
Abstract
This study assesses family physicians’ perceptions and utilization of LM principles in their primary care practices, and identifies reported barriers to implementation.
Most participants perceived the importance of LM core competencies and felt comfortable with practicing lifestyle interventions
Background
Lifestyle medicine (LM) is an evidence-based approach to preventing, treating, and reversing diseases by replacing unhealthy behaviors with positive ones. 1 It focuses primarily on 6 domains: eating healthfully, being physically active, managing stress, avoiding risky substance use (tobacco, alcohol, and illicit drug use), getting adequate sleep, and having healthy relationships or a strong support system. 1 Some lifestyle medicine societies also incorporate broader social determinants of health, like social and environmental factors, poverty, health inequity, and social isolation. 2 The goal of LM is to use therapeutic lifestyle behavior change as the primary modality to address the root cause of chronic disease. Lifestyle interventions are relatively inexpensive,3,4 accessible, and have been shown repeatedly to be effective in preventing, 5 treating,6-8 and in some cases, reversing chronic disease.9,10 Approaches to behavior modification like LM will become even more important as the burden of chronic disease continues to rise in both high- and low-income nations. 11
In the United States (U.S.), 60% of adults have at least one chronic disease, and 40% have more than one. 12 Chronic disease is the leading cause of death and disability and is responsible for $3.5 trillion in annual healthcare costs. 13 If costs continue to increase, Medicare and Medicaid alone will account for 20% of the U.S. gross domestic product. 14 The rise in chronic disease burden and its impact on healthcare costs, productivity, quality of life, and society as a whole is unsustainable. However, up to 80% of all chronic disease is preventable. 15 Furthermore, lifestyle and social determinants of health account for approximately 70% of population health. 16 This is highlighted in a prospective study of over 23000 adults that found people who never smoked, had a body mass index less than 30 kg/m2, performed 3.5 hours per week or more of physical activity, and adhered to healthy dietary principles had a 78% lower risk of developing a chronic disease compared to those who did not meet any of these factors. 17 Solutions to the chronic disease epidemic, such as LM, are needed.
Family physicians are well positioned to practice LM and lead efforts to reduce the burden of chronic disease. They also are uniquely trained to provide care to people and families throughout the entirety of their lives. 18 These long-term relationships with their patients and their families can help them adopt and maintain healthy lifestyles as they age. Family physicians already value whole-person, patient-centered care. The principles of LM are aligned with the values of family medicine and being well versed in the use of lifestyle modification as the first-line treatment not only expands the family physician repertoire but also meets patients’ expectations. 19 While the principles of LM can be incorporated into any medical specialty, it is particularly suited for primary care specialties and family medicine. Several studies have shown that counseling by primary care physicians is effective at helping their patients modify behaviors such as attempting to lose weight,20,21 increasing physical activity,20,22,23 and improving diet. 24
However, there have been gaps in the practice of lifestyle counseling interventions as only one-third or less of patients receive lifestyle counseling (such as diet or exercise) during ambulatory visits.25-27 Insufficient training or poor physician education has been cited by several studies as a major barrier to incorporating lifestyle counseling into clinical practice.26,28 For instance, the National Academy of Sciences (NAS) recommended for a minimum of 25 hours of nutrition instruction for medical students in 1985 to adequately prepare physicians to address nutrition concerns of their patients. 29 Yet, a survey in 2008-2009 found medical students receiving only an average of 19.6 contact hours of nutrition instruction over the course of 4 years of medical school. 29 Hence, the blue ribbon panel meeting hosted by the American College of Preventive Medicine garnered the consensus in 2009 that all practicing primary care physicians should possess the knowledge, skills, attributes, and values on 15 core competencies of LM; these competencies being categorized under various headings such as leadership, knowledge, assessment skills, management skills, and use of office and community support. 30
Although there is increasingly available research in LM, its implementation is still relatively new within conventional medicine. While family physicians are well positioned to practice LM, there is relatively little information available about family physicians’ perceptions of LM, perceived use of LM principles in practice, and perceived barriers of implementing LM. A recent study has cited the financial concerns, patient preference, and social resistance to change along with poor physician education as major barriers to incorporating LM into clinical practice and hospital systems.
28
More data is needed to identify when the opportune time is and how to best address these issues during medical training and beyond to better equip physicians to address the chronic disease epidemic at the patient and population levels. The purpose of this study was to assess family physician’s perceptions and utilization of LM principles in their primary care practices, as well as identify reported barriers to implementation. The specific questions to be addressed included the following: 1. What is the gap between the perceived importance and reported use of LM core competencies among family physicians? 2. What is the gap between the perceived comfort with and reported practice on the domains of LM among family physicians? 3. What characteristics of family physicians, their practices, and communities are associated with the reported use of LM practices? 4. What barriers do family physicians perceive to practicing LM?
Methodology
Study Design and Data Collection
This study employed a cross-sectional design utilizing a survey. The survey was administered between February and April 2021, during the COVID-19 pandemic, to family physicians registered with the American Academy of Family Physicians (AAFP). The survey questionnaire was mailed to 5770 family physicians. Among these family physicians, 4498 were also emailed the survey. In addition, two email reminders were sent. The data files for mail and online were combined, and duplicate IDs were identified. The record with the most questions answered was retained in the event surveys were received with the same ID. If the surveys were both complete, the survey with the earliest date was retained.
The survey questions contained three sections. The first section assessed the perception and practice of lifestyle medicine core competencies. We used nine core competency items in this survey. The participants were asked to rank the importance of these core competencies using a four-point scale from “not at all important” to “very important.” The scale was later converted into a binary variable, either “very important or important” and “not very important or not important at all.” Participants were also asked if they used these core competencies in their practice “regularly” or “‘some of the time.” The binary variable for this scale included “any reported practice, i.e., regularly or some of the time’ and ‘no reported practice.”
The second section assessed the perception and practice on 6 domains of lifestyle medicine. Physicians were asked about how comfortable they felt in prescribing these interventions using a four-point scale from “not at all comfortable” to “very comfortable.” This was converted into the binary variable “very comfortable or comfortable” and “not very comfortable or not at all comfortable.” Similarly, the participants were asked to rank their practice on these domains using a four-point scale from “never” to “every visit/almost every visit.” The binary variable for this scale included the options, “every visit, almost every visit, or most visit” and “some visits or never.”
The third section assessed the physicians’ perception of barriers to incorporating lifestyle medicine into their practice. The physicians’ responses on barriers were ranked using a four-point scale ranging from “to no extent” to “to a great extent.” This section also examined the roles of team members who were most likely to engage in lifestyle medicine interventions.
The basic socio-demographic characteristics of respondents were linked from the AAFP database using their AAFP ID. We used the 2015 Social Deprivation Index (SDI) at the ZCTA level (developed by Robert Graham Center) and matched the SDI scores with the zip codes we collected during the survey. 11 The SDI scores were developed based on seven demographic characteristics: poverty, education, single-parent household, rental housing, overcrowding, households without cars, and unemployment. The composite scores ranged from 1 to 100, the higher score indicating greater social deprivation. 31
Data Analysis
Descriptive statistics were used to summarize socio-demographic characteristics of the participants. The percentages and confidence intervals were calculated for each item under the first and second sections that involved assessment of perception and practice of LM core competencies and LM domains, respectively. The gap in practice of LM core competencies was considered if physicians reported any of the items listed under core competencies as “important or very important” but were not practicing it for any amount of time. Likewise, the gap in the practice of LM domains was considered if physicians reported being comfortable or very comfortable in prescribing any elements of LM domains but did not report practicing them regularly, that is, during almost every visit, every visit, or most visits. Any participant who did not respond to all the items under each section was dropped from that particular analysis.
The mean scores of the eight items (ranged between 1-4) under the practice of LM domains were combined to create a mean composite score. We evaluated the reliability by calculating Cronbach’s alpha, which was .85, indicating a good reliability for the combination of items. The higher mean composite score represented the higher frequency of practice of LM domains. We then used this mean composite score to examine whether any family physician, practice, and community characteristics affected the practice of lifestyle medicine interventions. A linear regression model was used to examine the association between the practice of LM and each of the characteristics mentioned earlier. Any variable with a P-value of .25 or less in bivariate analysis was included in a multiple linear regression model. Even though the findings from bivariable analysis for ownership, urban/non-urban residency, and Social Deprivation Index made them eligible for the multivariate model, we did not include these variables in the multivariate model because substantial observations were missing. For ease of interpretation, mean composite scores for various groups were reported rather than the regression coefficients. This was calculated using STATA’s predict command.
Lastly, the percentages and confidence intervals for the perceived barriers to incorporating lifestyle medicine into practice and team members who were most likely to engage in LM interventions were calculated.
Statistical Significance was Set at P-value of < .05
All the statistical analysis was conducted using STATA version 16.1. 32
Ethical Considerations
The ethics approval was obtained from the American Academy of Family Physicians’ Institutional Review Board, Protocol Number 20-400. Written informed consent was obtained from the participants and the responses from the participants who did not provide consent were excluded from the findings.
Results
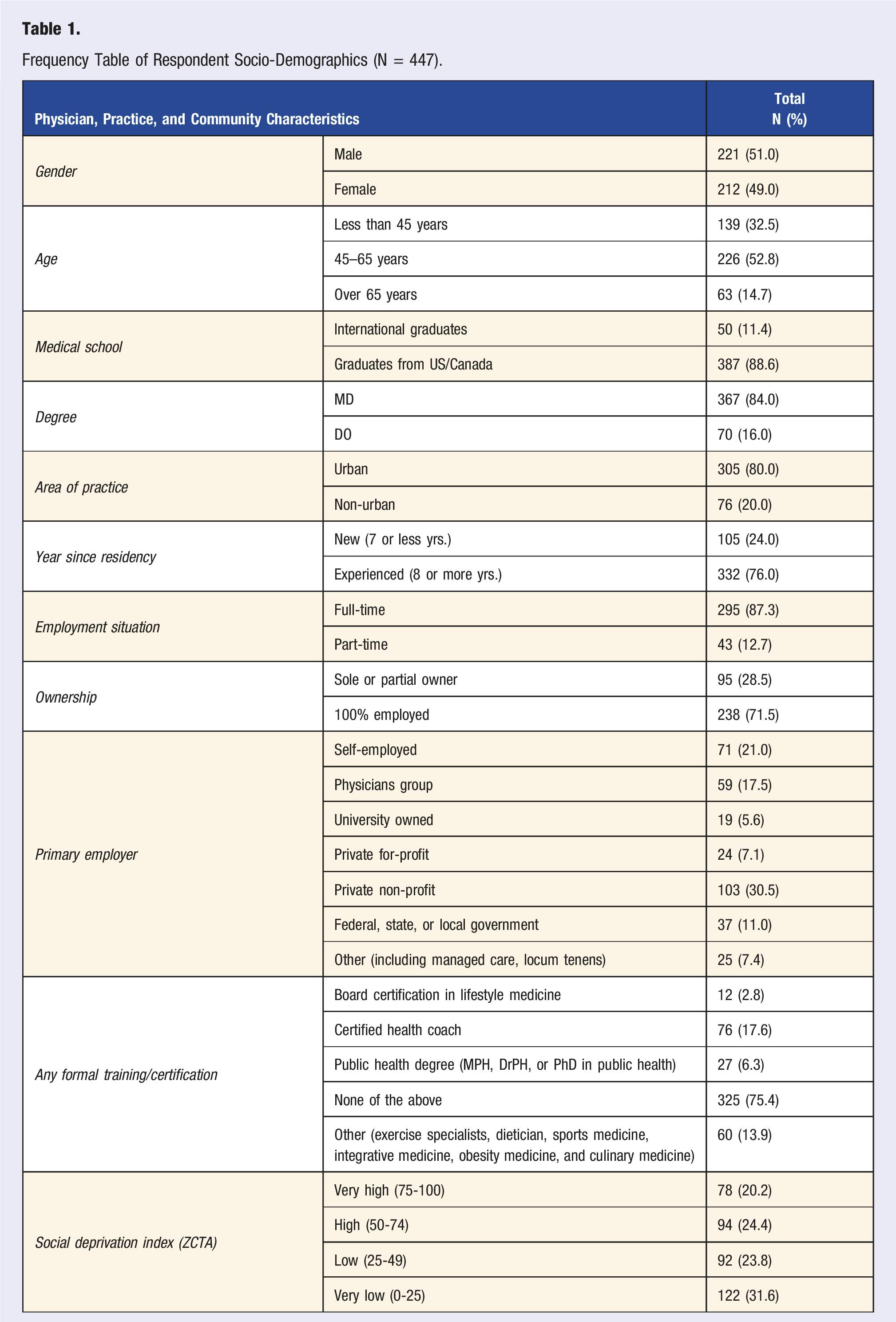
Frequency Table of Respondent Socio-Demographics (N = 447).
Gap Between Family Physicians’ Perceived Importance and Reported Use of LM-Related Core Competencies.
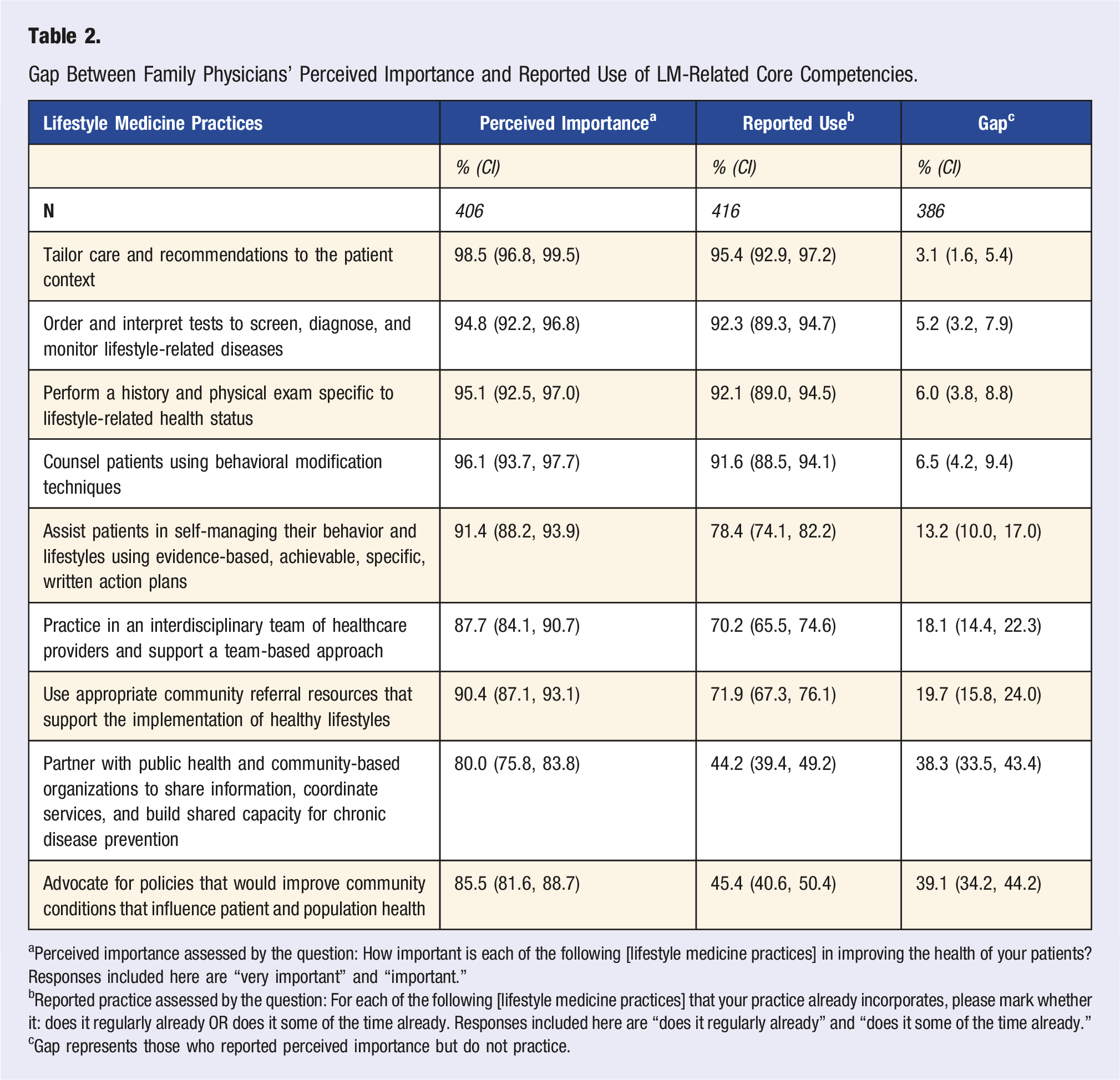
aPerceived importance assessed by the question: How important is each of the following [lifestyle medicine practices] in improving the health of your patients? Responses included here are “very important” and “important.”
bReported practice assessed by the question: For each of the following [lifestyle medicine practices] that your practice already incorporates, please mark whether it: does it regularly already OR does it some of the time already. Responses included here are “does it regularly already” and “does it some of the time already.”
cGap represents those who reported perceived importance but do not practice.
Gap Between Family Physicians’ Perceived Comfort with and Reported Use of Lifestyle Medicine Domains.
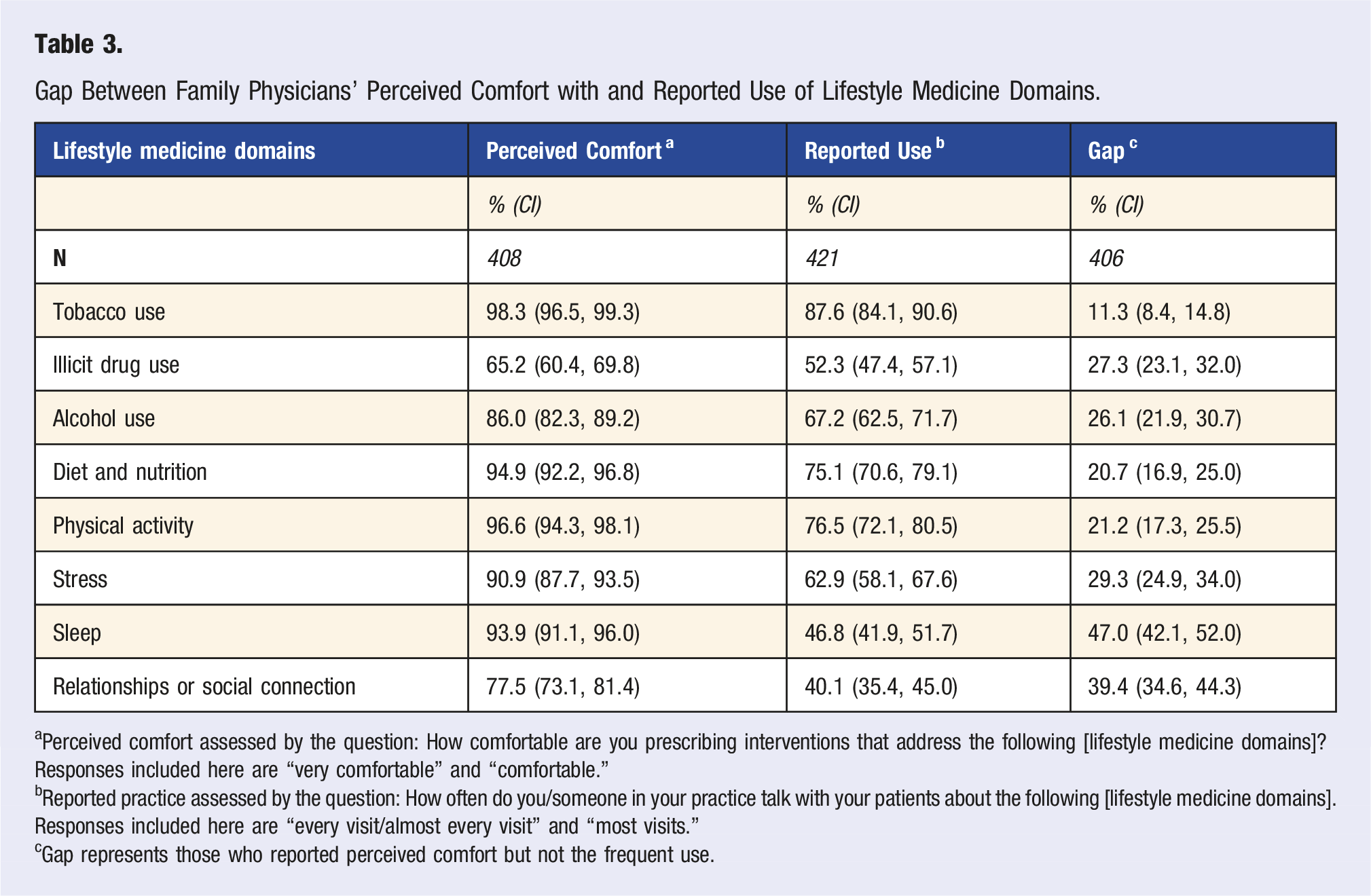
aPerceived comfort assessed by the question: How comfortable are you prescribing interventions that address the following [lifestyle medicine domains]? Responses included here are “very comfortable” and “comfortable.”
bReported practice assessed by the question: How often do you/someone in your practice talk with your patients about the following [lifestyle medicine domains]. Responses included here are “every visit/almost every visit” and “most visits.”
cGap represents those who reported perceived comfort but not the frequent use.
Family Physician, Practice, and Community Characteristics Affecting Use of Lifestyle Medicine Practices.
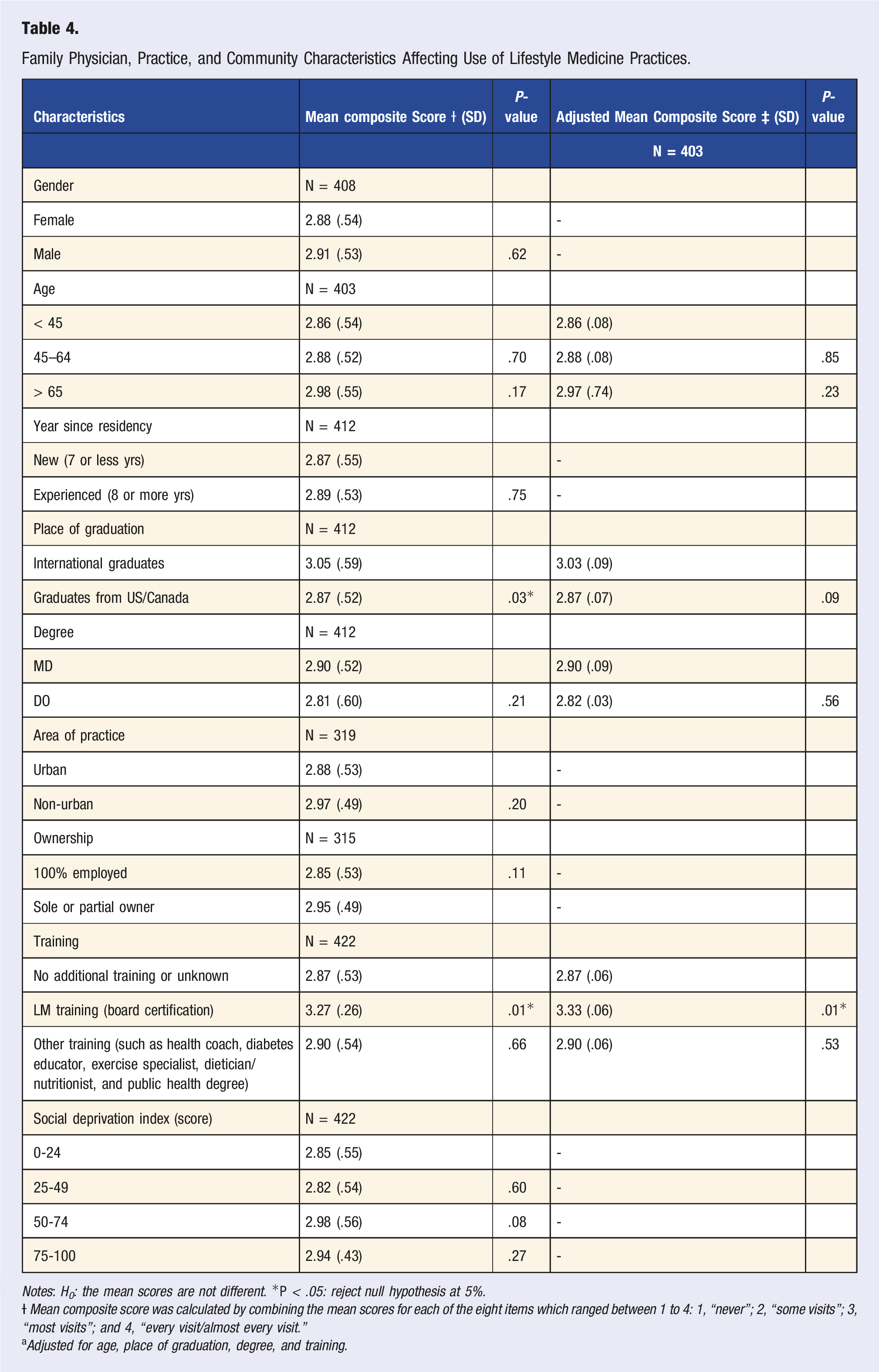
Notes: H 0 : the mean scores are not different. *P < .05: reject null hypothesis at 5%.
aAdjusted for age, place of graduation, degree, and training.
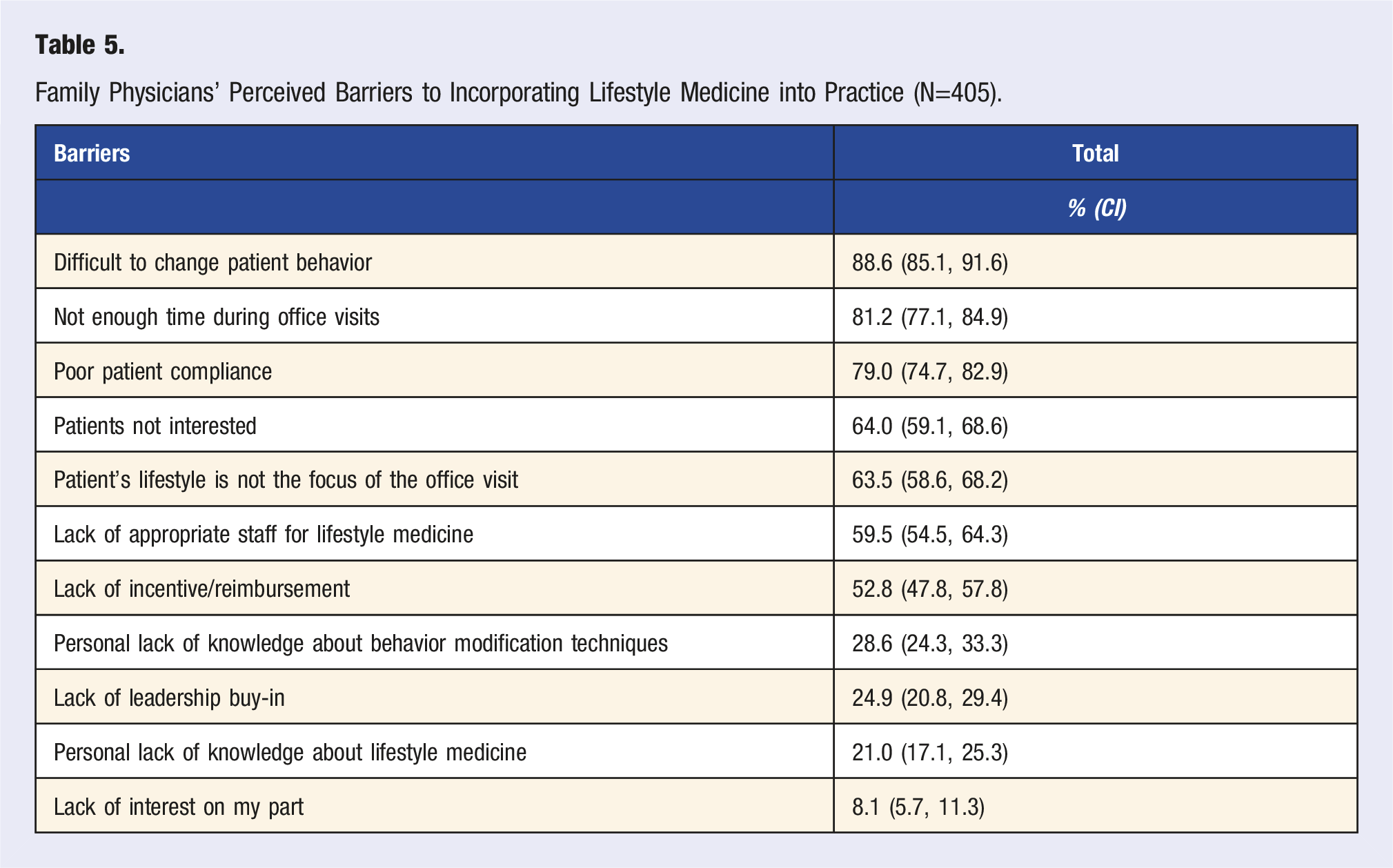
Family Physicians’ Perceived Barriers to Incorporating Lifestyle Medicine into Practice (N=405).
In terms of team members most likely to engage in LM, 73% of respondents reported that they or other physicians in their practice are practicing lifestyle interventions in their patient care. Thirty-one percent reported the involvement of nurse practitioners or physician assistants, 22% reported the involvement of nurses, and 14% reported involvement of other team members such as dieticians or nutritionists, behavior health counselors, pharmacists, case managers, social workers, or health coaches (see Figure 1). Team members engaged in lifestyle in interventions.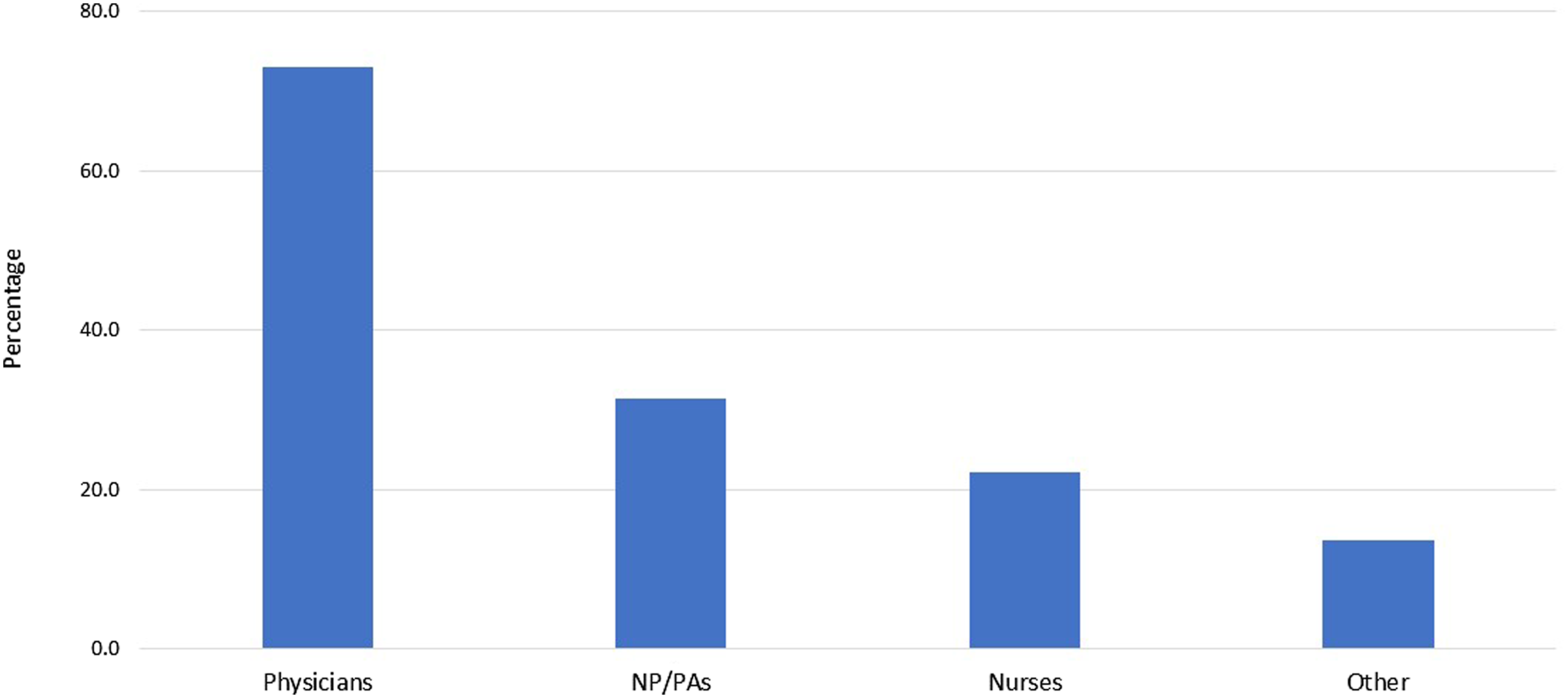
Sensitivity analysis: We conducted a subgroup analysis between online and paper respondents to see whether the mode of response affected the practice of LM domains. Like overall analysis, we found a significant association between LM board certification and LM practice among the paper respondents. Though the effect size was similar for online respondents, the P-value was insignificant for that group, which is not surprising considering the smaller sample size. (Supplementary Table 2 & 3)
Discussion
This is the first survey to elicit the perception and practice of LM among U.S. family physicians. Nearly 80% of responding physicians felt that all the LM competencies included in this survey were important, despite only 3% being board certified in LM. More than three-quarters of the family physicians reported using all of the LM principles, except for advocacy and public health or community partnerships. This suggests that lifestyle medicine concepts resonate strongly with family physicians and the clinical aspects are being incorporated into how they currently deliver care to their patients.
It is striking to find such a large discrepancy between family physicians’ values and behaviors regarding advocacy and community health partnerships. More than 80% of the participants indicated that it was important to partner with public health and community-based organizations, and to advocate for policies that would improve community conditions. However, only slightly more than half of these individuals reported actually participating in these activities. The COVID-19 pandemic may have played some role in influencing community partnerships or have shifted the focus. Needless to say, it is not surprising that physicians have gaps in partnership with public health and CBOs since public health is not usually a focus of education during medical school or residency unless specialty training is pursued, such as Master of Public Health (MPH), Master of Public Policy (MPP), Leadership Preventive Medicine Residency (LPMR), or similar. Family physicians might also not feel supported or cannot find opportunities to participate in the public policy process in their day-to-day lives. 33 In addition, partnerships with public health or community-based organizations are currently not a part of reimbursement. Shifting priorities towards community collaboration, public health education, and practice has been recognized by many organizations, including the American Medical Association (AMA). 34 The American Academy of Family Physicians (AAFP) offers multiple ways for family physicians to receive training and become engaged in public health initiatives. There are also possibilities for family physicians to get involved locally, such as engaging with school boards, food banks, homeless shelters, state medical societies, and population health department initiatives of their hospitals and clinics. Nevertheless, finding ways for organizations, government, and public health departments to effectively engage family physicians could significantly improve population health locally and nationally. Community engagement of family physicians would also capitalize on family physicians' credibility, build the trust between family physicians or healthcare organizations and community organizations, 35 and promote health equity. 36
Regarding the LM domains, at least three-quarters of physicians felt comfortable prescribing the interventions, except for illicit drug use. Physicians not feeling comfortable prescribing interventions for illicit drug use might be attributed to the complexity in identifying the patient with substance use disorder, stigma and poor attitude towards them, the lack of substance misuse curriculum in medical education, and the need for additional training.37,38 The prescription for illicit drug use may also be complicated due to the medicinal use of substances such as marijuana, psilocybin, and lysergic acid diethylamide (LSD) to treat anxiety, depression, and PTSD.39-41
It is worth noting that more than 50% of physicians do not routinely discuss sleep or social connection/relationships with patients. Upon further analysis, we found that 2% and 6% respondents reported never asking their patients about sleep and relationships/social connection, respectively. Considering the burden of sleep disorders in the general population, the scientific community suggests routine sleep assessment. 42 However, there is not a clear guideline on how often these domains need to be assessed. There is admittedly less available research exploring the impact of sleep or social connection on health outcomes relative to tobacco, alcohol, physical activity, and diet. The need for knowledge or skills discussing those topics may explain the substantial gap, as evidenced by our findings that the physicians with board certification in LM addressed these domains more frequently.
Another possible explanation for some of these gaps may be the type of barriers reported by physicians. The primary barrier cited by physicians was the difficulty associated with changing a patient’s behavior. This is followed closely by insufficient time during visits to address poor patient compliance, which closely resembles the findings from other studies. 43 These top-listed barriers go hand in hand, as making lasting behavior change requires additional time with the patient that can be challenging in a traditional practice setting. One solution could be to engage other team members beyond the physicians to play supportive roles. 44 We have found that various team members are already involved in supporting patient lifestyle interventions in family medicine practices. However, only 70% of physicians are practicing team-based care approaches. These barriers also reflect the need to help family physicians become better advocates for community change. Ecological models for health promotion already highlight the need to change the conditions in which people live in order to support effective behavior change.45,46 In an era of value-based care, it will become more important for healthcare organizations to focus on prevention in addition to treatment. Healthcare organizations may gain competitive advantage based on their ability to advocate for and change the community conditions in which their patients live that support positive behavior change. 47
Implications of the findings: The gaps in practicing specific lifestyle interventions and using particular LM core competencies suggested significant opportunities to further engage family physicians with additional education, training, resources, and support. We, however, did not find a significant difference in the practice of clinic-community partnership or advocating for public health policies with additional LM training (not presented in this study), suggesting the inability of current LM training to address these competencies. Hence, there might be opportunities to reevaluate the place for social determinants of health within current LM training curriculum and find ways to empower family physicians to address lifestyle interventions in their everyday practice.
Strengths and limitations: This is the first study to evaluate perceptions about lifestyle medicine among family physicians. The cross-sectional nature allowed for an efficient data collection process without having individuals lost to the follow up process. With almost 450 responses ascertained that are representative of the AAFP’s overall membership, we are optimistic that family physician preferences were accurately captured. Additionally, the AAFP is not an LM membership organization. We surveyed the representative members of AAFP, and most participants did not have additional training on LM. Therefore, their perceptions are potentially more generalizable to physicians who are also not versed in the LM principles. Our analysis was unique in that we are able to highlight gaps between physician perception and what they report practicing across both LM competencies and domains.
This study had several limitations. It was conducted during the COVID-19 pandemic, which may have altered perceptions and practices of the physicians being surveyed. This may have influenced who responded to the survey, their perceptions about certain issues such as mental health, or their view on the perceived inability to affect behavior change. The pandemic presumably contributed to a lower response rate than would have otherwise been seen. Our data set also had a considerable number of missing values for some participant characteristics such as ownership, area of practice, and Social Deprivation Index score, which made it challenging to include them in our multivariate regression analysis. It is possible that adjusting for these variables might affect the relationship between the practice of LM domains and training or the place of residency. The mean composite score for LM domains is higher for physicians living in non-urban areas and those who own their practice, although we do not have evidence to support these relationships.
Because of the cross-sectional nature of this study, there are no comparator time points. Hence, it is difficult to know if these perceptions resulted from recent changes to their views or clinical practice vs long-held beliefs. Furthermore, this represents a sample of physicians who are members of the AAFP. It may not accurately reflect perceptions and practices of family physicians who do not belong to this organization and may reflect the opinions of more engaged family physicians. With this study, we could only identify gaps and barriers in practicing LM, but further study is needed to ascertain why these gaps exist and what it would take to help address them.
Conclusion
Most participants perceived the importance of LM core competencies and felt comfortable with practicing lifestyle interventions. However, the gap in practice, especially in the competencies related to clinic-community partnership, community advocacy, and specific domains of LM such as sleep or relationships, suggests the additional need for training, education, and opportunities to enhance practicing these skills.
CME/CE Article Quiz
American College of Lifestyle Medicine (ACLM) members can earn FREE CME/CE credit by reading this approved CME/CE article and successfully completing the online CME/CE activity. Non-members can earn CME/CE for $40 per article. Visit lifestylemedicine.org to join the ACLM.
AJLM CME/CE Articles and Quizzes are offered online only through the American College of Lifestyle Medicine and are accessible at lifestylemedicine.org/store. ACLM Members can enroll in the activity, complete the quiz, and earn this CME/CE for free. Non-members will be charged $40 per article.
A Passing score of 80% or higher is required in order to be awarded the CME/CE credit.
Supplemental Material
sj-pdf-1-ajl-10.1177_15598276211072506 – Supplemental Material for Incorporating Lifestyle Medicine Into Primary Care Practice: Perceptions and Practices of Family Physicians
Supplemental Material, sj-pdf-1-ajl-10.1177_15598276211072506 for Incorporating Lifestyle Medicine Into Primary Care Practice: Perceptions and Practices of Family Physicians by Rajani Bharati, Kevin A. Kovach, Jonathan P. Bonnet, Polina Sayess, Elizabeth Polk, Keisha Harvey and Lauren Vorbeck in American Journal of Lifestyle Medicine
Supplemental Material
sj-pdf-2-ajl-10.1177_15598276211072506 – Supplemental Material for Incorporating Lifestyle Medicine Into Primary Care Practice: Perceptions and Practices of Family Physicians
Supplemental Material, sj-pdf-2-ajl-10.1177_15598276211072506 for Incorporating Lifestyle Medicine Into Primary Care Practice: Perceptions and Practices of Family Physicians by Rajani Bharati, Kevin A. Kovach, Jonathan P. Bonnet, Polina Sayess, Elizabeth Polk, Keisha Harvey and Lauren Vorbeck in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
We would like to acknowledge the family physicians who participated in the survey. We would also like to acknowledge the Member Insights Team within the American Academy of Family Physicians for administering the survey.
Author Contributions
RB contributed to the survey instrument design, data analysis, manuscript review and editing, and was the primary author.
KK designed the study, contributed to the survey instrument design, data analysis, and manuscript review and editing.
JB assisted with the survey instrument design, and manuscript review and editing
PS assisted with the survey instrument design, and manuscript review and editing
EP assisted with the survey instrument design, and manuscript review and editing
KH assisted with the survey instrument design, and manuscript review and editing
LV assisted with the survey instrument design, data collection, and manuscript review and editing
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ardmore Institute of Health
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.