
Abstract
Mental health symptoms are pervasive, with 1 in 5 American adults experiencing a mental disorder. Poor mental health is associated with a significant global cost burden, from disability to economic impacts. The field of lifestyle medicine, which emphasizes the role of lifestyle factors in the onset and treatment of disease and well-being, is well suited to address mental health. More recently, there has been attention to the need to incorporate mental health into the field of lifestyle medicine and to attend to the bidirectional role of mental health and lifestyle. Thus, there is a critical opportunity for the field of lifestyle medicine to incorporate mental health into each of the foundational pillars (diet, exercise, substance use, psychological well-being/stress, relationships, sleep) while also specifically targeting lifestyle interventions for populations with mental disorders. The current article provides a framework for the role of mental health within lifestyle medicine by addressing the scope of the problem, clarification regarding mental health, and areas of practice (ie, psychiatry), and providing an overview of the relevant mental health literature for each pillar. This article serves as a call to action to explicitly address and include mental health within all aspects of lifestyle medicine research and practice.
‘Mental health symptoms and disorders comorbid with chronic physical health conditions can result in exacerbation of barriers to effective and sustainable lifestyle changes that may be critical to good outcomes.’
From humble roots, the field of lifestyle medicine has shown exponential growth in recent years as burgeoning clinical interest aligns with an increasing appreciation for the role of lifestyle factors in the etiology and treatment of disease, as well as overall well-being. The foundations of lifestyle medicine research and practice are framed within foundational pillars, which include (plant-centric) nutrition, physical activity, sleep, risk reduction of substance use, psychological well-being and stress management, and healthy interpersonal relationships. 1 The 2020 Lifestyle Medicine Research Summit recommendations noted that mental health is related to each of the lifestyle pillars and is highly relevant to healthy lifestyle and overall quality of life. Recommendations from the summit specifically outlined the motivation and ongoing efforts to further develop the empirical foundation of the 6 pillars of lifestyle medicine. 2 Importantly, among the key areas that require further development, as noted by the committee, several are related to mental health and include the following: dietary interventions for brain health (mental health and neurocognitive disorders); interventions to better address stress and resilience; how lifestyle medicine can be utilized for the prevention, early detection, and intervention for substance use disorders; and better understanding and application of positive psychological interventions for individuals and communities. 2 Given the understanding that mental health is inextricably linked to lifestyle factors, and therefore lifestyle medicine, it stands within reason that further appreciation for, and development of, mental health within lifestyle medicine is necessary.
Lifestyle Medicine for Mental Health
Whereas the current lifestyle medicine paradigm may be well applied to psychologically healthy individuals, millions of individuals worldwide suffer from mental health symptoms and disorders, which greatly influences health behaviors and quality of life. Mental disorders such as major depressive disorder, as well as subclinical symptoms of depression, often overlap with serious and chronic physical health conditions (ie, diabetes, cardiovascular disease [CVD]) and add to the burden of such conditions. Mental health symptoms and disorders comorbid with chronic physical health conditions can result in exacerbation of barriers to effective and sustainable lifestyle changes that may be critical to good outcomes. Health disparities and social determinants of health are also highly relevant to mental health. There is a preponderance of mental disorders in certain populations—for example, increased risk of negative mental and behavioral health outcomes (ie, greater rates of symptoms and disorder) among groups who experienced more adverse childhood events. 3 Individuals and groups of lower socioeconomic status are also disproportionately affected by mental disorders and typically have less access to resources to support a healthy lifestyle across the life span (ie, fresh produce at grocery stores, safe environments for physical activity). 4 Furthermore, some individuals and groups are at greater risk for chronic stress that is related to myriad sociocultural factors—for example, the well-documented physical and mental health implications of cumulative experiences of racism and minority stress.5,6 Attention to the factors that affect access, engagement, and efficacy of lifestyle medicine interventions is critical to the development of this important field. Thus, for many individuals, a framework that specifically attends to mental health and that applies some of the foundational mental and behavioral health literature from psychiatry and psychology may most effectively allow lifestyle medicine interventions to support individual and population health.
The Current State of Lifestyle Medicine Research
Much of the lifestyle medicine research, such as the impact of diet and nutrition on mental health, has been conducted over the past decade and has begun to provide emerging evidence of the key role of nutrition in the onset, symptomatology, and treatment of mental disorders, particularly anxiety and depression. 7 Research, and implementation to clinical work, has been slow to emerge for a variety of reasons—namely, methodological challenges—because few randomized controlled trials (RCTs) have been conducted to date. 7 Thus, it should be noted, that even for those areas of lifestyle medicine with more research, much of the psychiatry and mental health research is correlational in nature. This means that although we can appreciate the association between constructs (ie, X is related to Y), we cannot infer causation (ie, X directly caused Y).
Further research is necessary to draw conclusions about causal relationships between lifestyle behavioral and mental health outcomes. 8 Although emerging science may be key to addressing the global burden of mental health, the applications to psychiatry and psychology practice remain nascent, and more research on both the biological pathways that may be influenced as well as mental health interventions are necessary to establish evidence-based practices that can inform lifestyle medicine. 7 Despite these empirical limitations, sufficient evidence indicates the importance of understanding and addressing mental health within lifestyle medicine to allow for effective interventions, lifestyle changes, and optimization of quality of life among all people.
Where Can We Go From Here?
There is an important opportunity to continue to develop the field of lifestyle medicine consistent with the recommendations outlined by the 2020 Lifestyle Medicine Research Summit committee. Specifically, there is a need to lay groundwork to better address mental health within lifestyle medicine and provide evidence-based lifestyle medicine for all regardless of where they fall on the spectrum of mental health. During this formative time of lifestyle medicine, specifically addressing mental health within each pillar, and lifestyle medicine at large, is a critical opportunity. Emerging science demonstrates the myriad pathways through which biological, psychological, and social factors influence mental health, including the potentially negative implications of poor health behaviors (ie, insufficient sleep) on mental health. 8 Ignoring the bidirectional role of mental health within each pillar of lifestyle medicine would not only add to the pervasive stigma that already surrounds mental health, but would also exclude a large, and important, subset of the population.
Thus, to begin to address some of the important issues that stem from specific consideration of acute and chronic mental health symptoms and conditions within the scope of lifestyle medicine, the current article outlines foundational mental health definitions, application of psychiatry and psychology in lifestyle medicine, the current state of the literature connecting mental health with each of the 6 pillars, and manners of conceptualizing mental health that are relevant to lifestyle medicine practice.
Foundations of Mental Health
The American Psychological Association defines mental health as a mental state that includes the ability to effectively adjust behavior, emotional well-being, lack of disabling symptoms, and the ability to develop quality relationships and cope with daily life stressors 9 (Table 1). The American Psychiatric Association emphasizes effective functioning in daily life for mental health, specifically functioning in work, education, relationships, and coping with adversity. 10 Mental health accounts for psychological, social, and emotional well-being and is influenced by overlapping biological, psychological, and social factors. 11 Whereas mental health is a transient state, which may be primarily positive or primarily negative, mental illness is indicative of a diagnostic mental health disorder. A mental disorder is a psychological or behavioral syndrome that reflects an underlying psychobiological dysfunction that results in significant distress or dysfunction and is not an expected response to typical stressors or societal conflict. 12 Of note, mental disorders fall on a spectrum, ranging from the experience of one or more symptoms of a mental disorder to a cluster of symptoms that do not meet full diagnostic criteria. Each of these foundational definitions is relevant to lifestyle medicine theory and practice as well to various disciplines and provider types that align with lifestyle medicine.
Definitions of Mental Disorder, Health, and Illness.
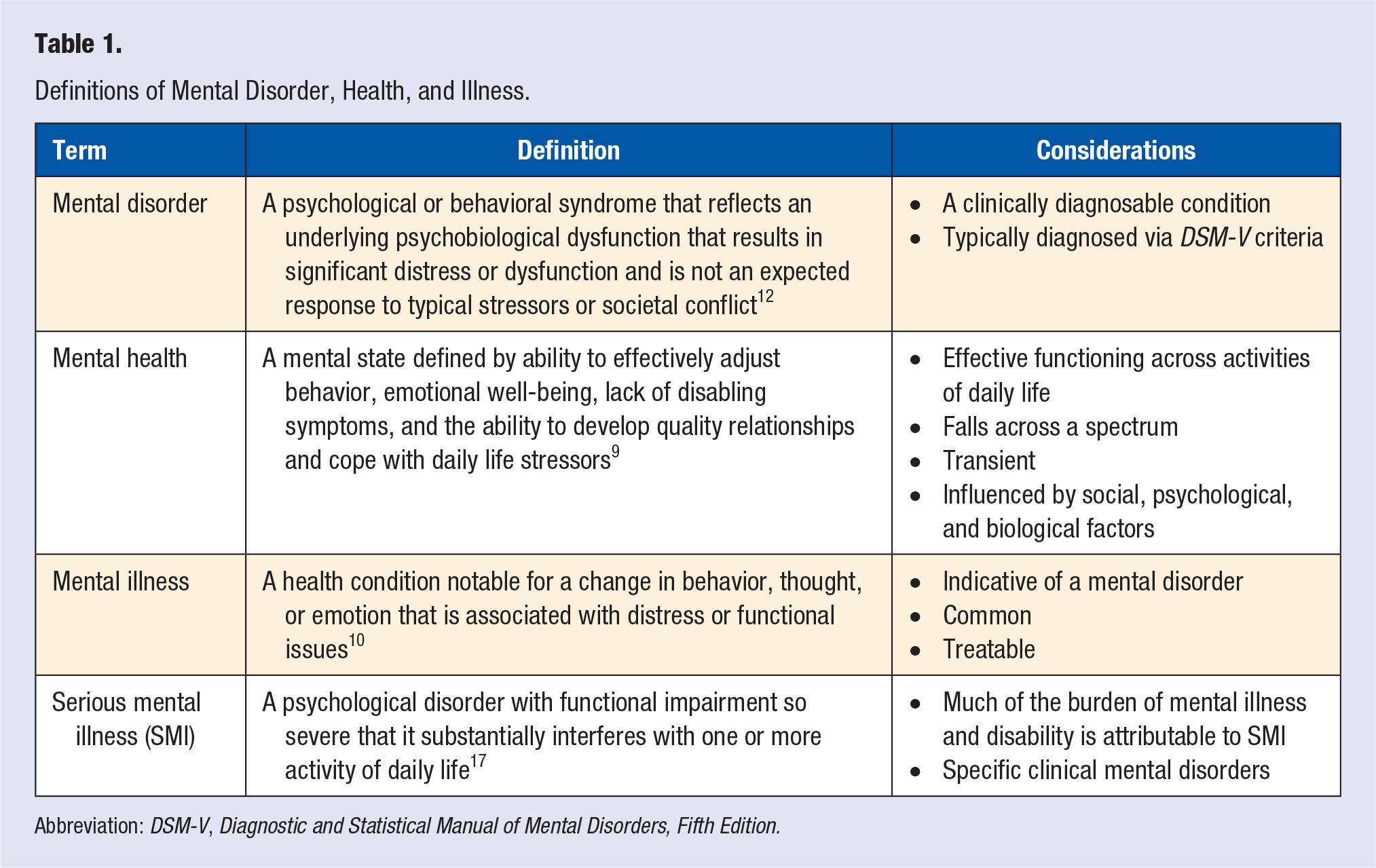
Abbreviation: DSM-V, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
Mental and Behavioral Health Disciplines
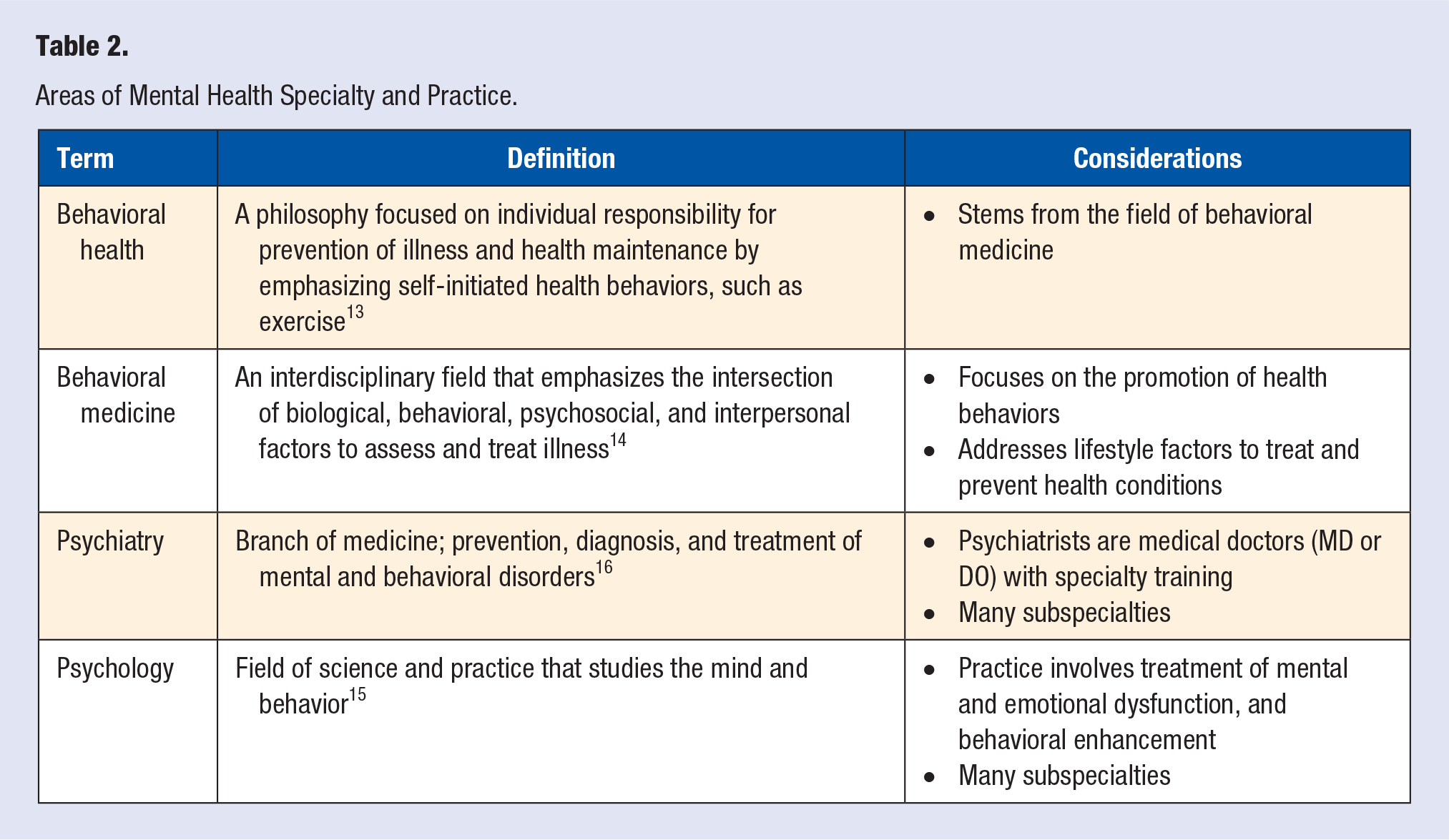
The philosophy of behavioral health is focused on individual responsibility for prevention of illness and health maintenance by emphasizing self-initiated health behaviors, such as exercise 13 (Table 2). Behavioral health stems from the field of behavioral medicine, an interdisciplinary field that emphasizes the intersection of biological, behavioral, psychosocial, and interpersonal factors to assess and treat illness. The field of behavioral medicine specifically seeks to promote health behaviors and address lifestyle factors to treat and prevent physical and mental health conditions. 14 Behavioral medicine has some overlap with the broad field of psychology. By definition, psychology is the study of behavior and the mind, and the practice of psychology focuses on treating dysfunction (ie, mental, emotional) and enhancing behavior. 15 Similar, yet distinct, psychiatry is an area of medicine that encompasses the prevention, diagnosis, and treatment of mental and behavioral disorders. 16
Areas of Mental Health Specialty and Practice.
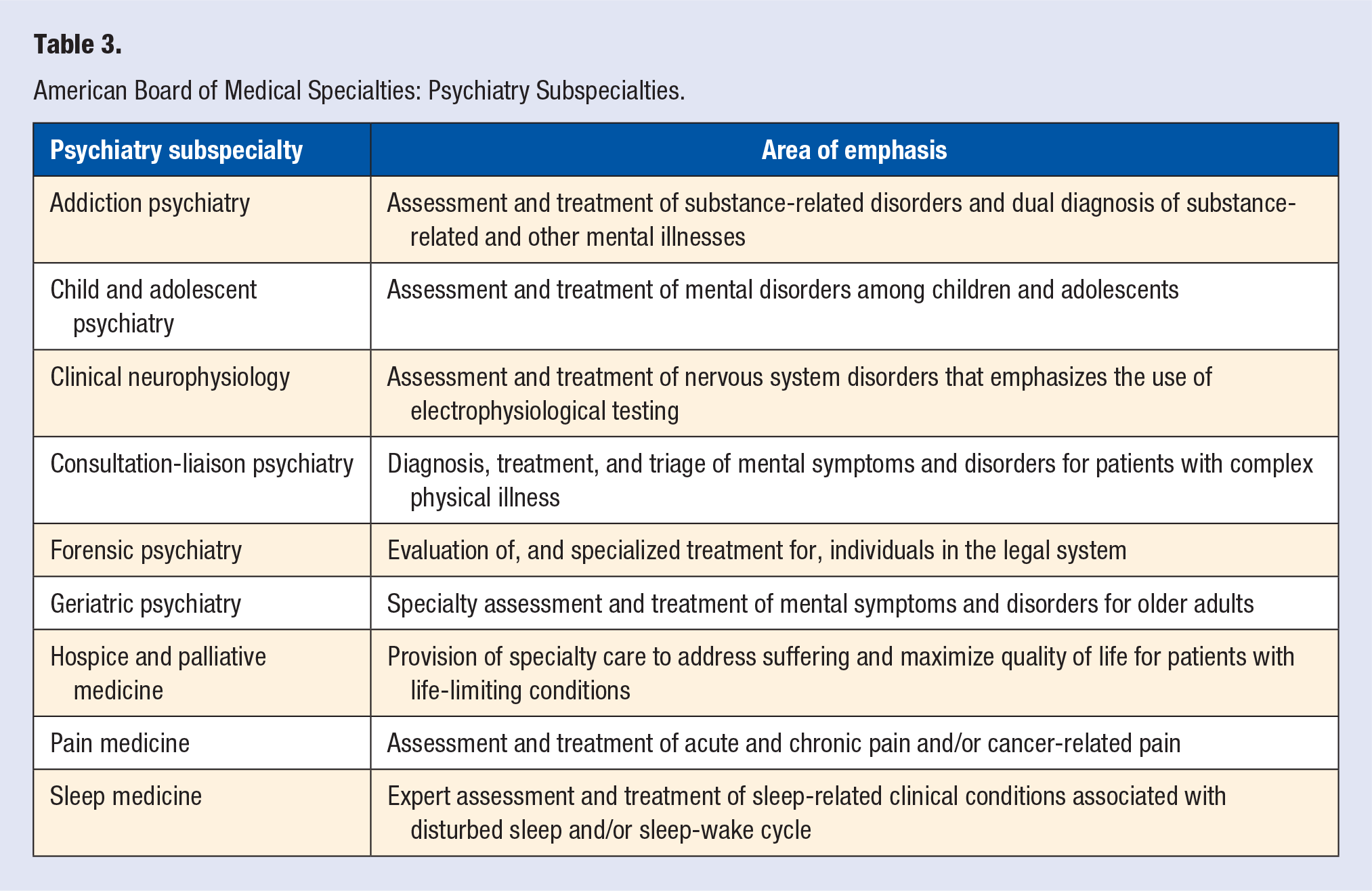
Psychiatry joined the American Board of Medical Specialties (ABMS) in 1935. 17 Over the past 85 years, the field has developed a robust body of literature as well as several ABMS subspecialties of psychiatry practice, including sleep medicine and addiction psychiatry (Table 3). Understanding and differentiating among these important, and often interchanged, definitions and areas of specialization, is an important foundation for the integration of mental and behavioral health understanding within lifestyle medicine.
American Board of Medical Specialties: Psychiatry Subspecialties.
Scope of the Problem
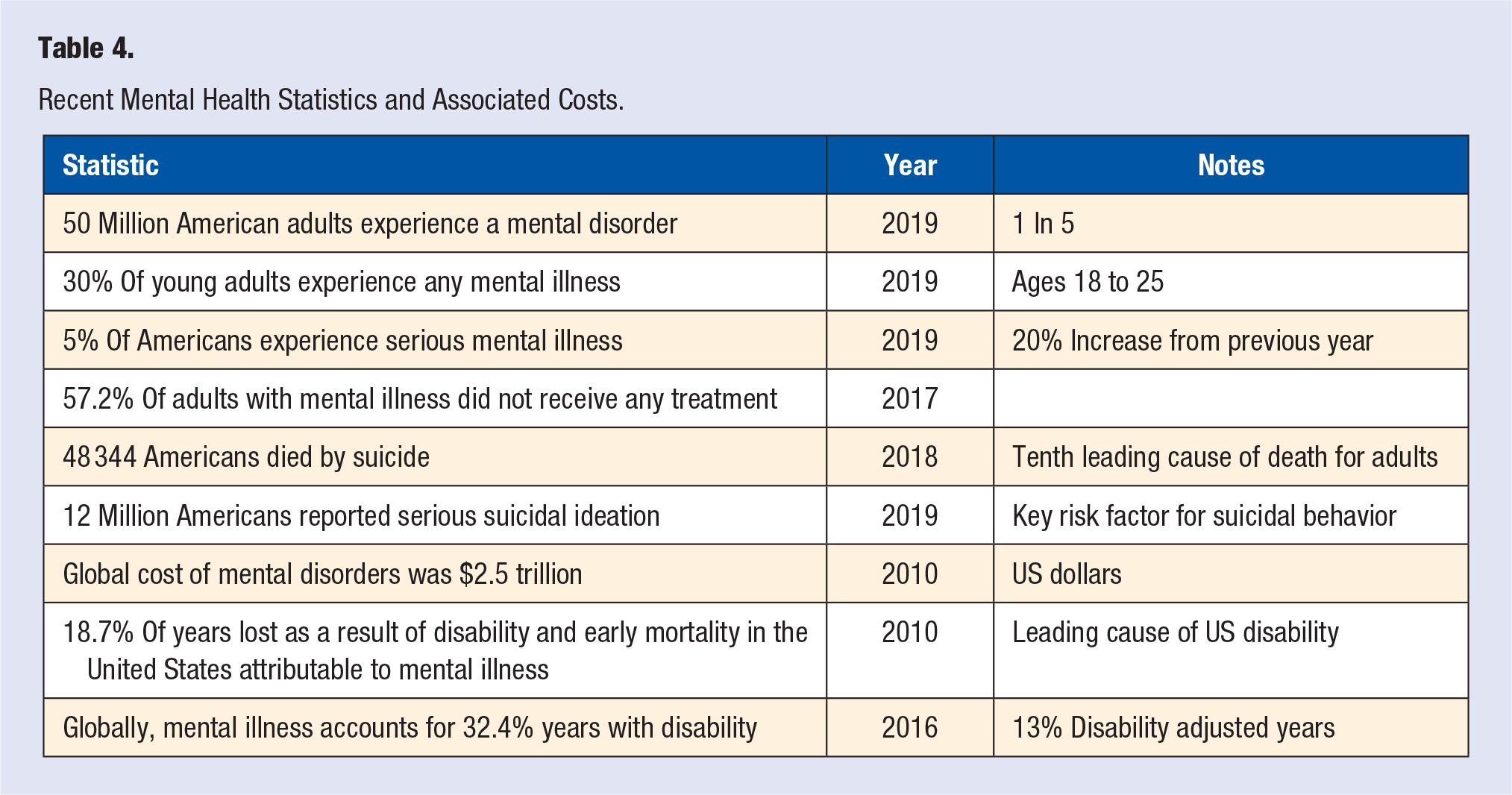
As of 2019, more than 50 million, or 1 in 5, American adults experienced a mental health condition. Young adults, 18 to 25 years old, appear to be especially affected, with almost 30% experiencing any mental illness in 2019. 18 Almost 5% of people experience a severe mental illness, such as schizophrenia. 19 Even prior to the psychosocial impact of the COVID-19 pandemic, rates of mental health conditions have continued to rise in the United States, with a 20% increase in incidence from 2017 to 2018. 19 However, according to the National Institute of Mental Health, less than half of people with mental health conditions sought treatment in 2019, whereas almost 25% of people with a mental illness reported that their treatment needs were unmet, a statistic that has not changed over the past 10 years.18,19
A dangerous and impactful aspect of mental health is suicide. Over the past 20 years, rates of suicide have demonstrated a continuous annual increase, with men almost 4 times as likely to die by suicide as women. 20 Despite the focus on homicides in the media, approximately 2.5 more people die from suicide each year than from homicide. 21 As of 2018, suicide was the tenth leading cause of death among adults in the United States. Even more striking, it was the second and fourth leading causes of death for people 10 to 34 years old and 34 to 54 years old, respectively. 21 Even prior to the COVID-19 pandemic, suicidal ideation, an important risk factor for suicidal behavior, has also been on the rise. 19 In 2019 alone, 12 million Americans reported serious suicidal ideations, with approximately 3.5 million people making a plan to end their lives22,23 (Table 4). In sum, mental illness and suicide have a profound impact on the quality of life of a large proportion of Americans and their loved ones. Thus, it is important to appreciate the threshold for symptoms of mental illness, such as depression or anxiety, and the extent to which they affect functional status and daily life.
Recent Mental Health Statistics and Associated Costs.
The Cost of Poor Mental Health
To meet criteria for a clinical mental disorder, symptoms must be associated with distress and/or an impairment in daily functioning, such as in work, relationships, or daily hygiene. Whereas many people experience mood symptoms, it is the impact on functional status that often differentiates a diagnostic condition. Distress, impairment of functional status, and mental health symptoms, in combination, are associated with significant cost and disability.
The World Economic Forum has previously sought to quantify the costs associated with mental health by considering the loss of human capital, direct and indirect economic impact, and individual costs (ie, out-of-pocket medical expenses). As of 2010, the global cost of mental disorders was estimated at 2.5 trillion US dollars, with more than half of this cost associated with indirect costs, such as loss of income and productivity. These costs, in turn, affect a country’s economic growth because the rate of lost economic growth associated with mental health morbidity and mortality is comparable to other medical conditions such as CVD. 24 The costs associated with mental illness, serious mental illness in particular, are more than just economic. Mental illness has been shown to affect life span, educational attainment, and employment. 25 The leading cause of disability in the United States, is in fact, psychiatric conditions, which account for almost 20% of years lost attributable to disability and early mortality. 26 On a global scale, mental illness accounts for 32.4% of years lived with disability and 13.0% of disability-adjusted years. 27 Further contributing to the cost and disability burden is the frequent overlap between mental and physical health conditions, particularly chronic diseases.
The relationship between physical and mental health is bidirectional and is affected by both direct and indirect effects. A 2017 study on the relationship between physical and mental health found that past mental health has a significant direct effect on physical health, 8% of which was directly attributable to physical activity, whereas 13.6% was indirectly attributable to social interaction. The reverse is also true: past physical health has a direct effect on mental health, with 7.5% of this relationship directly accounted for by physical activity and further indirect impact from social interaction and smoking cessation. 28 Thus, lifestyle factors and health behaviors play key roles in both physical and mental health and their overlap, and this relationship is true to both acute and chronic medical conditions.
Mental Health and Physical Health: Important Overlap
Serious and chronic medical conditions are inextricably linked with mental health symptoms, as well as treatment engagement, and recovery from both mental and physical health conditions. Altered immune responses (e.g., amplified inflammatory responses) have been suggested as one key biological mechanism linking mental health to physical health conditions. Indeed, inflammation may be a key mechanism underlying CVD among individuals with mental health symptoms. For example, individuals with higher depressive symptoms three months after the death of a spouse had higher levels of proinflammatory cytokines than those with lower depressive symptoms.29 The relationship between mood symptoms, such as depression, and CVD is also bidirectional, with mood conditions associated with exacerbated risk for CVD, and CVD diagnosis, symptoms, and treatment associated with increased risk for depression, anxiety, and traumatic stress. 30 Research suggests similar findings for other serious and chronic medical conditions, such as diabetes, cancer, and chronic pain. Additionally, mental health plays a critical role in prevention and health maintenance because affective symptoms are well understood to interfere with adherence and optimal health behaviors. 31 Research suggests that individuals with comorbid mental and physical health conditions are higher utilizers of acute care, including emergency departments, and are more likely to be rehospitalized within 30 days of hospital discharge. 32
The relationship between mental health and health behaviors, specifically psychosocial risk factors, is particularly salient to substance use. Despite declining rates of tobacco use in recent years, almost 50 million Americans were current smokers in 2019, with approximately half of those individuals smoking daily. Additionally, millions of American report regular cigar, pipe tobacco, and/or smokeless tobacco use. 22 In 2019, approximately 5% of the US population met criteria for an alcohol use disorder, whereas almost 5 million people met criteria for marijuana use disorder. 22 These staggering numbers do not account for all substance use.
Furthermore, individuals with mental health conditions are more likely to be high utilizers of substances, in part as a maladaptive coping mechanism. For example, in 2016 almost 34% of adults diagnosed with any mental health condition reported tobacco use, which is more than 10% higher than the base rate for individuals without a mental health condition. 33 Adults who smoke tobacco are also more likely to engage in heavy alcohol use or binge drinking, misuse prescription medications, and use marijuana and illicit substances. 33 Although all substance use disorders are important to consider for both physical and mental health, this article will focus on tobacco use, in alignment with the American College of Lifestyle Medicine’s pillars of lifestyle medicine.
In summary, the global impact of mental disorders is significant. Good mental health is critical for optimal health behaviors, effective and sustainable lifestyle change, and overall quality of life. Thus, mental health not only plays a critical role in lifestyle, including each of the pillars of lifestyle medicine, but specifically addressing mental disorders may be critical to the efforts of lifestyle medicine as a field.
Mental Health Considerations for Lifestyle Medicine
Lifestyle factors, such as diet and stress, are key contributors to mental health and play an important role in the prevention, etiology, and management of mental disorders. Emerging literature, consistent with well-founded behavioral medicine research and practice, suggests that lifestyle medicine interventions that emphasize some or all of the pillars of lifestyle medicine may be well suited to prevent the onset, reduce the symptoms, and slow the progression of mental health symptoms and disorders. As noted by Catherine Collings in a 2020 article published in the American Journal of Lifestyle Medicine, whereas much of the emphasis of lifestyle medicine practice has been on nutrition, the area with the most evidence-based work to date, there remains much opportunity to continue to develop the other pillars. 34 Furthermore, as outlined below, there is significant opportunity within the field of lifestyle medicine to effectively incorporate the bidirectional relationships between mental health and each key area of lifestyle medicine. The sections below will thus describe key mental health studies and their applications to the 6 pillars of lifestyle medicine.
Diet and Nutrition
Numerous studies suggest that diet and nutrition contribute to the incidence of mental health conditions, such as depressive disorders. 35 There appear to be 4 major mechanisms by which diet affects psychological health: the gastrointestinal (GI) microbiome, inflammation, epigenetics, and the effects of macronutrients and micronutrients.
Gastrointestinal Microbiota
Numerous studies have indicated a bidirectional interaction between the GI microbiome and the brain, with pathways through the nervous and endocrine systems, as well as through immune pathways. 36 Research suggests that substances produced by the GI microbiome may enter the brain through the bloodstream, and the brain can influence the microbiome through neuronal pathways as well as lifestyle behaviors. Although multiple neurotransmitters are thought to affect these neuroendocrine pathways, tryptophan, the precursor to serotonin, appears to have the greatest impact on mental health. The understanding of the relationship between the GI microbiome and mental health is in its infancy, but emerging research has begun to highlight the significant effect of environmental factors and dietary behaviors on the composition of a healthy intestinal microbiome. For example, higher intake of refined carbohydrates, sugar, simple carbohydrates, and alcohol have been associated with less microbiome biodiversity. 37
Interestingly, the composition of the GI microbiome for patients with depression has been shown to be different from that of nondepressed patients in human and rodent studies. Similarly, some studies have found that individuals who suffer from specific mental disorders, such as schizophrenia and bipolar disorder, have less microbiota diversity, which may have important treatment implications. 38 Furthermore, lower microbiome diversity and global community differences in GI microbiota have been noted in a review looking at schizophrenia and bipolar affective disorders. 39 One study found that the transplantation of fecal content from patients suffering from schizophrenia into rodents, resulted in worsening of psychomotor activity and dysfunctions in learning and memory. These studies point to the promising possibility that addressing the GI microbiome will have positive implications for mental health.
Among individuals with generalized anxiety disorder, improvement in the diversity and health of the GI microbiome through the introduction of probiotics has been associated with reduced symptoms of anxiety and lesser perceived stress. 38 Social stress has also been noted to specifically influence the composition and diversity of the GI microbiome. 40 Such changes may be mediated by the neuroimmunological and neuroendocrine mechanisms of the central and autonomic nervous systems that control key GI processes. Furthermore, individuals with mental disorders are diagnosed with comorbid functional GI disorders at greater rates than the general population, further indicating the important relationship between brain and GI health. 41
Of note, many of the current treatment modalities available for depression and anxiety disorders involve chemicals that regulate mood in the brain, many of which originate from the amino acid, tryptophan. 42 Tryptophan is produced by enterochromaffin cells in the GI tract, and its availability may be regulated by the gut microbiota. Tryptophan is also metabolized into many of the chemicals that are substrates of many psychotropic medications. 42 Similarly, the gut microbiome is implicated in producing numerous other neurotransmitters, such as GABA, dopamine, serotonin, and norepinephrine, which have implication for mental disorders. 43 As research continues to understand the GI microbiome and the complexities of the gut-brain axis lifestyle interventions may play an important role in the prevention of mental disorders and/or potentiate the need for medications.
Inflammation
Attention to the role of inflammation in health outcomes and disease has increased exponentially in recent years. Based on recent findings, it appears likely that an inflammatory response related to diet is associated with an increased risk of developing, or worsening, symptoms of depression and anxiety. The problematic implications of a proinflammatory diet on mental health are thought to occur secondary to neuronal damage from neuro-oxidative stress and inflammation. 44 Thus, dietary patterns and specific food types have been studied for their relationship to biomarkers that indicate inflammation and resulted in the development of measures such as the Dietary Inflammatory Index (DII). 45 A 2018 study found that a proinflammatory diet, as assessed by the DII, was associated with greater risk of symptoms of anxiety and depression as well as lower overall well-being. 46
There are also modifiable factors, such as omega-3 fatty acid intake, that are understood to contribute to, or exacerbate, inflammatory pathways. Eicosapentaenoic acid (EPA; omega-3 fatty acid) is a precursor to anti-inflammatory eicosanoids and has been found to modulate neurochemicals in the brain. 47 A double-blind clinical trial found that supplementation with EPA was associated with lower incidence of mental disorders, including depression and schizophrenia. 48 Additionally, excess adiposity has been associated with increased production of the proinflammatory leptin and tumor necrosis factor α. 47
Epigenetic Effects
Epigenetic changes are an important pathway by which lifestyle changes may exert their physiological effects. Epigenetics refers to the processes and structures that regulate how DNA is packaged and transcribed within the cell. The epigenome, which consists of various chemical markers, attached to genes and associated histone proteins, responds to intrinsic and extrinsic environmental factors and causes differential expression or inactivation of genes. Therefore, the epigenome represents a mechanism by which certain pathologies may arise without the alteration of DNA itself.49,50 Growing evidence suggests that a wide variety of diseases are linked to epigenetic changes, including many cancers, cognitive dysfunction, autoimmune disorders, and mental disorders. 51 Unhealthy lifestyle behaviors may influence the onset and progression of many diseases through epigenetic mechanisms. On the other hand, healthy lifestyle behaviors have been shown to result in health-promoting gene expression through epigenetic regulation. The field of nutritional epigenetics has made significant headway in elucidating the effects of diet on gene expression, whereas the effects of other lifestyle factors have been less studied. Given the role of epigenetics in the development and severity of mental disorders, and the relationship between diet and epigenetic mechanisms, it is expected that diet may play an important role in mental health outcomes from an epigenetic lens, and more research in this domain is warranted.
Nutrient Imbalances
Based on the current state of the literature, it appears that diet may affect mental health at the micronutrient and macronutrient levels. Nutrients are essential cofactors for the production of the neurotransmitters that are critical to mental health. For example, tyrosine is a necessary precursor to the production of dopamine and norepinephrine, with cofactors of iron, tetrahydrobiopterin, pyridoxal phosphate, and ascorbic acid. A deficiency in any of these nutrients may lead to a deficiency in critical neurotransmitters in the brain. Thus, typical treatment utilizes medications to modulate imbalances and/or deficiencies in neurotransmitters. Similarly, insufficient levels of vitamin D, an essential vitamin, has been associated with depression and seasonal affective disorder, and research has suggested that vitamin D supplementation is associated with decreased depressive symptoms. 52 Although there is a nutraceutical market for pure amino acids, with the intention that they will positively affect key neurotransmitters, such supplements are neither a regulated nor evidence-based treatment.
Much of the research on nutrition and mental health has focused on the importance of omega-3 fatty acids, which include EP, α-linolenic acid, and docosahexaenoic acid (DHA). Although there are insufficient trials of the effects of supplementation of omega-3 fatty acids for the prevention and treatment of mental disorders, research has strongly suggested that an omega-3 deficiency is associated with increased risk for the development of depression, bipolar disorder, schizophrenia, attention deficit disorder, and neurocognitive disorders (dementia). 53 Deficits in EPA and DHA are especially linked to the development of mental health conditions, and studies assessing the efficacy of supplementation for mood are beginning to emerge. 53 However, the National Institutes of Health recommends people get as many of their nutrients as possible from food. 54 Whereas the typical American diet includes an overabundance of dietary fat, a Western diet also tends to include omega-6 fatty acids at many times greater amounts to omega-3 fatty acids when the optimal ratio is 1 to 1. The implications of this imbalance are thought to exacerbate omega-3 deficiency and has been associated with low mood, hostility, and even substance use disorders. 55 Again, more research is warranted to better understand such a potentially important relationship. Overall, promising research on the relationship between diet/nutritional factors and mental health continues to emerge and is expected to grow with further trials and epidemiological research.
Dietary Patterns
Research has also begun to understand the impact of broader dietary patterns on mental health. For example, a 2010 study that compared a “traditional” diet that emphasized fruits, vegetables, whole gains, and lean meats was associated with lesser incidence of depression and anxiety disorders, as compared with a “Western” diet that included processed foods, refined grains, sugar, and alcohol. 56 Although the exact mechanisms that account for such a relationship between dietary pattern and mental health outcomes are unclear, the research emphasizes the importance of better understanding the relationship between diet and mental health. Recent research on the Mediterranean diet, one of the most well-studied dietary patterns, has served as an important foundation for the understanding of the potential benefits of a plant heavy diet to mental health. One study found that participants who moderately adhered to the Mediterranean diet demonstrated a 27% reduction in risk for depression, whereas those who demonstrated a high level of adherence reduced their risk of depressive episodes by 32%. 57 Although much work remains to well understand and leverage diet for mental health, there is a sufficient foundation to appreciate that diet and mental health are inextricably connected and should be mutually considered within ongoing lifestyle medicine research.
Exercise
Many studies have demonstrated a link between physical activity and brain health as well as the positive effects of exercise on mood.58,59 Exercise has been associated with neuroprotective effects and is thought to play a role in the etiology and treatment of mental health disorders through processes such as neurogenesis, angiogenesis, and synaptogenesis as well as structural changes. For example, functional magnetic resonance imaging studies have indicated increased volume of gray and white matter volume throughout the brain following exercise. 60 Exercise appears to affect the hippocampus, a limbic system structure that is critical for learning and memory, which has been specifically associated with increased neurogenesis. 61 Similarly, angiogenesis (neural blood vessel growth) may occur in the context of physical activity and improve cognition by allowing for increased blood flow and cortical blood supply. 62
Although the precise mechanism by which these neurological changes occur is not fully understood, evidence indicates that the role of increases in neurotrophic factors, such as insulin-like growth factor and brain-derived neurotrophic factor (BDNF), is critical. BDNF appears to promote neurogenesis, reduce neuroinflammation, and increase white matter volume, all of which may reduce risk for mental health symptoms and disorders. 63 For example, several psychotropic medications (ie, antidepressants, mood stabilizers) have been associated with increased BDNF, whereas stress has been associated with decreased BDNF. Thus, BDNF is thought to play a critical role in the etiology of bipolar disorder.64,65
Given the role of neurological function and change as a foundation for mental health, it stands to reason that the cognitive benefits of movement would extend to benefit mental health more generally. As conceptualized by McAuley and Morris in their 2006 review, 66 mental health status is one of the factors through which physical activity affects quality of life, and psychosocial constructs, such as self-esteem and self-efficacy, allow for the indirect effects of physical activity on quality of life. Physical activity has also been utilized as an effective intervention to improve mental health among individuals with mental health disorders. Results of a 2014 meta-analysis indicated large effect sizes for physical activity for each symptom of depression and schizophrenia. Physical activity was also moderately associated with overall quality of life. 67 Thus, the utility of physical activity as a lifestyle intervention to address mental health symptoms and disorders is promising and should be further explored as the physical activity science and practice is expanded with lifestyle medicine.
Substance Use and Tobacco Cessation
More than 20 million Americans (7.4%) met criteria for an alcohol use disorder in 2019, with even greater numbers engaging in problematic behaviors related to alcohol use. 68 As of 2019, almost 50 million Americans aged 12 years and above (17.5%) reported marijuana use in the past year, with rates as high as 35% among young adults (age 18-25 years). 68 Rates of marijuana use have also increased across demographic groups (ie, race, age) over the past 2 decades, in part as a result of the legalization of recreation marijuana in some US states. Furthermore, there are persistent rates of illicit substance use and prescription medication misuse, all of which is bidirectionally related with mental health.
Regarding substance use, research suggests a causal link between alcohol use disorder and depression, with alcohol use disorder thought to cause increased risk for major depression. 69 Whereas marijuana use has been shown to predict greater risk for a substance use disorder, abstinence from marijuana has been associated with fewer symptoms of alcohol use disorder, anxiety, and nicotine dependence. 70 Although substance use disorders are typically categorized as mental disorders (based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition), any substance use is relevant to mental health. Specifically, many individuals rely on substances to cope with symptoms of mental illness, such as depression, anxiety, and shame.71,72 Although data have yet to emerge, there is documented concern regarding the rates to which individuals have or will rely on alcohol and other substances to cope with the stress of the COVID-19 pandemic. 73
Research to date suggests that cessation of tobacco use is an important modification to reduce risk for mental disorders. 8 Although it remains unclear whether mental illness triggers smoking or if smoking leads to a higher prevalence of mental illness, individuals with mental disorders smoke at much higher rates than the general population. 33 A 2005 meta-analysis found that the international prevalence of smoking was 62% among patients with schizophrenia and 44% for bipolar disorder.74,75 One theory for these high rates is that smoking is a coping mechanism and/or a method of self-medication. 76 However, other studies have demonstrated that smoking is associated with an increased risk of mental illness, including depression, anxiety, panic disorder, and schizophrenia.77-80 In a meta-analysis of more than 50 000 adults, smoking significantly increased the prospective risk of depression over 1 to 6 years. 81 Regardless of the direction of etiology, individuals who smoke are at increased risk of vascular diseases and associated neuropsychiatric effects.
Research on the effects of smoking cessation for individuals with mental illness has been promising. A meta-analysis of longitudinal studies of adults diagnosed with a mental disorder found that across 26 studies, smoking cessation was associated with decreased symptoms of anxiety, depression, and self-reported stress. The authors also noted that those who stopped smoking tobacco (for at least 6 weeks) also experienced improved mood and overall quality of life. Interestingly, the effect sizes reported in the meta-analysis were equal to or greater than the effect sizes for treatment with antidepressant medications. 82 Attending to mental health and individual health beliefs regarding tobacco use is critical to successful tobacco cessation and continued abstinence. A qualitative study of the barriers to smoking cessation found that participants with a variety of mental disorders and comorbid nicotine dependence reported themes in key expectations that smoking cessation would result in anxiety exacerbation, worsening state of mental health, and loss of a critical coping mechanism as well as loss of a pleasurable activity. 83 As the authors noted, an individual’s perceived risk-benefit analysis regarding tobacco cessation is an important driver of motivation and self-efficacy and especially relevant for those managing mental health symptoms.
Interpersonal Relationships
As is recognized by lifestyle medicine, a healthy lifestyle does not occur in isolation, and the benefits of close relationships for health and well-being are well documented. The famous Grant Study, a 75-year longitudinal study designed to examine the predictors of healthy aging, found that interpersonal relationships had the greatest impact on satisfaction with life. 84 Quality relationships and adequate social support may also help people better cope with stress and have been associated with delays in mental and physical decline for older adults. For example, research has indicated better health outcomes for individuals with long-term partners, and the quality of one’s partnership (marriage) across the life span has been found to be associated with a range of health outcomes, including mental health. 85 Whereas the benefits of quality interpersonal relationships are many, the detrimental effects of isolation are just as prevalent.
Social isolation has been of particular concern during the COVID-19 global pandemic. Research continues to emerge on the implications of the months-long social isolation, but previous studies indicate that social isolation is associated with worse mood symptoms, loneliness, helplessness, and overall decline of mental health. 86 Emerging research has indicated that COVID-19–related social isolation has been especially detrimental for the mental health of older adults, who have experienced increased rates of anxiety, depression, and worse sleep quality. 87 Deficiency in social relationships has even been associated with inflammation and impaired immune function, which as previously noted, is highly relevant for brain health. Furthermore, a seminal study found that even after controlling for confounding factors, such as socioeconomic status and health behaviors, those with the fewest social ties were at more than twice the risk of death compared with those with the most social ties. 88 Thus, the quality of and access to interpersonal relationships are critical to mental health and warrant more study and attention within lifestyle medicine, particularly in an era of increased reliance on technology and less in-person social interaction.
Stress Management
The implication of stress for health, quality of life, and functional status are vast. Exposure to stress throughout the lifetime, or chronic stress, has been shown to be cumulative and correlated with the prevalence of mental disorders. Studies suggest that chronic stress can result in changes in hypothalamic-pituitary-axis regulation, which has implications for serotonin transmission as well immunosuppression, which may be responsible for the development of depressive symptoms. 89 Exposure to acute stress is associated with transient increases in systemic inflammation. Importantly, the stress response system may be enhanced in the presence of mental health symptoms. For example, individuals with more depressive symptoms exhibited enhanced inflammation in response to a standardized laboratory stressor compared to those with fewer depressive symptoms. 90 A whole field of work, psychoneuroimmunology, has emerged in an effort to better understand the complex interactions between brain structure and function, the immune system, and psychophysical health that often plays out in the form of mental illness. 91
Importantly, despite individual differences in perception of stress, chronic stress is well understood to exacerbate risk for mental illness. Chronic stress has been understood to disturb many physiological systems, including immune, digestive, cardiovascular, and reproductive, which in turn may influence mental health. In fact, individuals who suffer from chronic health conditions, such as chronic pain, for which management is stressful, experience greater than normative rates of disorders such as depression. 92 The literature has also linked chronic stress to the onset of major depressive disorder, bipolar disorder, and posttraumatic stress disorder, and it is thought to play a role in treatment-resistant mood symptoms. Also of note, the relationship between stress and mental health begins early in life. A great deal of work has linked early life stressors, often called adverse childhood events in research, to poor mental health outcomes. A 2013 review of 44 studies, found that traumatic early life experiences, such as abuse and neglect, were associated with mood and anxiety disorders, whereas emotional abuse was also associated with schizophrenia and personality disorders. 93 Such research indicates the long-term implications of early-life stressors on mental health, which is likely to also have important implications for lifestyle and quality of life. Thus, the identification of stressful early-life experiences, chronic stress throughout the life span, and individual coping strategies, including health behaviors that support stress management (ie, yoga), is critical for mental health and prevention of illness. Effective management of stress, and mitigation of chronic stress, may help delay the onset and progression of symptoms of mental illness. Future research to better understand the neural and endocrine pathways that contribute to the stress response, and its chronic activation, will lead to better prevention and further development of effective evidence-based treatments that support mental health and address mental illness.
Sleep
Sleep is an often overlooked, yet critical aspect of lifestyle because it influences each of the other aspects of lifestyle medicine. In fact, with emerging evidence of sleep being an independent risk factor for mental health and neurological disorders, psychiatrists and neurologists with sleep expertise have called for further study of, and intervention for, sleep-wake disorders. 94 Sleep is not only critical for maintaining healthy biological function, but also there is a likely bidirectional relationship between sleep and mental illness. Sleep problems, including insomnia, obstructive sleep apnea, circadian rhythm disorders, restless leg syndrome, and insufficient sleep (quality and quantity), have been associated with impaired cognition, dysregulated mood, and poorer immune function. 95 Furthermore, sleep disturbance plays a role in most mental disorders. 96 Because sleep is such a vital biological process for maintaining physical and mental well-being, sufficient quantity and quality of sleep is crucial for the management of mental health symptoms. For example, disrupted sleep is a common symptom of depression as well as a diagnostic criterion for major depressive disorder. 12
In addition, many psychiatric medications interfere with sleep onset and maintenance, which can further exacerbate underlying mood and cognitive symptoms. 97 Thus, ensuring healthy sleep is not only important for symptom reduction, but also to reduce the burden of psychotropic medication for the many people who rely on medications to manage mental disorders. Some providers argue that sleep should be the first addressed issue because poor and/or insufficient sleep has implications for dietary pattern, energy to engage in physical activity, ability to manage stress, psychological energy for engagement in interpersonal relationships, and engagement in healthy coping mechanisms. The lifestyle medicine pillar of sleep would benefit from consideration of the implication of sleep for mental health as well as the significant influence of mental health on sleep duration and quality.
The Path Forward
With approximately one quarter of American adults experiencing a mental disorder, and even more experiencing mental health symptoms, attention to mental health is more relevant than ever. 18 The current article provides an overview of the bidirectional relationship between mental health and lifestyle medicine. Key mental health definitions, and statistics outlining the impact of mental health on disability, mortality, and quality of life, were provided as foundation for understanding the imperative of recognizing and addressing mental health within lifestyle medicine. Based on such critical information, the current article serves as a call to action for both individual providers and the field of lifestyle medicine to effectively incorporate mental health into practice across all pillars. Furthermore, to meet the needs of all people, lifestyle medicine research and practice must be tailored to those who suffer from mental illness, which may require a unique framework, beyond the scope of the very valuable and useful coach approach.
With the burgeoning of lifestyle medicine, now is the time to address the inclusion of mental health and persons with mental disorders. As addressed above, there is foundational research connecting each of the key areas of lifestyle medicine with facets of mental health, and each pillar appears to have a unique bidirectional relationship with quality of mental health, mental health interventions, and even treatment outcomes. To exclude mental health and persons with mental disorders, could be analogous to the exclusion created in response to the 1910 Flexner report and subsequent closure of most historically black medical schools, which has resulted in a dearth of Black physicians, a contributing factor to the significant health disparities experienced by Black Americans. 98 As lifestyle medicine lays the foundation for a new, more sustainable approach to medicine and overall health and well-being, inclusive practices will be critical to the growth and influence of the field. As this effort moves forward, well-studied mental health conceptual frameworks, which serve as a foundation to mental health diagnosis and treatment, can be utilized to conceptualize mental health within lifestyle medicine and address mental health symptoms and disorders from a lifestyle medicine perspective.
Although many gaps remain in lifestyle medicine science, particularly the overlap between mental health and lifestyle medicine, members of the field have an important opportunity to continue to grow and develop research and clinical practice in a way that incorporates mental health and provides for individuals with mental illness. Such goals may be best achieved with the strategic inclusion of, and collaboration with, psychiatrists, other physicians, and allied health providers, such as health psychologists, who have expertise in both mental health and lifestyle change. Leveraging such expertise among lifestyle medicine providers to specifically address mental health will be consequential to the development of the field of lifestyle medicine.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.