
Abstract
We have previously identified a number of “determinants” of chronic disease, using the acronym NASTIE ODOURS. These have been given the collective term “anthropogens,” in this journal and other publications, to help direct the management of modern chronic ailments to a monocausal focus, akin to that afforded infectious diseases by the “germ theory.” We suggested the acronym NASTIE ODOURS as a starting point for a taxonomy of lifestyle medicine determinants. In the current article, we add 3, less quantifiable, but currently increasingly more important psychosocial experiences to these: Lack of Meaning, Alienation, and Loss of culture, changing the previous acronym to NASTIE MAL ODOURS. As with other determinants, all have accumulating evidence of an underlying low-grade, systemic, inflammatory physiological base (“metaflammation”), but with the need for further research to solidify these findings.
‘“Metaflammation” is increasingly recognized as a link between determinants and disease.’
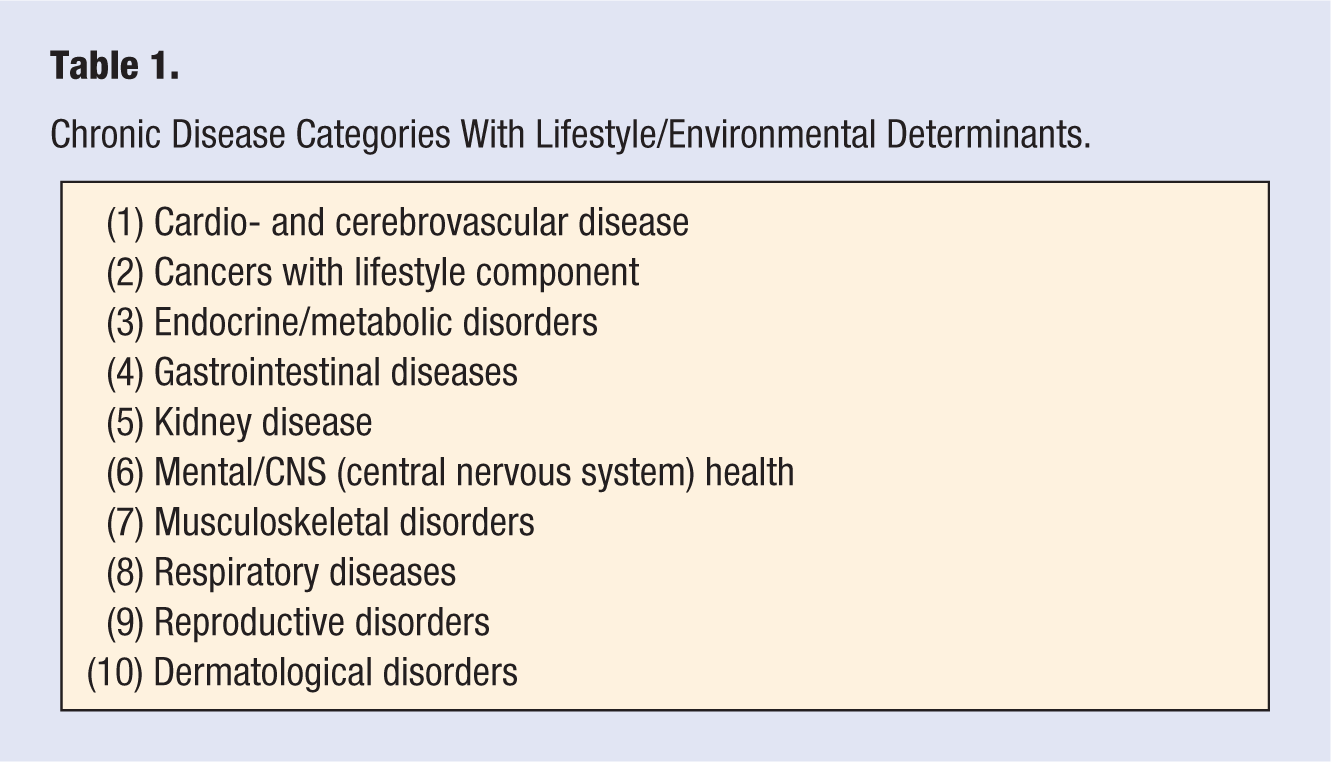
Lifestyle medicine (LM) is an evolving discipline, generally aimed at decreasing or moderating the modern rise in chronic diseases, listed in Table 1, which have, or may have, lifestyle and/or environmental “determinants.”1-5 (A determinant, or driver, is defined here as “a key linear force behind disease causality,” 6 as distinct from a direct “cause.”)
Chronic Disease Categories With Lifestyle/Environmental Determinants.
A structure and pedagogy for LM has previously been described.7-9 This recognizes 4 main points of difference with conventional clinical practice: (1) the epidemiological base (the “knowledge”), (2) the skills (the “art”), (3) the tools (the “materials”), and (4) the procedures (the “actions”). Within 1 (the epidemiological base), a number of determinants of modern chronic diseases have been proposed, 8 expanding the range of these from those most often implicated (inactivity, poor nutrition, and smoking, or “feet, forks, and fingers” 9 ) to include social, cultural, occupational, environmental, and other factors, which interact with each other in a “systems” type model. 10 The list of potential determinants have been elaborated elsewhere,7,11-14 as existing in a hierarchy, as shown in Figure 1. They have been listed under the acronym NASTIE ODOURS and given the collective term “anthropogens,” which are defined as: “Man-made environments, their by-products and/or lifestyles encouraged by those environments, some of which have biological effects which may be detrimental to human health.” 15 Although not directly synonymous with “cause,” the concept of anthropogens as determinants, provides a focus for management of chronic diseases not dissimilar to that afforded infectious diseases by the “germ theory” of the early 20th century. 16
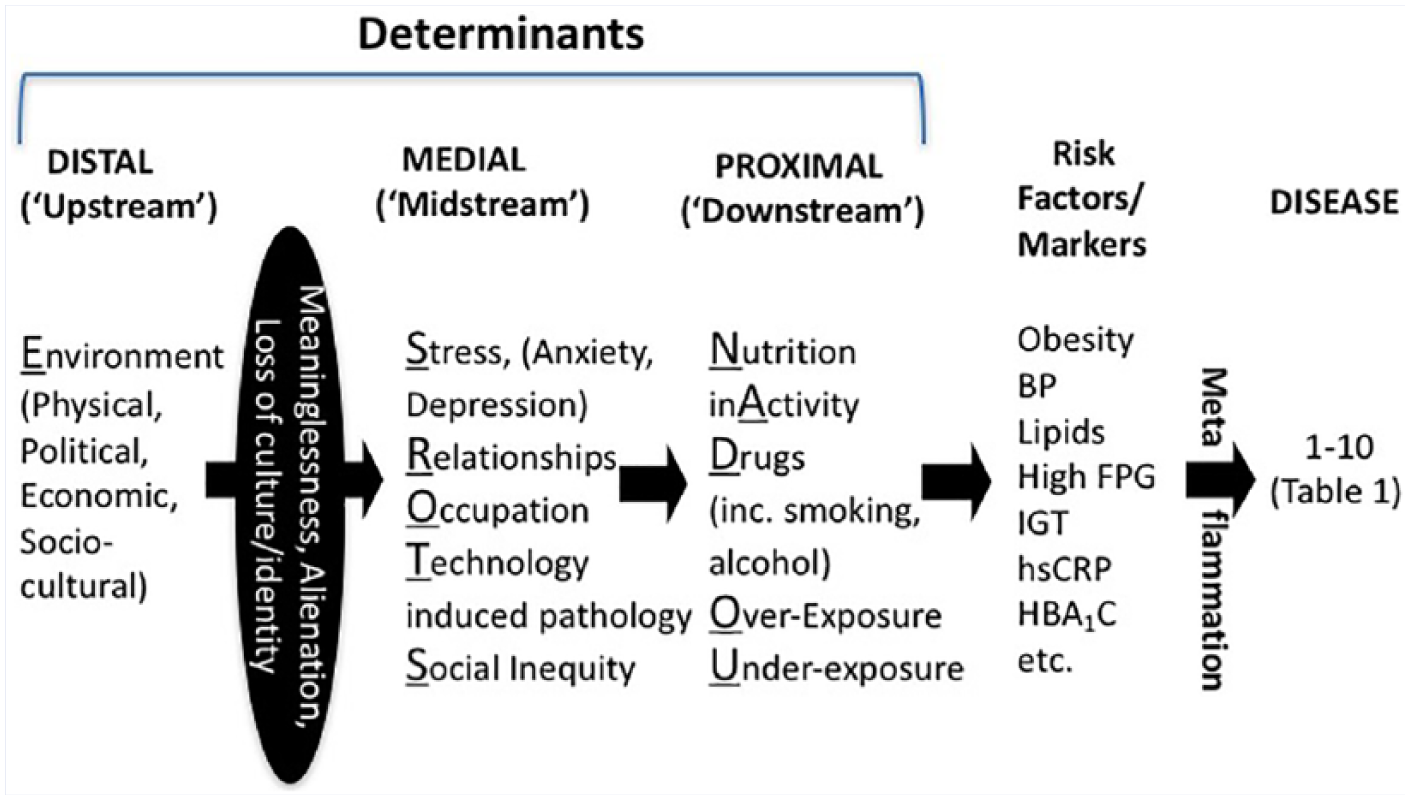
A hierarchy of lifestyle/environmental determinants in chronic disease “causality.”
The list of anthropogens shown in Figure 1, in clear print, was never meant to be definitive, but more as a starting point for discussion around the discipline of LM. Since developing the list, obvious exclusions that have been recognized are psychosocial factors, which can have outcomes in many of the modern chronic diseases listed in Table 1, in a similar fashion to the more obvious determinants previously described.
There are other possible psychosocial determinants, but here we identify and discuss 3 with accumulating evidence for a link with chronic disease. These are
Lack of Meaning, or purpose in life
Alienation
Loss of culture and/or identity.
These are shown in solid print in Figure 1 and now expand the acronym proposed for determinants, to NASTIE
The Meaning of Meaning
The importance of meaning, or purpose in life, was explored by Victor Frankl in his 1959 book Man’s Search for Meaning. 22 Imprisoned in a World War II concentration camp, Frankl found the survival and well-being of fellow Jewish prisoners was related to the extent to which each had purpose in their lives. This could have a spiritual or religious basis but could also be secular and spring from attachments to family, culture, occupation, or interests.
Much literature now supports Frankl’s view. 23 The ability to find meaning in life is associated with better physical health, reduced risk of stroke, 24 myocardial infarctions, 25 and suicide, 26 as well as reduced overall mortality 27 and psychological well-being when faced with chronic pain. 28 Lack of meaning is associated with depression, which can act as a mediator for ill-health. 29 Other work has linked purpose to physiological changes, 30 including inflammatory markers, 31 indicative of “metaflammation,” although this evidence is currently not extensive. Associations of metaflammation with reduced quality of life 32 and lesser life satisfaction 33 suggest this would be the case (although this could be a case of reverse causality).
In one recent study, people with more purpose were found to have better patterns of health care utilization, hence possibly explaining better health outcomes. 30 Meaninglessness is linked to behavioral factors, such as drug use, smoking, stress, inactivity, and poor nutrition, that have an impact on the risk of poor physical outcomes. According to Roepke et al, 23 meaning can mediate the relationship between other variables and physical health, as well as be mediated by other factors in its relationship to physical health. Presence of a sense of meaning has also been found to be a robust measure of healthy lifestyle behaviors in European adolescents. 34 Metaflammation is an important intermediate pathway in the association between stress and measures of ill health, 35 and can be genetically upregulated by a conserved transcriptional response to adversity. 36
Meaning, along with other components of psychological well-being, has become the focus of several intervention studies, 37 including “logotherapy,” 38 designed to improve a person’s life outlook, thus providing a potential point of intervention for improving health outcomes in a Lifestyle Medicine context. Johnson et al, 39 in a systematic review, also note several randomized control trials that showed a link between C-reactive protein, a potent, albeit acute inflammatory marker, and psychosocial stress. Interestingly, those at risk who escape meaninglessness have been found to have greater social cohesion and resilience. They can make sense of what is happening to them and respond accordingly. 40
Alienation, Estrangement, and Loneliness
Alienation is a form of withdrawal or estrangement that can result from many different experiences such as discrimination, 41 social isolation, 42 or rejection from friends, parents, family, peers or society, all of which have been shown to be reflected in metaflammation. At a less obvious level, it can result from the alienation from society that many feel, although they may not recognize.
Mediating factors such as loneliness, 43 psychosocial stress,39,44 and loss of control,39,45 may play a part in the link shown in these studies between alienation, inflammation, and long-term chronic disease outcomes. Experimental trials have even shown a neural link with metaflammatory processes due to social rejection.45,46
Of particular interest is the growing evidence relating to the effects of adverse childhood experiences (ACEs) on long-term alienation, metaflammation, and chronic disease. A ground-breaking survey in the United States of over 17 000 predominantly middle-class American adults by the Centers for Disease Control and Prevention and health care provider Kaiser Permanente47,48 showed that more than 1 in 8 (12.6%) had experienced 4 or more ACEs, including physical, sexual or emotional abuse, death of a parent, violence in the household, and so on, on a 10-point ACEs scale. There was a close relationship between ACE scores and health outcomes 50 years later. More important, the relationship was strikingly dose-dependent. Chronic obstructive pulmonary disease (COPD) was 2.5 times higher in those with an ACE score of >4; depression 4 times; heart disease 3 times, and suicide 12 times. Population attributable risk figures showed that 54% of current depression and 58% of suicide attempts in women in the US sample could be ascribed to ACEs.
The original ACE study came from observations made during an extensive weight loss study in the United States. 48 The study had a high drop-out rate, particularly among obese patients who had successfully lost weight. Exploring the reasons for this, the researchers found that obesity is often used as a shield against sexual abuse, and hence is often caused by unconscious or occasionally conscious behaviors like overeating and inactivity that were put in place as solutions to negative early experiences.
Some of the outcomes of ACEs may be due to lifestyle factors like poor nutrition and inactivity, as well as to more self-harming but self-medicating behaviors like smoking, alcohol and drug abuse, or sexual promiscuity that results from alienation and psychosocial stress. These are dangerous enough in themselves, but there are also physiological links with altered brain structure in a highly plastic developing brain, and effects on the hypothalamic-pituitary-adrenal (HPA) axis, 48 which can affect later health. Metaflammatory responses are more common in later adulthood among children surviving adverse early experiences, 42 possibly because of alterations to the immune system because of trauma in early life. 49 At least one study has shown that this can be reversed in low–socioeconomic status youth through family-oriented psychosocial intervention. 50
There is also a large and growing body of literature linking social isolation and loneliness to adverse health outcomes. 51 Loneliness, for example, often initiated by alienation but also mediated by inadequate social skills 52 is associated with an increased rate of mortality, 53 and could be as prevalent as 1 in 10 in modern society. 54 There are limited data to suggest that metaflammation may have an underlying and mediating basis in loneliness,43,55 although to date, it is unclear whether the effect is directly due to loneliness or to accompanying variables, such as stress, or accompanying ill health. 56
Loss of Culture and Identity
Loss of culture and/or identity arise from dispossession, displacement, conflict, climatic events or natural disasters, and even confused identity around sexual orientation or family disruption. All result in a loss of purpose or alienation and the effects of these discussed above.
The effects of loss of culture are seen most evidently in Indigenous First Nation cultures such as in Australia, 57 the United States, or Canada 58 where dispossession and cultural disruption is most marked. Close and complex spiritual links with the land mean that environmental dispossession has negative consequences for health, which are only just beginning to be understood. 59 Aboriginal Australians, for example, have rates of cardiovascular disease, diabetes, and chronic kidney disease, 4 times that of Non-Indigenous Australians and an average reduced life expectancy of 10 to 12 years. 60
The experience of loss of culture and identity is not unique to dispossessed Indigenous populations. There are growing numbers of migrants, especially those forced to move for fear or famine (eg, in 2014 the UNHCR estimated that there were 59.5 million forcibly displaced people, the highest ever recorded). Displacement of communities, often through conflict,61,62 but also climatic events 63 or natural disasters 64 also typically result in adverse health outcomes often associated with disruption of culture and reduced social, cultural, and economic capital. 65 At least one study has shown that loss of self-control in these situations can lead to increased metaflammatory processes associated with an increased prevalence of chronic disease, 45 although there is a lot more work to be done in this area.
Conclusion
There is a considerable and growing body of evidence to show that the psychosocial factors discussed here (meaninglessness, alienation, and loss of culture) warrant inclusion into the list of anthropogens previously considered as determinants of chronic disease. In considering determinants, however, it is important to treat these as a series of complex interactions in a “systems” type model, as shown in Figure 2, rather than as a singular determinant in a “linear” fashion contributing to disease outcomes. While the often-used mnemonic of “feet, forks, and fingers” has been proposed as all that is required to cover the bulk of lifestyle-related chronic disease etiology, Figure 2 illustrates that while these are most visible above the water line, below the water line the gamut of determinants can react independently, or interactively, to lead to a disease outcome. Ignoring these below-the-water-line factors can lead to an incomplete approach to treatment. Inadequate sleep, for example, can lead to inactivity and poor nutrition, and can increase depression and result in excessive drug use. Similarly, lack of meaning, alienation and loss of culture may not be directly causally linked with coronary heart disease, stroke, or metabolic problems per se, but could form a link through unhealthy lifestyle behaviors, environmental exposures, or stress. Such a link appears to be accompanied in most, if not all instances, by the physiological process of low-grade, chronic, and systemic inflammation (“metaflammation”).
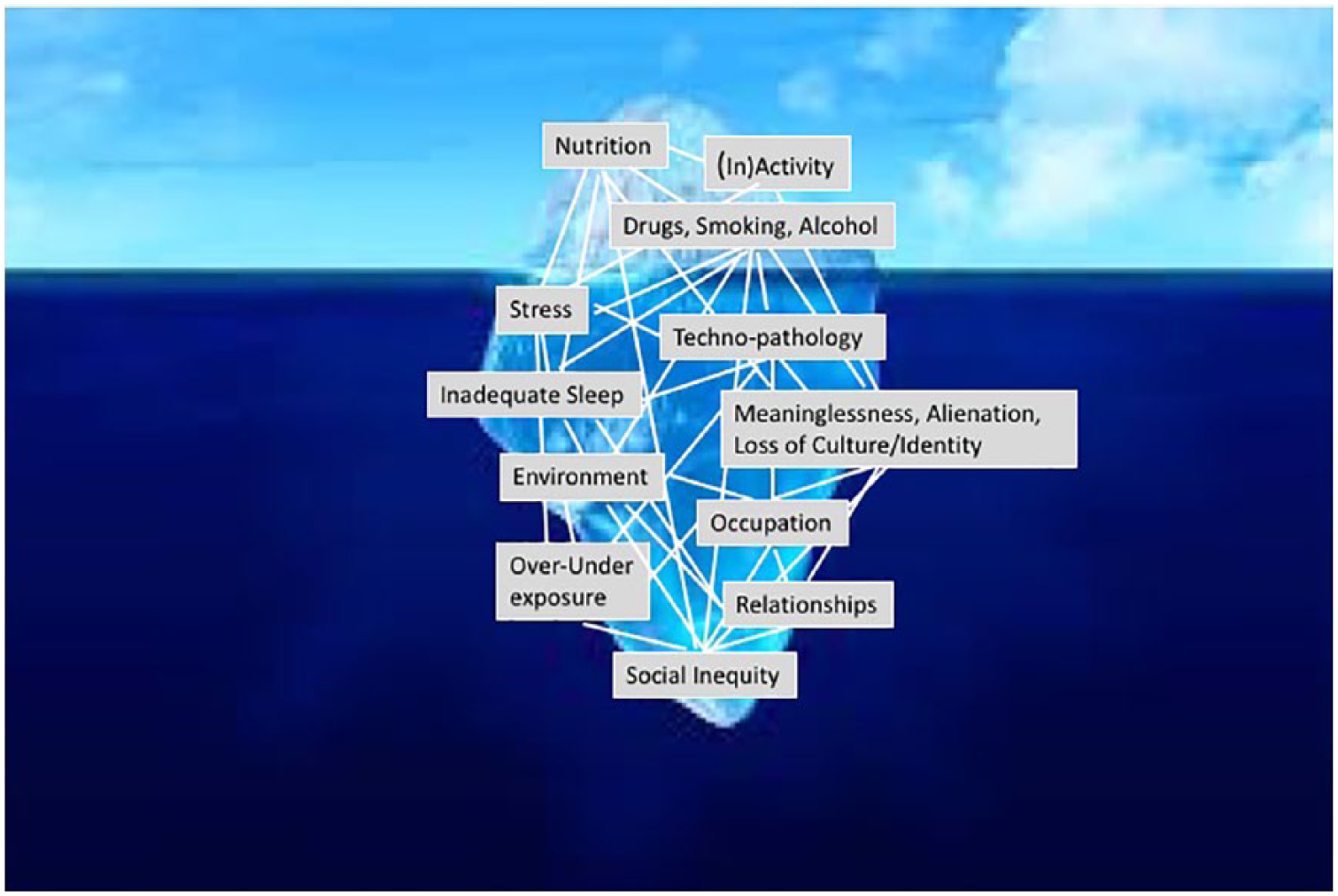
An iceberg analogy of the interactions between lifestyle/environmental determinants
The psychosocial determinants of chronic disease outlined here add to the effects of breakdown in relationships and social inequality covered in the previous NASTIE ODOURS acronym (now expanded to NASTIE MAL ODOURS) and illustrate the importance of less well recognized chronic disease determinants. As shown in Figure 1, the psychosocial (MAL) determinants discussed here form a “midstream” level of determinants, often overlooked in the epidemiology of chronic diseases but within the ambit of LM. Although beyond the scope of this article, it is incumbent on chronic disease specialists therefore to develop screening, diagnostic, and intervention tools for dealing with the MAL factors identified here as part of a “toolbox” for LM practitioners. Whether channeled through inactivity, nutrition, drug use, or other lifestyle behaviors, their outcome appears linked to the metabolic processes (metaflammation) characteristic of other chronic disease determinants shown at different levels in Figure 1.
While the clinical options for dealing directly with these psychosocial determinants of ill health may be limited, they should not be ignored. Neither should their outward expressions (stress, diet, inactivity, drugs, etc), only be treated downstream, ignoring the more distal sociocultural, political, and physical environmental factors giving rise to their existence upstream. Experiences with logotherapy in those with lack of purpose, art therapy, parenting education in lower socioeconomic status children, developed resilience of those at risk from traumatic events, and simply recognizing and sympathetically discussing the issue with MAL affected patients, offer a possible way forward.
New procedures in LM such as shared medical appointments, social referral, group education, and self-management processes shown to be popular, particularly in underserved groups, 4 may help ease the situation. Most important, the process of LM should teach us that attention should be diverted from treating the disease to treating the individual, in some cases capitalizing on existing cultural and community strengths that have otherwise been lost, as well as looking more “upstream” for the drivers behind what seem simple lifestyle-related behaviors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.