
Abstract
Perceived health is a widely used proxy for measuring individuals’ health status across different populations, including older adults. This measure is commonly reported as a subjective indicator, as a strong predictor of longer-term morbidity and mortality, and as a method to identify high-risk groups with health needs. This study examined differences in physical activity (PA) and physical function (PF) among older adults living in a retirement community located in the Midwest region of the United States as a function of perceived health. Results suggest that older adults perceiving their health as excellent reported significantly higher PA and performed significantly better on PF assessments than those reporting it as good or fair. Programs focusing on increasing PA in older adults living in retirement communities should be considered as potential strategies to enhance the health and health perception of this population.
PA [physical activity] is a key health component that has the potential to prevent or delay the onset of numerous detrimental health conditions common among the older adult population.
According to the US Census, by the year 2030, all baby boomers will be older than 65 years of age. 1 This marks an important demographic turning point in US history. Currently, those aged 65 years and older account for about 16% of the US population, and by 2060 this number will rise to 23%. 1 As the number of older adults increases, the health of this group also becomes a growing concern. This is based on health information among older Americans where approximately 70% of them have multiple chronic conditions, and treatment for this population accounts for 66% of the nation’s health care budget.2,3 The prevalence of other conditions such as difficulty in performing activities of daily living among this population is also high. 4 Chronic conditions negatively impact health and quality of life and contribute to the leading causes of death among this population.5,6
Perceived health is a widely used proxy for measuring individuals’ health status across different populations, including older adults. This measure is commonly reported as a subjective indicator, as a strong predictor of longer-term morbidity and mortality, and as a method to identify high-risk groups with health needs. 7 Several factors have been associated with perceived health among older adults. This includes, but is not limited to, social disconnectedness and perceived isolation, weight loss, functional limitation, number of chronic diseases, socioeconomic status, and behavioral factors such as smoking habits, physical activity (PA), and activities of daily living.8-14 In terms of PA, a study conducted in 1024 older females between the ages of 60 and 99 years demonstrated that high- and medium-intensity PA (expressed as MET × hour/week) accounted for significant variance in ratings of perceived health. 13
PA is a key health component that has the potential to prevent or delay the onset of numerous detrimental health conditions common among the older adult population.14,15 There is compelling evidence of the association between increased levels of PA and improved health in older adults.15,16 For instance, findings from a recent study comprising a 3-year follow-up demonstrated that older individuals presenting with higher levels of PA showed less decrements with aging in functional variables than those reporting lower levels of PA. 17 However, this population presents with lower rates of PA participation compared with younger age groups.18,19 We recently reported that older adults living in a retirement community reported to spend about 10 hours per day in sedentary activities. 20
Studies focusing on perceived health have concentrated on older adults living in the community, and little is known about correlates of perceived health in those living in retirement communities. Increasing the knowledge regarding factors associated with perceived health in retirement communities may help devise strategies and intervention aiming to improve health and perceived health tailored for this particular population. A recent literature review demonstrated that there is a diversity of complex and multidimensional factors related to reasons to move to a retirement community, including, but not limited to, debilitated health and the need for assistance to perform activities of daily living. 21 Difficulties to perform activities of daily living is highly linked to low levels of physical functioning. 22 Thus, acknowledging the important role played by PA and physical functioning in older adults’ perceived health, the present study examined potential differences in PA and physical function performance among categories of perceived health in older adults living in a retirement community. This is important because although most older adults (approximately 93%) live in the community, about 7% live in retirement communities; however, with the rapid and continuing growth of the older adult population, this number will certainly increase. We hypothesized that older adults perceiving their health as excellent would present with higher PA scores and would perform better in physical function compared to those reporting their health as good and fair.
Methods
Participants
This study represents a secondary data analysis from a previous cross-sectional study conducted in a retirement community located in the Midwest area of the United States. 20 Please see referred study for details on sample recruitment and setting. Briefly, only residents living in the independent apartments, duplex living, and personal care apartments were eligible to participate. Out of 236 residents aged 60 years and older, 100 individuals fit the inclusion criteria and volunteered to participate in the study.
Measures
Perceived Health
Perceived health was self-reported assessed using the following question: “Would you say that in general your health is?” Responses were rated on a 5-point scale as follows: excellent, very good, good, fair, and bad. For the purpose of the present study, responses were further grouped/categorized into 3 different categories so that 3 different groups could be formed: (a) excellent (excellent and very good), (b) good (good), and (c) fair (fair and bad). Similar procedures have been reported in previous studies.11,23
Physical Activity
Different from exercise and physical fitness, PA is defined as any bodily movement produced by the skeletal muscles that results in energy expenditure above resting levels. 24 To this end, PA was measured using the Physical Activity Scale for the Elderly (PASE). 25 The PASE is a 10-item instrument designed to assess PA in large samples of older adults over a 1-week period. This instrument assesses frequency and duration of participation in leisure activities (ie, walking outside the home, light, moderate, and strenuous sport and recreation) along with participation in housework, lawn work/yard care, home repair, outdoor gardening, and caring for others. The PASE scores have been reported to be a valid measure of PA engagement in the older adult population26,27 and are expressed as activity counts.
Physical Function
Physical function (PF) was measured using the Short Physical Performance Battery (SPPB). The SPPB is an objective and valid assessment tool for evaluating lower extremity functioning in older persons.28,29 This battery assesses lower extremity function based on a 3-part assessment, including standing balance, gait speed, and lower extremity strength. Standing balance is assessed by asking participants to maintain upright posture for up to 10 seconds per test while standing with feet side-by-side, semi-tandem, and tandem positions. The balance assessments occur in a progressive order wherein participants passed one test in order to attempt the subsequent, more challenging test. Gait speed is assessed based on the time taken by a participant to walk a 4-meter course at a normal pace. Lower extremity strength is assessed by a chair-stand test in which participants are instructed to sit in and fully rise from a chair 5 times as quickly as possible, without using arms for support. Participants are first asked to attempt and complete a single sit-and-rise before beginning the entire chair stand test. Performance scores for each SPPB individual assessment (ie, balance stand, gait speed, and lower extremity strength) and a summary score aggregating the individual assessments are calculated as per standard SPPB protocol. Each of the 3 performance assessments is assigned a categorical score ranging from 0 (inability to complete a test) through 4 (highest level of performance) using standardized scoring, and the summary ranging between 0 and 12 can be calculated by summing the standing balance, gait speed, and lower extremity strength categorical scores. Higher scores reflect better lower extremity function.
Other Measures
A collection of demographic and health-related information was gathered using a questionnaire developed to attend the purpose of the present study. Demographic variables included age, gender, and ethnicity. Health-related information included body mass index (BMI; calculated as weight in kilograms divided by height in meters squared), 30 number of diagnosed chronic diseases, and number of prescribed and over the counter medication taken.
Procedures
All assessments were completed in a single session in the fitness center office located on the first floor of the retirement community. The questionnaires and the SPPB were administered by an experienced research staff with experience in assessing older adults. Complete assessments (for the entire primary study) took an average of 87 minutes for each participant. Participants scheduled for assessment reported at the fitness center office to read and sign the informed consent. After signing the informed consent the research staff started administering the questionnaires, which were completed in the following order for all participants: PA and demographic/health. Following questionnaires, participants were led to the main area of the fitness center to undertake the SPPB tests. Upon completion, participants received a modest cash compensation for their time.
Data Analysis
Data were analyzed using SPSS version 24 (IBM Corporation, Armory, NY), and significance was set at P < .05. Descriptive statistics (mean and standard deviation) were used to display PA and SPPB scores information. One-way analysis of variance (ANOVA) was used to examine potential differences in PA and SPPB scores among categories of perceived health. Because PA and BMI have a direct relationship with physical function, we further conducted analysis of covariance (ANCOVA) with contrast analysis to examine differences in SPPB scores among perceived health categories controlling for the referred variables.
Results
Detailed characteristics of participants are given in Table 1. Briefly, the average age of participants was approximately 84 years, with no significant difference among categories of perceived health. The majority were female, being classified as overweight with over 60% presenting with ≥3 chronic diseases and taking on average 4 different prescribed medications.
General Characteristics of the Sample Separated by Categories of Perceived Health a .
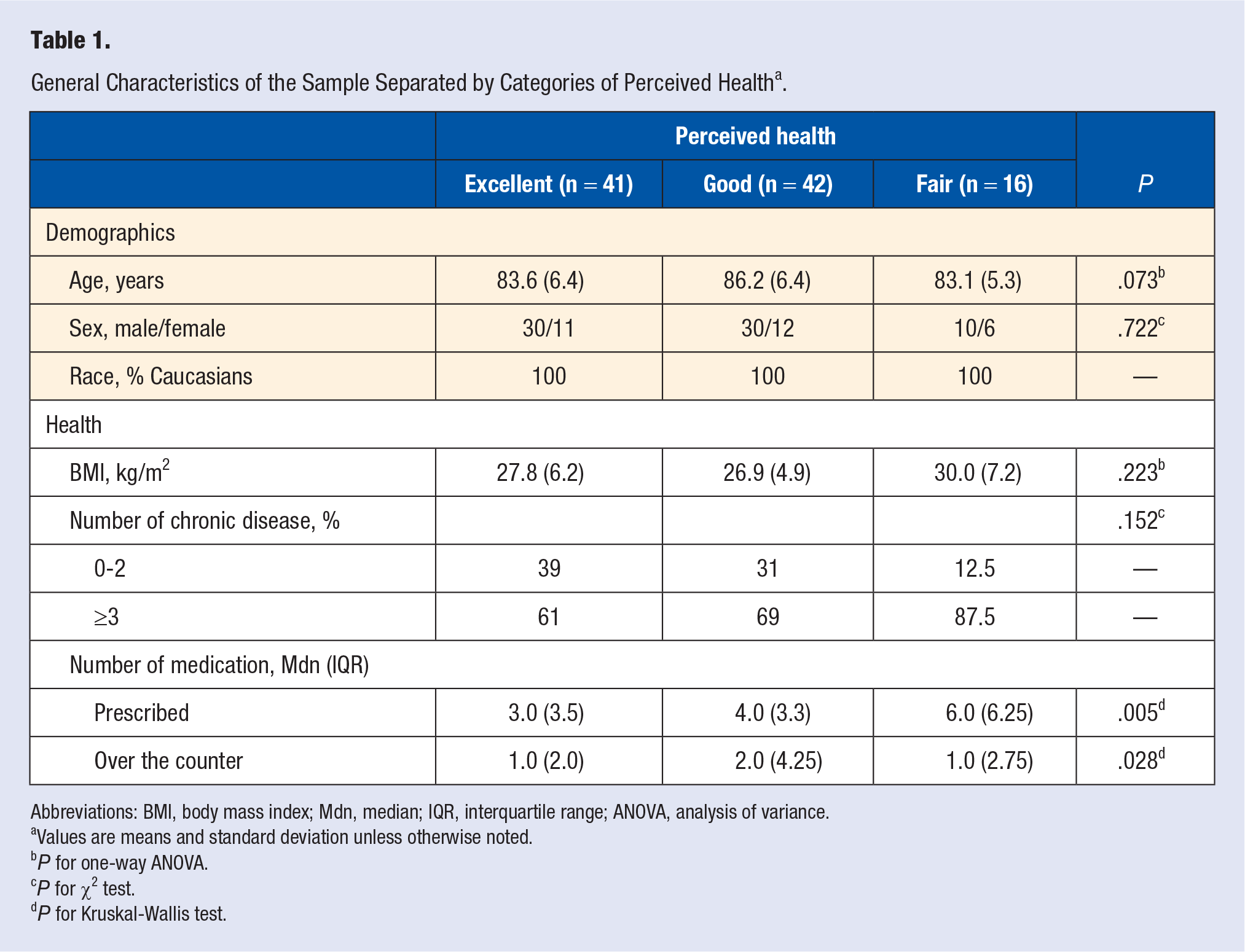
Abbreviations: BMI, body mass index; Mdn, median; IQR, interquartile range; ANOVA, analysis of variance.
Values are means and standard deviation unless otherwise noted.
P for one-way ANOVA.
P for χ2 test.
P for Kruskal-Wallis test.
Information on PA and PF is given in Table 2. Briefly, ANOVA revealed a significant difference (P < .05) on PA and PF among categories of perceived health.
Descriptive Values for Physical Activity and Physical Function of Older Adults and Results of the Analysis of Variance and Post Hoc Tests.
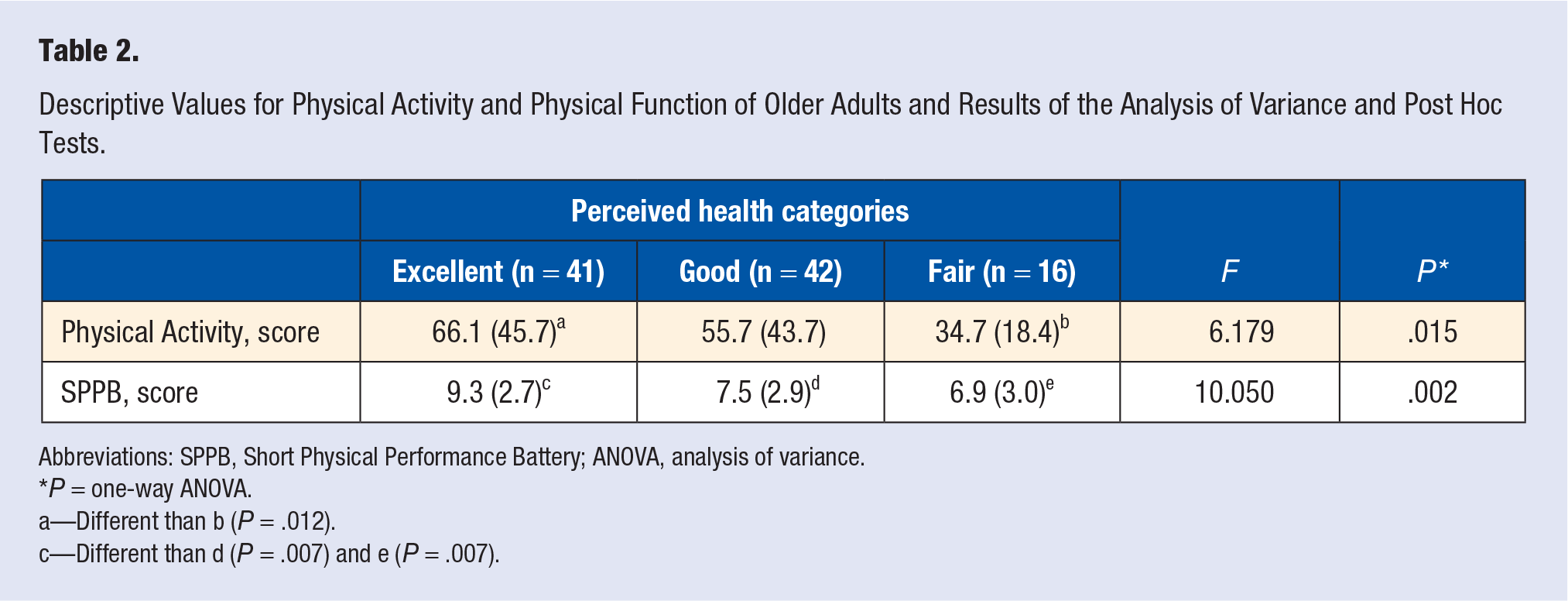
Abbreviations: SPPB, Short Physical Performance Battery; ANOVA, analysis of variance.
P = one-way ANOVA.
a—Different than b (P = .012).
c—Different than d (P = .007) and e (P = .007).
Covariate Analysis
Figure 1 displays the estimated marginal means for the SPPB assessment by categories of perceived health. Because PA has an impact on PF and revealed to be significantly different among categories of perceived health, we conducted analysis of covariance with contrast analysis to determine differences in PF (SPPB scores) as a function of perceived health category controlling for PA scores and BMI. The contrast analysis revealed a significant difference among perceived health categories on PF level measured using the SPPB, F(2, 92) = 4.349, P = .016.
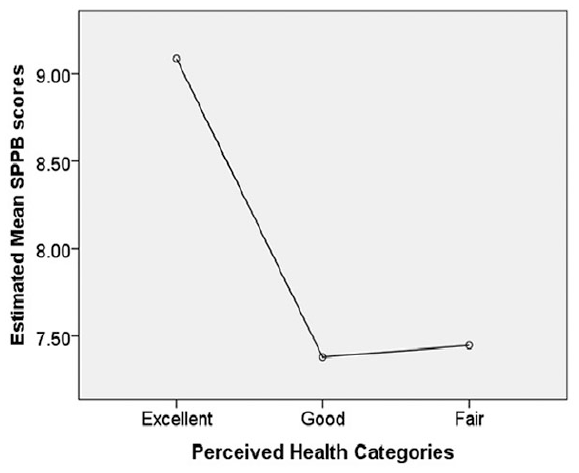
Estimated marginal mean scores for physical function measured using the Short Physical Performance Battery (SPPB).
Discussion
The present study examined differences in PA and PF performance among categories of perceived health in older adults living in a retirement community. We observed that older adults perceiving their health as excellent reported significantly higher levels of PA and better PF performance than those who perceived their health to be good or fair. Similar findings were observed for those reporting their health as good compared to their counterparts reporting it as fair. Our findings further demonstrated that even after controlling for PA levels, PF performance remained significantly different among perceived health categories. These findings corroborate our hypothesis that older adults perceiving their health as excellent would present with high PA scores and would perform better in PF compared to those reporting their health as good and fair.
The majority of the older adults participating in the present study reported their health as excellent or good. This is consistent with previous research conducted in older adults living in the community 11 and in retirement communities. 9 By contrast, research studies conducted in dependent-care facilities (eg, nursing homes) and nonagenarians living in the community observed a significant amount of their participants reporting their health as fair or poor.13,31 For instance, one study found that 62% of Brazilian nonagenarians reported their health to be poor. 31 Similar findings were observed by Eifert et al, who reported that over 50% of the older women in their study perceived their health to be fair or poor. 13 Other studies have revealed that a lower percentage of women rate their perceived health as favorable compared to their male counterparts.10,11 One study explored gender-related differences in psychosocial determinants of self-perceived health among older adults living in nursing homes. Assessing over 500 older adults (70% women), the authors observed that overall only 9.4% of women reported their health as excellent or good compared to 17.7% of men. 32 Further analysis separated by age group revealed a similar pattern for the 65 to 74 and 75 to 84 years age groups—where less women perceived their health as excellent or good compared to men. However, a different pattern emerged when observing the 85 years and older age group. That is, a higher percentage of women (43.5%) perceived their health as excellent or good compared to men (13.6%). 32 Collectively, it appears that in general, perceived health is a function of age for some age groups, residential status (ie, older adults living in the community vs those living in x nursing homes), and/or gender. That is, the oldest older adults, those that reside in dependent-care facilities (ie, nursing homes), and women perceive their health to be poorest.
We observed that PA was associated with perceived health in our study, meaning that those reporting their health as excellent, reported higher PA compared to their counterparts reporting it as either good or fair. This is consistent with other studies assessing the relationship between perceived health and PA in different populations of older individuals.11,13 For example, Eifert et al 13 assessed the relationship between a number of personal, social, and behavioral factors (ie, age, BMI, disease, financial security, spiritual satisfaction, marriage status, smoking, and PA) and perceived health status in an all-female older adult population. The authors observed that PA was the second strongest predictor of perceived health status (doctor-diagnosed diseases was the strongest predictor). Fonta et al 11 found that 74% of older adult Ghanaians, who engaged in moderate exercise, reported their health as good compared to only 26.5% of their physically active peers reporting their health as poor. Similarly, Garatachea et al 33 found significant relationships between several measures of PA (eg, total activity time, weekly energy expenditure, vigorous activity) and older adults’ ratings of well-being. The relationship between physical activity and health is well established.14-16 PA has been recommended for individuals of all ages, including older adults and people with chronic diseases14,15,34 as it is considered a key behavior for optimal health. Although we cannot stablish a cause-and-effect relationship due to the nature of the study (cross-sectional), our findings reinforce the benefits of PA for older adult’s health and underscores the need to develop strategies and interventions in retirement communities using PA, especially for those reporting their health as fair.
We further observed an association between PF (SPPB scores) and perceived health, where better perception of health was associated with better PF performance. Debpuur et al 10 assessed the relationship between self-reported health and functional limitations in older adults. They found that the proportion of older adults reporting poor health was much higher among those reporting lower functional ability. Similarly, Garatachea et al 33 revealed significant correlations between numerous assessments of PF (ie, chair stand, arm curl, agility) and older adults’ ratings of well-being. Taken together, the findings of different studies suggest a consistent association between perceived health and PF. Collectively, the findings may help devise interventions focusing on improving PF (eg, PA and exercise interventions) in older adults as it has been shown to have a close relationship with health perception in this population.
The present study focused on relationships between perceived health, physical activity, and physical functioning of older adults living in a retirement community. Previous studies have mostly focused on correlates of perceived health of community-dwelling older adults. It is important to understand the unique experiences of those residing in retirement communities and related settings as this population will certainly increase in time. Furthermore, retirement communities constitute a crucial setting for the development of accessible and feasible strategies and interventions aiming to improve residents’ overall health. For example, PA interventions can be tailored for a variety of populations, including health and diseased older adults. In fact, PA has been regarded as a key component to achieve optimal health and well-being, and highly recommended for this population. 14 Interventions focused on increasing PA in retirement communities are especially important because environmental factors are strongly linked with PA participation.35,36 For instance, a literature review demonstrated consistent associations between PA and perceptions of accessibility, opportunities, and the aesthetics of the environment among older adults. 36 In retirement communities, residents may be prevented from partaking in several types of activities due to setting logistics and rules. One study conducted in retirement communities observed that shops far away, unfamiliar surroundings, no indoor exercise facility, discouraging relationship with family, and no encouragement from staff were some of the barriers to PA reported by women living in retirement communities. 35 Interventions to increase PA in this population are further important because there is evidence suggesting older adults living in retirement communities engage in about 10 hours of sedentary activities per day. 20
Thus, due to the challenges faced by older adults living in retirement communities, it is paramount that interventions focused on increasing PA in this population be multilevel. This means that interventions should focus on different levels/domains such as individual, interpersonal, environmental, and policies (eg, training individuals to advocate for improvements in their physical and social environment). This is reinforced by a research study protocol where the authors proposed a multilevel ecological intervention for PA in retirement communities that addresses individual, interpersonal, and community influences on behavior change. 37
The findings of the present study should be interpreted with caution due to limitations. Our data comes from only one retirement community that could be regarded as wealthy. We do not know if we would find similar results in other retirement communities or communities with different backgrounds. In addition, our study had a very homogenous racial/ethnic make-up (100% Caucasian older adults). We further adopted a self-reported measure of PA. It is well-known that self-report measures of PA tend to overestimate PA levels. Future studies should attempt to replicate our findings using objective measures of PA such as accelerometer, including retirement communities with different backgrounds (eg, different socioeconomic status) and heterogeneous samples of older adults (eg, mix of race/ethnicity and those whose residents represent concentrated minority groups [eg, Hispanic-Latino or African American]). This would help us better understand different factors that may contribute to perceptions of health and its relationships with PA and PF. Another limitation of our study lies in the use of a single measure of PF. Although we used an objective measure of physical functioning (ie, SPPB), we did not use variety of widely used tests (eg, TUG, walking speed, agility). Future studies should take a similar methodological approach but include a collection of measurements of PF. Despite these limitations, we were able to engender important information that may help in the development of more effective strategies focusing on improving the overall health of older adults living in a retirement community. A possible intervention would be the implementation of a program focusing on increasing PA levels of this population. This would potentially have a significant impact on older adult’s health and consequently quality of life.
Overall, we observed that older adults living in a retirement community that perceived their health as excellent report higher levels of PA and performed better on an objective measure of PF compared to their counterparts reporting their health as good and/or poor. Due to well-known benefits of PA in maintaining or improving PF, and overall health and quality of life, strategies and intervention focusing on promoting PA, targeting those perceiving their health as fair/poor should be considered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dean’s Office, College of Education, Northern Illinois University (Dean’s Research Grant CoE-NIU 2017-2018).
Ethical Approval
This study represents a secondary data analysis from a previous study that received IRB approval (IRB Protocol # HS18-0011).
Informed Consent
Based on the ethical approval statement above, informed consent was collected from all participants in the previous study prior to data collection.
Trial Registration
Not applicable, because this article does not contain any clinical trials.