
Abstract
The field of Lifestyle Medicine (LM) is growing rapidly as individuals and communities seek real solutions to the hardship of chronic disease. Providers across various medical specialties and allied health professions are gaining certification in this field, and yet are struggling with implementation. Time constraints, concern about reimbursement, and lack of clinical experience in counseling patients are often cited as obstacles. This article will address these issues and demonstrate how LM can be successfully practiced in a standard primary care setting. Active participation in the local community is essential. Office visits must be prepared for efficiently, and encounters should focus on teaching simple concepts to patients. At-home learning activities can then be used to build on these concepts. Referral to health coaches and outside programs are helpful options as well. Equipping providers with practice tools to promote lifestyle change will improve satisfaction for patients and providers alike and is an important step toward advancing the field of LM.
Keywords
‘. . . the challenge for today’s practitioners has shifted toward being able to successfully translate LM principles into clinical practice.’
Historically, practicing Lifestyle Medicine (LM) successfully was contingent on conducting original research, publishing a book, presenting at conferences, earning celebrity status, and starting a private practice. The early pioneers embraced this and helped pave the way for current LM practices. As the field of LM is now well established, the challenge for today’s practitioners has shifted toward being able to successfully translate LM principles into clinical practice.
Much is known about the benefits of lifestyle change for prevention and reversal of chronic disease, but providers lack the tools necessary to convey this information to patients in an effective and efficient manner. Time constraints as well as lack of training and confidence in counseling present barriers. 1 Furthermore, many primary care providers have not yet built the interdisciplinary team and community network necessary to assist their patients, or may lack the support of their broader health system to begin to build this structure. Although these obstacles are challenging, they can be overcome with a well-planned approach to a LM clinic.
Considerations for Building a LM Practice
The look and feel of LM practices can vary substantially. Successful models range from private practices, to extended retreats, to large academic centers, to community-based programs.2-5 Any of these approaches can work but a successful transition requires a vision of how the clinic will operate and how care will be delivered. The LM model described in this article represents a culmination of experiences as a trainee in a variety of LM models, as well LM oriented rotations such as bariatrics, pediatric obesity clinic, and oncology survivorship. It is a LM hybrid positioned within a traditional Family Medicine practice in a large hospital system. Utilizing the conventional fee-for-service model, insurance is billed using standard Evaluation and Management (E&M) codes with typical ICD-10 (International Classification of Diseases, 10th Revision) current procedural terminology (CPT) codes. While many factors ultimately contribute to the success of a LM practice, the following pearls can enable one to transition to a prosperous LM practice.
Starting a LM practice is difficult without first creating some name recognition and demand. The “Lifestyle Medicine” label is a great start; certification will pique the interest of both employers and the public. Beyond that, there are many ways to captivate the local community:
Health clubs, libraries, places of worship, local restaurants, educational programs, public events, and health fairs are often looking for speakers.
A talk on reversing diabetes may appeal to the Endocrinology department, or the Oncology department may enjoy a discussion of plant-based nutrition for optimizing cancer outcomes.
Cardiologists and other specialists are often looking for effective primary care practitioners for their patients. Taking the time to build relationships with other providers can pay dividends for an individual practice and can lead to more aligned treatment plans for patients.
For the savvy individual, social media can be highly effective, at little cost. Connect with other similarly minded individuals and groups on these platforms as well.
Create a space with a few shelves in the clinic and have the local used bookstore keep an eye out for works from preferred authors. Ask a health-oriented local restaurant to put a crate out to collect donations. Invite patients and the broader community to exchange books, cookbooks, and DVDs as they please.
Get to know like-minded professionals such as plant-based chefs, yoga and tai chi instructors, or mindfulness and meditation teachers. This can lead to valuable collaborations and professional relationships.
LM certification is offered as an adjunct to those who are already credentialed in another specialty or profession. 6 Within Family Medicine, LM can be practiced in a manner that overlaps with the scope of this field. This is particularly important for billing, as reimbursement is generally poor for strictly LM-specific codes (eg, obesity counseling 7 ). Practicing in a traditional Family Medicine setting allows a provider to maintain a full schedule while building the LM side of the practice.
A thorough previsit patient form will help to obtain relevant information prior to the encounter, so that visit time can instead be spent on counseling and developing a plan. Include questions that pertain to a typical medical history, lifestyle behaviors, and a patient’s health goals (Figure 1).
In order to have a sustainable practice, one cannot spend 60 minutes personally educating each patient and answering every question that arises. Current insurance payment models limit the time that providers have available. Curating a collection of LM teaching aids and using them to convey simple concepts in the office is effective and efficient. Examples of simple, teachable concepts include: Hyperlipidemia: Start by using a 1-page chart to show how a patient’s cholesterol levels compare to average levels.
8
Follow this by reviewing a 1-page teaching aid explaining that cholesterol is only found in animal-based foods, and fiber, which helps to reduce our cholesterol, is only found in plants. Overweight/Obesity: Review a 1-page teaching aid on calorie density and how food volume generally increases satiety.
8
Food addiction behaviors: Explain how hyperprocessed foods are designed to be addictive and show an infographic that outlines wholesome foods to focus on instead.
9
This can transform the patient’s approach from a restrictive one to one that emphasizes incorporating healthier foods. This will help to limit consumption of processed foods. Diabetes: Few patients are aware that type 2 diabetes can be a reversible disease. Consider showing a short video to patient waiting to see a provider that shows how a plant-based diet can actually reverse insulin resistance.
10
Additional teaching aids and educational handouts are available on the American College of Lifestyle Medicine (ACLM) website
8
as well as from various other LM groups.
11
This is where the majority of the learning occurs. Once simple concepts are taught in the office, patients are inspired to learn more. Using books,12-14 video clips, 15 smart phone applications, 9 or other resources 16 as at-home learning activities can reinforce and expand on LM concepts that are taught in the office.
This “flipped classroom” style of learning has been shown to be an effective and efficient teaching method, allowing more time for face-to-face problem solving and collaboration. 17 Images of book covers and other resources can be printed 4-per-page, cut out, and handed to the patient at the end of the visit. Alternatively, a 1-page master list of favorite resources can be created, and recommended resources for specific patient can be highlighted during the encounter. These will serve as tangible reminders for the patient after the office visit.
Throughout this process, the provider acts as a guide and the majority of the learning is done independently by the patient. This is integral in helping patients make lasting lifestyle changes. At follow up visits, provide additional resources as the patient advances, or help them to set S.M.A.R.T. goals. These are detailed goals that are specific, measurable, achievable, relevant, and time-based. 18 Providing these tools help patients remain goal-directed and engaged between office visits.
The majority of encounters can be billed as 99203 or 99204 for new patients and 99213 or 99214 for established patients, with standard ICD-10 diagnostic codes (eg, cancer, diabetes, dyslipidemia, heart disease, or hypertension). For greatest efficiency, encourage couples to schedule appointments together, which allows for more counseling time. When cancellations leave extra time for other patients, billing for time with 99214 (25-minute encounter, with greater than 50% of the time spent in counseling) or 99215 (40 minute encounter, with greater than 50% of the time spent in counseling) can be utilized. Allot 15 to 20 minutes for the majority of office visits, as is typical for primary care encounters, and plan a double slot for new LM patients. Group visits can serve as adjunct practice offerings and are an effective and time efficient method for practicing LM as well. 18 While some feel that the traditional fee-for-service system is not financially sustainable for a LM practice, the above methods have resulted in greater productivity as compared with that of strictly Family Medicine peers.
For patients who require a higher level of support, refer to outside resources. Identify local health coaches that understand plant-based nutrition and the other pillars of LM. Community engagement and networking will help to uncover these individuals. Also, consider referring to community programs for exercise, smoking cessation, addiction, and other lifestyle-related interventions. There may be a Physician’s Committee for Responsible Medicine Food for Life class in the local community, a YMCA with a Silver Sneakers program, or a smoking cessation class offered at the local hospital system. Last, consider referral to online programs, such as Mastering Diabetes or to online health coaches who teach plant-based nutrition. A comprehensive LM program may not exist in the community, but oftentimes the elements can be pieced together.
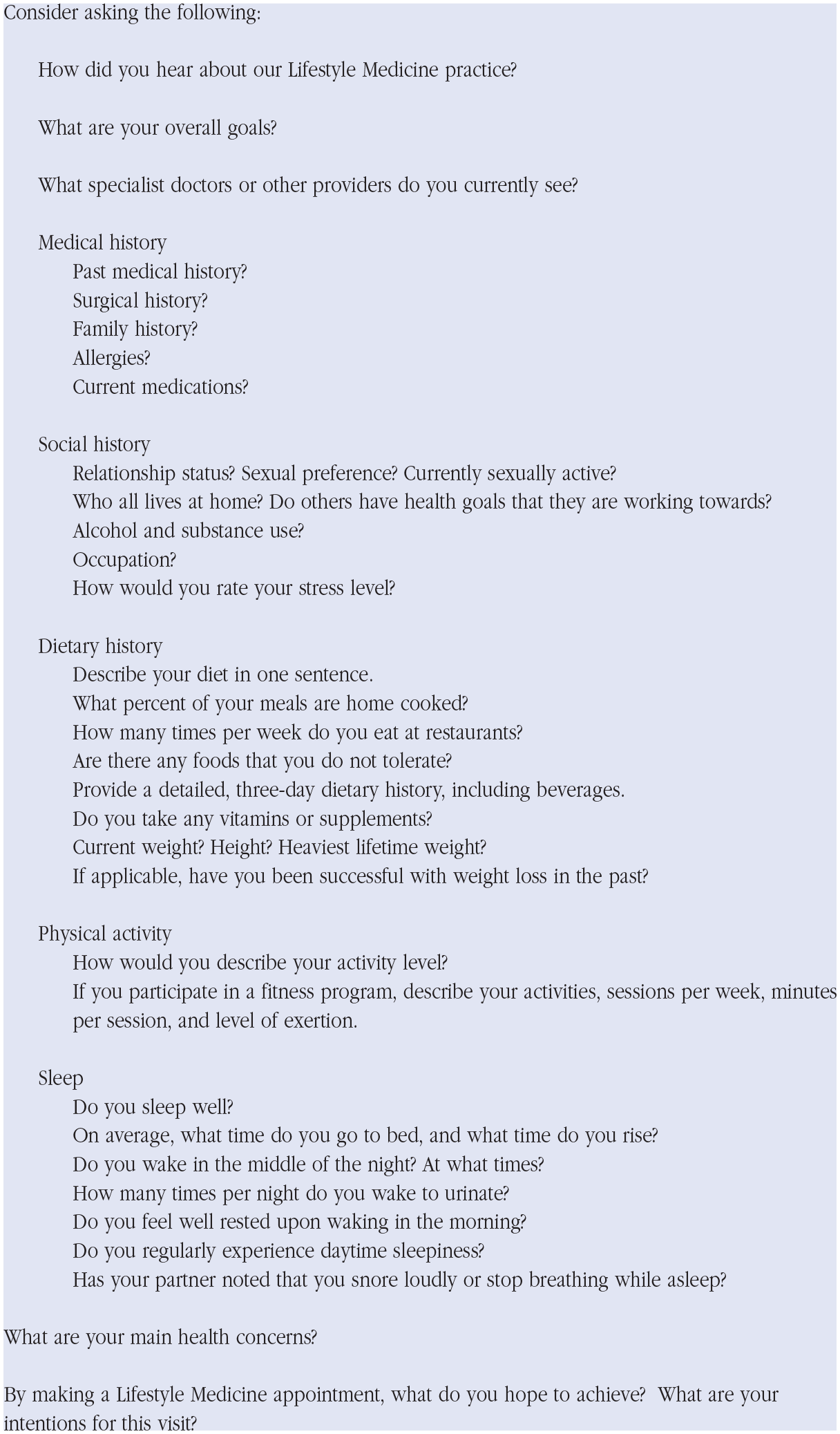
Lifestyle Medicine intake form questions.
Conclusion
Most LM programs begin on a smaller scale. The methods discussed here can be used to lay the foundation for a variety of program styles, ranging from a solo practice clinic, to a heart disease reversal program, to a multimillion-dollar comprehensive LM center. Involvement in the community, efficient use of time during the office visit, and utilization of teaching aids, at-home learning activities, and community referrals are essential. The tools and resources to develop a thriving LM practice in any community already exist. Embracing these can lead to greater fulfillment for providers and improve the health of patients and communities alike.19,20
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
{kind=link}