
Abstract
Keywords
It seems logical that medical school curricula would consider including education about the role of lifestyle to prevent and treat chronic disease.
Introduction
The United States spends a staggering $3 trillion on chronic disease care, 1 which is the most of any industrialized country, but life expectancy ranks in the bottom quartile in a comparison of nations. 2 According to the World Health Organization, 80% of chronic diseases such as coronary artery disease, stroke, hypertension, dyslipidemia, type 2 diabetes, and obesity could be prevented primarily through improvements to diet and lifestyle. 3 It seems logical that medical school curricula would consider including education about the role of lifestyle to prevent and treat chronic disease. However, lifestyle medicine (LM) is only taught in a minority of medical schools.4-6 In this article, we describe a pilot project of introducing a brief LM course taught within the Mayo Clinic Alix School of Medicine (MCASOM). The main purpose of the course was to introduce the students to LM as a specialty practice and to provide students with foundational knowledge of healthy lifestyle habits. The goal was not only to enhance students’ personal health and well-being, but also to better equip them during their first-year health coaching practices.
Background
The absence of LM training in medical school may have long-term negative consequences for medical professionals and patient outcomes. It has been reported that a significant cohort of physicians recognize having a low confidence level to effectively counsel healthful nutrition, exercise, and stress management, even though they believe that it is their duty to educate patients about these health behaviors.7,8 They frequently feel insufficiently prepared to adequately self-manage their own health behaviors while practicing medicine. Medical practice is considered to be one of the most stressful careers, with the highest suicide rate of all professions 9 and one of the highest rates of career burnout. 10 Burnout often begins in medical school. 11 Furthermore, broad absence of LM training can adversely affect patient outcomes because physicians’ own health-promoting practices (or lack thereof) may predict whether physicians counsel patients about the benefits of a healthful lifestyle.12,13 In contrast, those who live a healthful lifestyle themselves counsel LM more frequently.14-17 A longitudinal study following more than 11 000 participants suggests that an individual’s lifespan increases with the adoption of each primary health behavior (eating 5 or more fruits and vegetables daily, exercising regularly, consuming alcohol in moderation, and not smoking). 18 Research has shown that including LM training in the medical school curriculum results in a greater likelihood of physicians engaging in personal health-promoting behaviors and counseling patients regarding such behaviors.19,20 Additionally, patients are more willing to engage in a healthful lifestyle when their physicians model these behaviors. 21 They view physicians as the most trusted source of health-related information and, therefore, when LM is prescribed, consider them to be a credible source to inspire motivation for change.12,22,23 To improve patient adherence to lifestyle behavior change, physicians should have communication skills based on behavior change science such as motivational interviewing and health coaching (HC). 24
In 2019, the MCASOM in Arizona piloted a curriculum development project to introduce LM training into the medical school education. All 49 first-year students participated in an 11-hour LM course, spread over 3 days, as part of the Science of Healthcare Delivery. The course was taught by a multidisciplinary team of clinician medical educators. Students also participated in a course in Health Coaching. The LM course focused on several pillars of health behavior, which included classroom education in nutrition (5 hours) and exercise (4 hours) as well as stress management and sleep hygiene (2 hours). Course content was taught using the flipped classroom method, 25 in which students completed prereading and/or online learning to prepare for discussion of key teaching concepts during the instructional class time. The assigned amount of prework was based on 10% of the scheduled class time. The flipped classroom model empowers students to begin the learning process before the class and lays a foundation to support interactive practical applications of the content rather than didactic education, 26 which, in turn, improves time efficiency. 27 In this pilot project, flipped classroom teaching was adopted to more readily engage students in the process of making healthful decisions about their own lifestyle. Students were also expected to improve HC skills to promote LM. We discuss both the HC and the LM curriculum below.
Health Coaching
In addition to the LM curriculum, all first-year medical students at MCASOM participate in HC throughout the entire first year. This course is taught by a physical therapist who is a certified health and wellness coach. Integrating HC into a more traditional medical school curriculum is considered value added: students develop professional competence as they learn about methods of health care delivery. 28
The HC curriculum combines in-person classroom instruction (6 hours) with supervised practice both in large and small groups (4 hours), 5 online modules combined with independent peer coaching (5 hours), and client coaching (5 hours). Mayo Clinic employees volunteer as clients, and the students provide HC that is relevant to the client’s needs rather than simulated role playing. Students learn strategies to support health behavior change, using HC methods with an emphasis on patient-centered communication, shared decision-making, and motivational interviewing.29,30 In previous years, prior to the client coaching practice, students had expressed that although they felt confident with the coaching communication techniques, they lacked specific knowledge about a health-promoting lifestyle. The goals of our LM course were to increase students’ confidence in both their coaching skills and also their foundational knowledge of exercise, nutrition, sleep, and stress management—all typical topics addressed during client coaching sessions.
Overview of Lifestyle Medicine Curriculum
Prior to the LM course, students (1) watched a 10-minute Introduction to LM video, 31 (2) read an article outlining physician competencies for prescribing LM, 32 and (3) completed a brief LM assessment survey to create awareness about their personal lifestyle behaviors. The course started with a 30-minute overview of chronic disease as the leading cause of death and disability, the economic burden of chronic disease, and the impact of different risk factors for premature death, including specific health behaviors and social determinants of health. This was followed by an introduction to the 6 pillars of LM (healthful eating, exercise/physical activity, stress management, healthy relationships, restorative sleep, and avoidance of substance use) using infographics from the American College of Lifestyle Medicine (ACLM). 33
Nutrition
According to the Global Burden of Disease Study, 34 the largest study of disease risk factors in history, an unhealthy diet is one of the leading causes of chronic disease and premature death in the United States.35,36 Therefore, physicians’ most important tool may be competency in nutrition and ability to educate patients about the basics of nutrition. Unfortunately, only 25% of medical schools require a single course in nutrition. 37 And more concerning yet, many physicians feel that they have more understanding of nutrition than they actually do. 38 Therefore, advancing nutrition education in medical school ought to be valued as a justifiable and prudent objective.
Our nutrition curriculum focused on preventing, reversing, and treating chronic disease, with an emphasis on evidence-based whole foods plant-based diets. Health-promoting diet education was provided with the purpose of guiding students’ shift toward healthier eating patterns and teaching them how to educate patients about health-promoting diets. The curriculum was a mixture of lecture and small-group interactive instruction. Topics included a comparison of popular diets (including whole-food plant-based, paleo, keto, and Mediterranean diets), fasting, tips and tricks for busy students to create healthful meals, how to identify evidence-based whole-food plant-based resources, label reading, and a virtual grocery store tour. We set out to make our curriculum as interactive as possible by creating activities to help the students effectively learn the material. For example, we asked them to write a healthy diet prescription for one another and to plan a day of health-promoting meals on a student budget. Students were asked to watch one of the following documentaries on their own time: The Game Changers, Escape Fire, or Forks over Knives. Then, these films were discussed in class. We also provided a whole-food plant-based lunch for the students from a local plant-based meal service.
Exercise
Per a 2012 study in The Lancet, “In view of the prevalence, global reach, and health effect of physical inactivity, the issue should be appropriately described as pandemic, with far-reaching health, economic, environmental and social consequences (p.227).” 39 The authors concluded that physical inactivity may cause 1 in 10 premature deaths worldwide, and if physical activity increased by 25%, more than 1.3 million deaths worldwide could be averted every year. Furthermore, deaths attributable to a physically inactive lifestyle are now nearly equal to those from smoking, giving rise to the saying, “Sitting is the new smoking.” 39 The 4-hour exercise portion of this course focused on the evidence for exercise and physical activity as medicine and for cardiovascular fitness as well as the importance of strength, balance, and flexibility. 40 The difference between physical activity and exercise was clarified. In addition to using exercise as medicine for chronic disease, students were introduced to the evidence for targeted exercise as an effective treatment for many specific musculoskeletal disorders, often as or more effective than injected analgesics or steroids or a surgical alternative. 41 In addition to instruction, students were provided with personal assessments and hands-on physical examinations such as 12-minute run test and tests for strength, flexibility, and balance/proprioception. Students also learned how to calculate a target heart rate, how to create an exercise prescription, 42 and the importance of documenting a Physical Activity Vital Sign 43 in the electronic health record. Emphasis in wellness coaching principles such as “the patient as the expert in their life,” motivational interviewing, and exploration of exercise options, all helped address anticipated challenges of adherence. Students were encouraged to consider their own personal exercise routine, to ask future patients about exercise, and to encourage exercise at every clinic visit. The team-based approach was emphasized, including the importance of collaboration with professionals with expertise in exercise, such as physical therapists, exercise physiologists, physical trainers, and wellness coaches. Students were encouraged to investigate and utilize resources such as the websites Exercise is Medicine 44 and ACLM. 45
Sleep and Stress Management Combined
In our LM curriculum, we combined restorative sleep and stress management, 2 of the 6 components of LM, into a single class. Prior to this class, students read about the effects of melatonin on the circadian rhythm 46 and millennial medical student stressors, 47 and they also completed the ACLM’s Perceived Stress assessment instrument. 48
According to the Centers of Disease Control, 1 in 3 adults do not get enough sleep. Lack of sleep may contribute to several chronic diseases and conditions, including type 2 diabetes, heart disease, obesity, and depression. 49 Sleep has been described as one of the foundations of LM because of its effect on mood, motivation, focus, and decision-making. 50 Our sleep curriculum included the impact of sleep on the nervous, endocrine, and cardiovascular systems, health risks of chronic sleep deprivation, and strategies for optimal sleep. Because medical students are at higher risk for sleep deprivation, 51 we shared evidence showing that high-quality sleep may improve grades and performance in medical school. 52 We also addressed specific barriers to getting enough good quality sleep both during their medical school years and during residency. These include the high intensity and long duration of their study, overnight on-call duties, the emotional challenges of the work, and lifestyle choices. 53
The stress management component addressed the definition of stress, eustress versus distress, the stress response, the effect of chronic stress on physical and mental health, symptoms of stress, and strategies to enhance resilience and create a sense of well-being. Students also learned about the wide range of conditions that may be worsened by chronic stress, including cardiovascular disease, hypertension, dyslipidemia, type 2 diabetes mellitus, headaches, inflammatory arthritis, anxiety, and depression. 54 Mindfulness and meditation were addressed with emphasis on “on-the-spot” mindfulness techniques. Students participated in guided mindfulness practices such as 1-minute breath awareness. In addition to learning how to better manage their own stress, students also learned about the effect of chronic stress on their future patients. Because almost 50% of adults suffer adverse effects of stress and between 75% and 90% of all primary care visits are for stress-related ailments, 55 future health care providers must be equipped with effective tools for stress management not only for themselves, but also for their patients.
Students’ Self-assessments and Feedback
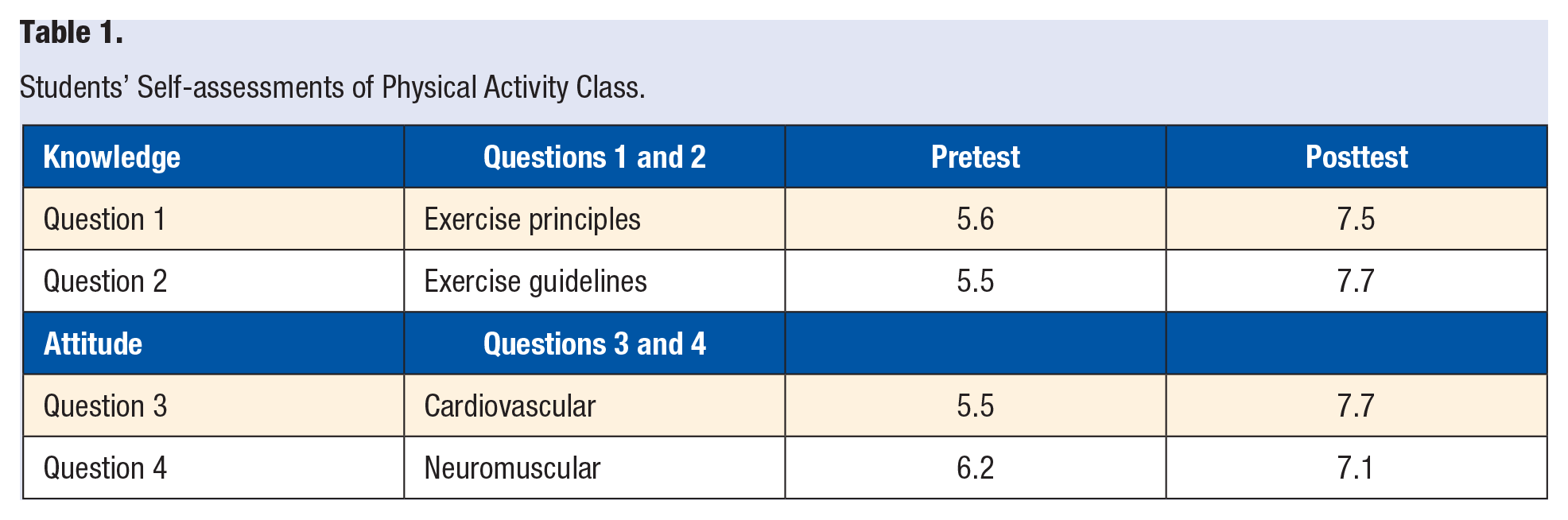
All 49 course participants were asked to complete a 4 question pretest and posttest for the exercise class. The questionnaire was designed on a 10-point Likert scale, with “0” representing “not at all” and “10” representing “very well” (please see attached questionnaire in the appendix). In all, 28 evaluations were completed at baseline and 27 were completed on completion of the class. Two questions were knowledge based and asked how much students understood the principles of exercise prescription and the exercise guidelines for health and fitness. The other 2 questions were attitude based about students’ sense of whether their own personal aerobic fitness and personal neuromuscular fitness was satisfactory for their age/gender. The intent of these pretest and posttest surveys was to help the faculty improve the teaching process.
Students’ responses showed improvement for each question, as noted in Table 1. The greatest improvement was in understanding the exercise guidelines and students’ sense of satisfactory personal aerobic fitness.
Students’ Self-assessments of Physical Activity Class.
In addition to the physical activity evaluation, all students were emailed an optional survey with 3 questions about what they had learned overall from the LM course, if they had made any lifestyle change based on the information, and how the curriculum could be improved. Again, the purpose of this assessment was to assist faculty with quality improvement for potential future classes. This email was sent 8 months after the course, and a total of 4 students responded. The following are quotes from the feedback from this limited pool of responses: “I think all of the topics that were presented were so informative and so important for our medical education.”
With regard to the nutrition component, a student commented that they were surprised a whole-food plant-based diet was health promoting. They noted a shift in their appreciation for legumes stating that they were “eating way more beans” and particularly “darker legumes because they contain more antioxidants.” Additionally, another student responded, “the teachings on beans were a great reminder of their wealth of nutrients and the[ir] unique phytonutrients.”
Another reported other improvements in their own nutrition: “I purchase more dark, green leafies, and I’m more cognizant of just how bad fast food is for me.” Finally, another student commented, “I do not have the same appetite for meat as I had before.”
Students seemed to find the label-reading portion of the nutrition component the most useful for themselves and for being teachable to their future patients. They also mentioned that they hoped that the nutrition curriculum could become more interactive, similar to the exercise portion.
About the exercise component, 1 student said, “It was really interesting to participate in the exercise testing and see how my own health compared to my expectations. A 12-minute run doesn’t sound terrible, but doing it was harder than I bargained for. It was also interesting to see how medical students performed on a routine exercise test, especially if we will be sending our patients for these tests in the future.” They enjoyed the personalized focus of this topic and stated, “I loved this part! I have never had someone test my flexibility, measure my leg length, etc. so I was very excited and engaged (especially because it was about my own health!).” Additionally, students highlighted the connection between what they were learning about their own fitness and how it might pertain to their future patients’ fitness. One student noted that “lifestyle changes can sometimes be just as good or better than medicine (like exercise for depression).” And, finally, this introduction piqued students’ curiosity and left them wanting to understand more about prescribing exercise, such as “I think it would be really helpful to know how to create and recommend specific types of exercises and routines for patients as a starting point.”
With regard to the sleep and stress management component, students appreciated feeling that their instructor was actively helping them learn to manage their stress. Ideally, they will use these techniques with their future patients. A student noted, “I love when you lead a meditation (to date you are the only teacher we’ve ever had who took a minute to have us breathe/meditate/check in with ourselves)!”
Of those students who responded to the survey, all stated that they saw the value in these classes. One summary comment included, “I think that all of the information was so valuable. I think the most relevant—if the content has to be condensed—diet, food label reading, exercise, meditation/sleep with a focus of each of these on how to instruct patients about how to carry them out.” Furthermore, some students made numerous healthy lifestyle changes as a result of the instruction. One student noted, “I have gone back to eating mostly plant based whole food and think it has really helped me feel healthy. I also try to make time in the morning to do 20-30 minutes of exercise. We meditate before bed, especially when stressed, to help improve sleep quality. I also feel much more informed when shopping.” Finally, about 6 months after our course, another student stated, “I switched to a plant-based diet and started exercising more . . . I’ve lost about 20 pounds since then.”
Strengths and Weaknesses
Our original intent of this course was to assess its feasibility and to better understand how future iterations might fit into our ongoing medical curriculum. We share the strengths and weaknesses of our course in hopes that it might be of use to those considering creating a similar course at their school. Strengths of this curriculum included the flipped classroom approach, which was particularly effective for maximizing discussion given limited classroom time. The in-person classroom setup made it feasible for students to pair up during the physical activity section and for instructors to provide feedback on technique. The students who responded to our questionnaire seemed to appreciate the importance of what they were learning. Another strength of the course is that because of their new knowledge of LM, several students formed an LMIG (Lifestyle Medicine Interest Group) in partnership with ACLM.
We also recognize limitations of our curriculum and reporting of the pilot. First, because LM is a specialty of substantial breadth and depth, attempting to summarize the most impactful lessons of LM into 11 hours was challenging. Because of time limitations, we had to omit teaching about many key studies as well as the LM pillars of healthy relationships and substance use avoidance. Furthermore, our informal survey yielded a low return. A pretest and posttest for each section of the course would have provided more reliable quantitative data. The authors intend to conduct formal research on educational outcomes of the curriculum in the near future.
Conclusion
In summary, students were introduced to LM and its impact not only on their own lives, but also on that of their future patients. Not surprisingly, practicing physicians already recognize the value in LM, and nearly all agree that lifestyle needs to be taught in medical school.56-58 We postulate that the value of LM will continue to gain wide acceptance among clinicians and that it will take its proper place in all health care curricula.
Footnotes
Appendix
Acknowledgements
Thank you to Dr Patti Thorn and Ms Joslyn Vaught at MCASOM for their curriculum guidance. We also thank MCASOM leadership for their forward-thinking vision recognizing the value of adding health coaching and LM education into the school’s curriculum.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.