
Abstract
There is a high prevalence of children with obesity who are participating in sports. Appropriate nutritional considerations are important to optimize health and training adaptations. This review focuses on macronutrient recommendations and their effect on weight management and/or benefits for athletic training for children ages 5 to 18 years. Equal distribution of protein intake throughout the day (~25-30 g/meal) and during postexercise recovery is recommended. Special attention should be given to increasing protein intake during breakfast because it is often the meal with the least protein intake. Both postexercise recommendations for protein (~0.3 g/kg of body weight) and carbohydrate (~1.0-1.2 g/kg/h) were not determined in children with obesity, and require future verification. Individual carbohydrate needs of training to meet fuel costs are recommended, but ~200 to 500 g/day of carbohydrate may be required depending on a child’s level of sport participation and competition. Fat intake should follow general recommendations to meet the accepted macronutrient distribution range in children (25% to 35%) and reduce saturated fat intake. No evidence suggests that additional dietary fat modifications would improve training adaptations in children. Longitudinal studies are required to further our understanding of age and sex effects and confirm the appropriate quantity of macronutrients for active children with obesity.
‘In line with the prevalence of obesity in the general population, there is also a high prevalence of obesity in children who are participating in sports.’
The high prevalence of childhood obesity is contributing to a rise in metabolic complications earlier in life and in adulthood.1-3 Recent statistics in a nationally representative sample of children ages 2 to 19 years in the United States reported the prevalence of obesity was 17% and extreme obesity was 5.8% in 2011 to 2014. 4 The Centers for Disease Control and Prevention cut-points define overweight and obesity as ≥85th and ≥95th percentiles for body mass index (BMI) for age and sex, respectively. These definitions will be used for overweight and obesity unless otherwise stated below. The word “children” in this review includes children and adolescents and will be used to refer to individuals ages 5 to 18 years unless otherwise stated.
In line with the prevalence of obesity in the general population, there is also a high prevalence of obesity in children who are participating in sports. Some data are provided using preparticipation physical evaluation data, which were collected at the start of competition season for organized sports in the United States. Kropa et al 5 reported 20% and 24% of student athletes were overweight or obese, respectively, in a sample of 2678 athletes in Philadelphia. Similarly, Stiefel and colleagues 6 reported the prevalence of obesity was 23.5% in students participating in sports in Mississippi between 2009 and 2012 based on 7705 preparticipation physical evaluation results. Even in children participating in sports, the data showed a greater risk for high blood pressure in children with obesity compared with children without obesity defined by BMI-for-age cut-points.5,6 High blood pressure identified in young athletes with obesity warrants concern. 6 Stiefel et al 6 reported that participating in more than one sport reduced the relative risk of obesity and high blood pressure by at least 1.42 and 1.30 times, respectively. Another study reported that sport participation was beneficial in children (mean age = 8.4 ± 1.4 years) for reducing clustered cardiovascular risk score, which was composed of fasting serum triglyceride levels, insulin resistance, total high-density lipoprotein cholesterol ratio, and systolic blood pressure. 7 More specifically, participating in organized sport over 53 weeks decreased insulin resistance and fasting insulin levels by 3.5% and 2.6%, respectively. 7 When discussing obesity and cardiovascular risk, it is also important to consider cardiorespiratory fitness. Although increasing fatness is associated with cardiovascular risk in adolescents (mean age = 16.1 ± 0.5 years), higher fitness is associated with a reduced effect of increasing fatness on clustered cardiovascular risk. 8 In children ages 11 to 18 years, sports participation increased the chances of being fit (odds ratio = 13.5; 95% confidence interval = 4.6-39.9), independent of moderate-to-physical activity. 9 Therefore, sports participation may also improve fitness in children and reduce cardiovascular risk factors.
In the study by Stiefel et al, 6 the authors noted that in children identified as single-sport athletes, certain sports showed a higher obesity prevalence. The top 3 sports with the highest obesity prevalence included American football (39.4%), softball (25%), and golf (25%) for the adolescents examined in the study. 6 Indeed, there seems to be a selection bias for children who are overweight or obese in select sports, such as American football, which has also been shown in other studies.10,11
In many studies on obesity and sports participation, we acknowledge that obesity classified using BMI-for-age percentiles has its limitations. A better indicator of obesity would be identifying abnormal or excessive fat accumulation with measurements of body composition. The possibility of higher muscle mass, especially in athletes, could be misleading when BMI is used as the only criterion for determining obesity. However, measurements of percent body fat are not as readily available and difficult to collect in population-based studies because of the additional time and equipment necessary. Studies in athletes have reported BMI tends to overestimate fatness in adults 12 and children.13,14 In adolescent athletes ages 11 to 19 years, obesity was found in 13.1% of the adolescent athletes according to BMI compared with 6% according to percentage of body fat. 13 Hence, 62.0% of the adolescents classified as obese based on BMI were false positives. 13 In another study, 9.7% of a sample of boys who played rugby were identified as overweight based on percent body fat percentiles. 15 These studies indicate a significant proportion of young athletes are still classified as overweight or obese based on excess adiposity.
In a previous review, we emphasized the importance of discussing nutritional considerations for young athletes with obesity and highlighted the many gaps in the literature surrounding the topic. 16 The review summarized available data on carbohydrate and fat metabolism during exercise in children compared with adults and discussed the limited literature about differences in substrate metabolism due to sex, obesity, or puberty. How sex and obesity affect carbohydrate oxidation and fat oxidation remains unclear in children.16,17 In general, exogenous carbohydrate oxidation rate (mg/kg of body weight/min) during moderate intensity exercise is higher in prepubertal children compared with postpubertal children and adults.16,18 When carbohydrate is not ingested right before exercise, majority of studies have reported carbohydrate oxidation rate (mg/kg of body weight/min) increases and fat oxidation rate (mg/kg of body weight/min) decreases with puberty during moderate intensity exercise.16,19,20 Therefore, puberty may be an important factor to consider; however, developing nutritional guidelines specific to puberty could be difficult because of variability in the onset of puberty. There is substantial evidence to suggest a positive association between increased adiposity and early maturation in girls,21-23 whereas there are more conflicting views in boys. 24 Some studies have reported increased adiposity is associated with early maturation in boys, 21 while others have reported the opposite. 23
For the purposes of this review, discussing nutritional considerations in children with obesity who participate in sport, weight management will be addressed with an emphasis on increasing muscle mass and reducing fat mass, and not necessarily weight loss. Evaluation and treatment for children with obesity usually involves the assessment of both physical activity and dietary habits. 25 One method of increasing physical activity and/or fitness is through sports participation. Our focus will include considerations for optimizing muscle adaptations to training, which are beneficial for both health and athletic performance, in children with obesity. Another topic discussed is whether or not there is a need to shift nutrient guidelines to a more individual approach because nutrient requirements may vary based on a child’s level of sport participation and competition.
Energy Requirements and Macronutrient Recommendations
Energy Requirements
To optimize growth and maturation in children, it is important to ensure that appropriate nutrients are available from the diet. In children with obesity, there may be additional caution to avoid excessive energy intake. Estimating energy requirements for children with obesity who participate in sports can be challenging because of the variability in energy costs associated with growth and levels of physical activity. 16 When determining metabolic equivalents for different activities, body weight is assumed to be corrected for by applying a mass-specific resting metabolic rate. 26 However, compendiums of energy expenditure in youth can underestimate energy costs in heavier youth for some activities, and caution should be used in applying these energy costs independent of body weight. 27 To the best of our knowledge, compendiums of energy expenditure in children and adolescents have not included a large proportion of children with obesity.26,28-30 Therefore, their accuracy for determining energy costs in children with obesity is questionable. Given these challenges, it is recommended for children with obesity to estimate their own average energy intake and energy expenditure through their training regime with the help of their parents, clinicians, and/or coaches. To estimate average energy intake and expenditure, a food and physical activity record for at least 1 week should be completed. Next, specific goals for the child should be identified. Any adjustments to dietary intake should be made with professional guidance and during a time when the child’s weight is stable, so that improvements can be more easily monitored. As mentioned above, this review will focus on optimizing muscle adaptations to exercise. An understanding of the macronutrient composition of diets and their influence on health and training adaptations can help with optimizing muscle growth and strength, which are usually advantageous for athletic performance. Recommendations are provided below using available evidence-based studies to date; however, it is unfortunate the research in children is still very scarce.
Protein Recommendations
Information about protein turnover after resistance training in children was summarized in a previous review article. 16 Based on the limited studies available, it was concluded that there was inadequate support to suggest increased protein consumption for children with obesity in sport compared with children with normal weight. However, there is evidence to suggest that protein intake beyond the recommended dietary allowance (RDA) has implications for weight management and optimizing adaptations to training. In general, adaptations to training may include optimizing the musculoskeletal, cardiovascular, and immune system, 31 as well as optimizing physiological function. 32 However, depending on athlete-specific outcomes, adaptations to training may vary from accrual of lean mass such as with resistance training or balancing the loss of leucine with endurance exercise. 32 The RDA is the estimated average requirement plus 2 standard deviations, which includes nutrient requirements for 97.5% of the population of healthy individuals for a particular group based on age and sex. 33 Most of the data in support of protein intake beyond the RDA are obtained from adult studies. If protein intake beyond the RDA can help optimize health and training adaptations, we need to better understand how much should be recommended for children with obesity.
The RDA for protein is 0.95 g/kg/day for boys and girls ages 4 to 13 years and 0.85 g/kg/day for boys and girls ages 14 to 18 years. 34 As previously described, 16 past studies suggested an RDA of 0.85 to 0.95 g/kg/day was inadequate for positive protein balance in both healthy nonactive and active children.35,36 Boisseau and colleagues 36 recommended an RDA of 1.4 g/kg/day for active children (mean age = 13.8 ± 0.1 years). There has not been any published data to determine how effective this quantity of protein intake influences growth or training adaptations in children with obesity. However, one study showed a high protein (1.5-2.0 g/kg/day), very low calorie diet over 10 weeks led to significant weight loss and improved aerobic fitness (VO2max) relative to body weight, but not absolute VO2max in children ages 7 to 14 years. 37 This suggests that improvements in VO2max were mainly attributed to weight loss, but how this could improve athletic performance in a child with obesity was not examined. There was no control group for comparison. Based on increasing evidence in adults, high protein intake during periods of energy restriction can help with retaining fat free mass,38-40 which would suggest benefits for athletic performance related to strength if this were also the case in children.
Maintaining a positive protein balance as much as possible is thought to be optimal for growth. Based on adult research, to strive for a positive protein balance as often as possible, the common suggestion is to distribute protein intake equally throughout the day at each meal and during recovery after exercise training. 41 Studies in nonoverweight children support the benefits of postexercise protein intake42,43; however, future research on the timing of protein intake throughout the day in children is needed. Consuming protein equally throughout the day is thought to promote anabolism because the ingestion of essential amino acids (eg, leucine) stimulates muscle protein synthesis. 32 Ingested protein after exercise also slows muscle protein breakdown rates, leading to net protein accretion in recovery after sport participation or training.32,44 Because protein synthesis cannot be stimulated beyond a certain capacity and excess amino acids are not efficiently used or stored, the consumption of all of one’s daily recommended protein in one meal is an ineffective strategy. Furthermore, evidence from studies in adults,45,46 as well as adolescents (mean age = 19 ± 1 years),46-48 with overweight or obesity support positive effects of protein on appetite control, satiety, and weight management, which suggests equal protein distribution throughout the day could be beneficial.
One strategy to balance protein intake is to aim for a high-quality protein breakfast, because it is often a meal that is skipped or rushed, and is usually the meal with the lowest protein consumption compared with other meals. 49 In adolescents (mean age = 19 ± 1 years), who normally skipped breakfast, a high protein breakfast with 35 g of protein led to less gains in fat mass and daily intake over 12 weeks compared with a control group who continued to skip breakfast. 47 In contrast, a breakfast with 13 g of protein, which was considered a normal protein breakfast, did not prevent increased fat mass or daily intake compared with the control group. 47 In general, studies have reported that adolescents who skip breakfast have greater body fat content and cardiovascular risk factors.50-53 Therefore, ensuring children and adolescents do not skip breakfast and consume a high-protein breakfast is one modifiable lifestyle factor to consider that could assist with satiety and weight maintenance. Leidy and colleagues 46 concluded in their review that higher protein diets with 1.2 to 1.6 g/kg/day of protein, and meal specific protein intakes of 25 to 30 g/meal, showed improved appetite control shown by increased satiety accompanied by increases in PYY (peptide YY) concentrations, as well as improved weight management and cardiometabolic risk factors. The recommendation was based on some data collected in children, but were not limited to studies in children.
A consideration for maintaining positive protein balance and optimizing training adaptations in overnight recovery is to add presleep protein ingestion, because negative protein balance is likely to occur overnight. It is important to note that this has not been tested in children and the support has only been shown in adult studies so far.54-56 In adults, recreational athletes who completed resistance exercise in the evening and ingested a 20 g recovery drink were unable to maintain elevated muscle protein synthesis during overnight recovery. 57 Rather, data from Res and colleagues suggest that at least 40 g of protein or ~0.55 g/kg before sleep is necessary for an increase in muscle protein synthesis overnight.54,56 Without supplementation, meeting 40 g of protein intake before bed would require consuming a fairly large portion of food. Examples of protein sources to provide 40 g of presleep protein include 7 eggs, 5 cups of low-fat milk, 2 chicken breasts (176 g), or 2 scoops of protein concentrate in 300 mL of low-fat milk. 56 Thus, special attention should be given to how this quantity of protein would increase daily intake, especially in children with obesity. More research in children is necessary before justifiable recommendations for presleep protein can be provided. One study in children with normal weight reported a high protein beverage (~0.3 g/kg) helped maintain positive whole body protein balance for 24 hours after exercise. 42 Therefore, this could be effective for presleep protein intake until there is evidence to suggest a greater amount for children. Neither observational studies nor longitudinal studies have examined the effect of presleep protein on weight management in children with obesity.
The quality of protein ingested is also important. The majority of studies have included the use of high-quality, animal-based proteins, such as whey protein. The effect of animal-based proteins versus plant-based proteins in children is not well understood. Based on the US Department of Agriculture National Nutrient Database for Standard Reference (ndb.nal.usda.gov/), it seems that lean animal-based proteins allow for the greatest protein content with the lowest caloric intake compared with other sources of protein. 31 Therefore, in the absence of dietary restrictions, lean animal-based proteins may be preferred for children with obesity who would also like to focus on weight management. Skim milk is a good source of protein after exercise and helps maintain whole body protein balance in children with normal weight. 42 More research is required to compare the benefits of different types of protein in children with obesity.
Carbohydrate Recommendations
The RDA for carbohydrate in adults and children is 130 g/day, which is based on the minimum amount of glucose used by the brain. 34 This value does not consider replenishment of glycogen stores with exercise. Average carbohydrate intake summarized from a few studies was ~200 to 300 g/day in children with normal weight and up to 500 g/day in young athletes, with ages ranging from 9 to 20 years in the studies.16,58,59 The consumption of more complex carbohydrate sources, such as whole grains, and less simple sugars are recommended. 60 The accepted macronutrient distribution range (AMDR) for carbohydrate intake in children is 45% to 65% of energy. 34 As previously discussed, 16 data do not exist to suggest different carbohydrate recommendations for children with obesity compared with children without obesity.
When considering how carbohydrate intake may help optimize training adaptations at the level of the muscle, the primary concern is replenishing glycogen stores so that energy is available to sustain volume of training, and delay fatigue. In the 2014 Sports Dietitians Australia Position Statement, it was highlighted that amended guidelines for carbohydrate were moving away from a “one size fits all” approach, and that individual carbohydrate needs to meet fuel costs of an athlete’s training were recommended. 61 General guidelines that are scaled to body weight are available (see Table 1); however, they were developed based on adult research, 62 and age and size should be included in future developments for guidelines. Table 1 provides carbohydrate guidelines for immediately after exercise (0-4 hours), daily recovery based on intensity and volume of training, as well as recommendations for during sport participation based on duration. Since general carbohydrate recommendations were developed in adults, their application to children participating in sport should consider differences in fuel utilization between adults and children, which we have previously summarized. 16 Additionally, there is not enough empirical evidence to suggest children with obesity require different carbohydrate guidelines from children with normal weight 16 ; however, it is possible for carbohydrate utilization to vary with obesity and exercise training.63,64 Hence, individual monitoring of carbohydrate utilization and intake should be considered.
Carbohydrate Guidelines Based on Adult Studies a .
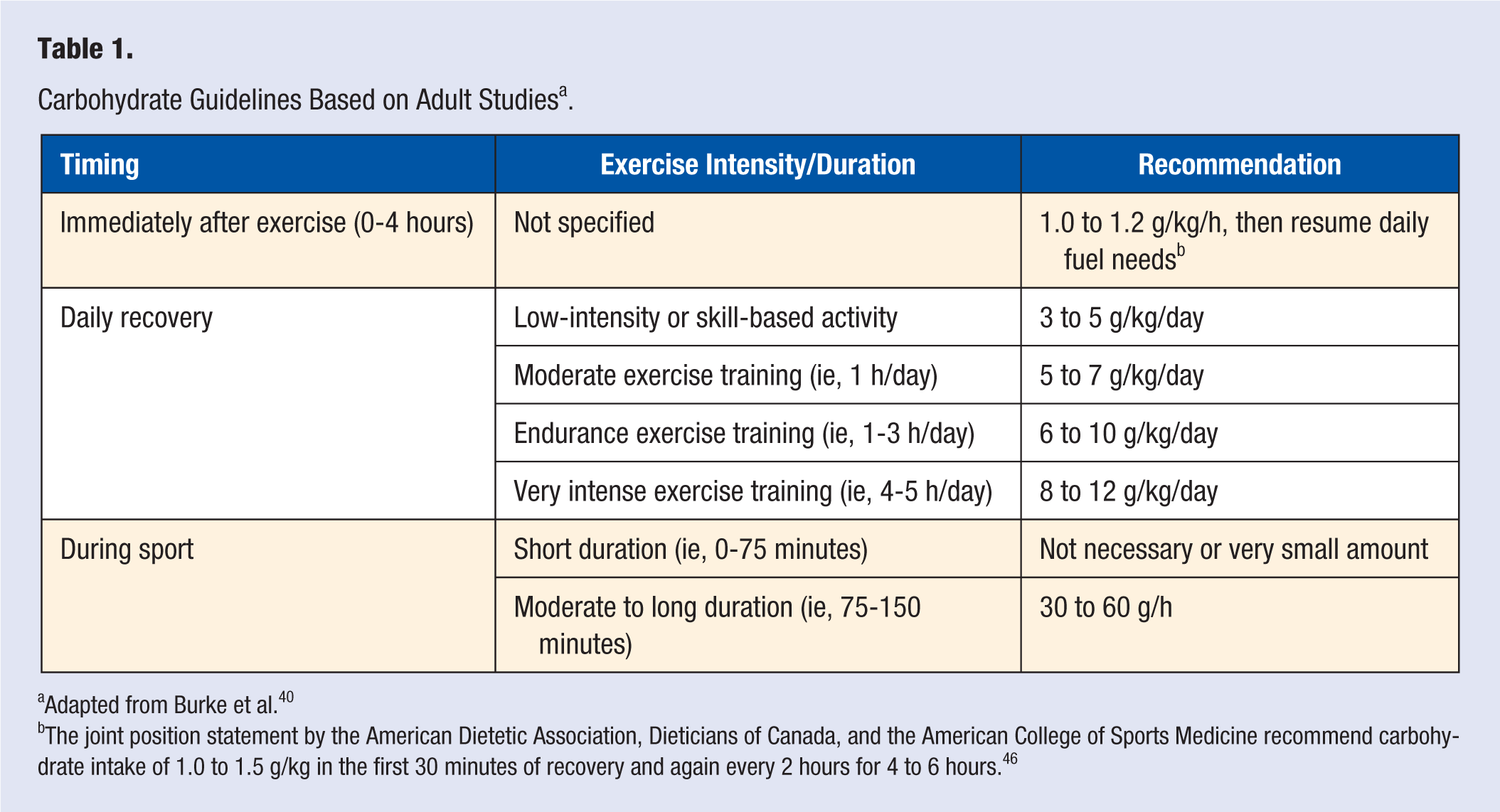
Adapted from Burke et al. 40
The joint position statement by the American Dietetic Association, Dieticians of Canada, and the American College of Sports Medicine recommend carbohydrate intake of 1.0 to 1.5 g/kg in the first 30 minutes of recovery and again every 2 hours for 4 to 6 hours. 46
Dietary Fat Recommendations
An RDA for total fat intake does not exist, because a level of fat intake that helps prevent metabolic disease is not supported by any data. The AMDR for dietary fat in children ages 4 to 18 years old is 25% to 35%. 34 Special nutrient considerations for fat intake are not necessary for children with obesity who participate in sport. 16 General dietary fat recommendations for health include increasing essential fatty acid consumption and decreasing cholesterol and saturated fats in the diet.16,34,65 No evidence to date indicates a role of dietary fat for optimizing training adaptations.
There have been some discussions about low carbohydrate (<25% energy), high fat (>60% energy) (LCHF) diets within the sports performance world in adults. 66 However, there remains insufficient data to support the use of adaptations to fat utilization for optimizing training and performance. 66 In addition, how LCHF diets influence sport performance in children is unknown. However, some studies suggest an LCHF diet in children ages 12 to 18 years could aid in reducing risk factors associated with type 2 diabetes, including hyperglycemia and insulin resistance.67,68 Nevertheless, further research on macronutrient contribution of diets in children is warranted, because recommending an LCHF diet would be in contrast to guidelines for type 2 diabetes prevention in adults, which includes a low-fat, high-carbohydrate diet.68,69
General Nutrient Requirements Versus Individual Training Needs
To date, there has not been a lot of discussion about whether general nutrient guidelines are sufficient for children or if considerations for individual training (ie, level of competition) should be recommended. For example, should children with obesity be provided the same recommendations for nutrient intake despite different levels of sport participation and competitions? Sport participation can vary from recreational activity 1 or 2 times per week to practices and competitions almost every day. At this time, there is a paucity of information on how effective general guidelines for nutrient intake for young athletes are. However, there also has not been a clear method described to determine individual nutrient needs based on type and intensity of athletic training. For treatment of childhood obesity, it is encouraged that healthy behaviors and interventions are tailored to the individual child and family. 70 Therefore, nutrient considerations for children with obesity who participate in sport should also probably shift toward an individual approach.
A good starting point is to look at general estimated energy requirements determined for children based on sex, age, and physical activity level.16,34 Because there can be limitations with applying general energy requirements, monitoring changes in weight is advised. For weight management in children, a step or staged approach is recommended, which is described in detail by Spear et al. 70 The stages include (1) prevention plus (healthy lifestyle changes), (2) structured weight management, (3) comprehensive multidisciplinary intervention, and (4) tertiary care intervention. 70 Weight recommendations according to age and BMI-for-age percentile are summarized in Table 2. Usually, children with obesity who attend weight management programs are not recommended to aim for weight loss but to maintain their weight as they grow. 70 The weight recommendations described in Table 2 for children between the 85th and 99th BMI-for age percentile includes weight maintenance until BMI-for-age is <85th percentile or slowing of weight gain, but never weight loss more than 2 lb/week. Based on individual weight goals, the child, parents, clinicians, and/or coaches should decide if a moderate energy deficit is necessary. Monitoring changes in weight over 3 to 6 months should provide an indication of whether dietary modifications are helping meet the child’s weight maintenance or gradual weight loss goals.
Weight Recommendations Based on Age and BMI-for-Age Percentile a .
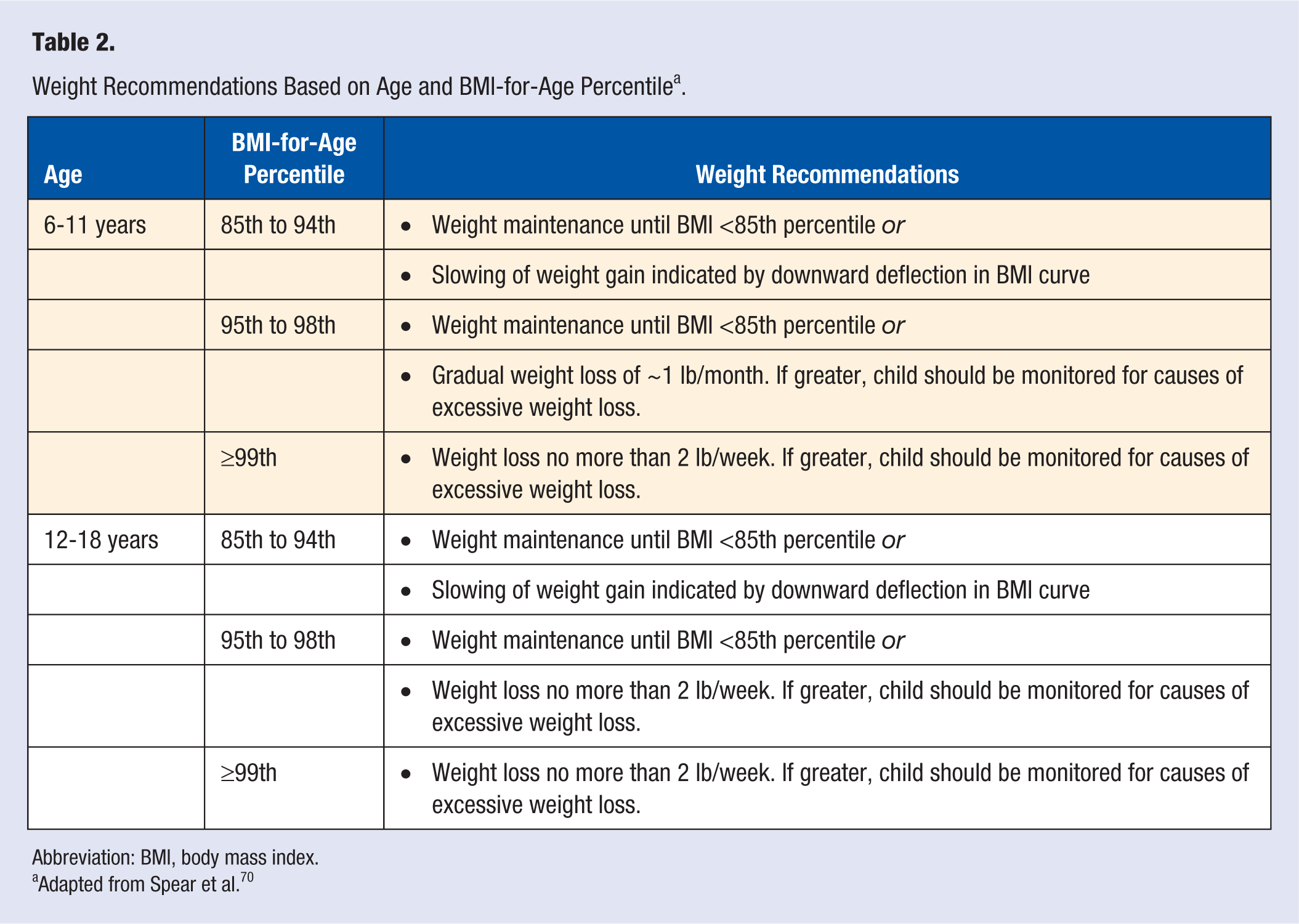
Abbreviation: BMI, body mass index.
Adapted from Spear et al. 70
Next, macronutrient breakdown of caloric intake can be estimated through diet records. General AMDR for protein (10% to 30%), carbohydrates (45% to 65%), and fat (25% to 35%) can be used for comparison. 34 As described above, protein intake balanced throughout the day and during postexercise recovery is recommended. Protein intake can be determined using general guidelines because it is difficult to determine whole body protein balance outside of the laboratory and a feasible field based test is not available for athletes. Protein intake after exercise and presleep protein may include ~0.3 g/kg of body weight, because greater amounts of protein intake have not yet been confirmed in children. Carbohydrate intake during postexercise recovery is dependent on the child’s individual training regime and the intensity and duration of sessions. Unique recommendations for carbohydrate intake for children with obesity compared to children with normal weight are not necessary.
Summary
Nutrient recommendations for children with obesity who participate in sport have not been clearly delineated in the literature. Protein intake seems to be the macronutrient that could have the largest influence on health, weight maintenance, and training adaptations. Based on results reported by Boisseau and colleagues 36 in active children with normal weight and Leidy and colleagues 46 in children with obesity, higher protein intakes ranging from 1.2 to 1.6 g/kg/day would be beneficial. More specifically, protein intakes of 25 to 30 g/meal 46 and 0.3 g/kg during postexercise recovery are recommended. 42 However, the protein recommendation for postexercise recovery was not studied in children with obesity and warrants confirmation. Meeting individual carbohydrate requirements is also important. The minimum requirement of carbohydrate independent of training is ~130 g/day, but young athletes may require 200 to 500 g/day depending on their individual needs for sport training and competitions. A small snack with a large protein content and some complex carbohydrates could help maintain positive protein balance and replenish glycogen stores overnight, but the optimal amount for children with obesity is unknown and requires future examination. In regard to fat intake, there is no convincing literature to suggest additional modifications to fat consumption that would improve training adaptations. Moving forward, longitudinal studies are needed to confirm the effect of these macronutrient recommendations on health and training adaptations in active children with obesity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LC was supported by a CIHR doctoral award (Frederick Banting and Charles Best Canada Graduates Scholarship) and the 2014 Marco Cabrera Student Research Award provided by the North American Society of Pediatric Exercise Medicine. BWT holds a Canada Research Chair in Child Health & Exercise Medicine.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.