
Abstract
With more than 85% of health care costs attributable to chronic health conditions, an emphasis on treating the underlying causes of these conditions is imperative. Lifestyle medicine offers treatments that can reverse a wide range of chronic health conditions at minimal cost and without negative side effects. Although one might expect its use to be widespread among health care professionals, it is far from common in everyday practice. A significant contributing factor is the lack of financial incentives for health care providers who practice lifestyle medicine. Current practitioners generally do not receive remuneration consistent with the cost savings resulting from reversing chronic health conditions using lifestyle medicine. The Actuarial Patient Value model offers a new approach to encourage the practice of lifestyle medicine through the use of cash financial incentives based on actual patient health outcomes. This model aligns the incentives of the 3 primary stakeholders in the health care system by offering providers increased compensation, giving patients the opportunity to learn about and achieve optimal health, and reducing costs for health care payers.
‘Currently, successful practitioners who help patients reverse chronic health conditions generate considerable future cost savings but are provided with little reward in return.’
The ability of lifestyle medicine to effectively reverse and prevent chronic health conditions is well documented in the scientific literature. 1 However, with 18% of U.S. GDP consumed by health care costs largely attributable to chronic health conditions, it is clear that the use of lifestyle medicine has not been widely adopted.2,3 One of the primary reasons is the lack of financial incentives motivating health care professionals to practice lifestyle medicine.
Currently, successful practitioners who help patients reverse chronic health conditions generate considerable future cost savings but are provided with little reward in return. Reimbursement systems such as fee-for-service actually penalize providers for using lifestyle medicine because patients do not need as many (or potentially any) procedures, prescriptions, or office visits. This results in lower revenue for their practice. Salaried providers also have no financial incentive to use lifestyle medicine, as their income remains constant regardless of patient health.
Newer methods, such as value-based reimbursement methods, while promising, are not structured to incentivize lifestyle medicine since the value of services provided, as measured by patient health outcomes, is not being quantified. Many of these value-based arrangements rely on the Healthcare Effectiveness Data and Information Set (HEDIS), which consists of about 80 different measures that are “used by more than 90 percent of America’s health plans to measure performance on important dimensions of care and service.” 4 The Centers for Medicare and Medicaid Services also use these measures as part of its Quality Payment Program whose goal is helping providers “focus on care quality and the one thing that matters most—making patients healthier.” 5 However, as Harvard economist Michael Porter observed, “In practice, quality usually means adherence to evidence based guidelines, and quality measurement focuses overwhelmingly on care processes.” He characterized HEDIS primarily as “process measures, and none are true outcomes.” 6
To clarify the distinction between care processes and health outcomes, consider the measure “Comprehensive Diabetes Care: HbA1c Poor Control,” which is the percentage of patients who have HbA1c readings of greater than 9% or failed to have their HbA1c recorded during the year. 7 Given that accepted diabetic control is HbA1c less than 7%, a goal of 9% does little to encourage treatment proven to reverse diabetes. 8 Although most physicians themselves do not believe that these and other similar measures are indicative of care quality, they are incentivized to make sure patients take their medications, preventative screenings are performed on schedule, and the resulting data is recorded in the medical records, rather than focusing their practice on techniques that reverse chronic disease. 9
It is no surprise how existing reimbursement systems have developed, as it is much easier to assign a dollar figure to an office visit, prescription fill, or surgical procedure than to determine what a patient’s health outcome is worth. Further complicating matters is the lack of appreciation by health care reimbursement systems that chronic conditions such as heart disease or diabetes can be reversible. Even among those who are familiar with these treatments, reimbursement of lifestyle medicine is often viewed as impractical. For example, one cannot prove that a heart attack would have occurred had a patient not changed their lifestyle. Without proof of how much money was saved, the value of health improvements achieved by the practice of lifestyle medicine are not recognized in existing reimbursement systems.
However, despite the apparent complexity, it is possible to design and implement a reimbursement model offering financial incentives tied directly to patient health outcomes. While it is true one cannot determine whether health “events” such as a heart attack or diabetic complications will or will not occur for any given patient, by correlating certain patient health indicators and health care claims from a large actuarially credible population, the average expected cost savings due to health improvements from lifestyle change can be quantified. Then, a portion of these savings can be paid to the responsible health care provider. This not only makes lifestyle medicine financially viable, but lucrative to practice in this fashion as well.
The first step in developing such a reimbursement model is to determine measures that provide a clear and objective view of patient health. Some possible measures to consider include, but are not limited to, body mass index, blood pressure, HbA1c, cholesterol levels, triglycerides, insulin sensitivity, C-reactive protein, and endothelial function. The key is to select a small number of measures that minimize administrative burden, but still serve as a reliable predictor of health care costs. The second step is to associate actual values of these measures with the health care cost data for individual patients. For example, with adequate data, it is a relatively simple actuarial exercise to quantify the expected annual health care expenditures for individuals at varying levels of HbA1c (eg, HbA1c of 9.0 = $15 000, HbA1c of 8.0 = $12 000, etc). Then, if the correlation between HbA1c and health care costs is high, HbA1c would be a likely candidate to use as a value-based measure. If one measure alone does not demonstrate predictive value, it may be necessary to use multiple measures. That is, a moderately high body mass index may not have a significant relationship to costs, for example, but when combined with HbA1c results in an improved correlation. This suggests that both measures should be used.
Once it is determined which measures to use and the accompanying cost data is captured, the model can be implemented. An example of this Actuarial Patient Value (APV) model illustrated in Table 1 shows that a patient with an HbA1c of 9.0 is expected to incur $15 000 in total annual health care costs, of which the primary care provider receives $1500. If the patient’s HbA1c is reduced to 6.5 the annual expected cost drops to $7500. Assuming the relationship is linear from 9.0 to 6.5 one could observe that every 1-point drop in HbA1c is worth $3000 in cost savings (eg, 9.0 − 6.5 = 2.5; $7500/2.5 = $3000). The provider has done a great service in helping the patient improve his or her health and reduce overall costs, but in a fee-for-service environment, the revenue generated by this provider drops to $750 since the patient has less need for future medical services. However, with the APV model, the provider receives an incentive payment of $2000, bringing the total revenue to $2750, an increase of 83%. After accounting for this $2000 incentive payment, a net savings of $5500 is still achieved. The model also takes a long-term approach, recognizing that reversing a chronic condition will result in significant savings for the remaining lifetime of the patient. As a result, the $2000 incentive payment continues for many years, with the amount potentially increasing if patient health improves further.
Actuarial Patient Value Model. a
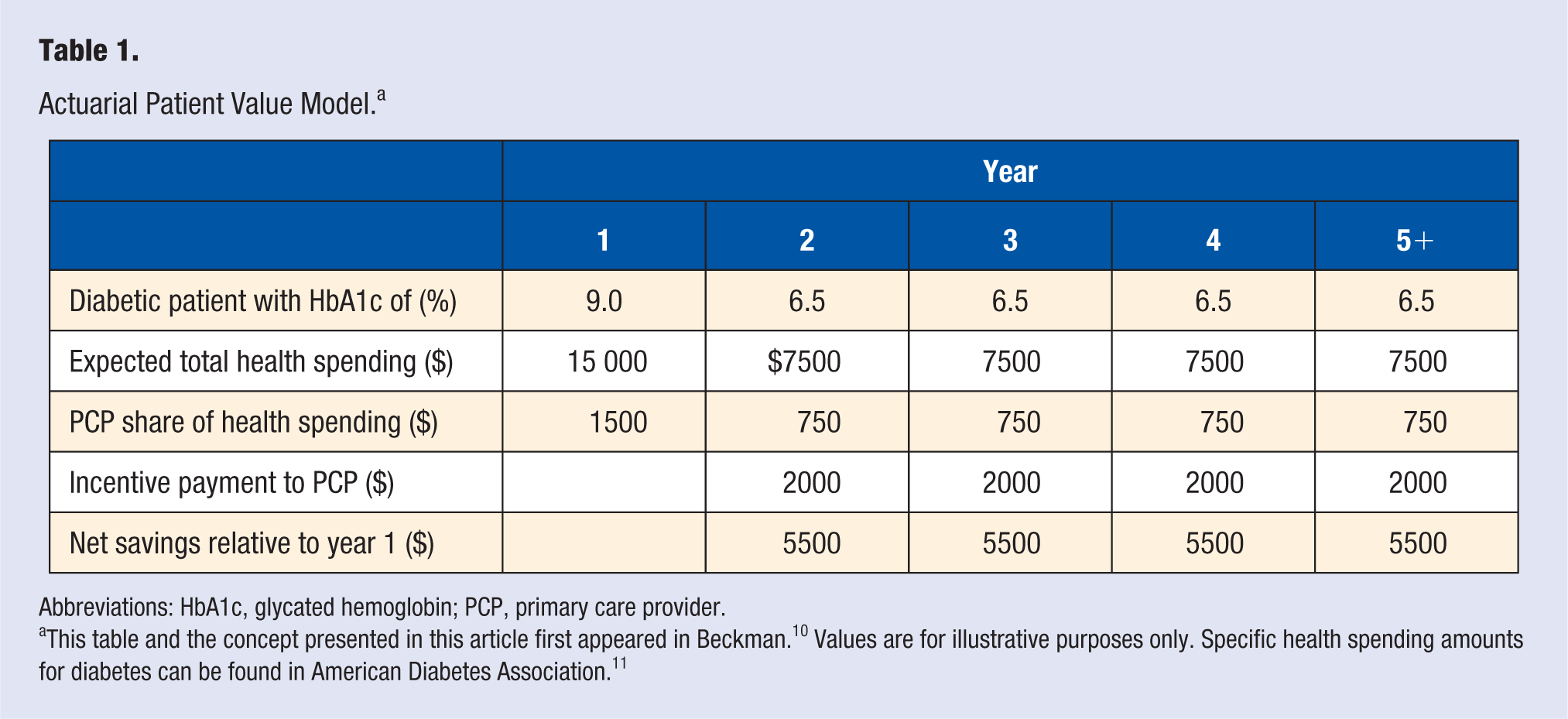
Abbreviations: HbA1c, glycated hemoglobin; PCP, primary care provider.
While the example in Table 1 illustrated a primary care environment, the concept of the APV model can used in many other clinical settings. Applying this model to specialists performing high cost procedures could result in significant reductions in health care spending. There are many common elective procedures, such as bypass surgery, angioplasty, stents, and bariatric surgery, which in many cases can be avoided by choosing a lifestyle medicine approach. Consider the case of a patient who has been referred to a cardiac surgeon for bypass surgery. The surgeon will earn $5000 for this and every other bypass in a procedure costing $150 000 in total. Purely from a financial perspective, the surgeon has an incentive to perform as many surgeries as possible. However, under the APV model, the surgeon would be paid $10 000 to not perform the surgery—by giving the patient the option to avoid the procedure (and the potential complications and side effects) simply by adopting whole food plant-based nutrition and other intensive lifestyle changes. As a result, the surgery is not performed, the patient is able to stop the progression and potentially reverse the heart disease, the surgeon earns more money, and overall spending on health care is reduced by $140 000.
While the APV model offers attractive financial incentives for health care providers, some providers may consider it difficult to participate because of their unfamiliarity with lifestyle medicine or lack of infrastructure to provide the ongoing education and support that patients need when making lifestyle changes. However, it is not necessary for the provider to become an expert in every aspect of lifestyle change. The primary role of the provider is to simply make the patient aware that lifestyle medicine could achieve equal if not superior health outcomes (with no significant risks or side effects) compared to treatments based on drugs and surgery. For practical and in-depth guidance in implementing and maintaining lifestyle changes, the provider can refer the patient to a third-party expert.
There are many individuals and programs with proven expertise in delivering this type of education and continuing support through the use of in-person seminars, online programs, telephone coaching, and other methods. By using these resources, the provider does not have to devote any additional funds to building new facilities or hiring additional staff. They merely invest a small amount of time learning the basic concepts of lifestyle medicine so that it can be confidently explained as a viable treatment option, similar to what would be done with any prescription drug or procedure. There would be minimal or no upfront cash costs to the patient or provider for the services of the third-party expert. Instead, a portion of the incentive payment earned by the referring health care provider would be shared with the third party. In contrast to traditional “wellness” programs that typically come with an upfront cost per participant, these incentive payments are not made until it has been actuarially demonstrated that cost savings were achieved based on confirmed patient health outcomes. This unique “paying for results” feature serves as a powerful motivator for both the referring health care provider and third-party expert to work together using the best possible methods to achieve optimal patient health outcomes. Additionally, since there is no downside risk of capital, it eliminates a significant potential objection to implementing the model by the ultimate payers of health care, primarily self-insured employers and governments in the United States. Furthermore, payers do not have to dismantle existing provider reimbursement systems. The incentive payments from the APV model are made in addition to any compensation arrangements already in place. While adoption by government payers such as Medicare and Medicaid may require legislative action, self-insured employers, who are not subject to regulatory restriction, could implement this model quickly by corporate decision.
The financial incentives for health care providers to offer patients drugs and procedures are very effective and the resulting unsustainable trends in health care costs continue to reflect this fact. Lifestyle medicine offers a realistic solution, but currently lacks incentives for widespread adoption. The APV model rewards health care providers for their success, offers patients an opportunity to achieve optimal health, and benefits health care payers through substantially reduced expenditures. By moving away from a system focused on paying for health care services to one that values health care outcomes, the incentives of all stakeholders are aligned and real health care reform can be achieved.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.