
Abstract
Chronic disease epidemiology currently lacks the mono-causal focus germ theory provides infectious diseases. However, the discovery of a form of low-grade, systemic, and chronic inflammation (“metaflammation) underlying many, if not all, chronic diseases induced by a range of stimulants labeled “anthropogens” may help change this. Anthropogens are “man-made environments, their by-products, and/or lifestyles encouraged by these, some of which are detrimental to human health.” While an exhaustive list of anthropogens associated with chronic disease may be as elusive as a comprehensive list of “germs” with the potential to cause infection, a broad taxonomy provides a focus for the practice of lifestyle medicine. Such a list is considered here under the acronym NASTIE ODOURS.
‘The concept of a lifestyle and/or environmentally based cause of disease leads only to a general understanding of chronic disease etiology.’
The crossover from infectious to chronic disease dominance in developing countries, otherwise known as the “epidemiological transition,” 1 provides the impetus for a discipline of lifestyle medicine. 2 Yet the concept of a lifestyle and/or environmentally based cause of disease leads only to a general understanding of chronic disease etiology. It does not provide the mono-causal focus afforded to infectious diseases with the development of germ theory in the 19th and early 20th centuries. 3 As a consequence, multicausality remains the dominant approach to chronic diseases leading to a “silo” system of disease management—heart disease, type 2 diabetes, cancers, and so on—with little underlying common thread other than a broad environmental–“lifestyle” related etiology.
The discovery of a common element in the form of low-grade, systemic, and chronic inflammation (“metaflammation”) in the early 1990s, 4 and recognition of this as underlying much, if not all, modern chronic disease,5 -8 provides an opportunity for a better epidemiological understanding of chronic disease as a whole, and hence greater opportunity to reach beyond the “silos” for the practice of lifestyle medicine. Research over the last decade shows that metaflammation is induced by a range of factors broadly considered under the concept of “anthopogens.” 9
Anthropogens and Lifestyle
The term anthropogens has been used to describe “man-made environments, their by-products and/or lifestyles encouraged by these, some of which may be detrimental to human health.” 9 Several authors have identified a range of anthropogens through their metaflammatory effects on humans7,10 -13 We have proposed an evolutionary explanation for this in suggesting that pro-inflammatory anthropogens have arisen as a consequence of, and since the industrial revolution, and as such are “inducers” (in contrast to antigens) of a different form of immune inflammatory reaction leading initially to oxidative stress, inflammation, and dysmetabolism, 14 as shown in Figure 1.
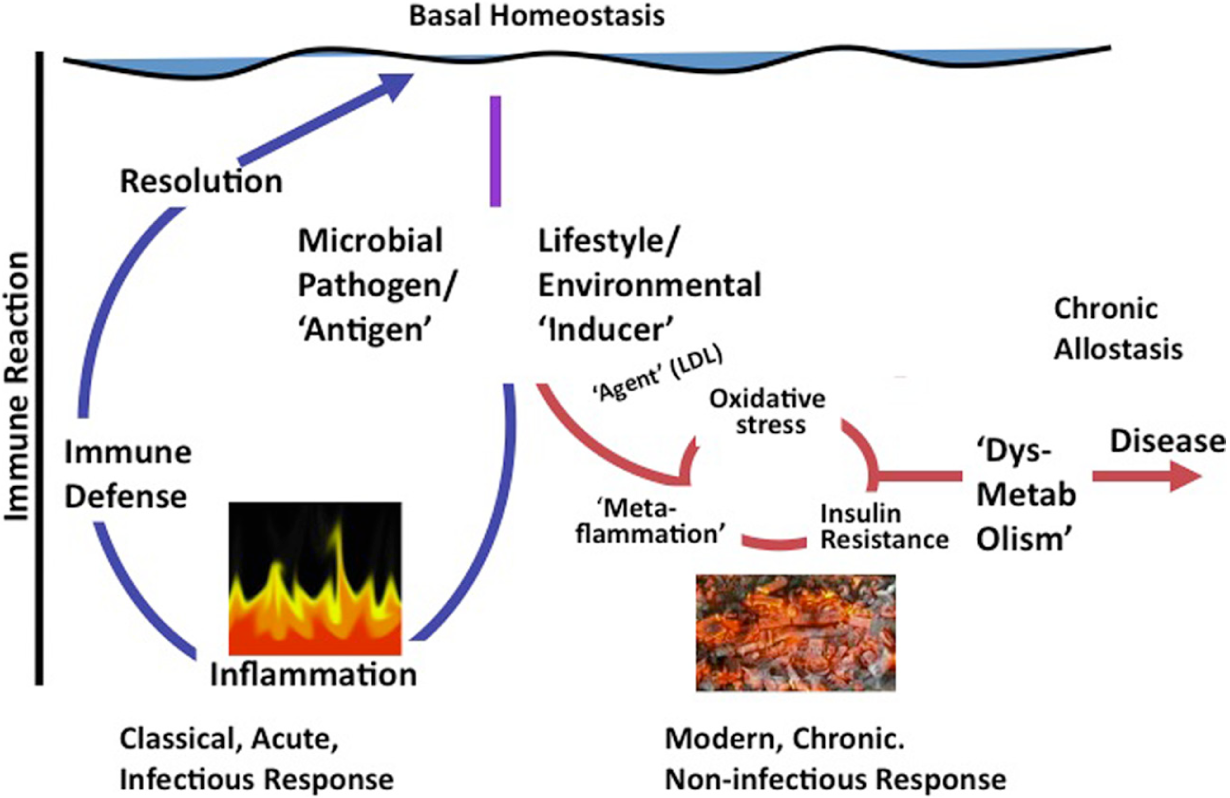
A Graphical Representation of the Difference Between Classical Inflammation Initiated by a Microbial Antigen or Injury and Metaflammation Caused by Lifestyle or Environmental Inducers (Adapted from Egger and Dixon 14 ).
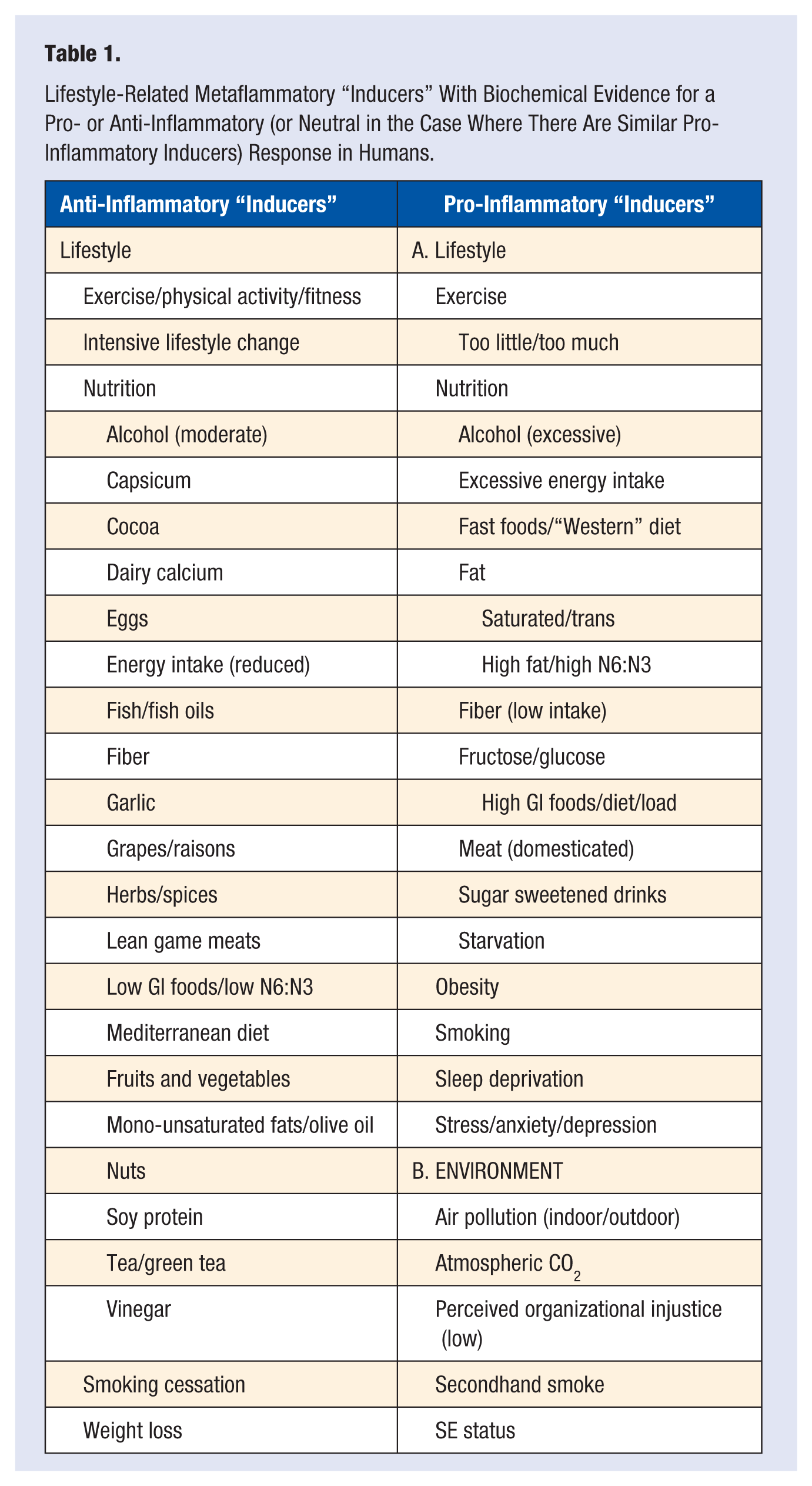
A list of anthropogens with evidence of a pro-inflammatory effect in humans is shown alongside equivalent stimuli with anti-inflammatory or neutral effects in Table 1.
Lifestyle-Related Metaflammatory “Inducers” With Biochemical Evidence for a Pro- or Anti-Inflammatory (or Neutral in the Case Where There Are Similar Pro-Inflammatory Inducers) Response in Humans.
Initially, it was thought that obesity might be the prime inducer of metaflammation 4 and that this, in turn, has lifestyle factors as determinants. However, as shown in Figure 2, obesity is not always a prerequisite for metaflammation, as several metaflammatory inducers, for example, smoking, depression, starvation, excessive activity, environmental pollution, and so on, do not require obesity to cause pathology. Indeed, fat from ectopic supplies in the liver, blood, and muscle, resulting from “spillover” from fat stores in adipocytes that have reached their functional capacity at different levels of total body fat, may explain some of these discrepancies. 15 Other effects may come from direct induction from lifestyle-associated physiological toxicants, for example, chronic cortisol exposure from prolonged stress, 16 sleep deprivation, 17 or environmental stimuli such as particulate matter in the atmosphere.18,19
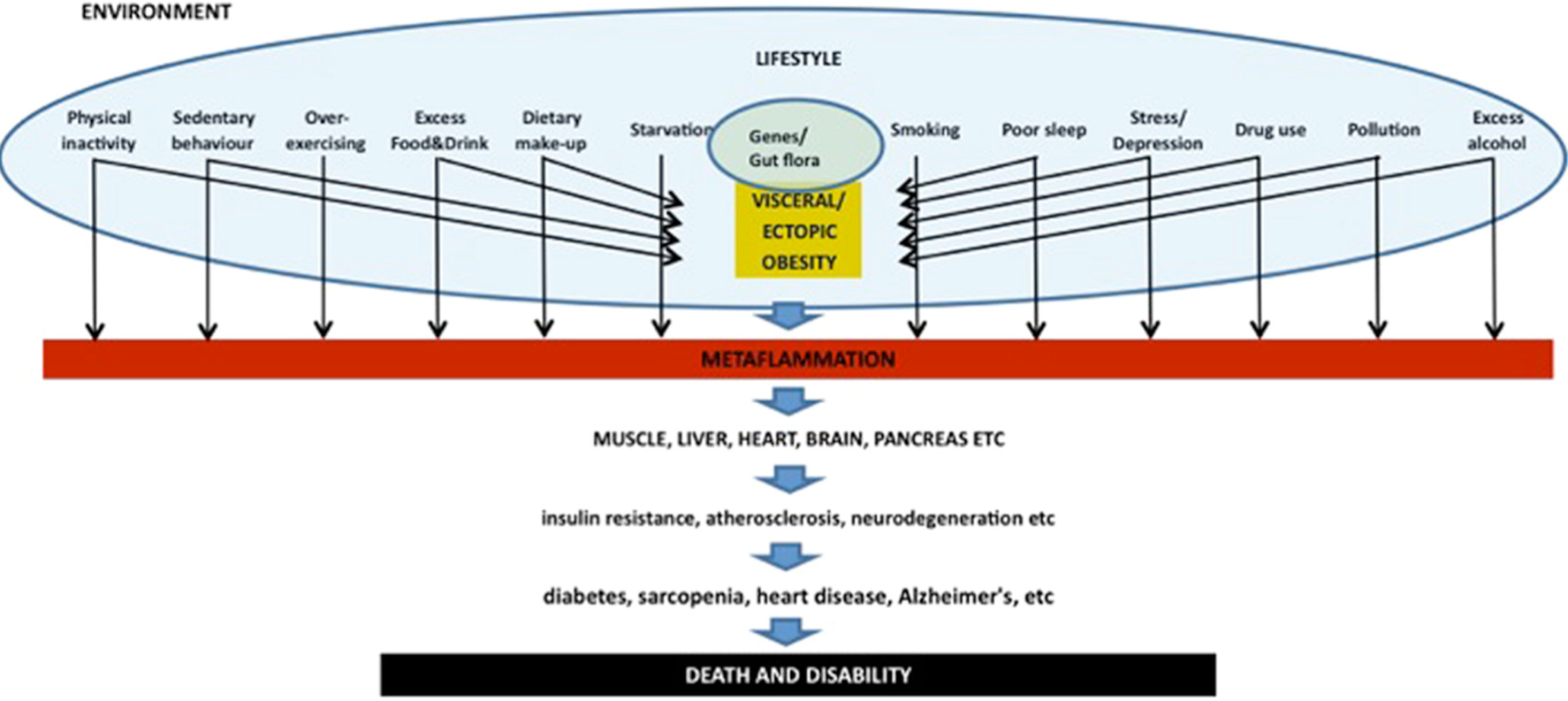
Inducers of “Metaflammation” (Adapted From Egger and Dixon 14 ).
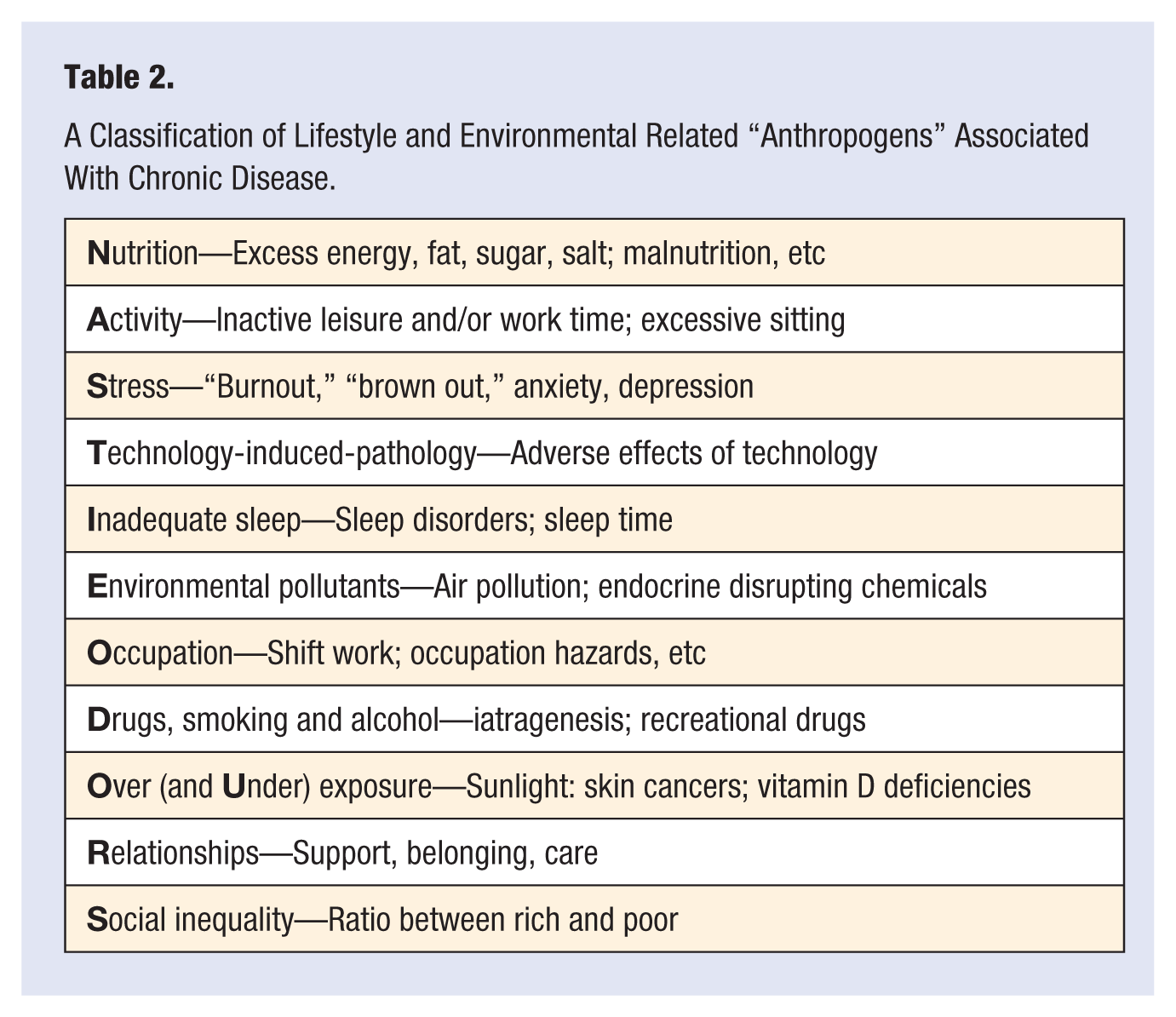
More useful from the perspective of lifestyle medicine would be a taxonomy of risk factors covering the range of modern chronic disease-related anthropogens shown in Table 1. Table 2 provides a list of these summarized in the text below. Together these provide the basis of a content for the science of lifestyle medicine. This is not meant to be comprehensive, but to stimulate discussion for a further expansion of the field. We will consider current available processes for facilitating the art of such a practice in a separate article.
A Classification of Lifestyle and Environmental Related “Anthropogens” Associated With Chronic Disease.
Anthropogens and Risk
While the anthropogens discussed below provide a structure for classifying determinants of chronic disease, it is clear that there is a vast current literature for each. The ensuing discussion provides only a snapshot of each of 12 broad categories with links to chronic disease. It should also be noted that the anthropogens listed here are “downstream” (proximal), or at best “midstream” (medial), determinants of disease, as shown in Figure 3. While inadequate nutrition and inactivity in particular, as downstream determinants, can be thought of as the “penicillin” of lifestyle medicine, 2 more midstream and upstream determinants, or the “cause of the cause” and the “cause of the cause of the cause” need also to be identified for a full understanding of disease epidemiology. 20 Stress, peer influences, and other social determinants are midstream factors influencing nutrition and activity levels. Modernization, political structure, the occupations that come from this, and the drive for minimally regulated economic growth lie at the root of much of the determinants identified here and should not be ignored in an overall perspective of disease causality. 21 These are discussed in summary form below under the acronym NASTIE ODOURS.
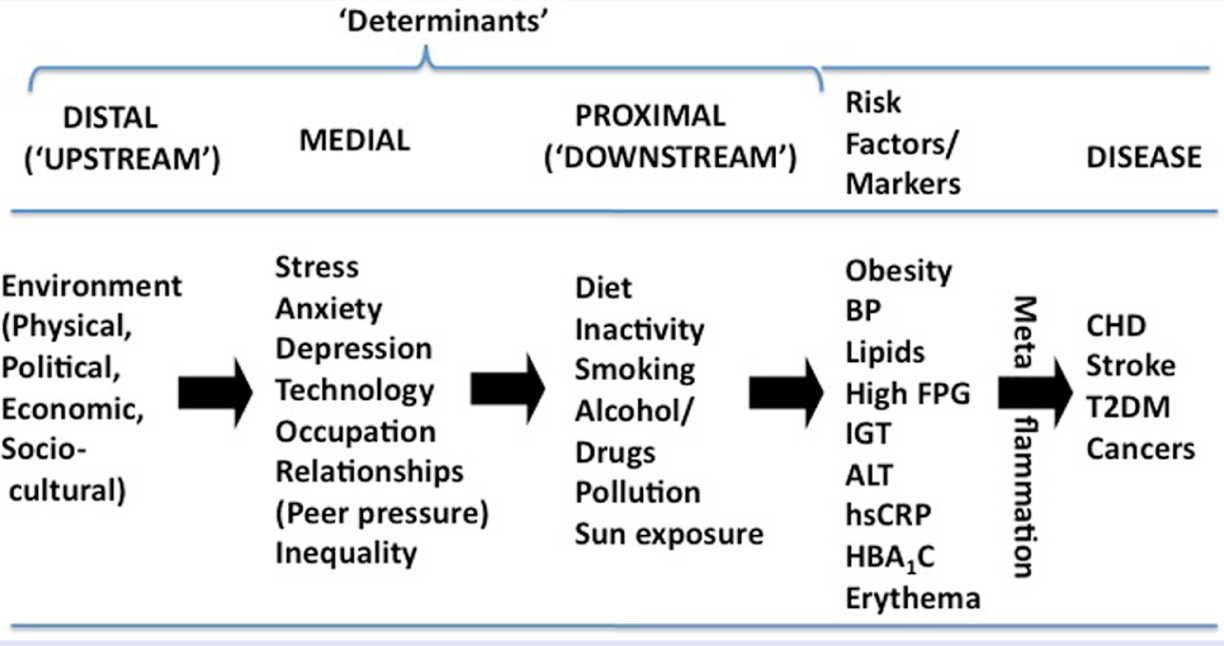
Hierarchy of Determinants and Risk Factors in Chronic Disease.
Nutrition
Inadequate and overnutrition (excessive calories) have been regarded as being at the core of much modern chronic disease. 22 This is somewhat paradoxical given that malnutrition, from inadequate and undernutrition, has been a prominent risk factor for disease throughout human history. 1 It remains a problem, alongside obesity, from overnutrition of nutrient poor, processed foods, thus delivering a double burden in developing countries. 23
In addition to excess total energy intake, modern western diets suffer from both nutrient excesses (eg, certain fats, sugar, salt, alcohol) and insufficiencies (fruits and vegetables, fiber, n-3 fatty acids). More specifically from a modern intervention perspective may be the level of processing of such foods. Monteiro, 24 for example, defines 3 levels of foods and drink: (1) whole foods, relatively unprocessed (fruits, vegetables, etc); (2) substances extracted from whole foods (oils, fats, flours, pastas, starches, and sugars) used as ingredients in preparation and cooking; and (3) ultra-processed foods made up from group 2 substances to which no or relatively small amounts of minimally processed foods from group 1 are added. Health values decline with increasing levels of processing from group 1 to group 3.
Supporting this are findings showing pro- and anti-inflammatory or neutral values of certain foods7,10,12 (as shown in Table 1), with the former coming predominantly from “new” or “modernized” foods and the latter from whole foods to which humans have adapted over several millennia.
Michael Pollan’s 25 dictum to “Eat food. Not too much. Mostly plants” would appear to be an appropriate goal focus for lifestyle medicine.
Activity
Levels of physical activity are reflected in chronic disease prevalence in individuals and populations. 26 Inactivity, or lack of sufficient activity, is one of the most underappreciated causes of chronic disease. Booth et al, 26 for example, list 35 chronic conditions for which there is evidence of a preventive or rehabilitative role for physical activity/exercise. The evolutionary basis of this seems obvious, as the current generation is possibly the first in history for which some level of activity has not been a daily requirement. This has led to a feed-forward association of genes and activity, such that a degree of physical activity is “expected” through genetic preprogramming. 27
More recently, data are accumulating to suggest that sedentary activities like sitting, which are characteristic of the modern environment and workplace, can be an independent risk factor for chronic disease. 28 Screen time among children has also been more strongly associated than physical activity with overweight and obesity. 29 Whether activity levels are increased through aerobic movement or resistance exercise seems less important than the fact that it is carried out. 30 It would appear that “anything is better than nothing, but more is better than a little.” The appeal to “think of movement as an opportunity, not an inconvenience” is an appropriate prescription for managing the psychological component of inactivity. 31
Stress, Anxiety, and Depression
Although endemic to humanity, the nature of stress has changed in recent times from an acute warning signal to a chronic strain on physiological adaptation. The outcome, while one is still striving to adapt, can be anxiety, or “feared helplessness,” once elegantly defined as “a thin stream of fear trickling through the mind. If encouraged, it cuts a channel into which all other thoughts are drained.” 32 When striving ceases, depression, or learned helplessness, can result, with attendant channels into a range of chronic diseases. High levels of depression are ubiquitous with chronic obesity and cardiometabolic disease, 33 which has led to new Heart Foundation guidelines on screening and treatment of depression in heart disease. 34 Strategies for preventing and dealing with the effects of stress thus become a cornerstone of the practice of lifestyle medicine.
Techno-Pathology
The history of human advancement is paved with evolving health challenges. The nomadic existence, for example, predisposed to the elements and injury, agrarianism to zoonotic diseases, and urbanization to the rapid spread of pestilence-related ailments.
In recent times, lifestyle has become the dominant etiology. But the modern environment must also share the blame. Pollution and work-related conditions of the early industrial revolution have given way to the technological age of the late 20th and early 21st centuries, and along with this has come new, albeit, less obvious challenges.
“Techno-pathology” is here defined as “the ill-health effects of certain forms of modern technology.” This can range from death or injury from modern machinery to hearing problems from loud music. 35 At the extremes, it involves mortality and morbidity from the use of high-tech weapons and chemical agents in warfare, but includes apparently obscure problems such as computer-related dermatoses, 36 impaired vision, 37 and repetitive strain injury 38 from excessive computer and small screen use.
Even more obscure is the use of improved agricultural technology (eg, hydroponics) leading to excessive toxicity of recreational drugs such as marijuana, and advances resulting in production of powerful synthetic drugs. Appreciation of the breadth of technology-induced pathology effects should lead to approaches to identify, modify, or at least moderate these through lifestyle and other changes.
Inadequate Sleep
Together with inactivity, inadequate sleep is one of the most underrated lifestyle risk factors for chronic disease. 39 This is associated with an increase in inflammatory markers, as well as more classic risk factors. 40 Research suggests that it is not the hours spent in bed but the amount of good sleep that is important. Less than 7 hours over 24 appears to be the bottom line, although this differs between individuals, with some people requiring much less. 39 Sleep disorders form a special category of sleep problems that can add to problems of inadequate sleep.
Modern lifestyles are often in direct competition with sleep, so much so that it could be argued that the majority of modern sleep problems have a basis in other lifestyle choices. The combination of sufficient sleep with other lifestyle factors (eg, physical activity, a healthy diet, moderate alcohol consumption, and nonsmoking) has additional value in heart disease prevention than sleep alone. 41 Unfortunately, chronic disease often interferes with sleep quality and quantity generating a bidirectional vicious cycle, a situation commonly encountered in lifestyle medicine. The good news is that sleep can be dramatically improved with a healthy approach to lifestyle and a structured approach to sleep hygiene. 42 Simple actions like the removal of interactive media from adolescent bedrooms can be a starting point for better sleep. 43
Environment
Environmental influences come in many forms, from the effects on behavior through easy, unhealthy choices (eg, an “obesogenic” environment 44 ), to endocrine disrupting chemicals 45 and pollution and particulate matter in the air, water, and soil. 46 Given that such influences are ubiquitous because of the myriad of chemicals released into the atmosphere since the beginnings of the industrial revolution, 47 this probably affects all of humanity to some degree. The outcomes, in terms of chronic diseases, are only just beginning to be understood.
At the individual level, some protection may be provided by positive lifestyle changes such as good nutrition, adequate exercise, and avoidance of the stimulant cause, where possible.47,48 It should be obvious however that significant macro-environmental reforms, some of which may crossover with those required to moderate climate change and other environmental degradation, is necessary. 49 Hence, the need for lifestyle medicine to accommodate an environmental component.
Occupation
While occupational status and employment type, such as shift-work, 50 may influence health through direct effects on health and safety, concern has turned more recently to social factors such as perceived social justice, 51 “burnout,” 52 and security of employment relating to occupational status. Marmot’s 53 extensive work with the British Civil Service (admittedly not a random sample) has highlighted the extent of the problem, at least in English culture. Both the physical and psychological occupational environments need to be considered as part of a lifestyle/environmental perspective on health.
Drugs, Smoking, and (Excessive) Alcohol
Cigarette smoke includes some 300 chemicals, many of which have proven deleterious health effects. There is also a range of legal, as well as illegal, recreational drugs that that have adverse physical and mental consequences that are often poorly characterized. Approved drug therapy, used inappropriately or off-label, can deliver disturbing outcomes as illustrated by the performance enhancement in sport issues. Appropriate drug therapy delivering effective therapy for one malady can lead to predictable additional health issues; chemotherapy of cancer, major psychotropic medications, and immunosuppressive therapy are prominent examples.
Alcohol, through its dose-dependent effect, is a little more complicated. While a moderate, regular intake (1-2 glasses/day) appears to have some specific health benefits, excessive amounts, and binge drinking, are decidedly disease related. 54 The social impacts of alcohol use need also to be counted in any considered analysis of alcohol use.
Pharmacological developments have no doubt added to human well-being especially in the area of chronic disease and risk reduction. However, the downside of medications needs to be managed. Complimenting necessary drug therapy with a lifestyle approach to health management provides the art of medicine and delivers optimal health outcomes. A lifestyle approach may allow medication doses to be reduced or stopped all together. Patient engagement in chronic disease management is critical, and a well-informed collaborative relationship is needed to evaluate the costs versus benefits of all interventions. 55 Combining both lifestyle and medical therapies, where needed, provides a more logical choice than either lifestyle or medical treatment alone.
Over (and under)-Exposure
Many lifestyle-related behaviors have a linear association with ill health (eg, smoking; sleep) where more (or less) of a stimulus is associated with more (or less) disease risk. Others have a “U” or “Tick-shaped” association where too little or too much may be detrimental, but the appropriate amount of a stimulus is associated positively with health status. In the natural environment, overexposure to certain forms of UV light (eg, sunlight) is a case in point. Too much exposure is a major skin cancer risk, especially for fair-skinned nonnative populations in hot climates, such as Australia, New Zealand, and parts of the United States.56,57 Underexposure, or too little sunlight, on the other hand, can result in deficiencies in vitamin D, which a vast amount of recent research has highlighted as a risk factor in a range of health problems from cardiovascular disease, 58 to diabetes, 59 and even depression. 60 Again, metaflammation may play a mediating role. 61 Results of overexposure to other forms of man-made radiation and environmental chemicals crosses over with technology-induced pathology and environmental influences referred to above.
Relationships
While it may seem intuitive that social influences should flow through to human health, there is accumulating evidence to support this, and in particular, the quality of interpersonal relationships, 62 stemming back even to maternal separation in childhood. 63 The physiological link may not be fully elucidated, but inflammatory processes have also been associated with poor social relations. 64 Outcomes may be linked to the hypothalamic-pituitary-adrenal axis relating to stress, anxiety, and depression, 65 alluded to above, or the social inequality factors that often go with loneliness and lack of personal support discussed below. To this extent the lifestyle medicine practitioner may also need to be part relationship-counselor, or at least have referral networks to support this.
Social Disadvantage
The unhealthy effects of income inequality and financial- and employment-related insecurity are now established as recognized health risks. 66 This has been emphasized in particular by epidemiologists Richard Wilkinson and Kate Pickett in their analysis of relative inequality and health and social outcomes in OECD countries. 67
Again, the mechanisms are far from clear, although inflammation has been shown to play an intermediatory role. 68 Outside the impact of poor nutrition, absolute poverty seems less of a concern than relative poverty. 68 When incomes become vastly unequal the health impact is obvious at all levels of society and not just to those at the bottom end of the income scale. This can be seen between and within countries 69 and could be due to lack of trust and associated psychosocial stressors. 70 Market structures driving inequalities need also to be considered as distal determinants. 71
The link between relationships and inequality is an obvious one but is often considered outside the ambit of the clinician. And while this is true at the distal determinant level, these variables need to be considered in any comprehensive lifestyle/environmental diagnosis.
Omissions and Interactions
A noticeable omission to the list of determinants discussed here is obesity. This is deliberate, partly because obesity is more of a risk factor than a determinant (as shown in Figure 3), and excessive weight gain is a consequence along a number of pathways (nutrition, inactivity, stress, etc) to many other chronic diseases, but also because of the growing uncertainty of a direct causal link between obesity per se and chronic disease. 14 The effects of obesity risks pose the question of whether obesity is merely a “canary in a mineshaft” signaling problems in the broader environment rather than a direct cause of disease. 49
It should also be noted that a simple linear approach to lifestyle-related risk factors is inadequate when dealing with complex interactions between risks that require a more systems-type approach. It should be obvious that there are interactions and feedbacks, between all determinants making the model characteristics of a “systems” approach, 72 where all aspects of the model need to be considered, and not just independent, single factors. A prime example of this is the recent finding of more active neural responses to junk food images and higher food intakes in individuals after they are sleep deprived than after adequate sleep. 73 The effect may be even greater when combined with inactivity, stress, binge drinking, and the techno-pathological influences of manufactured high “energy” drinks.
Lifestyle medicine thus becomes an art in “nudging” clients along a spectrum of risk factor change (see Figure 4), while taking account of the science of all and not just some of the risk factors identified here. The analogy is with a barrel lock approach, where all columns on the lock need ultimately to be in alignment for the lock to open rather than a single lock and key approach, which is less likely to affect the underlying inflammatory basis of most modern lifestyle-related chronic disease.
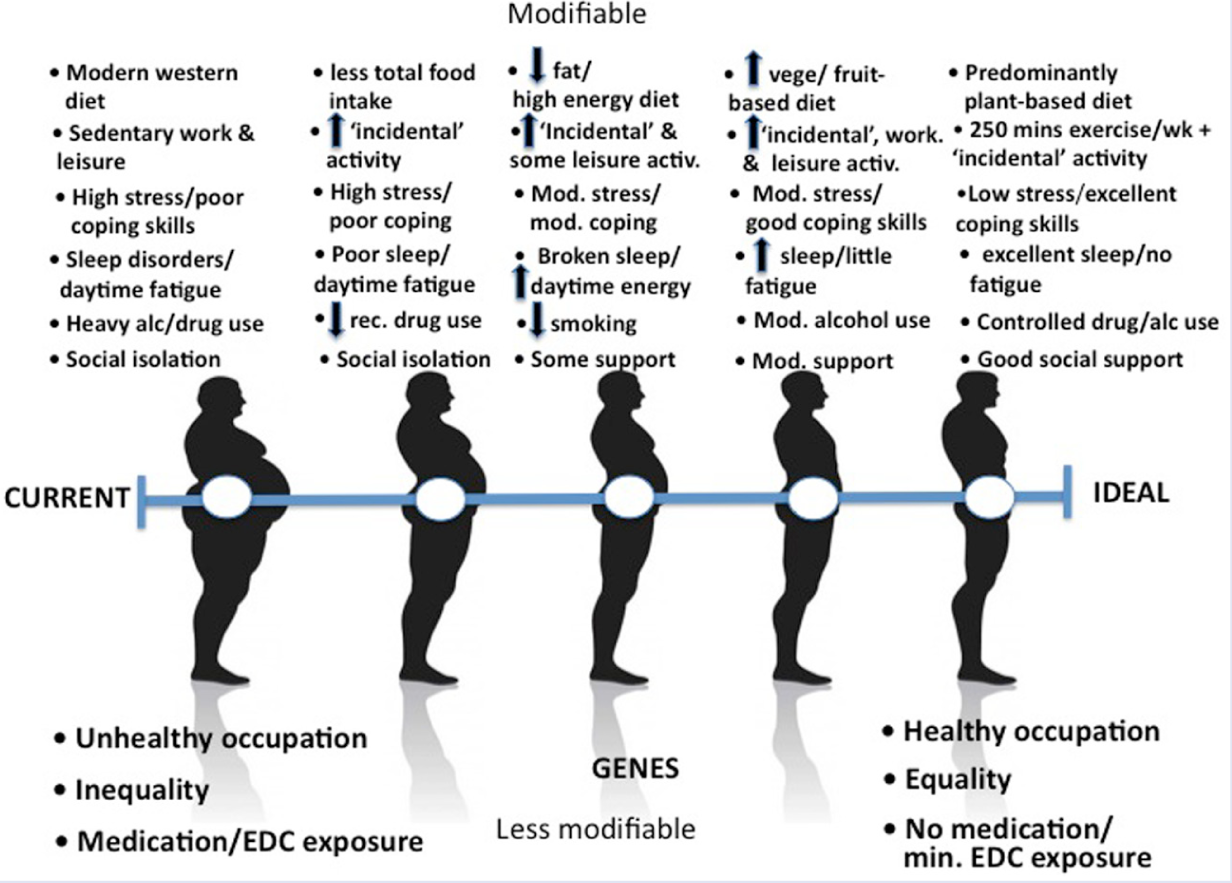
A Sliding Scale of Lifestyle Change.
Summary
Chronic disease epidemiology current lacks the mono-causal focus afforded to infectious diseases through the germ theory of the 19th and early 20th centuries. A classification of lifestyle/environmental risk factors under the term anthropogens, however, focuses attention on a limited number of modern risk factors identified by the acronym NASTIE ODOURS. More important, it shifts the focus from a “silos” approach to the individual management of chronic disease to a directed approach to disease determinants, providing a rationale for a discipline of lifestyle medicine.