
Abstract
A significant amount of illness has origins in oral microorganisms. The current SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) pandemic has reduced the general population’s access to and use of routine and nonemergency dental care. This creates a dangerous situation in which oral bacteria, fungi, and viruses may remain unchecked and allowed to flourish, which in turn increases risks for several systemic diseases as well as negative outcomes for pregnancies and surgical patients. This situation presents opportunities for health maintenance and disease prevention by individuals as well as for dental health professionals to use anti-infective treatments and procedures. Lifestyle medicine professionals have a chance to encourage behaviors that individuals can undertake to promote good oral health outside of the dentist’s office as well as shaping public perceptions about and reinforcing the importance of resuming dental visits as governmental restrictions allow.
Keywords
The relationship between poor oral health and systemic diseases has been increasingly recognized and scientifically correlated over the past 2 decades.
Oral health is central to a person’s overall health and well-being.1,2 One hundred years ago, Joseph Head, MD, DDS, wrote that infections of the teeth and gums causes directly or indirectly one-half of the fatal diseases. 3 The relationship between poor oral health and systemic diseases has been increasingly recognized and scientifically correlated over the past 2 decades. Oral bacterial and viral infections have clearly been associated and/or identified in the epidemiology of many aspects of human disease conditions and suffering. 4 Oral health is a window into the health of the body and can be an indicator of nutritional deficiencies, host immune status, and acute and chronic diseases.
During 2020, government restrictions due to the SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) pandemic have affected the general population’s access to and ability to utilize dental health care services, both preventative and restorative. On August 3, 2020, the World Health Organization recommended delaying nonessential dental care including routine cleanings and nonemergency visits. 5 This lack of care may have repercussions in the population’s overall health and exacerbate problems that already existed, such as abscesses and other infections, tooth loss, tooth decay, and gum disease. Even before the pandemic, there were several unrecognized opportunities for lifestyle medicine professionals to positively influence people’s overall good health by supporting improved dental care and prevention. The pandemic has highlighted these opportunities to an even greater extent. Poor oral health, including periodontal disease, is a significant public health problem that can affect a person’s effectiveness and quality of life at work, school, and home. 1 From a public health perspective, currently 133 million Americans suffer from chronic illnesses, with many of these associated with oral health and systemic invasion from oral inflammatory constituents. 6
Oral Bacteria and Systemic Disease
Slots has published on the complex nature of periodontal infections. 7 Periodontitis is associated with a variety of bacteria, fungi, and herpesviruses. 8 These oral microbiota may not remain as localized infections on periodontal surfaces but have been associated with at least 43 extra oral human diseases.9,10 To illustrate this point, in a recent study, cerebrovascular accident thrombi were analyzed and 76% were found to be polymerase chain reaction positive for Viridans streptococci—often found asymptomatically in the mouth, but a putative pathogen in the bloodstream. 11
A number of epidemiological studies have shown a link between poor oral health and a range of medical conditions, 12 including cardiovascular diseases, 13 type 2 diabetes, 14 adverse pregnancy outcome, Alzheimer disease,15,16 osteoporosis, 17 aspiration pneumonia, 18 and rheumatoid arthritis. 19 In particular, a bidirectional relationship has been noted between periodontitis and diabetes mellitus.20,21 Diabetes is also associated with an increased risk for periodontitis, and periodontitis affects the control of diabetes. In patients with periodontitis, treatment has been associated with an approximately 0.4% decrease in hemoglobin A1c levels. Health risk factors including obesity, physical activity, and diet have also been associated with the risk for periodontitis. Preliminary studies suggest an association between oral health and dementia including Alzheimer’s disease. 22 Oral health care has been associated with a lower risk for Alzheimer’s disease. 23 Allowing oral bacteria to flourish unchecked during the pandemic may result in increased incidence of numerous systemic health conditions and diseases.
SARS-CoV-2 Transmission and Dental Care
The current global pandemic of SARS-CoV-2 presents with a variety of symptoms including fever, dry cough, and myalgias as well as dysgeusia and hyposomia. 24 The virus may be spread through respiratory droplets, by contact with contaminated surfaces, and possibly by aerosolization. An individual may transmit the virus from contaminated surfaces with the oral, nasal, and eye mucosal membranes. 25
The dental office is a potential site of cross-contamination of patients and dental staff if adequate precautions are not in place. 25 Persons may transmit the virus whether they are symptomatic or asymptomatic in health and dental care facilities. Measures need to be taken to mitigate airborne, contact spread, as well as from contaminated surfaces of the virus. 26 Such measures could include body temperature measurement of patients, administration of a symptom questionnaire immediately prior to an office visit, hand hygiene, use of personal protective equipment by the patient and health care provider, disinfection of clinical surfaces, and management of clinical waste. 27 Recent reports28,29 indicate that patients’ fear of dental visits may be heightened during the SARS-CoV-2 pandemic, and dentists themselves have reported anxiety about contracting the virus or transmitting it to patients unknowingly. 30
While chlorhexidine is commonly used as a mouth rinse in the dental office, current evidence suggests it may not be effective against SARS-CoV-2. 31 Therefore, products containing 1% hydrogen peroxide, 0.2% povidone-iodine, or 0.25% sodium hypochlorite have been suggested for a 60-second rinse-swish-gargle preoperative oral anti-infective pretreatment protocol. Nasal saline irrigations, betadine, and other iodine-containing products have also been proposed as a means of decreasing the COVID-19 (coronavirus disease 2019) viral load in the nasal cavity and thus reducing the risk of transmission to health care providers and others.32,33
These and related considerations have led the UK National Health Service to the recently initiated the ELVIS COVID-19 trial in Scotland. 34 This is a randomized control study of hypertonic saline irrigation and gargling for patients with suspected or confirmed COVID-19. The goal of this study is to determine if nasal irrigation and gargling with saltwater helps patients with COVID-19 to recover more quickly. The number of times per day patients will perform nasal irrigation or gargling will depend on the severity of the patient’s symptoms. Patients may need to perform these procedures up to 12 times a day until they are well or on day 14 of their infection.
Oral Health Behaviors
Before the pandemic, several Healthy People 2030 goals were targeted at oral health behaviors and outcomes and included the following: 35
Decrease the proportion of adults aged 45 and older who have moderate and severe periodontitis
Increase the proportion of current smokers who receive information from dentist/dental hygienist on reducing tobacco use/or smoking cessation in the past year
Increase the proportion of persons with diabetes who are counseled by a dentist/dental professional regarding the benefits of checking their blood glucose level
The Office of the Surgeon General has also published reports on oral health. The first report on oral health published in 2000 outlined safe and effective disease prevention measures that everyone can adopt to improve oral health and prevent disease. 36 Twenty years later, the Surgeon General commissioned an update to that report that will document the progress in oral health, identify existing knowledge gaps, and articulate a public health vision for the future, with an emphasis on the the following:
Critical nature of poor oral health as a public health issue
Need to increase awareness of the importance of oral health to overall health and well-being
Promise of science to transform the oral health of the nation
The emergence of the pandemic has only increased the urgency and importance of these prescriptions.
Interventions to Reduce the Risk of Bacteremia and Systemic Inflammation
Addressing oral hygiene with low-cost interventions such as frequent tooth brushing and professional dental cleaning should reduce the risk of developing cardiovascular and other diseases associated with oral bacteria. Treatment and eradication of bacteria microbiome associated with periodontitis is essential.37,38 Specifically, exposing common oral microbiome biofilm to 5% and 10% povidone-iodine in vitro for 5 minutes or longer can suppress these pathogens. 39 Galvan et al also have reported that a 0.25% sodium hypochlorite oral rinse decreased dental plaque and bleeding as an effective approach to controlling periodontal disease. 40
Oral Health Care During Pregnancy
Maternity care has also been affected by the SARS-CoV-2 restrictions. Oral health care is important during pregnancy and has been associated with better pregnancy outcomes. 41 Higher rates of gingival inflammation can result in periodontitis, which, when untreated, is associated with preterm deliveries. Without the pandemic restrictions, the percentage of women who have had a dental visit during pregnancy was on the rise, with 38% visiting a dentist in 2009 and 42% in 2012. Studies on this topic have the deficiency of causing procedural metastatic inflammation. Anti-infective strategies to reduce biofilm entry during mucosal manipulation will likely help differentiate the true effects of periodontal inflammation and the pregnancy outcome.
Preoperative Oral Care
Biofilms are on the surfaces of the teeth and oral mucosa especially the tongue and can be mechanically removed to reduce pathogens. 42 Research has indicated that preoperative oral care can reduce the risk of postoperative pneumonia. Ishimaru et al studied 509 179 patients who underwent major cancer surgery in Japan. Postoperative pneumonia was associated with a significant decrease in patients who had preoperative oral health care. 43
What the Patient Can Do
The history of cleaning teeth began in 3500-3000 BC by the Babylonians. In the Middle Ages, Europeans used a handle embedded with hog bristles to clean teeth. In 1938, Dupont corporation pioneered the marketing of nylon bristles as a replacement for pig bristles.44,45 Oral health is central to a person’s overall health and well-being and the dentist/dental professional is now recognized to support this goal. Good self-care, such as brushing with an antiseptic oral mouthwash followed by a topical fluoride rinse, twice daily flossing, and routine professional depuration treatment may contribute to maintaining good oral health. The ultimate goal of self-care is to keep the periodontal interface free of inflammation and the teeth from developing decay. Health behaviors that can lead to poor oral health include tobacco use, excessive alcohol use, and poor diet.
A variety of products have been suggested for patients to use to remove dental biofilms and avoid the need for dental health care professional interventions. However, a review by Slots 7 indicated that only a few have been shown clinically effective and without significant side effects over the moderate term follow-up. Of the products studied, sodium hypochlorite (bleach) oral rinse seems to hold the greatest promise. Use of 0.25% sodium hypochlorite oral rinsing twice-weekly for 3 months was associated with a significant decrease in plaque-free surfaces and teeth showing no bleeding on probing in comparison with a control group and a decrease in subgingival levels of periodontopathic bacteria without a significant increase in tooth staining.
During the SARS-CoV-2 pandemic, the Centers for Disease Control and Prevention was concerned about the risks of closing dental practices during the shutdown. They warned about a combination of negative factors including economic challenges, oral health care access restrictions, increases in health risk factors, and elevated safety concerns that might pose significant challenges for providers and patients—particularly those in the most vulnerable population. 46 Fortunately, one recent report shows that US dental patients did not neglect their oral health care during the shutdown. A Delta Dental survey conducted in early October 2020 found that 86% of respondents made at-home oral health care a priority during the pandemic, recognizing the importance of oral health and its contribution to overall good health. 47
Dental Health in Working Populations
In addition to studies of dental health in the general population, some investigators have looked at employed populations in particular. Burton et al reported that for employees covered with fully paid biannual preventive health exams and cleanings, only 65.4% of employees had at least one annual preventive dental claim (see Figure 1). 48 Benefits administrators and occupational health professionals need to highlight the importance of routine dental care, especially when the out-of-pocket cost to the employee is so low.
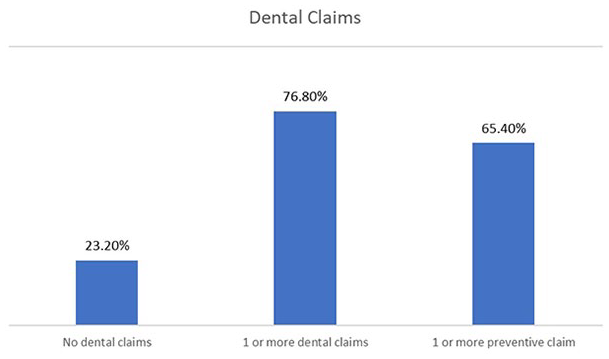
Preventive and total dental claims in employed population. 44
Conclusion
Dental school curricula generally do not include student education on available anti-infective strategies which take direct aim at reducing orally originated pathogenesis. Similarly, the physician community generally exists as a silo separate from the dental health professional community. Therefore, there is a significant opportunity for mutual education and collaboration. Such cooperation should focus on the risks from inadequate oral health care and how these risks can be mitigated—both separately and in combination—by health care professionals and by their patients.
It is essential that both dental and medical health professionals, as well as patients and those in the general public who are not patients, recognize that medical conditions can be caused directly by or are facilitated and/or amplified by disseminated oral biofilm constituents: bacteria, fungi, and viruses. Anti-infective dentistry is medically, ethically, and economically mandatory for optimal oral health and well-being. Reinforcing the importance of preventive dental care and its relationship to overall bodily health will require focused communications after the SARS-CoV-2 shutdown of dental services. Public and patient fears about going to the dentist should be addressed. More education is needed but governmental reassurance or recommendations to safely resume dental visits and preventive care might also be needed to encourage returns to good oral hygiene.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.