
Abstract
Introduction
Humans are naturally social beings, inherently dependent on other humans for physical, emotional, economical, and social well-being. When people lose or avoid connection with other people to a degree that results in loneliness, the effects can be devastating; so profound, in fact, that nations across the globe have determined loneliness to be a national health problem. Loneliness and social isolation have been identified as a public health crisis in the United States, 1 marked by the 2023 release of a U.S. Surgeon General’s Advisory on the epidemic of loneliness and isolation, which describes in detail the threat and profound implications of loneliness for public and societal health. 2 In recent years a “Minister for Loneliness” has worked alongside the United Kingdom government to address the issue 3 and in Australia, the national Ending Loneliness Together organization was formed to reduce the effects of loneliness and social isolation. 4 In Canada, where loneliness has been identified as an epidemic, 5 non-profits such as the Canadian Institute for Social Prescribing and the Canadian Coalition for Seniors’ Mental Health provide support, research, and guidelines for addressing social and structural factors such as loneliness and community connection.6,7 In addition, the World Health Organization has also established the Commission on Social Connection to address loneliness as an urgent public health threat. 8
Background
Loneliness, a subjective measure identified as the experience of not having one’s social needs met or experiencing connection to others to a lesser degree than desired, has increased in recent years.9,10 Even prior to lockdowns necessitated by the COVID-19 pandemic, which exacerbated feelings of isolation for many, loneliness was a serious threat to the health and well-being of people worldwide. 11 In recent years, loneliness persists as a key social determinant of health, affecting 1 in 3 U.S. adults who feel lonely at least once a week 12 and 1 in 5 who feel lonely every day. 13 Loneliness has been shown to affect between 37% and 43% of senior adults in the U.S.14,15
Risk Factors for Loneliness
Evidence identifying risk factors for loneliness is mixed. 16 For example, some studies show adults with higher levels of education are at greater risk of loneliness, while others find lower levels of formal education increase risk for loneliness. 16 Studies show loneliness rates are higher among older adults, yet other research indicates younger adults experience loneliness at higher rates.16-18 Survey data show that similar percentages of men and women experience loneliness (57% and 59% respectively). 19 Existing literature shows that loneliness is greater among individuals who live alone or in a residential care/nursing home, 16 which in the U.S. is 28% of older adults. 20 Loneliness is also more frequent among those who are divorced or widowed, or have physical and mental health problems.16,21 Adults with low income are more likely to experience loneliness,21-23 as well as individuals who identify as LGBTQ. 23 Recent evidence shows among older adults (ages 50-80), loneliness is most commonly reported among those who are not working. 21 Older adults may be more at risk of loneliness due to life events like retirement, having a chronic illness or disability, experiencing sensory deprivation like hearing loss, or experiencing bereavement. 15
Physicians are listed among the nation’s loneliest professionals. 24 Loneliness is common among family medicine physicians, 25 and is a major stressor for nurses and physicians. 26 For health care professionals, loneliness may in part be driven by the increase in technology, telehealth, and virtual visits27,28 resulting in fewer hours spent in the company of colleagues and patients.
Effects of Loneliness
Loneliness is associated with serious problems including illness,2,23 increased risk of stroke,2,29 depression,23,30 anxiety, 23 and suicidal ideation. 31 The mortality effects of social disconnection have been compared to the effects of smoking 15 cigarettes per day. 2 Other data show persistent loneliness increases risk for all-cause dementia, Alzheimer’s disease, vascular dementia, and cognitive impairment.2,32
Professionally, loneliness has been associated with poor occupational functioning and well-being among workers 33 and burnout, 25 which among health care professionals can lead to reduction in clinical effort or departure from practice. 34 High levels of loneliness are also associated with lower levels of meaning in life and purpose. 35 Loneliness may also have economic costs. In the U.S., workers experiencing loneliness may be less productive, costing an organization nearly $406 billion a year. 17 In addition, annual Medicare costs associated with care provided to socially isolated beneficiaries are increased by $6.7 billion. 36
Study Aims
Despite the abundance of literature on loneliness, including that focused on older adults and health care workers, there is little to no evidence of the prevalence of loneliness among older physicians in the U.S. This study aims to fill this gap by investigating the proportion of physicians aged
Considering its relationships with burnout, health issues, and suicidal ideation, loneliness has serious implications for the physician workforce, clinician well-being, and patient care access. Understanding how prevalent the phenomenon is among senior physicians, and its relationships with risk factors, will help health care organizations, policymakers, and public health entities establish effective policies and practices to help protect and support this population. For physicians who have retired from practice or left clinical medicine, these findings may identify methods to help maintain connections and lifestyle options that can prevent loneliness and sustain well-being.
Methods
Study Design and Sample
This cross-sectional survey was conducted between February 26 and March 12, 2024. The sample was generated from the American Medical Association Physician Professional Data (AMA PPD), independent of AMA membership status. Email invitations with a link to the online survey were sent to 168,296 physicians aged 65 or older at the time of the survey. After 14,634 emails were returned undeliverable, email invitations were delivered to 153,662 physicians.
This study was reviewed by the University of Illinois Chicago Institutional Review Board and determined to be exempt from human subjects research review (Study ID 2023-1538). All participants provided consent to participate after reviewing an information sheet and before initiating the survey. Investigators followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines in the presentation of this study.
Survey Instrument
The survey was developed by an interdisciplinary team including research staff and physicians. Survey items included demographic questions to collect information about gender identity, age, race, sexual orientation, practice status, geographical area, relationship status, and household status. Personal questions about social and health factors were also included. The survey included the 20-item UCLA Loneliness Scale 37 (used with permission from the creator of the survey, Dr Daniel Russell), a widely used survey instrument considered the “gold standard” for measuring loneliness. 38 The full survey can be found in the Supplemental Materials.
Survey Procedure
After clicking to provide consent, participants completed the self-administered survey using an online survey platform. There was no incentive for participation. Only complete responses were considered valid following a data cleaning process.
Statistical Analysis
Demographic, social, and personal characteristics were summarized using standard descriptive statistics. Loneliness scores were calculated by summing the scores of all 20 items in the UCLA Loneliness Scale, with possible scores ranging from 20 to 80. Bivariate analysis with two-sided significance testing was completed to calculate the mean loneliness scores across various sub-segments of the sample. In accordance with methods documented and recommended by the author of the UCLA Loneliness Scale, scores between 1 and 2 standard deviations (SD) from the mean were considered “moderately high” loneliness, and scores
Results
Participant Demographics and Characteristics.
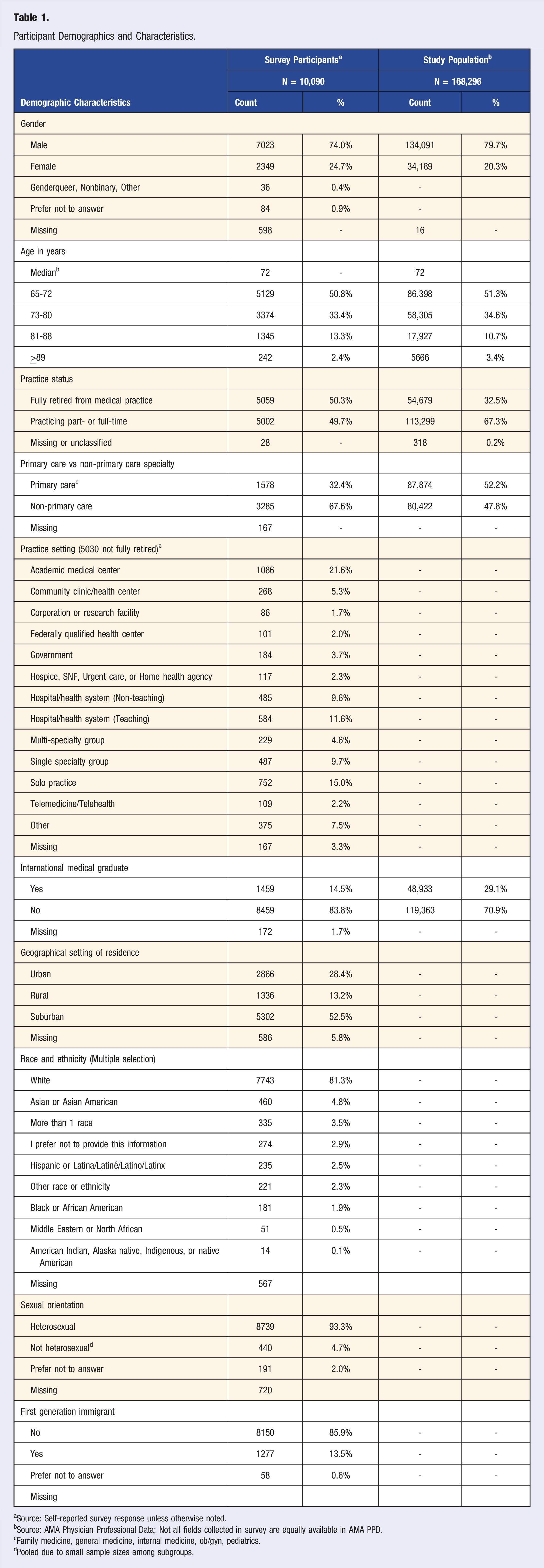
aSource: Self-reported survey response unless otherwise noted.
bSource: AMA Physician Professional Data; Not all fields collected in survey are equally available in AMA PPD.
cFamily medicine, general medicine, internal medicine, ob/gyn, pediatrics.
dPooled due to small sample sizes among subgroups.
Mean Loneliness Scores
Of the 10,090 respondents, 9098 completed all 20 items of the UCLA Loneliness Scale. The mean loneliness score was 38.04. Respondents with high loneliness scores comprised 18% of the sample (Figure 1). The majority of participants (68.9%) scored within the middle range, indicating most experienced neither moderately high nor very high loneliness. Percentage of respondents with moderately high or very high loneliness.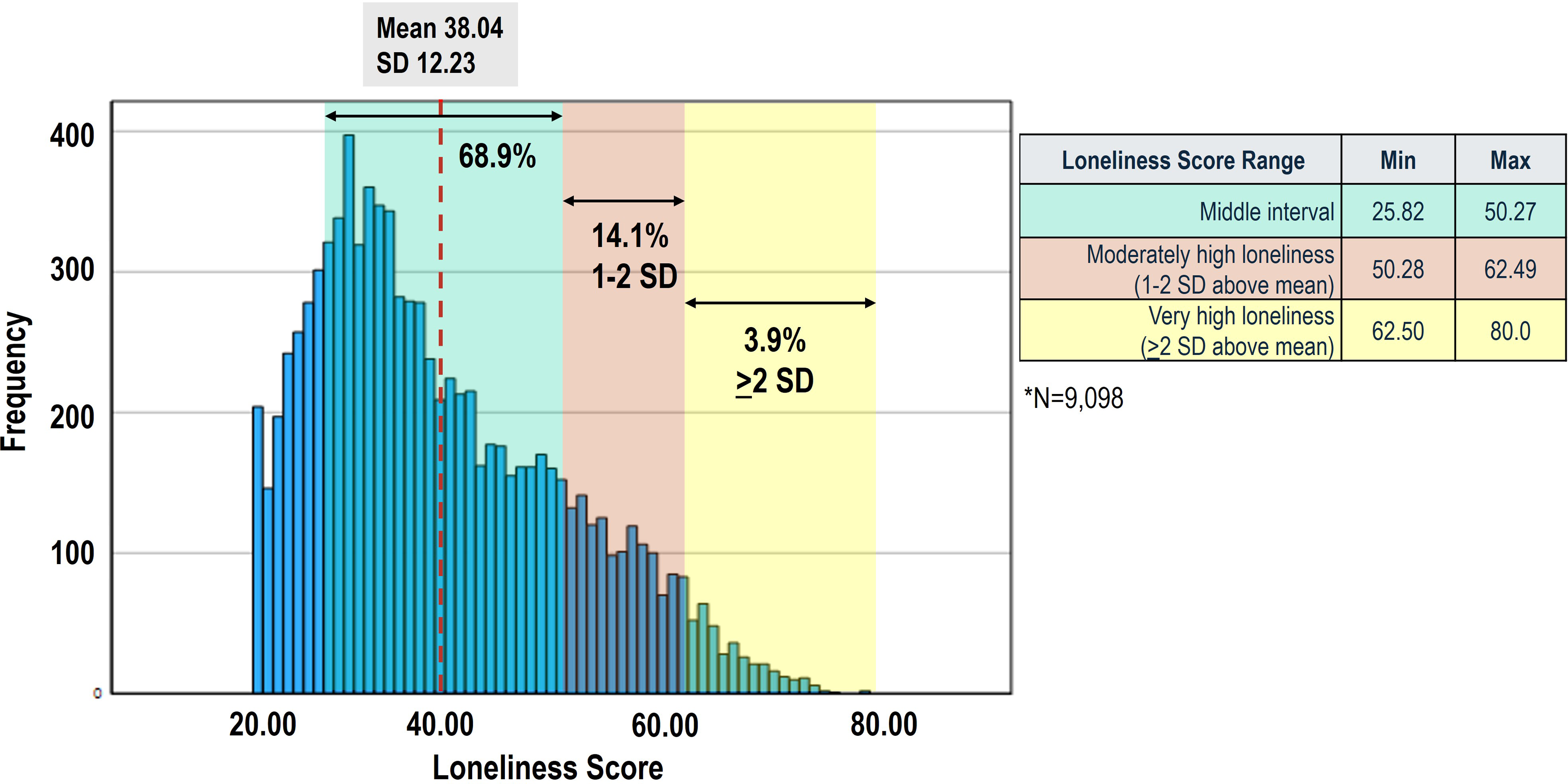
Mean Loneliness Scores.
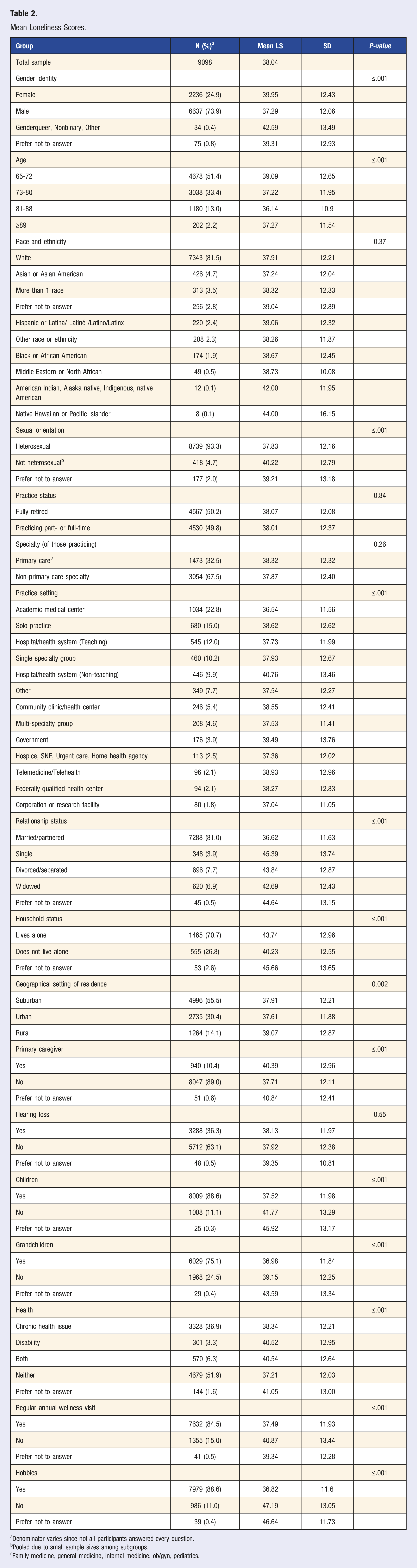
aDenominator varies since not all participants answered every question.
bPooled due to small sample sizes among subgroups.
cFamily medicine, general medicine, internal medicine, ob/gyn, pediatrics.
Senior physicians who were not married or partnered have significantly higher loneliness scores (mean scores 43.84 (divorced/separated), 45.39 (single), 42.69 (widowed)) than married/ partnered senior physicians (mean score 36.62, P
Senior physicians who are the primary caregiver of another adult had higher loneliness scores than those who are not (mean score 40.39 vs 37.71, P
Responses from the participants with high loneliness scores (
Multivariable Logistic Regression
Multivariable Logistic Regression Analysis of Association Between Loneliness Score and Personal, Health, and Social Characteristics.
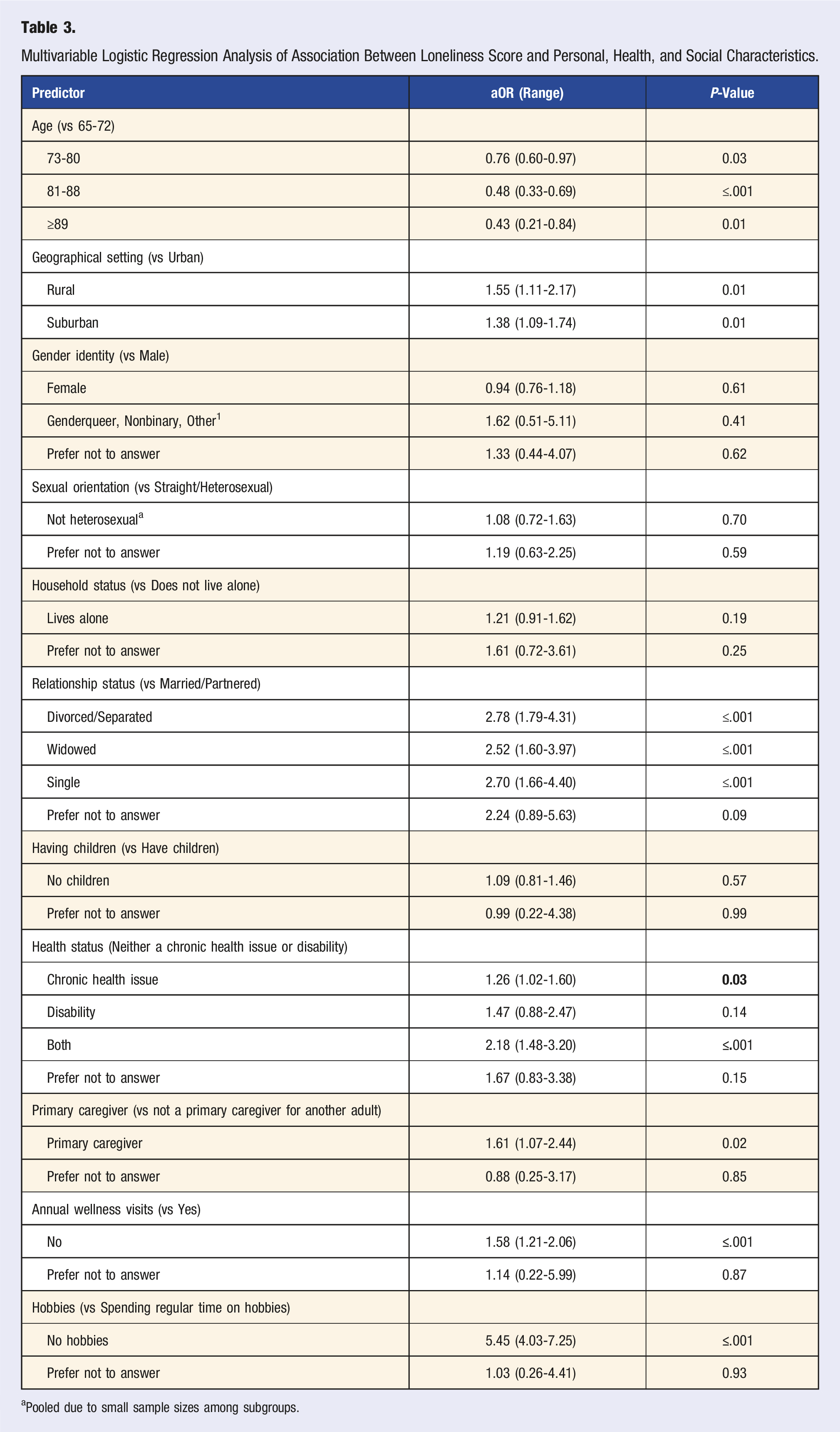
aPooled due to small sample sizes among subgroups.
Living in a rural region (OR 1.55 [95% CI, 1.11-2.17]), being divorced or separated (OR 2.78 [95% CI, 1.79-4.31]), widowed (OR 2.52 [95% CI, 1.60-3.97]), or single (OR 2.70 [95% CI, 1.66-4.40]) were all associated with high loneliness. Senior physicians with a chronic health condition (OR 1.26 [95% CI, 1.02-1.60]) or both a chronic health condition and a disability (OR 2.18 [95% CI, 1.48-3.20]) had higher odds of high loneliness than those without either of these. Not having an annual wellness visit was associated with high loneliness (OR 1.58 [95% CI, 1.21-2.06]) and not regularly spending time on hobbies or interests was associated with higher odds of experiencing high loneliness (OR 5.45 [95% CI, 4.03-7.25]).
Discussion
Nearly 1 in 5 senior physicians experiences high loneliness and several subgroups show higher propensity for high loneliness than others. Several important risk factors for high loneliness were identified. Among the at-risk groups are those who live in rural areas, are divorced, widowed, or single, suffer from disability and chronic illness, do not have an annual wellness visit, and do not have outside hobbies or interests. Our findings suggest that attention should be given to providing these groups with tailored support systems and greater opportunities for meaningful interpersonal interactions and community involvement. This may be especially important for those physicians who are part of additionally marginalized communities, such as individuals who are not male, not heterosexual, or have a chronic illness or disability.
Although there were no significant differences in mean scores among retired physicians and physicians practicing full- or part-time, it is notable that nearly half of participants still practiced medicine at the time of the survey, and that more than half of the high-loneliness cohort still practiced medicine. Considering this, it is evident that loneliness is not just a “retired physician” concern. Lack of meaningful connection with colleagues and patients, possibly a byproduct of the transactional relationships associated with the production-driven environment of U.S. health care, can lead to loneliness even for people regularly surrounded by people. This could also be a signal that the support systems in place, if any, are not sufficiently providing opportunities for physicians to establish and maintain strong connections.
Physicians of all ages may be at risk for loneliness, so it is important for stakeholders to ensure their programs and policies are created with this in mind. Here we make recommendations for actions that various stakeholders can take to reduce experiences of loneliness and improve well-being for senior physicians.
Organizations that employ physicians can establish employee resource groups which provide opportunities for physicians to meet others who may be facing similar situations or life events. This may be especially beneficial for senior physicians who are not male, do not identify as heterosexual, are recently widowed or divorced, or are a primary caregiver for another adult. Organizations can design team structures and physical spaces to enable opportunities for interactions with others. Scheduling longer visits so physicians have adequate time with patients could be advantageous for all. Sponsoring social or physical activities for physicians may contribute to feelings of collegiality and inclusion. Investing in conference attendance or organized medicine involvement, and providing coverage for the time away from work, can allow physicians to connect with colleagues and engage in meaningful interactions across the profession.
Policymakers also have opportunities to help reduce loneliness for physicians and the general population. Investing in infrastructure designed for humans, rather than cars and buildings, could improve walkability and invite more community facilities and green spaces, helping to foster connections. 40 Similarly, improving public safety would help seniors feel more comfortable walking around in public areas and socializing within their communities. Federal and state governments can issue guidelines for social connection and provide health care workers with guidance on how to screen for loneliness among patients. State and local governments can invest in intergenerational programs, which have been shown to strengthen social determinants of active aging among seniors and promote positive physical and mental health.41,42 Finally, policymakers can invest in further research to better understand loneliness, its risk factors and contributors, and its long-term effects on population health.
For individuals experiencing loneliness or trying to prevent it, seeking opportunities within the community, such as athletic or social clubs with group programming, to engage in non-work-related activities is a way to build connections and prevent isolation. Regular exercise, in natural settings when possible, can boost mental health and help combat loneliness and depression.43-45 Regular visits to a primary care physician for an annual wellness visit can ensure senior physicians manage their conditions, prevent new health issues, and maintain open communication with their health care team about potential psychosocial risks.
Conclusion
In this cross-sectional study, high loneliness was reported by 1 in 5 senior physicians. Certain cohorts have greater odds of high loneliness, including those who are 65-72, live in rural areas, don’t have annual wellness visits, don’t engage in hobbies or interests outside of work, and those with a chronic illness and disability. Institutional and community investment in programs and policies that support senior physicians in these groups may increase opportunities for social connectivity and help reduce risk for loneliness. Individual awareness and self-care can also ensure senior physicians can maintain healthy, balanced lifestyles that promote social connection and well-being. Further research is needed to observe potential causes of loneliness among senior physicians and potential associations with sense of purpose or loss of meaning-making activities. Additional study could also explore associations with financial security, depression, suicidal ideation, efficacy of interventions and programming for preventing loneliness, and to compare loneliness among physicians to the general public.
Reflecting on the sentiments expressed in the Surgeon General’s Report, 2 and considering the far-reaching consequences of loneliness, it is clear that there is a need—perhaps an obligation—to invest in addressing loneliness as the nation has invested in other critical public health issues. Given the implications for the physician workforce, access to care, and other significant human and economic costs, it is imperative to recognize and address loneliness as part of broader physician and population well-being initiatives.
Limitations
Our study is subject to limitations. The self-reported nature of the survey and the sensitivity of the issues being addressed can lead to bias in the responses. The cross-sectional design of the study allows us to observe correlations and not causation. The study population is not representative of all physicians in the U.S. so our results cannot be extrapolated to the national physician population. This study did not include a survey of the general population so direct comparisons are not advised.
Supplemental Material
Supplemental Material - Loneliness and Associated Factors Among Senior Physicians in the U.S.
Supplemental Material for Loneliness and Associated Factors Among Senior Physicians in the U.S. by Lindsey E. Carlasare, Samuel Lin, Purva Shah and Ved Gossain in American Journal of Lifestyle Medicine.
Footnotes
Acknowledgments
The authors would like to acknowledge and thank Alicia Johnson for her contributions to the data analysis and Alice Reed for her contributions to the conceptualization of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.