
Abstract
We have previously proposed a list of determinants (causes) of modern lifestyle-related chronic disorders, which provides a structure for the emerging discipline of lifestyle medicine. This consists of lifestyle factors with a common immune biomarker (metaflammation) that interact in a systems fashion linked with chronic disease outcomes. We considered this to be a work in progress and later added 3 psychosocial determinants into the causal mix: meaninglessness, alienation, and loss of culture and identity (MAL). Here, we propose adverse childhood experiences (ACEs) as deeper, or even more distal, disease drivers that may act directly or indirectly through MAL to influence later chronic disease. The links with metaflammation and the need for recognition of these embedded scars in the management of lifestyle-related health problems is discussed.
‘Health-related outcomes associated with ACEs have been shown to include obesity, type 2 diabetes, ischemic heart disease, cancers, depression, addictions, and decreased longevity . . .’
Introduction
Lifestyle medicine (LM) has been defined as “the application of environmental, behavioral, medical and motivational principles to the management of lifestyle-related health problems” (p. 3). 1 It arose, as an adjunct discipline late in the last millennium to help manage the rising incidence of lifestyle and environmentally related chronic diseases in Western societies. At the time, this seemed like a good idea, irrespective of the fact that there was little initially to differentiate LM from standard clinical practice.
To establish a discipline and pedagogy around LM, we proposed 4 categories of comparison with conventional medicine: (1) knowledge: the science; (2) skills: the art; (3) tools: the materials; and (4) procedures: the actions. We suggested, however, that this is a work in progress and therefore open to ongoing modification.
Under 1, the knowledge base, we proposed a number of determinants known to be linked with chronic disease, based on Bradfield-Hill’s 2 criteria for causality in chronic disease epidemiology. Determinants, or drivers, are the main linear forces behind disease causality in chronic conditions. (With chronic diseases—eg, cardiovascular disease, diabetes, cancers—the determinants are not necessarily microbiological, as with infectious diseases, and are therefore not strictly causes. They are therefore less amenable to Koch’s postulates 3 as the causes of infectious diseases.) In LM, determinants have often been reduced to 3 or 4 lifestyle or behavioral factors—for example, nutrition, inactivity, drugs/smoking, and stress—that account for the majority of chronic diseases. However, as we have shown, a number of other clear determinants (inadequate sleep, environment, relationships, social inequity, etc, as shown in Figure 1), although possibly only accounting individually for a small proportion of chronic diseases, interact with other determinants in a systems fashion 4 and hence cannot be excluded from any consideration of causality. To our initial determinants, we recently added 3 extra psychosocial determinants of chronic disease—meaninglessness, alienation, and loss of culture and identity (MAL)—that typically affect individuals, particularly the displaced, alienated, and marginalized, such as indigenous peoples, refugees, and lower socioeconomic groups in modern societies. 5
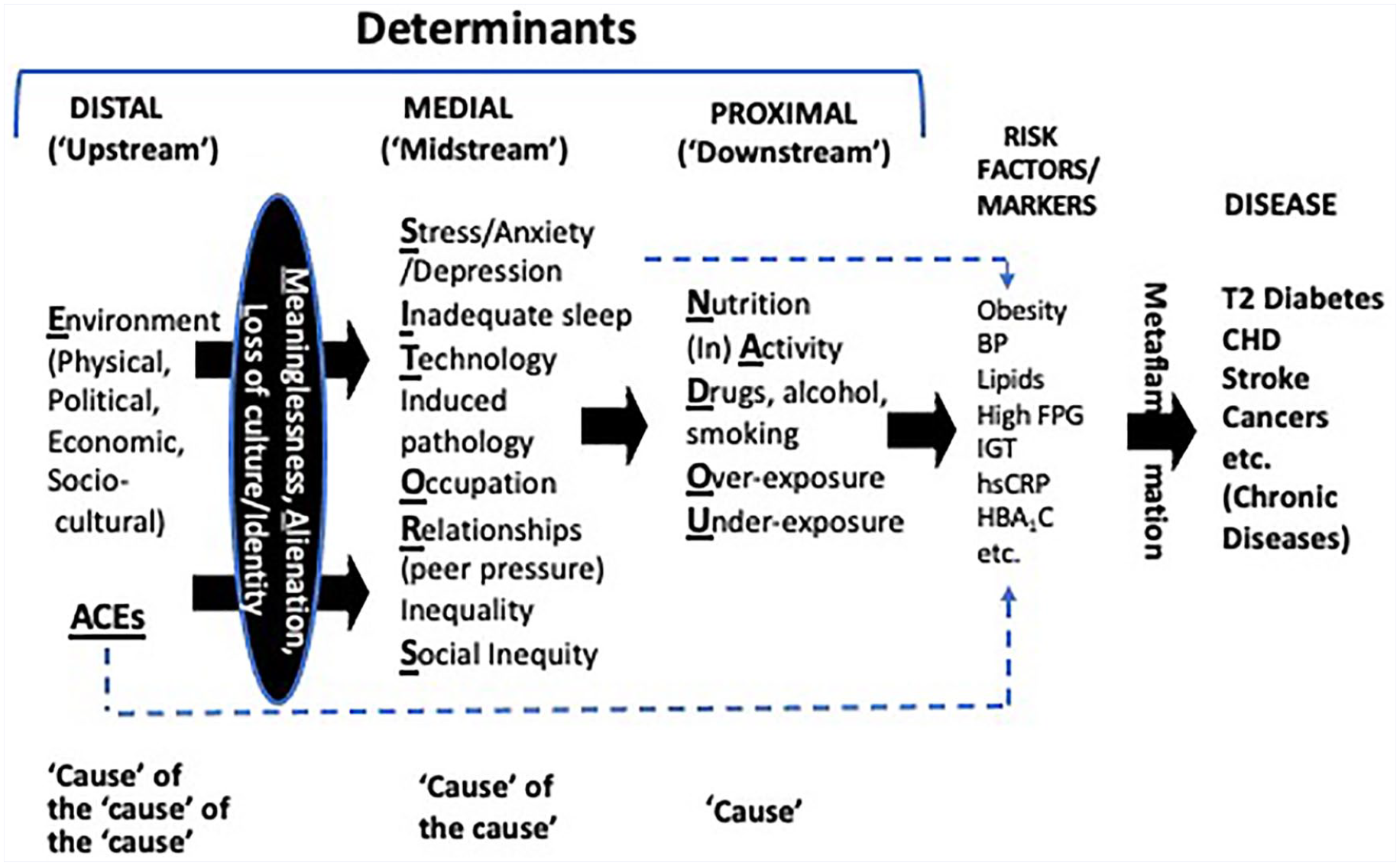
A hierarchy of disease determinants. Underlined letters in bold form the acronym NASTIE MAL ODOURS, which we have previously used 1 to delineate the determinants of lifestyle-related chronic diseases. For detailed explanation, see text.
Such determinants, as well as others identified to date in a causal hierarchy (Figure 1), exhibit evidence of an association with the early stages of an adaptive immune reaction to lifestyle-related inducers.6,7 This is a low-grade, systemic, and chronic form of inflammation (metaflammation or metabolically induced inflammation), initially thought to explain pathologies associated with obesity 6 and that occur in the intima of the arteries but now known to extend systemically throughout the body—kidneys, heart, liver, and so on 8 —and link ultimately with metabolic disorders (eg, oxidative stress, insulin resistance) and end-stage chronic disease. Metaflammation appears to characterize most, if not all, chronic disease determinants related to lifestyle and the environment. 1
In this article, we consider an expansion of the psychosocial determinants initially identified to include an important distal or upstream determinant of the chronic diseases typically associated with lifestyle and environments. Specifically, we have added adverse childhood experiences (ACEs) 9 and provide evidence of a link between ACEs and early-stage immune responses on the causal pathway to chronic disease. ACEs may act independently on biological outcomes (ie, independent of lifestyle), as shown in the dotted line at the bottom of Figure 1, or through the psychosocial (MAL) determinants and/or lifestyle to link with chronic disease. Stress may also act through lifestyle change or independently of lifestyle as shown in the dotted line at the top of Figure 1. Other complex interactions undoubtedly occur in this hierarchy, but we have left this to a further deeper analysis. It should also be noted (although not shown in Figure 1) that although ACEs may not necessarily affect biological risk factors through lifestyle, lifestyle can be a mediator, acting as a buffer and reducing the risks of ACEs on biological outcomes. We conclude that whereas there would be fewer more undisputed associations such as between ACEs and later health in the medical literature, the link has not been fully explored in the context of chronic disease epidemiology. The current article is a scoping perspective for the consideration of such a link, allowing hypothesis creation for further testing. To this extent, we have covered a broad review of the field rather than hone in on specific areas of research, the proposed outcome hopefully being a greater understanding of ACEs as determinants of later chronic disease.
Adverse Childhood Experiences
ACEs are traumatic events that occur early in life (eg, <18 years of age). 12 They can be emotionally painful or distressing and can have a hierarchy of effects that persist into adulthood.9-14 They include categories of abuse (physical, emotional, sexual), neglect (physical, emotional), and household dysfunction (mental disease, incarceration, mother treated violently, substance abuse, divorce).
Although studies linking childhood abuse to later health problems go back to the early days of psychotherapy and beyond, the extent of the problem was only objectified after the US Centers for Disease Control (CDC) and the Kaiser Permanente Association survey of 17 000 people from 23 states in the United States from 1995 to 1997. 15 This showed that up to 62% of adults had experienced at least 1 type of ACE, and nearly 17% had experienced 4 or more types. (A commonly used definition of potentially damaging ACE exposure is having experienced any 4 or more of 10 listed adverse experiences in childhood.) 15 Early studies illustrated the health effects of individual ACEs. However, more recently, it has become clear that cumulative ACEs can have a greater effect on chronic outcomes than single events. 12
ACEs and Chronic Disease
Health-related outcomes associated with ACEs have been shown to include obesity, type 2 diabetes, ischemic heart disease, cancers, depression, addictions, and decreased longevity as well as social outcomes, including unemployment, social dysfunction, and educational attainment.12-16 In a 2017 meta-analysis, Hughes et al 12 calculated odds ratios (ORs) for associations of 23 outcomes of ACEs, ranging from modest (ORs < 2.0) for physical inactivity, overweight, obesity, and diabetes, moderate (OR = 2-3) for smoking, heavy alcohol use, poor self-rated health, cancer, heart disease, and respiratory disease, strong (OR > 3-6) for sexual risk-taking, mental ill-health, and problematic alcohol use, to strongest (OR > 7) for problematic drug use and interpersonal and self-directed violence.
The association of intransigent adult obesity with ACEs is particularly pertinent to public health and clinical interventions such as through LM. This has been well established but is probably a confounding factor on the causal pathway. One systematic review of pooled observational studies linking ACEs to adult obesity, for example, has shown an OR of 1.46 (95% CI: 1.28, 1.64), with lifestyle factors, social disruption, and chronic stress responses being the most frequently mentioned explanation for this. 17
In the seminal CDC study of ACEs, Felitti and Anda 15 found that many cases of obesity (female in particular) did not respond to traditional weight loss methods, because this is often used as a defensive shield against further physical and/or sexual abuse suffered early in childhood. Yet McDonnell and Garbers 17 found a paucity of studies examining this in traditional weight loss and obesity treatments.
Whether obesity is a direct determinant of chronic disease or an associative factor resulting from other determinants (eg, energy overconsumption, inactivity, food environments) is unclear. 18 However, the failure to establish obesity reduction per se as successful in dealing with ACE-related chronic disease outcomes suggests obesity as a symptom and not a cause. Indeed, obesity has been described as a canary in a coal mine, 19 signaling a normal response to an abnormal environment 20 rather than the opposite. For this reason, we do not consider obesity treatment through health behavior changes alone as sufficient for the management of ACE-associated obesity. Just as the correction of distal determinants is necessary for fully managing other “causes of the cause” 21 of chronic disease, dealing with ACEs and MAL should be seen as a vital ingredient of other chronic lifestyle-related disease management.
Pathways
Although originally thought to be confined to obesity, modern lifestyle-related chronic diseases are now thought to be nearly universally associated with chronic inflammation. 22 Low-grade, systemic and chronic inflammation (metaflammation) appears also to be a common characteristic of ACEs (and other lifestyle-related chronic disease determinants), which begins with early childhood exposure to stress or trauma and can persist through midadolescence 23 to adulthood. 24 We have previously suggested that exposure to novel inducers in the modern environment can stimulate an immune response as indicated by an increase in metaflammation. 18 Through further involvement of the nervous, endocrine, and immune systems, this can then become embedded, causing a biological scar, 24 which can involve epigenetic changes of gene expression and have wide-ranging effects on dysregulation of various physiological systems. 25 A number of biomarkers, particularly relating to inflammatory processes (C-reactive protein, interleukin-6, suPAR, fibrinogen, etc26-28) have been identified as common in many, although not all, long-term effects of ACEs (especially those where no adverse later effects have been found). Systemic low-grade inflammation is often seen as a precursor to further allostasis and chronic disease risk.
The importance of this is now being noted in popular books on early experiences and changes in the human brain. Doidge, 29 for example, in The Brain that Changes Itself has explored the plasticity of the developing brain and susceptibility to adverse events, quoting several wide-ranging studies. This has been added to by van der Kolk 30 (The Body Keeps the Score), who presents evidence to show the embedding of these experiences in the adult brain if unchallenged. Burke-Harris 31 (The Deepest Well: Healing the Effects of Childhood Adversity) looks at the epidemiology and neurobiology of the negative effects of toxic stress caused by ACEs and implications for treatment. Without exhaustively listing primary sources referred to here, there appears to be significant evidence supporting the later disease effects of ACEs.
There are also a number of possible pathways for a connection between ACEs, MAL, and end-point chronic disease. However, disruption of homeostasis leading to dysregulation of the immune system as indicated initially by a rise in metaflammation 22 would seem to be a prime area for further investigation. This might develop early in life and be biologically imbedded. 24 However, ACEs may also cause immune dysregulation through changes in health behaviors (nutrition, smoking, stress, inactivity, etc), which have also been shown to have an independent effect on metaflammation through some other mechanism. This has been shown with unadapted lifestyle behaviors or more indirectly through components of the MAL determinants (meaninglessness, alienation, or loss of culture and identity), which have also been shown to be associated with metaflammation and to have an independent effect on chronic disease outcomes. 5 The causal pathway thus becomes complicated, and further investigation would be required to know where intervention may be best targeted.
It is hypothesized, therefore, that ACEs early in life, if untreated, can be distal (deep) determinants of later chronic disease, either directly, through health behaviors, or indirectly through biological scars resulting from the direct effects of MAL. Childhood trauma, for example, as shown even by early psychoanalytical theory, can influence an individual’s concept of purpose or meaning in life and/or cause alienation and loss of culture and identity. 15 The latter could presumably be a result of war, natural disasters, or dispossession of culture, where this can be used to define trauma associated with the displacement of large populations through ethnic cleansing or colonization of indigenous cultures. These can be deeper or more distal drivers of chronic disease either independently or through the medial drivers we have identified here as MAL.
ACEs and Lifestyle Medicine
As a result of the above analysis, we suggest that ACEs be examined further with a view to being added to psychosocial determinants of chronic disease that need to be considered within the purview of LM. There is a logical and experimental link with the MAL determinants. However, individual susceptibility to adverse experiences means that outcomes may vary dramatically, depending on modifiers such as genetics, gender, exposure components, resilience, and possible interventions. This begs the question of where treatment and intervention within LM might be targeted.
As an adjunct discipline, LM is primarily a clinical process. However, because it extends, through environmental influences on health behavior and ACEs, to distal causes shown in Figure 1, it provides greatest potential for correction in doing this if it is seen as a bridge between public health and clinical medicine, as shown in Figure 2—the former to help structure environments in a way that helps support lifestyle and behavior change and the latter to help modify individual unhealthy lifestyle behaviors. Expanded to this level, it also includes aspects of health promotion, combining both population and individual approaches and aspects of regulation and social influence as well as individual and/or parental responsibility within a classic health promotion context, 32 as shown in Figure 2.
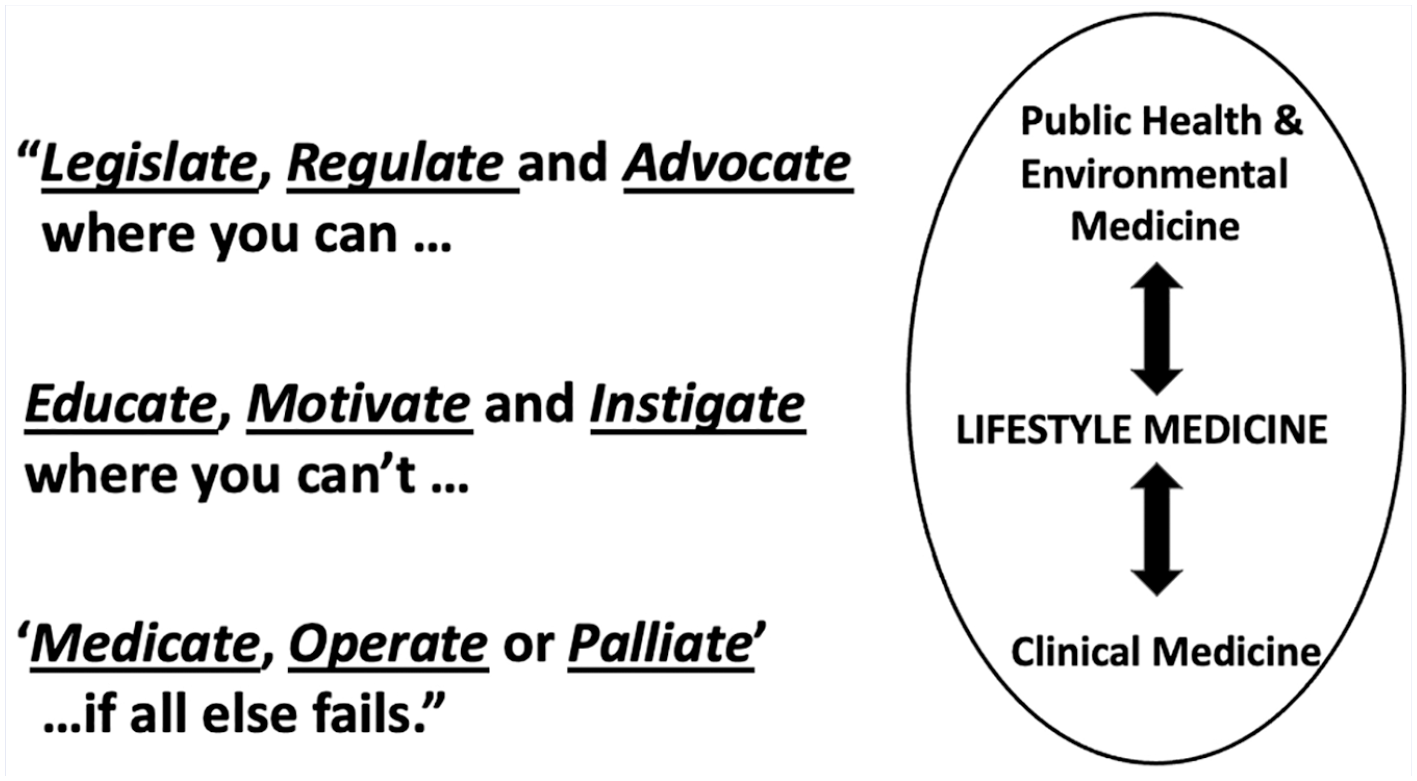
Strategies for intervention: an expanded role for lifestyle medicine.
The first line of Figure 2 focuses on public health initiatives, the second, clinical medicine and LM, bridging the 2 is shown in the middle. It is not the intention here to detail all possible processes for doing this but to offer a structure and some suggestions for dealing with the psychosocial side of a discipline of LM. Dealing with MAL at the medial level from Figure 1 for example, means treating meaninglessness, alienation, and loss of culture and identity, through known processes at the clinical level such as psychotherapy, cognitive behavior therapy (CBT), positive psychology, logotherapy, 33 resilience-informed therapy, 34 and so on.
At the more distal level of the causal pathway in Figure 1 or the top of Figure 2, it can mean the primary and secondary prevention of ACEs through a suite of technical packages 35 at the public health level to prevent violence that adversely effects children. At the level of cultural disruption, it might mean rehabilitation approaches such as cultural prescription, as a form of social prescription, 36 creativity in a cultural context, and cultural emersion, acceptance, pride, and so on. Movements such as Black Lives Matter are a process for doing this, but so also may be processes, formal or informal, such as encouraging indigenous art, learning new skills, volunteering, or political or community involvement, all of which can help fill an existential vacuum, which Frankl 33 sees as the underpinnings of logotherapy. Irrespective of type of intervention, it is clear that management of ACEs is an important process of LM, given the apparent potency of such experiences in later chronic disease determination.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.