
Abstract
The aim of the present study is to investigate the association between 20-year trajectories of physical activity status and cardiovascular disease (CVD) incidence, among Acute Coronary Syndrome (ACS) patients. GREECS study is a multi-centered prospective study. Almost all (n = 2172; mean age 62 ± 11 years; 1649 (76%) males) consecutive patients who were hospitalized in the cardiology clinics or the emergency cardiology departments were entered in the study. Four physical activity trajectories were formed regarding the 20-year tracking (from 2004 to 2024), of their physical activity levels (i.e., always inactive or active, turned from inactive/active). Of the 1913 ACS patients who participated in the 20-year follow-up, 51% were consistently inactive, 31% changed from physically active to inactive, 11% from inactive to active, and 7% were consistently active. During the 20-year follow-up 67% of ACS patients experienced a new CVD event. Consistently active patients had 45% lower risk for a recurrent CVD event during the 20-year follow-up period (95% CI, 12% to 64%), as compared to consistently inactive. Sustained engagement in physical activity is associated with a reduced risk of recurrent CVD events among ACS patients. These findings underscore the importance of promoting and sustaining physical activity as a key component of tertiary CVD prevention.
Keywords
“A key finding of our study was that only a trivial portion of ACS patients (7%) maintained a consistently active lifestyle over the 20-year follow-up period.”
Introduction
The public health burden of cardiovascular disease (CVD) remains substantial and is projected to persist at similar levels worldwide in the coming years.1,2 Acute Coronary Syndromes (ACS), encompassing conditions such as unstable angina and myocardial infarction, are major contributors to the global CVD burden due to their high morbidity, mortality, and associated health care costs.3,4 A series of observational studies, clinical trials and meta-analyses have demonstrated that lifestyle factors play a crucial role in the primary and tertiary prevention of CVD by reducing the risk of recurrent events and improving overall cardiovascular health. Adopting a heart-healthy diet, engaging in regular physical activity, maintaining a healthy weight, and managing stress can significantly lower blood pressure, cholesterol levels, and inflammation. Additionally, smoking cessation and moderating alcohol intake further enhance long-term outcomes, complementing pharmacological treatments to prevent disease progression.5-8
Among lifestyle factors, physical activity is a pivotal determinant in ACS prevention, with numerous studies demonstrating the protective effects of moderate to high levels of physical activity during both occupational and leisure activities in apparently healthy populations.5-7 Additionally, in the context of secondary ACS prevention, physical activity plays a vital role in improving disease outcomes, as patients who engage in higher levels of physical activity tend to exhibit better clinical profiles and longer life expectancy. 8 The biological pathways through which physical activity exerts its beneficial cardioprotective effects in primary prevention have long been suggested in the literature, through multiple interrelated mechanisms that improve cardiovascular health, for example, endothelial function improvement, lipid profile modulation, anti-inflammatory effects, reducing insulin resistance, blood pressure reduction, body weight management.9-11 However, while numerous studies have highlighted the benefits of physical activity in primary and short-term tertiary prevention contexts, there remains a significant gap in understanding how sustained or changing physical activity patterns over time influence long-term outcomes in ACS patients. Addressing this gap is crucial, as it could provide valuable insights into optimizing rehabilitation strategies, improving patient prognoses, and guiding tailored public health interventions for long-term cardiovascular health. Thus, under the context of the large-scale, multi-centered Greek Acute Coronary Syndromes Study (GREECS), the aim of the present study is to investigate the association between 20-year trajectories of physical activity status and CVD incidence, among ACS patients. The research hypothesis posits that sustained engagement in long-term physical activity could potentially reduce CVD risk, compared to sporadic engagement or complete cessation.
Methods
Study Design
The GREECS study is a multi-centered prospective observational study that was launched in 2003. The aims of the study were to evaluate the annual incidence of ACS, as well as the association of clinical, lifestyle and socio-demographic characteristics of ACS patients with the 30-day, 1-year, 10- and 20-year incidence of ACS, in Greece.
Setting
Between October 2003 and September 2004, the vast majority of (i.e., participation rate, 97%) consecutive patients that were hospitalized in the cardiology clinics or the emergency cardiology departments of 6 General Hospitals and had a discharge diagnosis of ACS, that is, acute myocardial infarction (AMI), with or without ST-segment elevation, or unstable angina (UA), were entered in the study. The participating institutions were the Hippokration hospital in Athens and the general prefectural hospitals in Lamia, Karditsa, Chalkida, Kalamata cities and Zakynthos Island Those hospitals were selected for the better representativeness of populations with diverse socio-economic, cultural, and regional characteristics. All hospitals but the Hippokration serve the entire reference population of their respective regions, encompassing both urban and rural areas.
Bioethics
The study was approved by the Medical Advisory Committees of the participating hospitals, and the Bioethics Committee of the Harokopio University (54/03.04.2024). The study was carried out in accordance with the Declaration of Helsinki (1989) of the World Medical Association. All patients were thoroughly briefed about the aims and procedures of the study and signed an informed consent before participating.
Sample at Baseline
In total, 2172 ACS patients were recruited in the study during the enrollment period; 1649 (76%) of participants were males, whereas the mean age of the total sample was 62 ± 11 years (P for age and gender differences <.001).
Diagnosis of ACS
AMI was defined by typical rise and gradual fall or more rapid rise and fall of biomarkers of myocardial necrosis (i.e., troponin, CK-MB) with at least one of the following: (a) ischemic symptoms, (b) development of pathologic ST waves on the electrocardiogram (ECG), (c) ECG changes indicative of ischemia (ST segment elevation or depression), or, (d) coronary artery intervention (e.g., coronary angioplasty). UA was defined by the occurrence of one or more angina episodes, at rest, within the preceding 48 hours, corresponding to class III of the Braunwald classification. 12 Moreover, a 12-lead ECG was performed, and biochemical markers suggesting cardiac injury and presence of AMI (i.e., troponin I, creatine kinase (CK) and the MB fraction of total CK (CK-MB)) were measured using standard procedures.
Measurements
Physical Activity Status Assessment
Physical activity status was evaluated using the translated and validated short version of the “International Physical Activity Questionnaire” (IPAQ).13,14 IPAQ is a tool of weekly energy expenditure that incorporates frequency (i.e., times per week, for at least 30 minutes/time, as the minimum period required to achieve health benefit), duration (in minutes per time) and intensity of engagement in sports or other physical activities. The question concerning the time spent in sedentary activities was not included as part of any summary score of physical activity. Patients were classified as (a) inactive, (b) minimally active and (c) health-enhancing physical activity (HEPA), using the number of days and duration in minutes engaged in moderate and vigorous physical activities, according to the guidelines of IPAQ scoring. 13 Moreover, four physical activity trajectories were formed regarding the 20-year tracking (from 2004 to 2024), of their physical activity levels. Specifically, participants were classified as (a) consistently inactive if reported sedentary or engagement in light physical activity in all follow-up examinations, (b) became inactive from physically active if reported sedentary or engagement in light physical activity in the follow-up examinations held in 2014 or 2024, (c) became active from physically inactive if reported engagement in physical activities in all follow-up examinations held, and (d) consistently active during the entire follow-up period.
Socio-demographic, Behavioral and Clinical Assessment
In addition, socio-demographic, lifestyle, clinical, and biochemical characteristics were evaluated once the patients were stabilized and capable of actively participating in the interview. Specifically, socio-demographic and lifestyle characteristics included age, sex, education status (in years of school), dietary habits (evaluated through a semi-quantitative Food Frequency Questionnaire which included foods and beverages commonly consumed in Greece), and smoking frequency (in cigarettes per day) and duration (in years). Changes in smoking habits during the 2004-2014 period were recorded in 4 categories, that is, never smoked, quitters, started smoking, and consistently smokers. The level of adherence to the Mediterranean dietary pattern was assessed using the MedDietScore (range 0-55; higher values indicate greater adherence to the Mediterranean diet). 15 Using as threshold the median MedDietScore (i.e., 27 units) patients were categorized into 4 groups (always close, always away, and from close to away and vice-versa) according to their adherence to the Mediterranean dietary pattern through the 2004-2014 period. Anthropometric characteristics included the assessment of weight (in Kg), height (in m), waist and hip circumferences (in cm), using standard procedures, and the calculation of Body Mass Index (BMI) as weight divided by height (in m)-squared. Changes in body weight status during the follow-up period 2004-2014 were also recorded. Medical history included, diagnosis and treatment of hypertension, hypercholesterolemia, type II diabetes mellitus, as well as a previous CVD event and hospitalizations. The assessment was performed by a collaborating physician.
Follow-Up Examinations
The 10-year follow-up examination was performed during the years 2013-2014 and the 20-year in 2024, both through in-person interviews by the study’s investigators. The interviews aimed to retrieve current information about patients’ current medical status, socio-demographic and lifestyle characteristics. Specifically, in 2013-2014, 1918 of the initially enrolled patients (n = 2172) were found and agreed to participate in the 10-year follow-up examination or provided mortality information (88% participation rate). In 2024, a total of 1913 of the 2172 patients either took part in the 20-year follow-up examination or provided mortality data (88% participation rate). Patients lost during the follow-up period (due to changes in contact information or denied being re-examined) were classified as censored, as their loss occurred after the first year of follow-up. For patients who died during the follow-up period, information was obtained from their relatives or other contacts designated by the patients during the baseline examination. No differences were found in baseline clinical and lifestyle factors, between those who participated in the follow-up examinations and their counterparts (all P-values > 0.50). (see flow-chart in Figure 1). Flow chart of the study’s sample during the 2004-2024 observation period.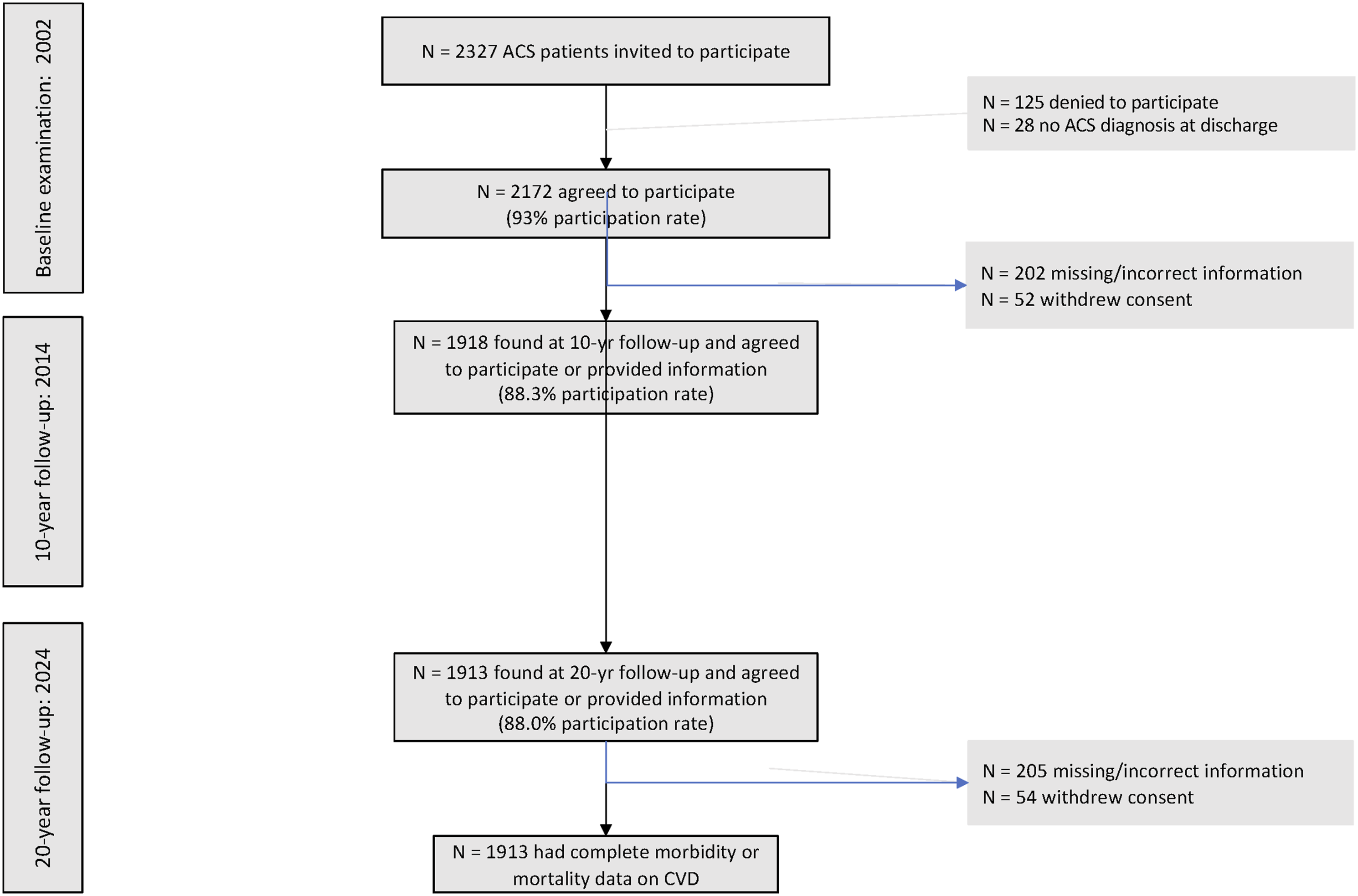
The endpoint studied in the follow-up was recurrent fatal or non-fatal ACS events, such as new AMI, angina pectoris, other identified forms of ischemia—WHO-ICD-10 outcomes coding 410-414.9, 427.2, 427.6-, heart failure and chronic arrhythmias—WHO-ICD-10 coding 400.0-404.9, 427.0 -427.5, 427.9, as well as potential cardiac interventions, for instance percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), both at entry and during follow-up. Further details about the methods and measurements of the GREECS study may be found in previously published work.16,17
Statistical Analysis
Continuous variables are presented as mean values (standard deviation), and categorical variables are presented as percentages. Normality of continuous variables was assessed through the P-P plot and equality of variances through the Levene’s test. Associations between normally distributed continuous variables and groups of the patients were evaluated through the t test for independent samples. Associations for not-normally distributed variables were evaluated using the Mann-Whitney U test. Associations between categorical variables were estimated using the Pearson’s chi-squared test. The association between physical activity status at baseline, during the 10-year after enrollment and 20-year ACS fatal or non-fatal incidence was evaluated by the Cox proportional hazard analysis, after adjustments for socio-demographic, lifestyle and clinical characteristics. The tested hypothesis was further evaluated after dividing patients into two categories; those with CVD history at baseline examination and those without. Model’s goodness-of-fit was determined using deviance and Pearson’s residuals. Results are presented as hazard ratio (HR) and 95% confidence intervals (95% CI). The enrolled sample was adequate to achieve statistical power >85% to test two-sided hypotheses of HR equal to 1.10, with the significance level set at 5%. All statistical calculations were performed using the Stata version 17 software (STATA Inc, College Station, TX, USA).
Results
Participants’ Characteristics According to Trajectories of Physical Activity Status
Characteristics of the ACS Patients Who Participated in 20-Year Follow-up, Stratified According to Their Physical Activity Trajectory 2004-2014; GREECS Study (2004-2024).
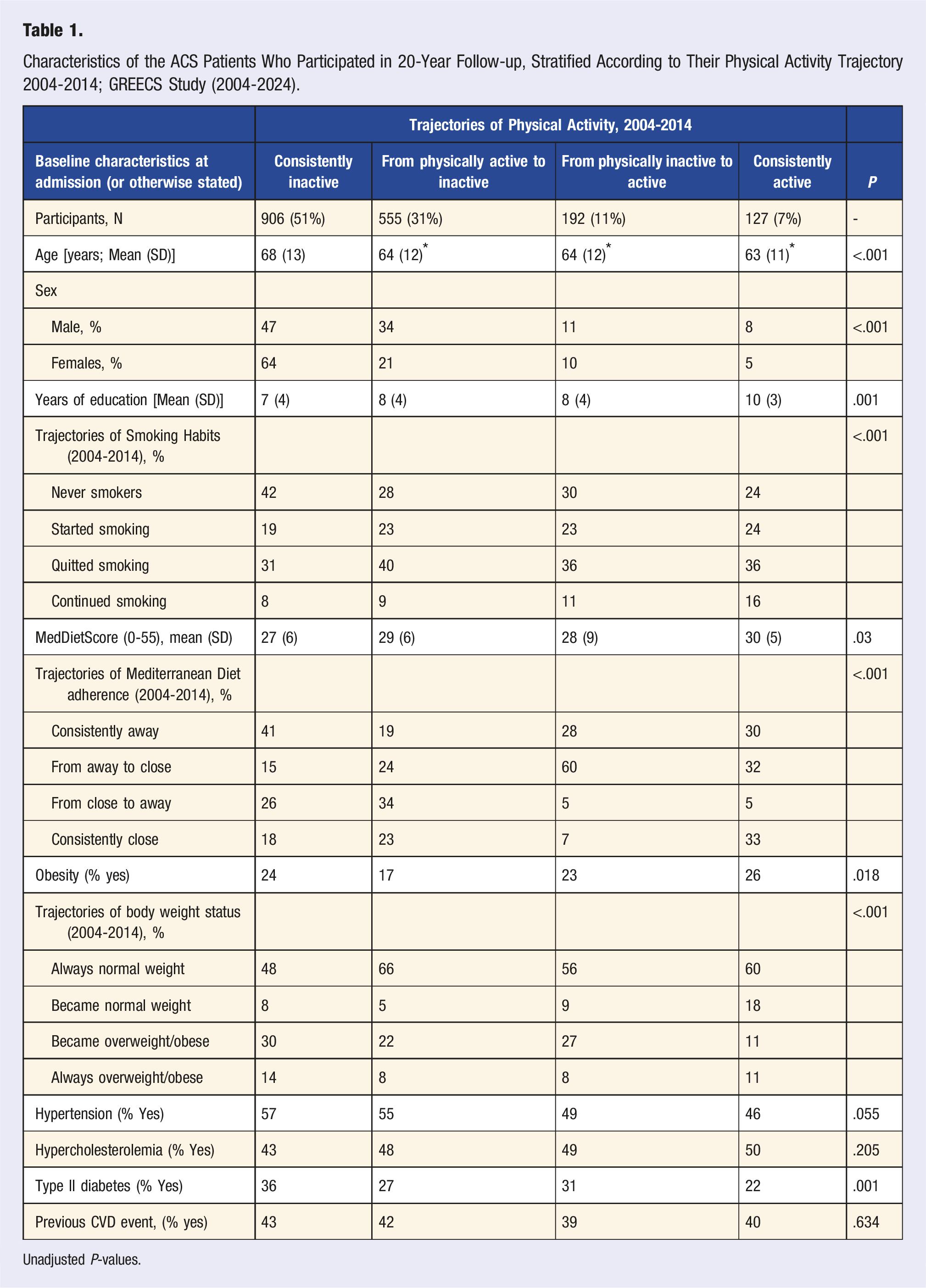
Unadjusted P-values.
Participants’ Characteristics According to Their Combined Recurrent CVD Outcome during the 20-Year Follow-up
Characteristics of the ACS Patients According to Their Combined (Fatal or Non-fatal) Recurrent CVD Outcome During 20-Year Follow-up; GREECS Study (2004-2024) (n = 1913).
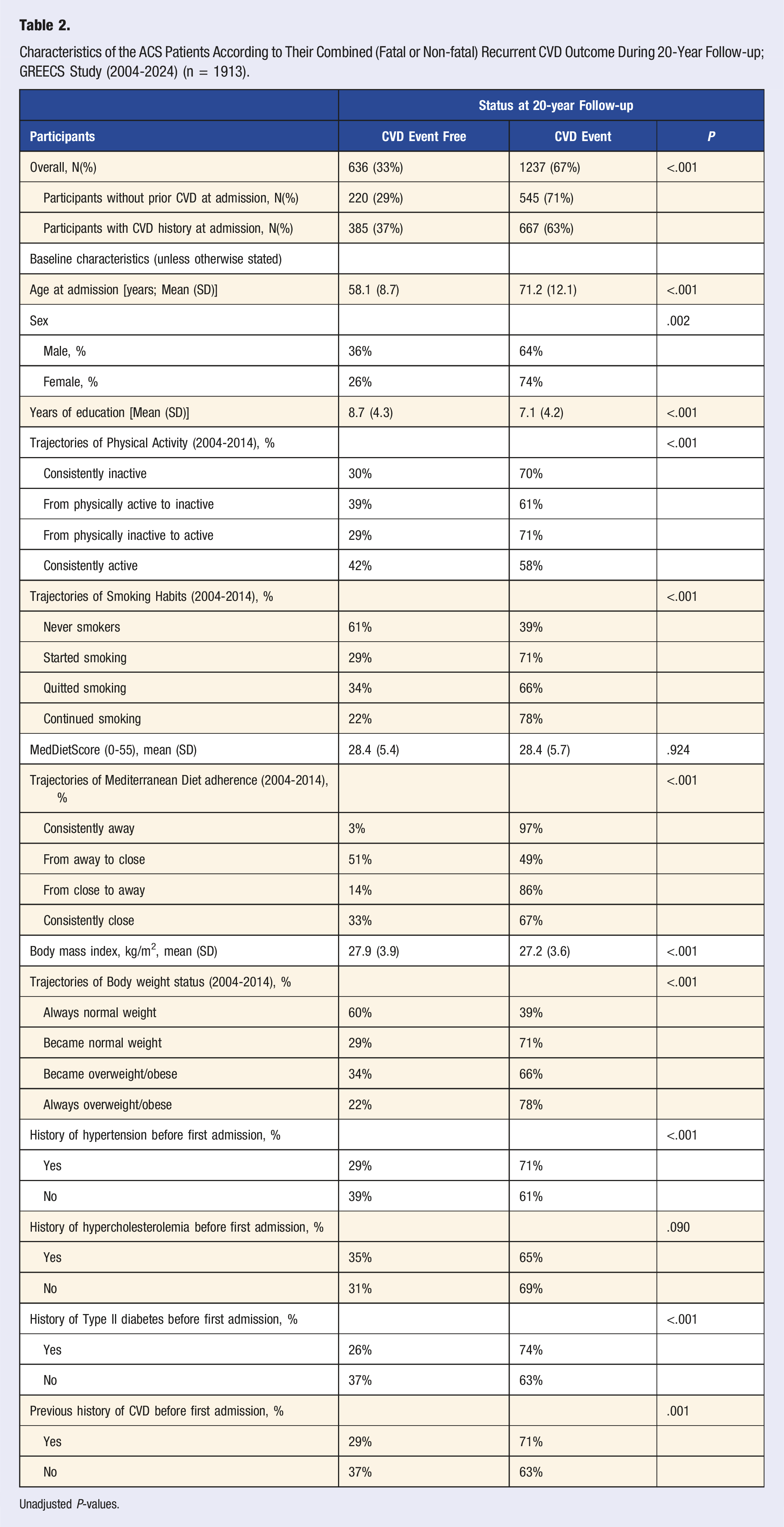
Unadjusted P-values.
Evaluation of Various Characteristics of ACS Patients in Relation to the Development of Fatal or Non-fatal CVD
Results From Nested Cox Proportional Hazards Models That Evaluated Various Characteristics of ACS Patients in Relation to the Development of Fatal or Non-fatal CVD, During the 20-Year Follow-up; the GREECS Study (2004-2024).
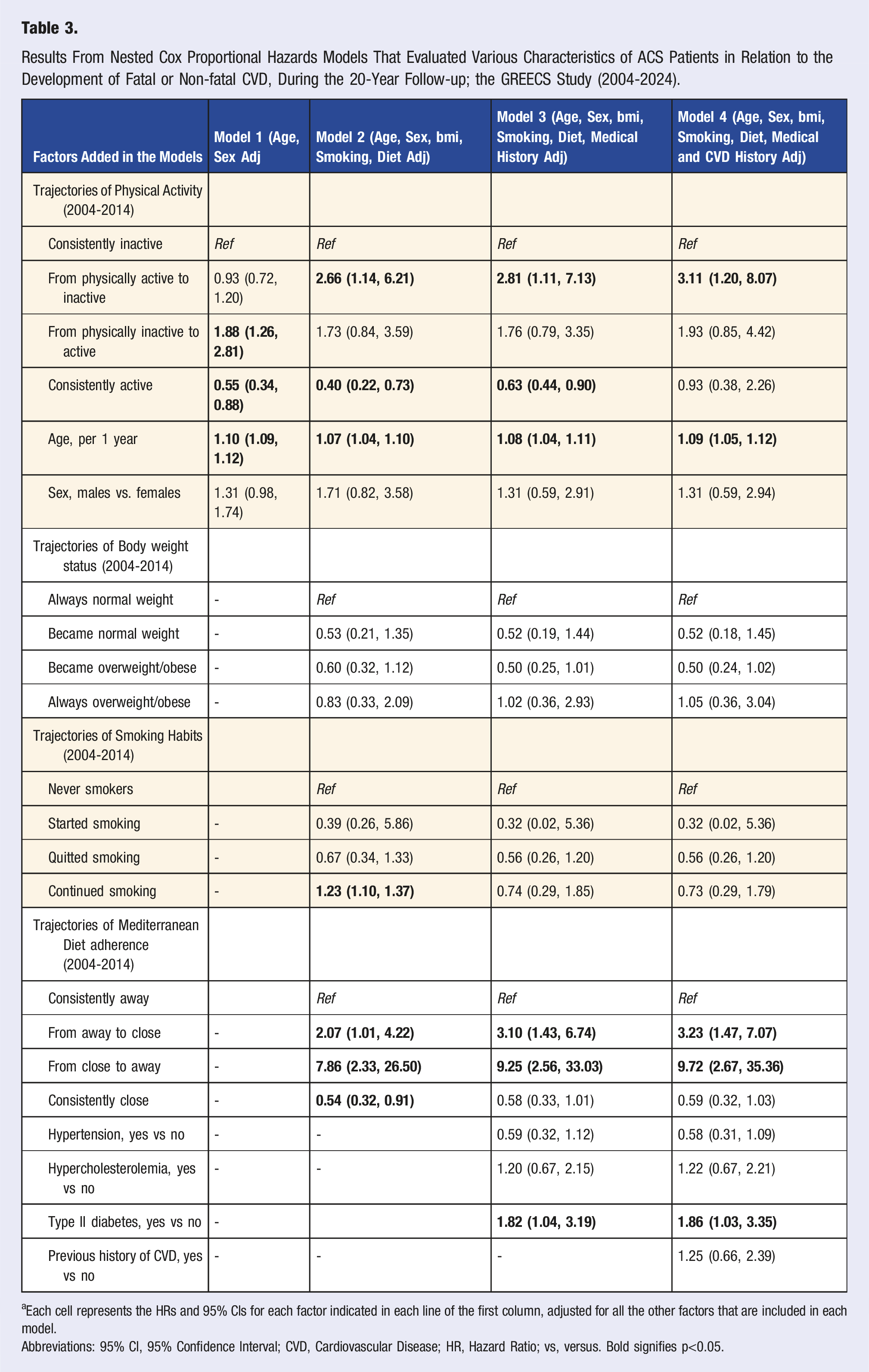
aEach cell represents the HRs and 95% CIs for each factor indicated in each line of the first column, adjusted for all the other factors that are included in each model.
Abbreviations: 95% CI, 95% Confidence Interval; CVD, Cardiovascular Disease; HR, Hazard Ratio; vs, versus. Bold signifies p<0.05.
Sensitivity analysis focusing on patients' medical history of CVD events showed that the protective effect of being consistently active remained significant only among those with prior history of CVD before hospital admission at baseline (HR 0.43 95% CI [0.20, 0.90]) as compared to physically inactive, whereas significance was lost among those without history of CVD (HR 0.61, 95% CI [0.32, 1.15]).
Discussion
The findings of the present study revealed that consistently being involved in physical activity was associated with an ameliorated long-term CVD prognosis in ACS patients. This study, conducted as part of the broader GREECS epidemiological investigation, aimed to assess the relationship between 20-year physical activity patterns and the incidence of combined CVD events in ACS patients. The prolonged follow-up duration of this study positions it as one of the few in the literature to longitudinally monitor heart patients over an extended period, offering critical insights into the long-term impact of various determinants on cardiovascular outcomes. Our findings provide robust evidence that sustained physical activity plays a critical role in long-term cardiovascular health, demonstrating a significant inverse association between consistently active lifestyles and recurrent ACS events. These results are in line with the growing body of evidence demonstrating the cardioprotective benefits of regular physical activity,18-20 while emphasizing that long-term commitment to physical activity is crucial to maximizing these benefits. 21
A key finding of our study was that only a trivial portion of ACS patients (7%) maintained a consistently active lifestyle over the 20-year follow-up period. In contrast, a significant proportion (i.e., 51%) remained consistently inactive, highlighting a significant public health challenge in promoting and sustaining physical activity among individuals with a history of ACS. 22 This is aligned with the findings of a previous population-based study where almost half of the participants remained physically inactive through the entire 20-year studied period. 23 Notably, a sizable proportion of patients (31%) transitioned from being physically active to inactive, suggesting a need for interventions to prevent relapse into sedentary behaviors. Moreover, individuals who transitioned from being physically active to inactive faced a higher risk of cardiovascular events, likely due to the loss of exercise-related protective effects on vascular function, lipid metabolism, and inflammation regulation. This decline can result in elevated blood pressure, insulin resistance, and systemic inflammation, thereby accelerating atherosclerosis and increasing vulnerability to other cardiovascular complications.
Nevertheless, patients who maintained an active lifestyle throughout the 20-year period, exhibited a more favorable lifestyle profile as compared to those who were consistently inactive. Specifically, regularly active individuals were more likely to adhere to the Mediterranean diet and maintain a normal and healthy weight. These findings underscore the interrelation of lifestyle factors in influencing cardiovascular health and highlight the potential for synergistic effects of multiple healthy behaviors. 24 Moreover, our findings revealed that changes in physical activity patterns over time were associated with significant differences in cumulative cardiovascular risk. Patients who transitioned from being inactive to active experienced some benefits in terms of risk factor profiles; however, these benefits were not as pronounced as those seen in consistently active individuals. This finding suggests that while initiating physical activity later in life can still be beneficial, earlier and sustained engagement may confer greater cardioprotective effects.25,26 Of particular interest is the fact that a significant percentage of patients transitioned from being active to inactive, which suggests that adherence to physical activity recommendations may be challenging for individuals with a history of ACS. This underscores the need for tailored interventions that address the obstacles and facilitators of physical activity adherence in this population. Factors such as lack of social support, fear of injury, comorbid medical conditions, and socio-economic characteristics may contribute to the decline in physical activity levels over time. 27
Several biological mechanisms may mediate the association between physical activity trajectories and CVD incidence. Physical activity has been shown to improve endothelial function, reduce inflammation, enhance insulin sensitivity, assist in blood pressure control, and promote favorable lipid profiles. 28 These mechanisms may contribute to stabilizing atherosclerotic plaques, reducing the risk of thrombotic events, and improving overall cardiovascular function. Physical activity has also been associated with reduced oxidative stress and improved cardiac autonomic function, additionally supporting its cardioprotective effects. Additionally, physical activity plays a vital role in cardiac rehabilitation by enhancing autonomic regulation, which improves heart rate variability and overall cardiovascular stability. Regular physical activity strengthens the myocardium, increasing its efficiency in pumping blood and reducing myocardial oxygen demand, which is particularly beneficial for individuals with existing heart disease. Improved heart rate variability reflects better autonomic balance, reducing excessive sympathetic activity that can contribute to arrhythmias. Furthermore, physical activity helps prevent cardiac remodeling and left ventricular dysfunction, key factors in the progression of heart failure. 29
Limitations
This is an observational cohort study, and as such is affected by several limitations that should be acknowledged before the generalization of the results. Physical activity assessment was completed by gathering self-reported data by the patients which may be subject to recall bias and social desirability bias. 30 Although the IPAQ tool used has been found reliable and valid for population studies, exact information on energy expenditure was not possible to be adequately evaluated. The trajectories in physical activity, as well as smoking, dietary habits, and obesity status were assessed during the first decade of follow-up to prevent overlap between lifestyle changes and the onset of the investigated CVD outcome and minimize the risk of reverse causality. Although the loss to follow-up in this cohort was relatively low (12%), differences in physical activity trajectories between participants who completed the 20-year follow-up and those who were lost to follow-up may affect the generalizability of the results. Individuals who dropped out may have had distinct lifestyle patterns, health statuses, or levels of physical activity over time, potentially introducing selection bias and limiting the extent to which the findings can be applied to broader populations.
Implications for Research and Practice
Notwithstanding these limitations, our findings have substantial propositions for research and practice. Based on the present outcomes, future interventions could be more appropriately customized to the specific needs and preferences of individuals and address the various barriers to physical activity adherence. Furthermore, the biological mechanisms through which physical activity utilizes its cardioprotective effects in ACS patients need to be more thoroughly investigated in the next years, potentially through multi-omics approaches. In clinical practice, emphasis on the importance of continuous physical activity as a foundation of secondary ACS prevention by health care providers might play a key role in health promotion. Patients could be encouraged to participate in regular physical activity and be given the necessary support and resources to achieve this goal. Cardiac rehabilitation programs, through integrate strategies to encourage long-term adherence to physical activity recommendations and emphasize the importance of addressing individual barriers and building social support, could also assist in the improvement of patients’ quality of life.
Conclusion
In conclusion, our study provides compelling evidence that sustained engagement in physical activity is associated with a reduced risk of recurrent ACS events. These findings underscore the importance of promoting and sustaining physical activity as a key component of secondary ACS prevention. Future research needs to focus on developing and testing interventions to improve physical activity adherence in this population, and health care providers could adopt a more decisive way to advocate for physical activity as an integral part of cardiac rehabilitation and long-term cardiovascular health.
Footnotes
Author contributions
N.D., concept, data analyses and interpretation, drafted the paper; V.N., S.K., P.K., L.K., E.T., C.T., performed clinical evaluations at follow-up, reviewed the paper; Y.K., P.S., G.P., S.Z., Y.M.; methodology, clinical evaluation, reviewed the paper; A.L., reviewed the paper; G.A., K.D.T., concept, reviewed the paper, C.P., D.P., designed the study, supervised data acquisition and analyses, wrote the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.