
Abstract

. . . a case for lifestyle medicine (LM) can be made for delivering improved patient outcomes, establishing cost savings, . . .
For a health care system, achieving high value in patient care by delivering health care that offers improved health outcomes at a lower cost remains the ultimate goal. Health care systems that are self-insured face the additional challenge of the increasing economic burden of managing chronic diseases among their covered lives. In addition, safety net hospitals are required to offer care to their uninsured and underinsured populations.
In the United States, over $1 trillion is spent annually on suboptimal behaviors, 1 thus highlighting the enormous need to both promote changes in lifestyle behaviors and reduce health care costs. With growing momentum toward value-based care, 2 a case for lifestyle medicine (LM) can be made for delivering improved patient outcomes, establishing cost savings, and creatively tapping into millions of dollars assigned to population health initiatives. The objective of this article is to describe the successful implementation of an LM philosophy at Midland Health (MH), a self-insured health care system in Texas. Specifically, we will describe how the return on investment in LM is more through revenue saved rather than revenue collected.
Why Implement LM?
Reducing health care spending calls for a focus on disease prevention in healthy populations and early disease reversal in chronically ill populations, 3 both of which can be achieved through lifestyle change. In 2014, MH redefined its mission, vision, and values, and this helped incorporate LM concepts into the broader initiative philosophically. The vision was being the “Leading healthcare for greater Midland” with a mission of “Making Midland the healthiest community in Texas.” There were 4 key reasons why MH began to move toward an LM approach.
1. Midland Health is self-insured
First, MH is self-insured and, in 2016, exceeded its budget for benefits costs by 3 million dollars, which resulted in an opportunity to offer the Complete Health Improvement Program (CHIP), which is an evidence-based, employee wellness program promoting a “whole health” approach aimed at preventing and reversing disease through lifestyle changes. CHIP, which has been documented in detail and offered for over 30 years, 4 is an 8-week program encompassing 18 sessions focusing on stages of lifestyle change, illustrating the benefits of change, and providing tools to maintain lifestyle change. While offering CHIP, the burden of chronic disease among MH employees has decreased, and less money was spent on chronic diseases such as diabetes, hypertension, coronary artery disease, hyperlipidemia, arthritis, and some cancers. First, MH conducted a formal study among 30 CHIP participants, and results showed improvements in biometrics, less reliance on prescription medications, and in some cases, reversal of disease among CHIP participants. Such data allowed us to concretely demonstrate to hospital administrators that LM could succeed at MH.
By implementing CHIP, MH concurrently created a broader “culture of health” that included lectures for CME credit encouraging clinicians to use LM, a “Food is Medicine” annual seminar that attracted over 500 people, and an online wellness portal for employees. Furthermore, whole-food plant-based options were included in the hospital cafeteria and on inpatient menus, and “Forks Over Knives,” an empowering documentary highlighting the health benefits of plant-based nutrition, was played on loop in the hospital for patients to watch. MH opened a community garden, arranged wellness tours and lectures in the community, and published newspaper articles to promote LM philosophies.
2. Midland Health was in the process of forming a clinically integrated network
The hospital was forming a clinically integrated network (CIN) to both lower the cost of the hospital employee benefit plan and improve health outcomes by promoting population health, clinical integration, and care coordination, which involves sharing information and organizing care among all individuals involved in the patient’s care to promote greater safety and effectiveness. These changes, combined with use of generic prescriptions and changes in the benefit plan that put the onus on employees by encouraging them toward ownership of their health with a higher deductible plan while offering lifestyle programs, yielded an astonishing 3 million dollars in savings in 2018. Most notably, in 2018 compared with 2017, there was a nearly 19% reduction ($2 million) in hospitalization costs and 29% reduction ($1 million) in pharmacy expenses.
3. Create a financially viable business model
Offering lifestyle-based intensive cardiac rehabilitation programs (ICR), LM clinics, and LM-based shared medical appointments (SMAs), with an established reimbursement model provides for a financially viable business model. Our system currently offers the LM clinic programs illustrated in Table 1.
LM Clinic Offerings and Associated Patient Costs at MH.
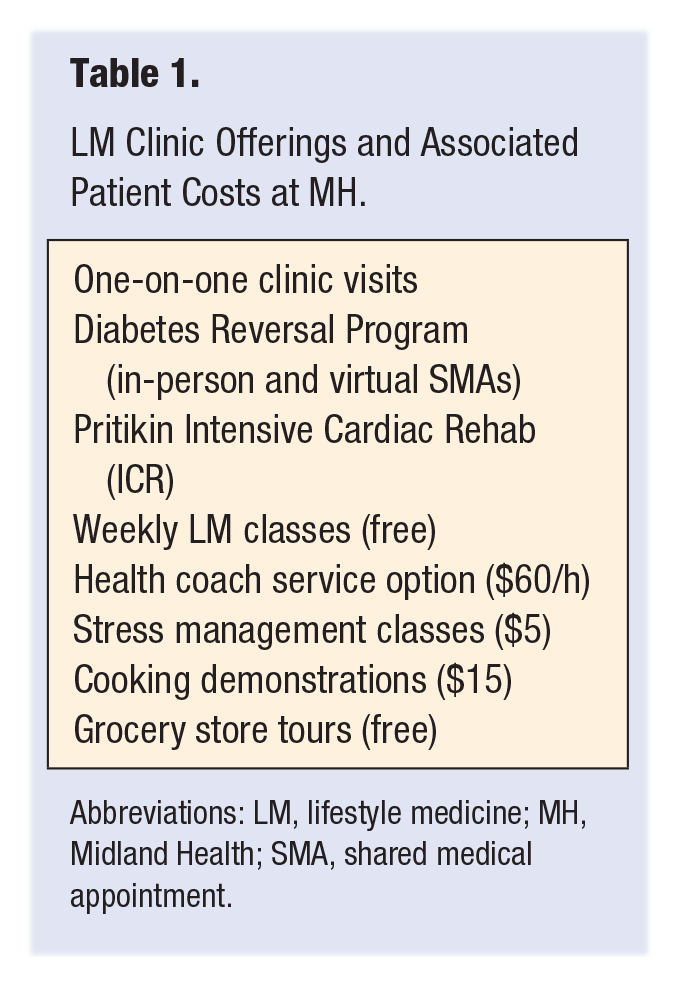
Abbreviations: LM, lifestyle medicine; MH, Midland Health; SMA, shared medical appointment.
In addition to the clinic offerings, MH also offers Pritikin Intensive Cardiac Rehabilitation Program (ICR). We recommend that every hospital consider an ICR, as heart disease is the number one killer in the United States, yet only 10% to 20% of eligible patients receive cardiac rehabilitation referrals. This highlights a huge potential to be capitalized upon. Medicare reimbursement is $110 per hour, which for traditional cardiac rehabilitation (36 hours) amounts to $3960. In contrast, ICR is 72 hours, resulting in a $7920 per patient reimbursement, which both financially benefits our network and improves the quality of health care offered to the patient. In terms of resources, we restructured our LM program to streamline staffing needs, thus saving costs. Table 2 illustrates LM staffing numbers after the restructuring.
MH Staffing for LM Program Implementation, After Restructuring (2020).
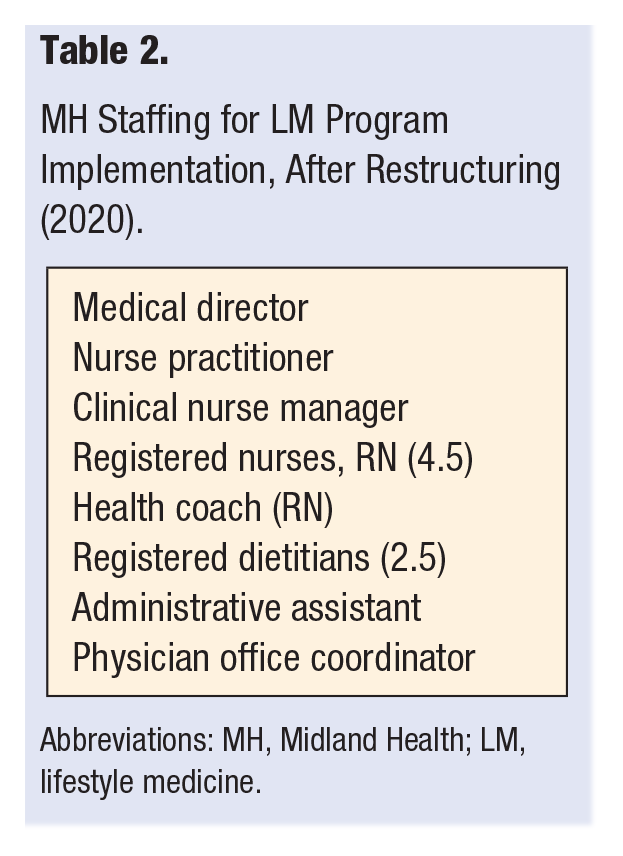
Abbreviations: MH, Midland Health; LM, lifestyle medicine.
Reimbursement models are moving away from fee-for-service and more toward value-based care. In 2021, it is predicted that the proportion of business aligned with pay-for-performance, bundled payments based on quality of care, rather than separate payments to each provider, and population-based payments will increase. Aligning with value-based reimbursement models has the potential to provide a longer term, more financially viable business model.
4. Improve equitable care and population health
Social determinants of health (SDOH) inevitably influence patient outcomes. In order to truly improve outcomes and promote greater equity, medical care, particularly in emergency department (ED) settings, must incorporate social and behavioral components. 5 Incorporating members within an LM team with specialized skill sets to focus on social needs would help link patients to valuable resources. 6 LM provides an enormous opportunity to work toward improving equity in care. First, a significant opportunity exists to grow unfunded and underfunded patient programs by identifying at-risk populations to better manage health and wellness by addressing SDOH. Second, we can identify and intervene among patients with frequent ED visits. Third, we can work to prevent hospital admissions and readmissions by providing resources to manage chronic health conditions. This includes providing outreach to patients identified as needing interventions to manage chronic conditions.
Data show that efforts aimed at improving equity in care have been successful at MH. In 2019-2020, ED visits dropped by approximately 50% after identifying the needs of these patients and offering them assistance, education, resources, and access. This is critical in our network because, as our community’s safety net hospital, we are obligated to see all patients regardless of ability to pay. Targeting patients with LM approaches improves outcomes for patients, reduces cost of care, and generates savings for our network.
Moving Forward
Following the great success of our LM program since 2018, MH is now looking for additional ways to grow the program. Potential strategies include utilizing direct-to-employer health care programs, through which MH would partner directly with providers, rather than insurance companies, to exercise greater control over benefits and cost of care. Also, the Centers for Medicare and Medicaid services offer shared savings programs such as the Medicare Shared Savings Program, by which eligible providers are incentivized to improve health at the individual and population levels, as well as lower health care costs.
Tapping Available Resources: Established Population Health Incentive Programs
Value-based care can financially benefit health care systems if they utilize state and federal population health incentive programs. MH has generated substantial revenue from these programs, as illustrated in Table 3. In total, 10% of MH annual funding stems from population health incentives. There is remarkable untapped potential for other health systems to similarly utilize such incentives. For example, in Texas, $3.1 billion has been allocated to the Delivery Service Reform Incentive Program (DSRIP) and $600 million to Quality Incentive Payment Program (QIPP). In 2021, legislators will discuss merging funding from these programs into a single entity using the same general metrics focusing on improving quality of care, reducing costs, and promoting greater care coordination.
Successful Utilization of Population Health Incentive Programs at Midland Health (MH).
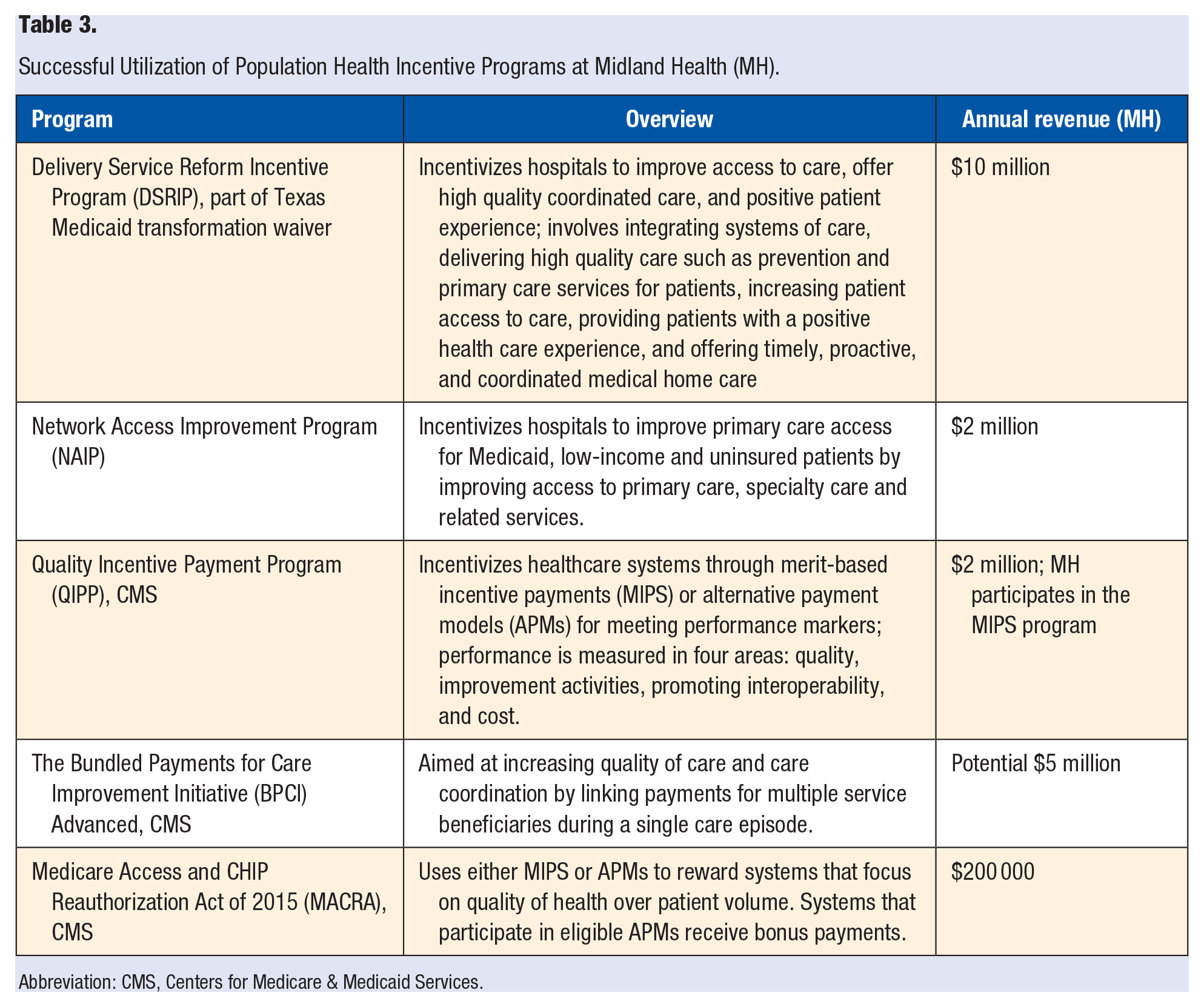
Abbreviation: CMS, Centers for Medicare & Medicaid Services.
Conclusion
Value-based care typically relies on 2 components: (1) bundling services rather than individual billing for services and (2) rewarding providers for meeting value-driven performance metrics. 7 The success of the LM program at MH demonstrates the great potential for value-based care, rooted in LM, to improve health and drive down health care costs. Pronovost et al 1 describe similar success by which a framework to eliminate defects in care and align incentives reduced annual per-member-per-year cost by 9% over the course of 12 months. This framework aimed to incentivize stakeholders toward a common purpose, including incentivizing employees toward evidence-based lifestyle changes and providers toward greater value. 1 Gulati et al 3 detail strategies to consider in creating value-based plans, many of which were implemented at MH, including required LM-based nutritional intervention programs, coverage for ancillary services such as nutritional counseling and behavioral health services, and required, comprehensive LM education programs for patients with lifestyle-associated chronic disease.
At its core, LM models provide incredible benefits for patients by offering resources to promote wellness and lifestyle improvements, in addition to focusing on disease prevention and treatment rather than costly and burdensome disease treatment. Funds assigned to population health initiatives are increasing, and LM provides great potential for cost-savings if available resources are capitalized upon. Integrating LM into a health care network can be successful and generate both savings and revenue by assigning already available population health funds to LM programs. To fix the broken US health care system, one in which providers and hospitals are more highly incentivized to treat rather than prevent disease, 1 integrating LM principles within healthcare systems is fundamental.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.