
Abstract
There is increasing evidence that diet can mitigate fatigue. The objective of this study was to assess the associations between dietary habits and sleep-related impairment (SRI) in a cohort of community physicians. In this cross-sectional study, we analyzed data from 245 physicians who had completed a wellness survey in March 2016 (98% response rate). Three dietary patterns were derived using principal component analysis: plant based, high protein, and high saturated fat and sugar. In the adjusted analysis, every SD increase in the plant-based dietary pattern score was associated with a 0.71-point decrease (β = −0.72; SE = 0.32; P = .027; 95% CI = −1.35 to −0.08) in the SRI score, and every SD increase in the high saturated fat and sugar dietary pattern score was associated with a 0.77-point increase (β = 0.77; SE = 0.32; P = .015; 95% CI = 0.15 to 1.39) in the SRI score. There were no associations between high protein diets and SRI scores. Physicians adhering to diets that are high in plant-based foods and low in saturated fat and added sugars had less SRI. Physicians currently face significant barriers to maintaining a healthy diet. This study highlights the potential role of workplace nutrition on SRI and work performance of physicians.
‘Potential mechanisms for the effect of diet on cognitive performance include regulation of hormones, neurotransmitters, and blood flow as well as reduction of oxidative stress and inflammation.’
Introduction
Fatigue resulting from sleep deprivation, interrupted sleep, and irregular sleep schedules is common among physicians and is associated with impairment in work performance.1-3 Sleep-related impairment (SRI) is defined as “perceptions of alertness, sleepiness, and tiredness during usual waking hours, and the perceived functional impairments during wakefulness associated with sleep problems or impaired alertness.”4-6 Recent studies revealed that SRI and fatigue are associated with burnout and detrimental health effects in physicians.2,7
Previous efforts to address fatigue in physicians have focused almost exclusively on either time allocated to sleep or on limiting work hours.1,2,8 Studies of physicians and nonphysicians suggest that nutritional strategies can mitigate fatigue and improve both cognitive performance and sleep quality.9-12 Potential mechanisms for the effect of diet on cognitive performance include regulation of hormones, neurotransmitters, and blood flow as well as reduction of oxidative stress and inflammation.12,13 The effects of diet on sleep quality have been attributed to the role of dietary factors in regulation of peripheral circadian clocks 14 and to synthesis of hormones and neurotransmitters that are involved in sleep regulation.11,15-29
Despite the apparent beneficial effects of nutrition on sleep quality and cognitive performance, efforts to improve workplace nutrition for physicians have received little attention. Several reports suggest that physicians engage in healthier lifestyle behaviors than the general population30-32 and that physicians believe that healthy eating at work would improve their professional performance.33,34 Nonetheless, only 1 small pilot study has evaluated the effects of a healthy diet on the work performance of physicians. 35 In the present study, we evaluated the associations between dietary patterns as assessed by a Food Frequency Questionnaire (FFQ) and SRI in a cohort of community physicians.
Materials and Methods
Study Design, Setting, and Participants
In this cross-sectional observational study (secondary data analysis), we used deidentified data from community physicians in the San Francisco Bay Area who completed an electronic Wellness Survey in March 2016. Medical specialties included primary care, pediatrics, internal medicine and internal medicine subspecialties, otolaryngology, gynecology and obstetrics, general surgery, and general surgery subspecialties. This study was deemed exempt by the Stanford School of Medicine Institutional Review Board.
Dietary Pattern Assessment
The intake of 13 food items during a typical week was assessed using a semiquantitative FFQ based on the MIND (Mediterranean-DASH Intervention for Neurodegenerative Delay) Diet food groups.36,37 The FFQ was developed by Martha C. Morris, ScD, at Rush University and modified by Andrea Hausel, MPH, RD, at Stanford University for brevity and ease of use in a physician population.
We derived dietary patterns using a principal component analysis of frequency of intake of 13 food items in an average week (ranging from 0 to 7+ per week): green leafy vegetables, other vegetables, nuts, berries, beans, whole grains, fish, poultry, red meats, butter and stick margarine, cheese, pastries and sweets, and fried and fast food. Sampling adequacy and intercorrelation of variables were supported by Kaiser-Meyer-Olkin (KMO) test and Bartlett’s test of sphericity (KMO value = 0.64 and Bartlett’s test of sphericity P < .0001, respectively). 38 Orthogonal transformation (varimax rotation), eigenvalues >1.25 criterion, and absolute factor loadings >0.30 for each food item were used to define dietary patterns. 39 The diet questionnaire also asked 2 additional questions to determine alcohol consumption during a typical week and the predominant type of oil consumed in the diet (olive oil vs other plant-based oils).
Sleep-Related Impairment Assessment
We used the National Institutes of Health (NIH) Patient-Reported Outcomes Measurement Information System (PROMIS) SRI short form (8-item) measure. The 8 questions address alertness, tiredness, and sleepiness in the past 7 days.4,40 The answers are based on a 5-point Likert scale with responses ranging from “Not at all” to “Very much” and the raw scores ranging from 8 to 40. 5 The NIH PROMIS guidelines can be used to identify T-scores that correspond with raw scores for each scale. T-scores of 50 or higher (with a SD of 10) in these instruments indicate higher than average SRI, compared with the general population.4,40 The NIH PROMIS instrument for SRI is a well-validated tool used to assess sleep-wake functioning and fatigue in clinical and research populations with or without sleep disorders.5,6,41,42
Covariates
Analyses were adjusted for covariates associated with sleep quality and cognitive performance determined a priori based on existing evidence. These include the following: age (<50 years, ≥50 years), gender (male, female), hours worked per week, physical activity, type of oil most commonly used in the diet (olive oil vs other types),43-45 and alcohol consumption (yes, no).46-48 Physical activity was measured using a previously validated questionnaire 49 to allow adjustment for adherence to the National Physical Activity Guidelines (≥150 minutes of moderate physical activity or ≥75 minutes of vigorous physical activity per week; yes, no).50,51 To maintain the confidentiality of participants, data on specialty was not included in the analysis. The survey did not assess height, weight, or smoking habits.
Statistical Analysis
All analyses were prespecified and hypothesis driven and performed using previously collected survey data from 245 physicians. No sample size or power calculations were performed. We used the IBM SPSS Statistics for Windows (Version 25.0, Armonk, NY: IBM Corp.) statistical package. All reported P values are 2-tailed, with statistical significance set at P <.05. Sample characteristics are presented as frequencies and percentages for categorical variables and as means and SDs for continuous variables. We used Mann-Whitney tests to compare the food group intakes between men and women. Linear regression models were used to assess the association between dietary pattern scores and SRI. We used multiple regression models to assess the relationship between dietary pattern and SRI scores with and without adjustments for age, gender, physical activity, type of oil commonly consumed, alcohol intake, and work hours. The presence of effect modification was examined by creating cross-product terms of dietary scores and potential modifiers (age, gender, alcohol consumption, physical activity, and type of oil) by entering them one at a time in the model. Missing data were excluded from analysis (<1% of data).
Results
A total of 251 out of 255 (98%) eligible physicians completed the survey. Of the 251 physicians who completed the survey, 245 physicians consented to having their deidentified data used for research or other quality improvement projects. The description of our study sample is presented in Table 1. Female physicians comprised 53.5% (131 of 245 physicians) of the total sample, and 68.7% of female physicians were less than 50 years old (compared to 38.9% of male physicians, P < .0001). Female physicians reported working fewer hours when compared with male physicians (44.3 ± 16.2 vs 53.2 ± 16.1 hours, respectively, P < .0001). Based on the PROMIS guidelines for interpretation of SRI raw scores, 4 the raw score of SRI (16.3) in this study is slightly higher than those in PROMIS reference populations (the 2000 General US Census and a clinical sample; raw score = 16). 4 There was no significant gender difference in SRI scores.
Survey Respondents’ Characteristics.
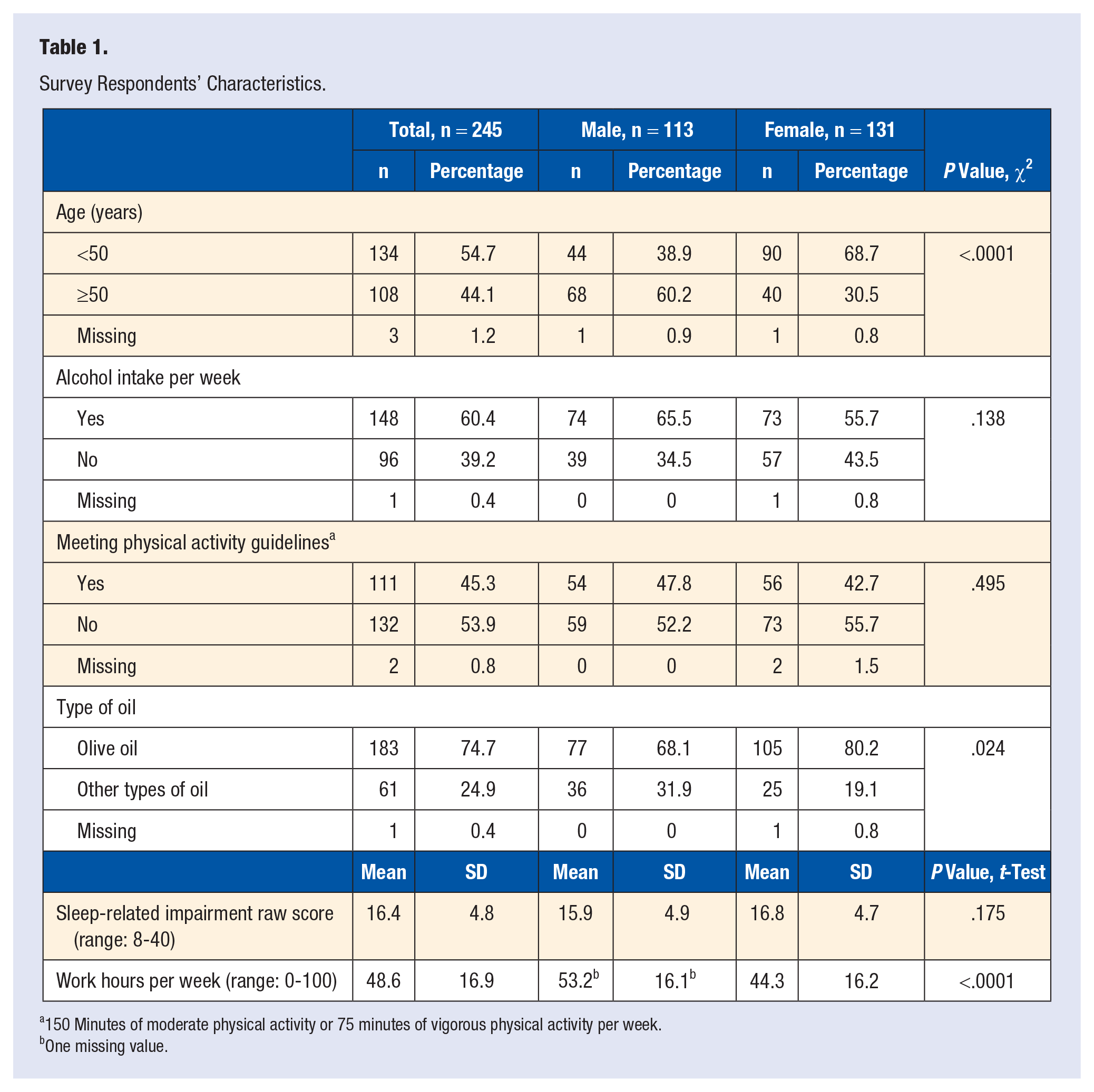
150 Minutes of moderate physical activity or 75 minutes of vigorous physical activity per week.
One missing value.
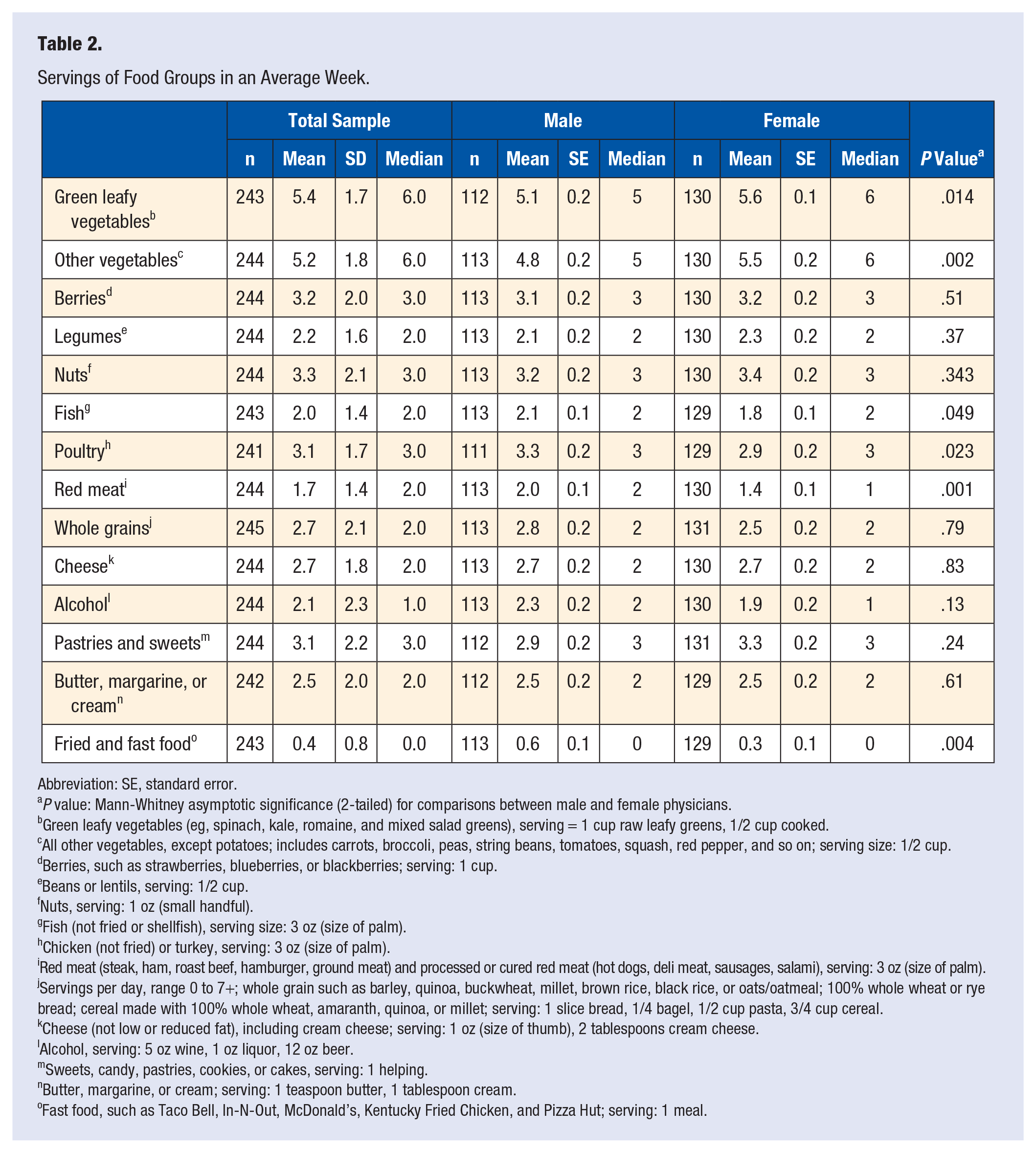
Table 2 represents the servings of food groups consumed in an average week for the total sample as well as for male and female physicians. Compared with male physicians, female physicians on average had significantly higher intake of green leafy vegetables and other vegetables and significantly lower intake of fish, poultry, red meat, and fast and fried foods.
Servings of Food Groups in an Average Week.
Abbreviation: SE, standard error.
P value: Mann-Whitney asymptotic significance (2-tailed) for comparisons between male and female physicians.
Green leafy vegetables (eg, spinach, kale, romaine, and mixed salad greens), serving = 1 cup raw leafy greens, 1/2 cup cooked.
All other vegetables, except potatoes; includes carrots, broccoli, peas, string beans, tomatoes, squash, red pepper, and so on; serving size: 1/2 cup.
Berries, such as strawberries, blueberries, or blackberries; serving: 1 cup.
Beans or lentils, serving: 1/2 cup.
Nuts, serving: 1 oz (small handful).
Fish (not fried or shellfish), serving size: 3 oz (size of palm).
Chicken (not fried) or turkey, serving: 3 oz (size of palm).
Red meat (steak, ham, roast beef, hamburger, ground meat) and processed or cured red meat (hot dogs, deli meat, sausages, salami), serving: 3 oz (size of palm).
Servings per day, range 0 to 7+; whole grain such as barley, quinoa, buckwheat, millet, brown rice, black rice, or oats/oatmeal; 100% whole wheat or rye bread; cereal made with 100% whole wheat, amaranth, quinoa, or millet; serving: 1 slice bread, 1/4 bagel, 1/2 cup pasta, 3/4 cup cereal.
Cheese (not low or reduced fat), including cream cheese; serving: 1 oz (size of thumb), 2 tablespoons cream cheese.
Alcohol, serving: 5 oz wine, 1 oz liquor, 12 oz beer.
Sweets, candy, pastries, cookies, or cakes, serving: 1 helping.
Butter, margarine, or cream; serving: 1 teaspoon butter, 1 tablespoon cream.
Fast food, such as Taco Bell, In-N-Out, McDonald’s, Kentucky Fried Chicken, and Pizza Hut; serving: 1 meal.
Three dietary patterns were identified (Supplemental Table 1A) based on the criteria described in the Methods section. The first pattern, the plant-based dietary pattern, was characterized by a high intake of green leafy vegetables, other vegetables, berries, legumes, and nuts and low intake of fast and fried foods. The second pattern, high protein and low carbohydrate diet, was characterized by high intake of fish, poultry, and red meat and a low intake of grains. The third pattern, high saturated fat and high sugar dietary pattern, was characterized by a high intake of foods high in saturated fat, added sugars, and refined carbohydrates. Each participant received a score for each dietary pattern, with a mean of 0 and a SD of 1. Each dietary pattern score is uncorrelated with the other 2 dietary pattern scores. Higher scores indicate higher intake of foods in that particular dietary pattern.
Table 3 presents the unadjusted regression analysis for the associations between dietary pattern scores and SRI. Every increase of 1 SD in the plant-based dietary pattern score was associated with a statistically significant 0.72-point decrease in the SRI score. Every increase of 1 SD in the high saturated fat and high sugar dietary pattern score was associated with a statistically significant 0.79-point increase in the SRI score. There was no statistically significant association between the high protein diet and low carbohydrate dietary pattern score and SRI.
Unadjusted Associations Between Dietary Pattern Scores and Sleep-Related Impairment (n = 235). a
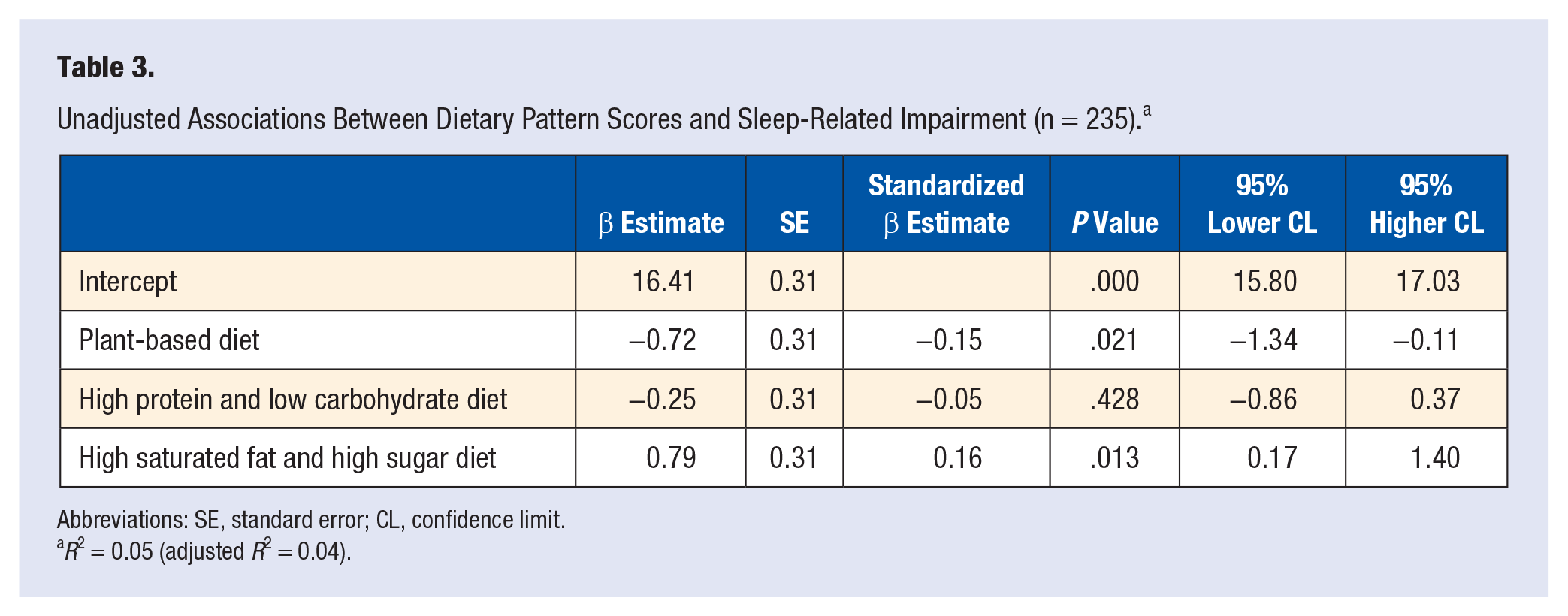
Abbreviations: SE, standard error; CL, confidence limit.
R2 = 0.05 (adjusted R2 = 0.04).
The results of the adjusted multivariate analysis for the associations between dietary pattern scores and SRI are presented in Table 4. After adjusting for other variables known to be related to SRI, every increase of 1 SD in the plant-based dietary pattern score was associated with a statistically significant 0.72-point decrease in the SRI score (β = −0.71; SE = 0.32; P = .027; 95% CI = −1.35 to −0.08; effect size [standardized β] = −0.15). Every increase of 1 SD in the high saturated fat and high sugar dietary pattern score, was associated with a statistically significant 0.77-point increase in the SRI score (β = 0.77; SE = 0.32; P = .015; 95% CI = 0.15 to 1.39; effect size (standardized β) = 0.16). There was no significant association between the high protein diet and SRI. We also found that for every hour increase in hours worked per week, there was a statistically significant 0.04-point increase in SRI score (β = 0.04; SE = 0.02; P = .029; 95% CI = 0.01 to 0.08). Age younger than 50 years old was also associated with higher SRI. There were no associations between gender, meeting physical activity guidelines, alcohol consumption, olive oil consumption, and SRI. There were no significant interaction effects between dietary pattern scores and gender, age, or any of the lifestyle factors.
Adjusted Associations Between Dietary Patterns and Sleep-Related Impairment (n = 229). a
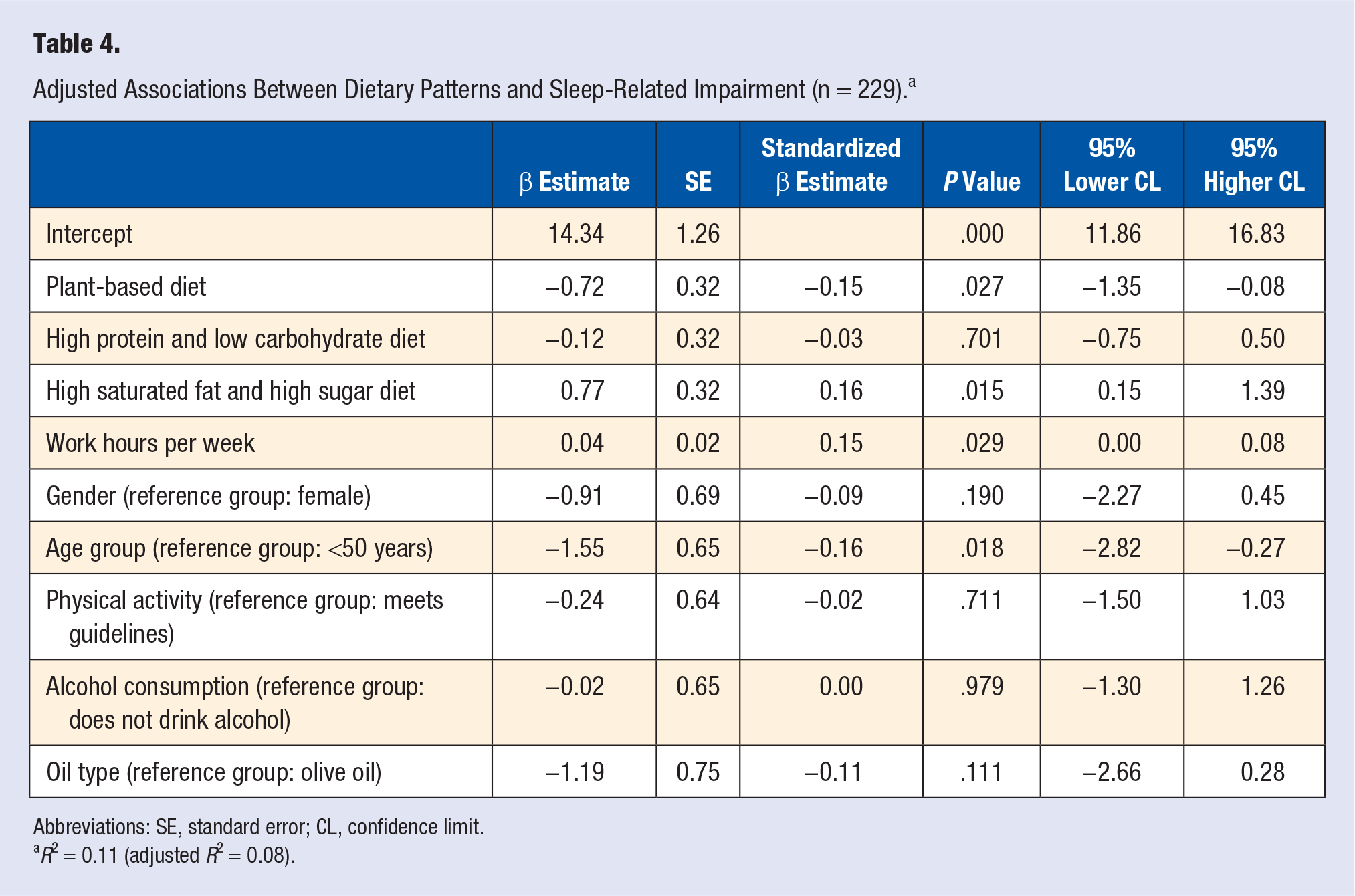
Abbreviations: SE, standard error; CL, confidence limit.
R2 = 0.11 (adjusted R2 = 0.08).
Discussion
The results of our study support the importance of healthy diets to physicians’ work performance, thus suggesting that dietary choices may ultimately affect the quality of patient care. Our results suggest that a plant-based diet is associated with lower SRI in physicians and a diet high in refined carbohydrates, sugar, and saturated fat is associated with higher SRI. Adjusting for work hours, age, gender, and lifestyle factors did not change the strength of the associations between dietary pattern and SRI. These results suggest that dietary interventions may be complementary to other strategies to reduce SRI as well as increase alertness and cognitive performance in physicians.
Because this study is a cross-sectional analysis based on food frequency information collected from a survey, our findings do not provide evidence of a causal relationship or the potential direction of effect. Evidence from studies of nonphysicians suggests that the relationship between sleep and diet is bidirectional. 12 There is strong evidence that sleep deprivation negatively affects dietary choices and behaviors through changes in appetite-regulating hormones and brain activity, resulting in increased energy intake from food and snacks high in added sugars, sodium, fat, and saturated fat.52-58 Although randomized controlled trials of dietary interventions provide the best evidence, there are unique challenges in recruitment and retention of physician research participants for randomized controlled trials of dietary interventions (eg, concern for interrupting patient flow, unpredictable work schedules, heavy work load and lack of time to complete study procedures, lack of time or discomfort with eating in clinical areas or in front of patients 33 ). Nonetheless, the present evidence suggests that there is merit in conducting such studies to evaluate the effects of dietary interventions on physician fatigue. Strengths of the current study include the very high survey response rate and novelty in examining associations between diet and SRI in physicians. In addition, these results add to the limited data on the role of diet in work performance in physicians33,35 and are consistent with studies of nonphysicians suggesting that poor nutritional intake results in irritability and frustration,59-61 feeling fatigued, 62 and reduced motivation 62 and changes risk tolerance and decision making.61,63,64
The results of our study are also in agreement with findings of previous studies in the general population. For example, low intake of total vegetables, green/yellow vegetables, and other vegetables is associated with poor sleep quality, whereas low sugar intake is associated with better sleep quality, as measured by the Pittsburgh Sleep Quality Index. 23 Although we found no association between the high protein diet and SRI, a study in airline pilots has shown that high protein diets result in poorer cognitive performance. 65
In the aviation industry, recognition of factors that can result in human errors—including fatigue, hunger, sleep deprivation, and mental and physical stress—has resulted in considerable improvements in air safety. Whereas some of these concepts, such as preoperative briefings and the use of checklists, have been applied to reducing human error in medicine, proper nutrition and hydration have not been addressed. 66 Reducing the risk of human errors caused by poor nutritional status is an important strategy that can be implemented as an auxiliary effort to other ongoing patient safety strategies. For more than a decade, physicians have been advocating for healthier food options in health care settings to advance the well-being of patients, staff, and all health care professionals.35,67-71 In spite of this, meals provided to physicians and trainees during weekly conferences, grand rounds, or annual scientific meetings are often high in added sugars, refined carbohydrates, and saturated fat.68,72 Although the majority of physicians eat prepared meals provided in health care settings, 72 physicians often have little to no input in the selection of the meals and snacks offered to them. 72 In addition, food vendors at health care organizations often display snacks high in added sugars, refined carbohydrates, and saturated fat (eg, cookies) at the point of purchase. 69 Our findings add to the evidence suggesting that changes in these practices may advance not just the health of physicians and other health care workers, but also the health of the patients for whom they care.
If the associations implied by the regression analysis in this study were to represent causal relationships, adjustment of dietary patterns could render small, but potentially meaningful, improvements in SRI. For example, a 2 SD increase in intake of plant-based foods coupled with a 1 SD decrease in high saturated fat and sugar foods would be associated with a 2.21-point [(0.72 × 2) + 0.77 = 2.21] decrease in SRI (Cohen’s d = [0.15 × 2] + 0.16= 0.46). Although clinically meaningful change estimates have not been established for SRI, published estimates for PROMIS measures are generally in the 2 to 6 points range (of the raw scores). 73 This is consistent with a finding of a recent study that has shown that increases in the raw SRI scores (range 8 to 40) of 2 points or more are associated with increased risk of burnout in physicians. 7 Although this effect size (Cohen’s d = 0.46) is considered small (Cohen’s d = 0.20 is considered a small, 0.50 a medium, and 0.80 a large effect size), it represents both well-rested and sleep-deprived physicians in our sample. The effect size may be larger during times of inadequate sleep, which are sometimes unavoidable in clinical practice. Future studies are needed to assess the effects of dietary interventions on physician SRI and to establish clinically meaningful change estimates for SRI.
Conclusions
Physicians face significant barriers in sustaining a healthy diet while at work as a result of long work hours; heavy work load; lack of or limited access to healthy meals, snacks, and drinks33,70,74; and an overall dearth of organizational policies to support physician nutrition. This study highlights the potential role of workplace nutrition on SRI and the work performance of physicians. The findings provide an evidence foundation for the influence of nutrition on SRI that supports the development and testing of dietary interventions and organizational nutrition policies to reduce fatigue and related performance detriments among physicians.
Supplemental Material
Appendix_Table – Supplemental material for Associations Between Dietary Patterns and Sleep-Related Impairment in a Cohort of Community Physicians: A Cross-sectional Study
Supplemental material, Appendix_Table for Associations Between Dietary Patterns and Sleep-Related Impairment in a Cohort of Community Physicians: A Cross-sectional Study by Maryam S. Makowski, Tait D. Shanafelt, Andrea Hausel, Bryan D. Bohman, Rachel Roberts and Mickey T. Trockel in American Journal of Lifestyle Medicine
Footnotes
Authors’ Note
The preliminary results of this study were presented in an oral presentation at the 2018 International Conference on Physician Health on October 13, 2018, in Toronto, Ontario, Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.