
Abstract
The purpose of this case study was to explore 2, early-relationship, same-sex couples on the strategies used to support their partner’s engagement in health promoting behaviors. A semistructured interview protocol was used to conduct 120-minute interviews with each couple and analyzed using grounded theory methods. Five organizing categories emerged during the analysis, resulting in a conceptual process model of health-related support in same-sex relationships. These categories, provided a snapshot of how processes interact with each other; they were context, relationship dynamics, health support processes, couple adaptation, and balancing physical/relational health. Couples described the balancing of relational and physical health as an ongoing, important theme in the success of health support. Implications for both health prevention and intervention are discussed.
‘Ecological models of health behavior identify what factors influence an individual’s engagement in healthpromoting or health-damaging behaviors, ranging from individual characteristics to larger systemic and societal forces.’
Recent reports have identified that significant health disparities exist between gay and straight men throughout the United Sates, with gay men experiencing higher risk for a number of health issues. 1 These disparities cover a broad range, with significant differences in specific health conditions (ranging from diabetes, heart or lung conditions, or physical disability); health behaviors, such as heavy drinking and smoking; and health care access/utilization. 2 To address these disparities, researchers have relied on models of health behavior to create health promotion interventions. Ecological models of health behavior identify what factors influence an individual’s engagement in health-promoting or health-damaging behaviors, ranging from individual characteristics to larger systemic and societal forces. 3 Factors that have received considerable attention in the ecological model are interpersonal factors, including the quality and dynamics of social relationships (particularly romantic relationships), with research suggesting that the primary mechanisms through which romantic relationships influence health is through support or control. 4 However, most of this research on health behaviors and social relationships has focused on heterosexual relationships.
Although a few studies exist that identify how same-sex and heterosexual relationships are similar or different in regard to health,5-7 the lack of attention is alarming such that the development of effective prevention and intervention strategies to help improve health outcomes in this underrepresented population will likely remain challenging. As such, the purpose of this case study is to identify underlying contextual and relationship factors that influence engagement and interaction around health support strategies. To address these gaps, this study utilized semistructured interview data from 2 gay couples in early marriage. Grounded theory methodology was used to understand the processes that emerged from the data.
Literature Review
Relationships and Health
A wealth of research has explored positive and negative aspects that social relationships can have on health and health behaviors.8,9 Particularly, one mechanism through which marriage affects health is spousal influence. 10 Past research has mainly focused on the mechanisms through which individuals in straight relationships influence each partner’s health behaviors—health-related support or control. 4 Indeed, the gendered research suggests that women do more to promote their husbands’ health, 11 which explains why men may “benefit” more than women. This literature has relied on gender socialization theory, which states that women are socialized to care more about others’ health and express this care more than men. 11 However, research has begun to examine health promotion in gay and lesbian relationships, 12 and scholars are interested in how relationship dynamics in same-sex relationships may influence health behaviors differently from straight marriages. Of particular interest to the current study is the relationship dynamics between 2 men.
Gay Relationships and Health Behaviors
Some research has investigated differences between gay and straight relationships. In 2012, a qualitative study identified aspects of health behavior in gay and lesbian relationships. 6 The authors identified 2 distinct types of health behavior “work”: specialized health behavior work and cooperative health behavior work. Specialized health behavior work refers to when one partner seeks to enhance the other’s health throughout the course of the relationship. This type of work is more common when one partner identifies as “unhealthy” and the other is the “health expert.” In cooperative health behavior work, partners work together in mutually reinforcing ways to promote one another’s (and their own) health, and this is intermittent—or, as needed. Participants in the study described 3 discourses of similarity to explain this phenomenon: (1) both partners have always been on the same page about health behavior work; (2) both partners are on the same page about health behavior work as needed; or (3) partners take turns initiating cooperative health behavior work.
In 2006, a qualitative study of 60 gay, unmarried couples identified the health control strategies and tactics partners used and if their partners saw these as health enhancing or health compromising. 5 They found that partners used a variety of strategies, which were dependent on the interdependence of the couple, and that they were motivated by the care and concern for the other and the relationship. This study, however, only investigated control strategies and not how the couple navigated health support strategies.
Specifics of Health-Related Social Support
What does health-related social support look like specifically? Four specific types of social support have been documented: (1) emotional support, which includes expressions of empathy, love, trust, and caring; (2) instrumental support by giving tangible aid and services; (3) informational support, which includes advice, suggestions, and information; and (4) appraisal support, information that is useful for self-evaluation. 13 Documentation on how these are associated with better health/health behaviors suggests that social support can influence health behaviors directly or indirectly by buffering the effect of stress, 4 enhancing mental/emotional health, 14 or fostering symbolic meanings.15,16 Despite this, it is unclear as to how these mechanisms look specifically in gay relationships and how individual factors and larger couple-related factors affect health support strategies.
Theoretical Orientation
Although a variety of conceptual models of social support exist,13,17 there are few conceptual models that consider the interaction between both partners. Informed by Interdependence Theory,18,19 the Model of Interdependence and Communal Coping 20 was proposed, suggesting that initiation and maintenance of health-enhancing behaviors is rooted in couple dynamics. This dyad-level theory offers insight into reciprocal processes that affect each individual’s behavior and identifies important areas for potential prevention and intervention. 21 Specific to the context of health behavior, dyad-level theories account for both the intrapersonal and interpersonal factors and acknowledge up-front the interdependence of cognitions, emotions, and actions of each person in the relationship. 22
Along this vein, an important construct highlighted in this dyad-level theory is Transformation of Motivation, 20 which is the process that “accounts for changes in couple members’ behavior from a primarily self-centered orientation or motivation to one that is more prorelationship and health enhancing.”20(p1373) This occurs when both partners attribute health behaviors and events as meaningful for both partners in the relationship, not just for oneself or one’s partner. Consequently, spouses may be more accommodating, cooperative, and flexible in their approach to health and health behaviors. Taken together, this transformation is a result of the overall factors in the relationship—the roles, rules, and norms; the commitment and trust present; and the emotional and cognitive functioning during the couples’ interaction and communication. 20
Although these concepts and theoretical viewpoints are helpful, health support processes have not been studied or validated in same-sex relationships or in relationships in which both partners are relatively healthy and satisfied in their relationship. This is important to construct the most effective prevention efforts and identify potential points of intervention for couples who may have significant health concerns. The present study was guided by the following questions:
RQ1: How do individual contextual factors influence health support processes?
RQ2: How do couples navigate engagement in social support strategies?
RQ2: How do these strategies affect the couple relationship?
Methods
Procedure and Recruitment
We recruited participants via local pride festivals and by word of mouth in a southwestern state in the United States. Inclusion criteria for participation in the study were identifying as male, identifying a nonheterosexual orientation, and currently in a same-sex marriage. If couples met the criteria, they were contacted by the researchers via email or telephone and invited to participate in the study. A total of 4 couples responded and met initial inclusion criteria; 3 agreed to participate in the interview, but only 2 couples were in early, happy marriages and fit the focus of the present study. After giving their consent to participate, each couple was interviewed together. Each couple received $20 in cash to participate. All procedures were approved by a university institutional review board.
Sample
Participants for this study consisted of 2 same-sex couples within their first year of marriage. All 4 individuals were in their 20s; 3 were Caucasian; and 1 identified as Hispanic. One member from each relationship was a student in college and the other member from each relationship was employed full-time. Using the Couple Satisfaction Index, 23 all 4 respondents indicated that they were very happy in their current relationship. Finally, only one member of a couple had been diagnosed with a significant health condition (high blood pressure).
Instruments
Semistructured interviews were conducted with the 2 couples. The interview consisted of several broad questions regarding similarity of perceptions in health and illness, negotiation/interaction around specific health behaviors (diet, exercise, sleep, and alcohol/drug use), what strategies each engaged in to support his partner, and the dynamics/make up of their relationship (see the appendix for list of prompt questions). Each interviewer was accompanied by the second author.
Transcribing and Coding
Recordings of the interviews were first transcribed by a team of undergraduate research assistants. Next, a team consisting of an assistant professor, master’s student, and undergraduate student undertook the process of coding the transcripts. The purpose of data analysis is to bring order to the data, so that answers provide meaning and credibility. 24 Grounded theory techniques and a critical theory perspective were used for the analysis of the transcripts. This process involved immersion in the data (carefully reading the interviews) and then labeling sessions according to conceptual meanings (open coding). Each transcript was read in its entirety using the “beginner’s mind” approach. 25 Next, more focused coding occurred as the concepts with the most explanatory power were developed into categories from the most meaningful codes. This was a natural process because some categories develop properties and dimensions, and others are set aside.
Reflexivity and Validity
In qualitative research and critical approaches, it is important for researchers to be reflexive about their presence. Scholars suggested that to preserve the integrity of a study, researchers should articulate the epistemological stance they espouse before carrying out research. 26 Additionally, our subjectivist approach acknowledges up-front the constructed nature of research results. Verification strategies were also used to ensure trustworthiness and rigor of results. These included using multiple coders for research triangulation, peer debriefing, memo taking, and an internal audit. 27 Despite these efforts, we acknowledge that any description of the analysis may not capture the complex, intuitive, and inductive nature of the process. 28
Results
What Are the Themes and Couple Processes Related to Same-Sex Couples and Health Behaviors?
The model that resulted from the analysis (see Figure 1) depicts the main concepts organized within 5 categories. In our initial stages, some of the categories were conceptualized as being too specific. However, as the analysis proceeded (in the axial coding and member checking phases) more overlap between these emerging themes was found and concepts were collapsed and refined. The final model shows the concepts that seemed to be relevant to both couples’ experience. The first category included the context that included themes relevant to each individual’s background. The second category included relationship dynamics and included several themes related to how the couple interacts and maintains the relationship, and underlying processes. The third category of health support processes referred to several processes each individual identified related to the actual giving of health support. The fourth category of couple adaptation included the process by which partners managed, communicated, and worked through health issues. Finally, the fifth category of balancing physical and relational health emerged as an overarching theme on how couples balanced their individual physical health and the health of their relationship with their partner.
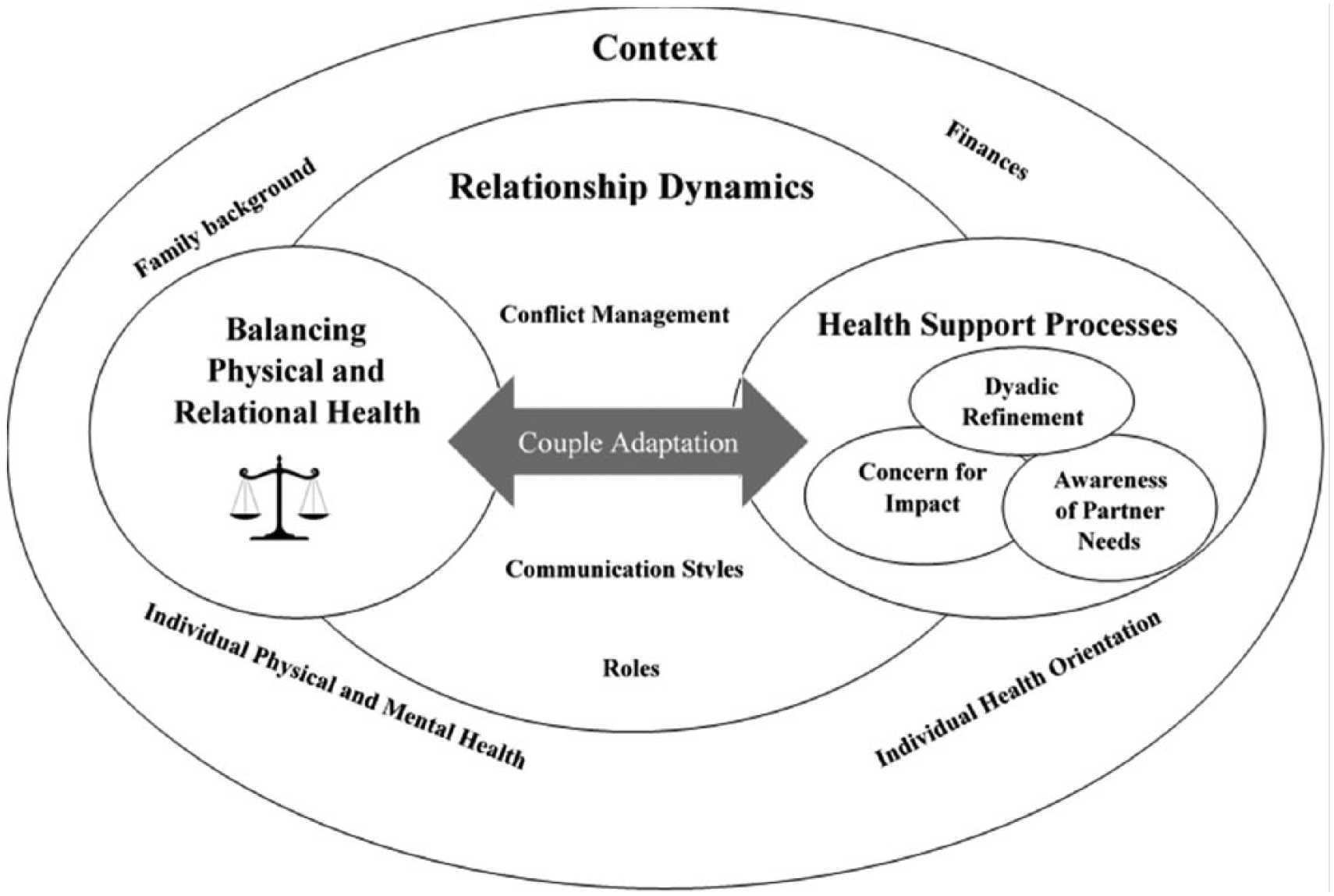
A process model of health-related support in early, happy, gay marriages.
Context
The category of context emerged as part of couples’ descriptions of the experiences and influences they brought to the current relationship. This category included 4 concepts that emerged during the interview: family background/history, individual mental/physical health, individual health goals/preferences/knowledge, and financial situation. For both couples, the category of context seemed to be an underlying process that affected all of the categories and concepts.
Family Background
Family of origin attitudes and behaviors about health were identified as important contextual variables that they identified and brought to the relationship. A member from the first couple identified it this way: Salt was a big deal and we had to redefine health. My family, the whole family tree is kind of just a bunch of foodies and so am I. We love flavor in all things and all cuisines and that usually involves salt in everything.
A member from the second couple described his experience with family background factors: [He] comes from a family that, they love their exercise every occasionally but they’re not nearly as health conscious as my family. They love to drink soda all the time, they love their sweets, whereas my family’s very conscious they never drink soda, they’re super health conscious, always trying to eat healthy foods. I’ve just grown up with that and have that consciousness.
Individual Mental and Physical Health
Individual mental and physical health refers to specific diagnoses or conditions that an individual reported as an important background factor. A member from couple 2 indicated his experience: “I’ve previously been diagnosed with an anxiety issue, and so that catches up with me a lot.” An individual from couple 1 reported some physical health conditions: “So I went to the doctor not long ago and the doctor said, “Yeah you’re, you need medication for blood pressure, and you’re just way up there. So we had to redefine what health means for me.”
Individual Health Preferences, Knowledge, and Goals
Individual health preferences, knowledge, and goals refers to the differing orientations toward health and health behaviors that each partner identified. A member from couple 2 described it this way: “I’m not saying that’s what he wants either but he’s much more into building muscle, I’m just more, our goals, exercise wise are different.” Another partner described it this way: “As far as physical health, he’s always a little more conscious about what he eats. He goes to the gym and doesn’t mind lifting weights. And I’m not one of those people that likes to lift weights at all.”
Financial Situation
Finances was an important contextual variable that influenced health and health behaviors. A member from couple 2 described it this way: “We’re, we’re kind of in the experimenting stage right now, trying to figure out what works with the budget but is still really healthy and we try to get enough meat and vegetables.”
Relationship Dynamics
The category of relationship dynamics emerged as part of couples’ descriptions of how they functioned together as a couple. This category included 3 concepts, including communication styles, conflict management, and roles. These were general and evident in matters not specifically related to health and health behaviors but were influenced by the aforementioned contextual factors.
Communication Styles
The concept of communication styles refers to differences in how members in the couple communicate and interact with the other and is embedded in context—that is, the contextual variables influence the relationship dynamics. A member from couple 2 described his communication style: “I’m much more passive, he’s much more, [snapping fingers] let’s iron this out now, and so I think we’ve learned a little bit about when we can, when he can push me a little bit and when to talk and to communicate a little bit more.”
A member from couple 1 described it as his orientation to communication: If I’m worried that I am not doing right by my husband, I try to address that as quickly as I realize it because you don’t always necessarily realize a problem until it happens a few times and it becomes apparent and I usually try to address that as quickly as I can because I don’t like the idea of putting him through any unnecessary stress or and hindrance simply because I didn’t know to ask a question.
Conflict Management
The concept of conflict management refers to the way couples described how they work through conflict together. A member from couple 1 defined conflict management this way: “When you have good communication nothing really feels like a negotiation. We kind of we tend to naturally gravitate towards same answer after we have put all of our thoughts on the table.”
Couple 2 described it this way:
Sometimes we’ll reach a point when we just need to hash it out, sometimes we can sense when we need to give each other a little bit of space. I think especially over the last year, we’ve both improved our communication skills a lot and we’ve realized the value of that.
Yeah, I think the reason I’m such a communicator is from the experience of habit. Because I’ve dated quite a few guys in the past. And I noticed that that was something that was probably the biggest issue, of all those relationships is communication. Not talking about things when issues were coming up, being passive-aggressive about things, deciding. . . . “I’ll wait until he figures out something’s wrong.”
Roles
The concept of roles emerged related to how they handle aspects of taking care of the home, financial management, and cleaning. A member from couple 2 defined it as having equal roles: “We cook pretty evenly. We take turns. We take turns grocery shopping, making the grocery list for like two weeks he’ll do it the next two weeks I’ll do it.” A member from couple 1 defined their respective roles differently, with one being more of a traditional homemaker and the other provider: “I have less time at home so he usually ends up doing things like the laundry and his favorite, the dishes and I go to work and do my thing. So we try both work but in our own ways.”
Health Support Process
The category of health support process emerged as important processes an individual recognizes when thinking about how to approach health-related support. These encompass awareness of their partner’s needs, concern for the impact it may have on their partner, and dyadic refinement—the process through which couples work through health-related issues. This category was embedded within couple relationship dynamics and influenced by those contextual factors.
Awareness of Partner’s Needs
The concept of awareness of partner’s needs refers to how one partner anticipates and takes into account aspects of their partner’s lives when making decisions about health behavior. A member from couple 1 described it this way: I’ll pay attention when he goes to the gym for example he’ll let me know “I’m going to be going to the gym for a couple of hours and be back” and I’ll change the dinner menu to have more protein depending on what he needs for that day. If I know he’s going to have some really late nights I’ll load him up with more immediate energy sources.
A member from couple 2 described it this way: It’s helped me so when I start to plan I start thinking, okay, he’s so healthy minded and he’s been working out. He works hard and he’s been seeing results but I also know that he’s been doing a lot of work outside of just my dinners. So I’ve been trying to incorporate a more healthy variety of food [when I cook for him].”
Concern for Impact
The concept of concern for impact refers to an individual’s awareness of how a health-support strategy may come across to their partner. This cognitive reflection emerged as an important aspect in how they phrased and worded their support attempts. A member from couple 1 referred to it this way: “Yeah not in like a rude way like “you’re not . . . no, no, no,” but I try to be as gentle with it as possible because the point is not to call him out in doing something wrong so much as just to point out like just make sure he realizes what he’s doing.” A member from partner 2 described it similarly: “I’ve never wanted to make him feel like he has to do it, and I, never ever want him to feel like he’s not good enough, so he needs to change something about his physical appearance or his eating habits or anything like that.”
Dyadic refinement
Dyadic refinement refers to the interdependent process in which partners in the relationship work to understand how support strategies are presented. Couple 2 defined this process in this way:
I notice you don’t really tolerate guilt strategies either. From me.
I hate guilt trips. I hate guilt trips to the point that if I sense a guilt trip I will intentionally push the opposite way . . . that’s the way I react to guilt. I feel like it’s someone trying to manipulate me and I’m sensitive to that. It was “can we do this together?” it’s really the best strategy I guess, after all those negative things, with the guilt and the manipulation has just been as simple as just asking.
A member from couple 1 defined the dyadic refinement process as follows (referring to health behaviors): At its core I feel loved, he knows me well enough to know that out of my best intentions I’m still going to forget some things. And what I really liked was we kind of reached a certain consecutive times I forgot to do something and he kind of just looked at me like, “How do we get better at this because this seems important for your health?”
Couple Adaptation
The category of couple adaptation refers to the process couples go through following a health-related support attempt and the way they discuss when one partner engages in a support strategy. Again, this category was influenced by previous contextual factors and relationship dynamics but emerged as an important process that occurred following the health support process.
A partner from couple 1 referred to it this way: It doesn’t feel like a negotiation it’s just something was on my mind, we discussed it, came to a conclusion or didn’t and kind of moved on so I guess in terms of negotiations it’s just very where we handle it frequently, often on smaller scale issues I guess . . . nothing accrues, nothing snowballs into this big fight.
A partner from couple 2 described their experience of couple adaptation: I mean, sometimes the, I guess it depends on how patient either of us are at the moment, when something comes up. Usually we clash, then, we get mad at each other, we’ll stop to each other for a minute, and then we’re like “Okay” and we’ll get back together, “let’s talk this out” and try to be respectful and not try to like, change each other too much . . . when we’re actually in those moments of talking about it.
Balancing Physical/Relational Health
Balancing physical and relational health emerged as an overarching goal of both couples—positive health behaviors are not an individual process that occur in a vacuum, but physical health is an interdependent process important for the health of the relationship.
A member from couple 2 described the balance this way: “It wasn’t me asking, but it was him that approached me and said, you know, if we can follow and can live by these guidelines, then I think this would be okay in our relationship. A member from couple 1 expressed the balance similarly: It’s also about future thinking of building your future together, that idea that concept really appeals to me uh and I don’t want to put myself in a position where I’m short changing him out of time with me because I decided not to diet and exercise. So in that sense of long term view of my life I’m now making healthier choices more so than I would have if I was on my own even if initially I was healthier on my own.
Discussion
The purpose of this study was to identify a conceptual process model of the themes that emerged related to how gay men and their partners in early, happy marriages interact around health/health behaviors. The 5 themes—context, relationship dynamics, health support process, couple adaptation, and balancing physical/relational health—seemed to emerge from both couples’ experiences. These findings are important and can inform future prevention and intervention efforts.
Although our study aligns with concepts from many of the ecological models of health behavior,29-33 it also extends models of social support (eg, the Model for the Relationship of Social Networks and Social Support to Health 13 ) in several important ways. First, the current study suggests a more nuanced delineation to the interpersonal level, highlighting that several important constructs operate within the interpersonal domain and affect health behavior. Specifically, the mechanisms of health-related support do not occur in a vacuum outside of the relationship dynamics, but the couple’s underlying dynamics influence how these processes operate. The themes of conflict management, relationship roles, and communication styles exhibit an important influence on how health-related support is received and perceived by a partner. This supports the theoretical construct of transformation of motivation, 20 in that the underlying processes of the relationship are taken into account when giving health-related support.
Second, on a related note, our study highlights the importance of the overarching construct of balancing relational and physical health. This finding suggests that health support operates in tandem with relationship well-being, such that a sort of give-and-take is present—when the relationship is doing well, health support is well received, but when the relationship is struggling, health support may harm the relationship. This supports research about perceptions of care and concern coming from a partner during health-related strategies in same-sex marriages 5 and is demonstrated in 2 important ways.
First, we identified important themes under health support processes within happy, early gay marriage relationships: awareness of partner’s needs, concern for impact, and dyadic refinement. Awareness of partner’s needs was the anticipation, forethought, and intentionality of knowing how to help support their partner. Concern for impact was a cognitive reflection on the tone, phrasing, and potential perception of how a support strategy could come across to the partner. Finally, dyadic refinement was the process by which both members communicated and interacted around health support strategies, and jointly decided which strategies were most helpful (or not). Taken together, these findings add to the knowledge base of the process by which health support operates in gay relationships, specifically that there are cognitive and emotional intent, and communication and interaction behind these strategies.
Second, the theme of couple adaptation emerged as the process by which partners manage how the health support strategies affect the balance of physical and relationship health. Although similar to the dyadic refinement process, this concept appeared more global to the relationship following the health support strategies. This finding supports the concept of communal coping in Lewis et al, 20 in that it is the shared, interdependent management and negotiation of health behaviors. It is during this process that couples decide how and if the health support is beneficial to the relationship (or vice versa) in which they make decisions related to engaging in a health behavior or not. It is perhaps this mechanism that might not only describe a reduction in risky health behaviors in the transition to marriage,34,35 but also explain why the married may weigh more and exercise less11,36,37—they take into account how their health behaviors may influence the relationship and adapt together.
Finally, our study supports the concept of context (or individual-level factors) from many of the ecological models of health behavior29-33 and that these seemed to influence core dynamics of the relationship. Specifically, the findings from the current study suggest that family background (including family history of physical illnesses and genetic influences), individual physical and mental health issues, the financial situation, and the individual’s own health orientation exert a force on couple dynamics. This answers one of the critiques of several ecological models of health behavior that a lack of research has identified how variables interact across levels. 3
Implications for Prevention and Intervention
Although the findings from this study were drawn from a sample of early and happy gay marriage relationships, they can nonetheless inform prevention and intervention efforts. First, as previously stated, the processes that emerged reflected important delineations in how the interpersonal and individual levels of ecological models of health behaviors interact and inform each other. As such, health education and promotion programs for same-sex couples should consider including the partner for maximum impact in prevention efforts. Health educators could include modules/discussion about relationship well-being, with specific focus on how health support strategies could be communicated via in tone, phrasing, and the potential impact it could have on the partner. Additionally, facilitators of these courses could help couples discuss the ways in which their strategies are perceived (modeling dyadic refinement), thus opening up space for these dialogs to continue in the future.
Conversely, because our study shows the interdependence between health support behaviors and relationship functioning, health educators and promoters could encourage or refer same-sex couples to attend relationship and marriage education programs that target important relationship skills, such as communication, conflict resolution, and balancing roles. 38 These skills could help with the indirect mechanisms associated with health (stress 4 and mental/emotional health 14 ) as well as make room for direct impacts on health by improving health-related communication and support.
Finally, specific to intervention, health care providers—who work with individuals with chronic illnesses or those who are struggling to maintain health behaviors—might consider including the partner in treatment.20,39,40 A multitude of studies have documented that spousal/partner factors do indeed influence an individual’s management of and engagement in health behaviors, such as diet and exercise, and specifically that couple processes can attenuate negative health outcomes.41-43 Our study specifically shows that same-sex couples are not exempt from the importance of including partners in treatment. Although the stigma that gay men experience in the health care system has been documented, 44 health care providers would do well to overtly address the stigma by inviting gay males’ partners to join in the health management process.
Limitations and Directions for Future Research
Although this study identified several important themes, they must be considered in terms of its limitations. First, although the themes that emerged were consistent between both couples, the sample size is low, and future research should include more couples to understand if the phenomenon is accurately representative of the population. Second, the emerging themes represented couples who were in the earlier stages of their marriage and were happy. These themes may not be consistent in same-sex couples who have been together for longer periods or who are more distressed/unhappy. Future research should include couples in all relationship stages and levels of stability. Third, as with any self-report and incentivized research, the interviews are subject to response and social desirability bias, and as such, responses may not accurately reflect true participant experience. Along the same vein, those interviewed represented couples who were motivated by financial incentives, and thus, those who were not motivated in the same way may have different perspectives or experiences. Fourth, as previously stated, we acknowledge the constructed nature of the reported results and that other researchers might interpret the findings differently according to their own experiences and knowledge. Finally, although the sample was somewhat diverse, the themes reflected above do not take into account cultural and racial diversity and, as such, may change or influence the model considerably. In addition, although we were cognizant of our presence as researchers, the results may have been influenced by the power and privilege related to the interviewer/interviewee dynamic and the interview process.
Conclusion
The present study is among the first to identify the “process” of how couple relationship dynamics unfold concerning health-related support in early, happy, same-sex marriages. Five important themes emerged: context, relationship dynamics, health support process, couple adaptation, and balancing physical/relational health. Overall, our study shows the interrelatedness of contextual variables and the influence they have on couple dynamics and health support processes. Additionally, our study makes a case for understanding the layers and complexities involved in balancing physical and relational health in same-sex marriages. These findings raise important considerations for health education, prevention, and intervention efforts.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.