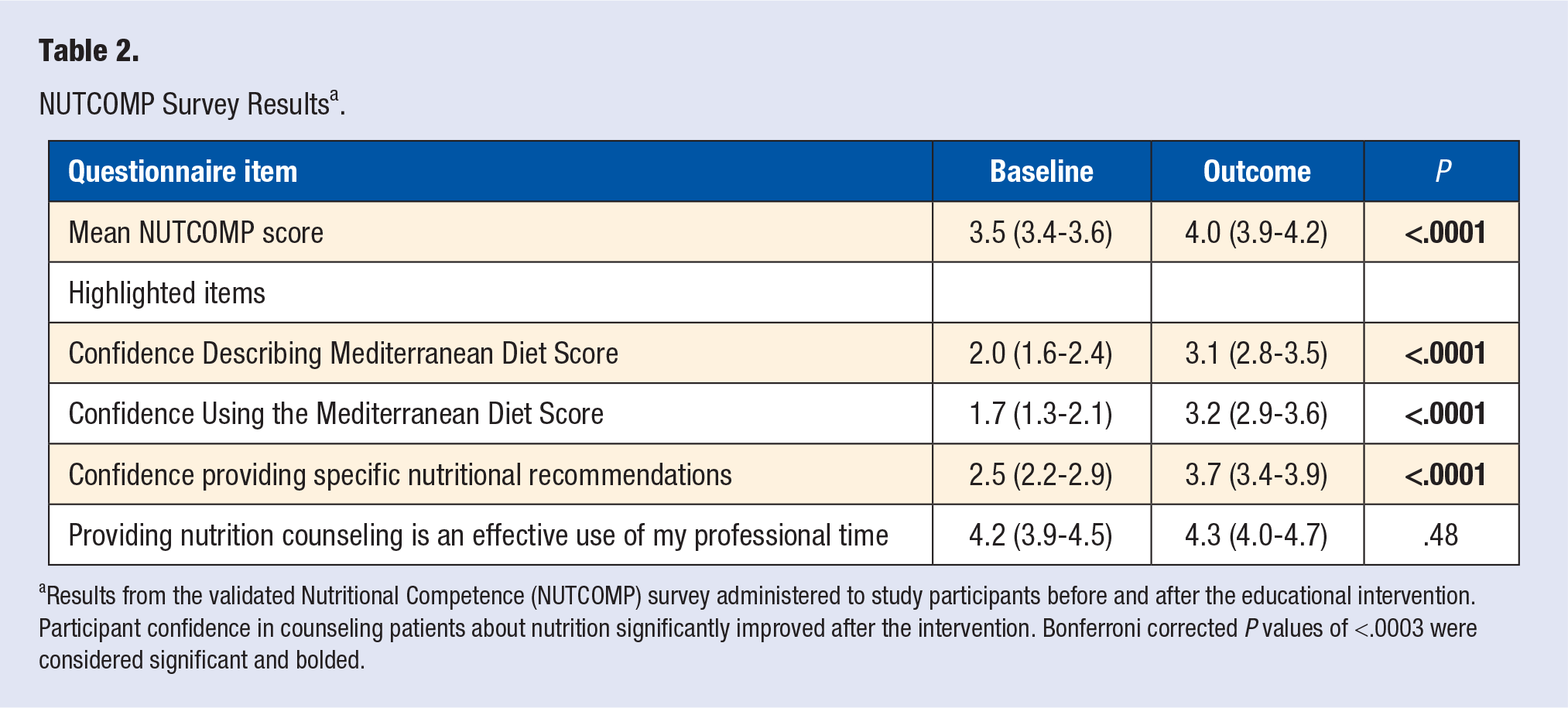
Results from the validated Nutritional Competence (NUTCOMP) survey administered to study participants before and after the educational intervention. Participant confidence in counseling patients about nutrition significantly improved after the intervention. Bonferroni corrected P values of <.0003 were considered significant and bolded.
Residents enjoyed the healthier lunch conference food more (before 3.5, 95% CI 3.2-3.7; after 4.2, 95% CI 3.9-4.5, P = .001) and felt that the lunch conference food was healthier after the intervention (before 2.9, 95% CI 2.6-3.3; after 3.9, 95% CI 3.5-4.3, P = .0006; see Table 3).
Conference Food Preferences a .
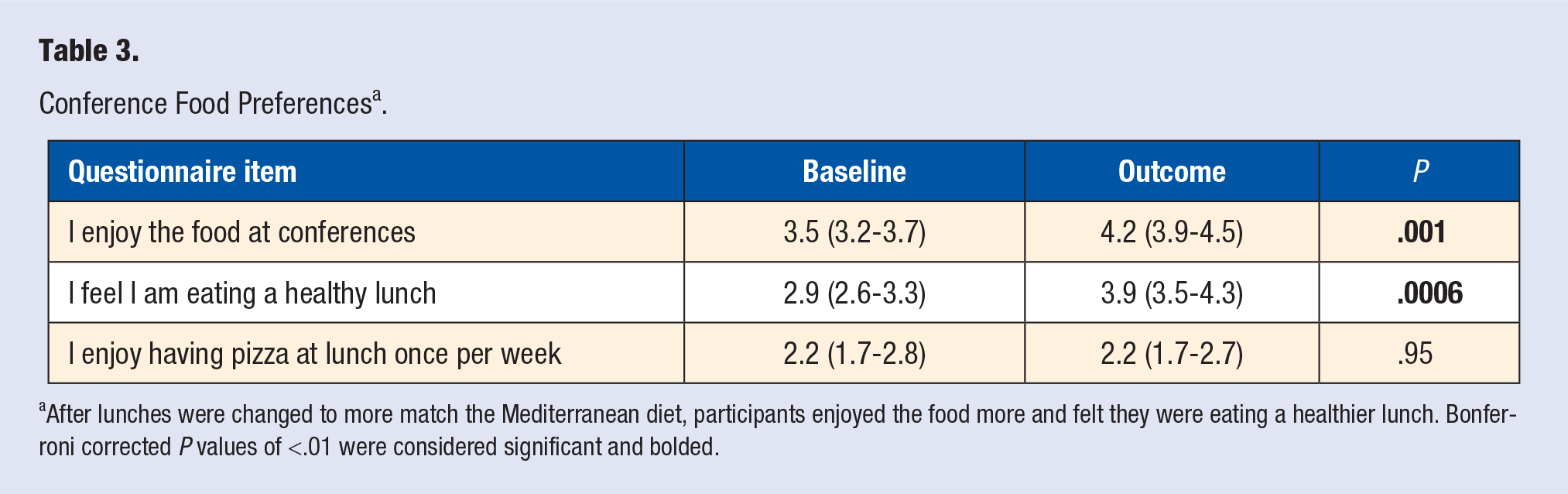
After lunches were changed to more match the Mediterranean diet, participants enjoyed the food more and felt they were eating a healthier lunch. Bonferroni corrected P values of <.01 were considered significant and bolded.
Table 4 describes the lunch menu and snack options before and after changes were made along with approximate costs. The costs for the lunch meals include delivery and catering fees. The approximate Mediterranean diet score of the provided food ranged from 1 to 4 pre-intervention compared to 4 to 7 after.2,4,5
Lunch Menu and Morning Report Snacks Provided a .
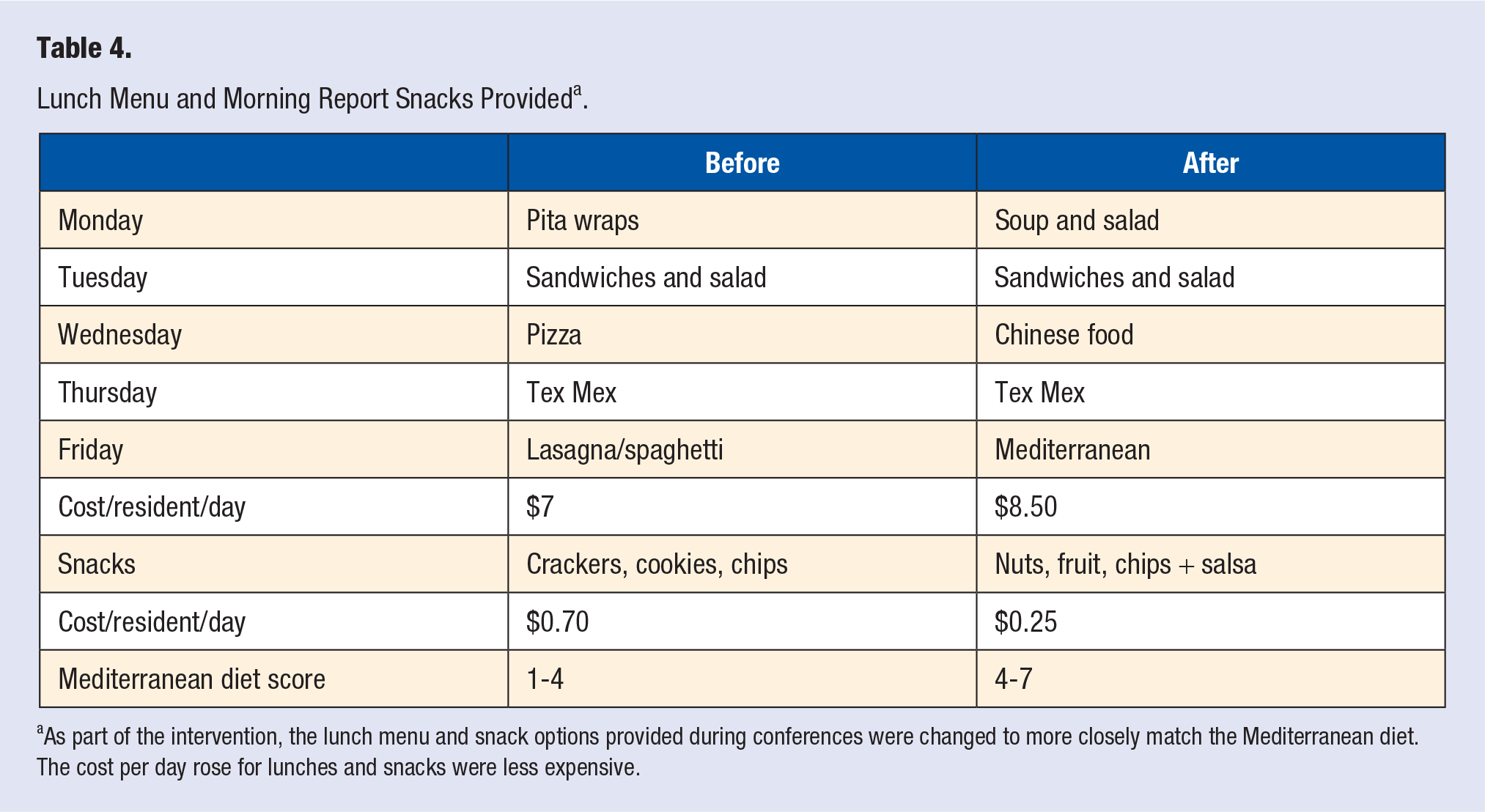
As part of the intervention, the lunch menu and snack options provided during conferences were changed to more closely match the Mediterranean diet. The cost per day rose for lunches and snacks were less expensive.
Feasibility
This intervention required significant support from the internal medicine residency leadership. Time at the residency retreat, didactic sessions, pre-clinic sessions, and grand rounds was used to teach this content. The processes for providing snacks and lunch conference food were altered. The chief residents used residency program funds to purchase healthier snacks and prepared them for morning report conferences. The healthier snacks were cheaper than the baseline unhealthy options, but the healthier lunches were more expensive. Overall more money was spent on food during this intervention.
Most of the curriculum was delivered by one chief resident and one faculty member, but others contributed as well.
Discussion
While many studies show the health benefits of proper nutrition, exercise, and other healthy behaviors, there is a lack of adequate education on nutrition counseling among health care professionals, residents, and medical students.21,33,35,36 Studies of medical students and residents show that while they are interested in nutrition education and they think it is important, they lack confidence in their knowledge of nutrition and nutrition counseling.20,21,23,37,38 Our residents corroborated these findings in our pre-intervention survey.
To our knowledge, there have been few studies evaluating nutrition education interventions among medical trainees.39,40 Our intervention was a multimodal approach that included several didactic strategies as well as overt changes to provided conference food. We intended to model the incremental changes we wanted residents to recommend to their patients by incrementally changing the provided food at conferences. This also helped us emphasize that physicians who improve their own diet tend to have more confidence recommending dietary changes to their patients.21,32,33
Studies show that providers with more training and confidence in nutrition counseling provide it to their patients more often.21,22,29 Our intervention led to improvements in residents’ confidence using the Mediterranean diet score, and confidence providing nutritional recommendations to patients. Our hope and expectation is that our residents will use the knowledge and confidence gained through this intervention to improve their own diet and to counsel their patients frequently about lifestyle and nutrition.
The main limitation in our study is that we did not ask or monitor how often residents are actually providing nutrition counseling to their patients. Studies of practicing physicians and residents suggest that dietary counseling is performed with a minority of patients and during <25% of visits.29,41-43 We hope that our residents are doing better than this but cannot confirm it. Other limitations include the single-program design, the small number of residents in our program, the lack of long-term data on sustainability, and that we did not assess residents’ knowledge gained from the curriculum.
We feel that much of our intervention can be applied broadly. This intervention was primarily driven by one chief resident and one faculty member with the consent of the residency program leadership. There was no protected time or full-time equivalent allotted for this intervention, and we did not involve our registered dietician colleagues. Our intervention did increase the cost of provided lunch conference food, but it decreased the cost of morning report snacks. Programs with a fixed food budget may still be able to incrementally improve the nutrition of their provided food by asking chief residents to obtain and prepare low-cost healthy snack food like apple and orange slices, chips and salsa, carrots, peanuts, or whole wheat crackers.
Conclusion
Through a multimodal intervention including teaching sessions and healthy changes to the lunch and snacks provided, residents at our program felt more confident in their nutrition knowledge and their ability to counsel patients about their dietary habits. Our residents also liked the healthier food options. This is a small start in a long road ahead of us to fill the educational deficit and prepare primary care physicians to provide nutrition and lifestyle counseling for our patients.
Supplemental Material
sj-docx-1-ajl-10.1177_1559827621994499 – Supplemental material for The Lunch Conference Diet: Fostering Resident Engagement in Culinary Medicine Through a Curriculum Centered on Changes to Provided Conference Food
Supplemental material, sj-docx-1-ajl-10.1177_1559827621994499 for The Lunch Conference Diet: Fostering Resident Engagement in Culinary Medicine Through a Curriculum Centered on Changes to Provided Conference Food by Richmond S. Doxey, Michael F. Krug and Rick Tivis in American Journal of Lifestyle Medicine
Supplemental Material
sj-pdf-1-ajl-10.1177_1559827621994499 – Supplemental material for The Lunch Conference Diet: Fostering Resident Engagement in Culinary Medicine Through a Curriculum Centered on Changes to Provided Conference Food
Supplemental material, sj-pdf-1-ajl-10.1177_1559827621994499 for The Lunch Conference Diet: Fostering Resident Engagement in Culinary Medicine Through a Curriculum Centered on Changes to Provided Conference Food by Richmond S. Doxey, Michael F. Krug and Rick Tivis in American Journal of Lifestyle Medicine
Footnotes
Acknowledgements
We would like to thank the residents, administration, and staff at the University of Washington—Boise Internal Medicine Residency Program who were very supportive of this project.
Authors’ Note
Preliminary data presented at Grand Rounds, Boise VA, March 7, 2019; and at the University of Utah Hospitalist Group, August 15, 2019. Preliminary data presented as a poster at Mountain West Regional SGIM, October 4, 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was reviewed by the institutional review board and determined to be QI/Program Evaluation exempt.
Informed Consent
Not applicable.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.