
Abstract
Objective. To evaluate the feasibility of disease-specific, community-based supervised exercise programs (CSEPs) to improve biometric and functional outcomes among persons with a variety of chronic medical conditions. Design. Feasibility, cohort study. Subjects were recruited through community placed flyers and provider offices. Exercise programs consisted of aerobic and resistance training that adhered to American College of Sports Medicine guidelines. A Wilcoxon signed rank test was used to assess program outcomes. Setting. Ten, community-based, medical fitness centers. Subjects. A total of 382 total participants. The number of participants in each CSEP ranged from 38 to 119. Individuals were 18 years of age or older and treated for various chronic medical conditions. Results. Varied by cohort, but generally consisted of (a) favorable changes in body composition ( P < .05), (b) significant improvements in submaximal exercise tolerance and functional outcome measures ( P < .05), and (3) significant increase in self-reported exercise behaviors ( P < .05). Conclusion. CSEPs improve outcomes in patients with chronic medical conditions and may be relevant within the continuum of care in outpatient rehabilitation medicine, particularly among bundled or value-based payment models. Further research is needed to evaluate outcomes from CSEPs versus controls.
‘. . . it is imperative that community-based models be explored, which have the potential to improve long-term patient outcomes and engagement.’
Population Health Management, Value-Based Care, and Outpatient Rehabilitation Medicine
As health care payment and delivery models continue to surface and evolve in the United States, it is now universally accepted that they are aligned with the “Triple Aim” paradigm articulated by Donald Berwick and others in 2008. 1 The primary tenants of the Triple Aim: (1) improving the individual experience of care, (2) improving the health of populations, and (3) reducing the per capita cost of care, have become the mantra and guiding forces behind most efforts to innovate in health care over the past decade. Implicit within this model is the belief that it is no longer appropriate or even “good medicine” for providers and health care systems to principally focus on growing volumes and market share. To the contrary, Berwick has challenged the health care community to envision a future where the delivery of care is patient centric, population focused, and engineered to both quantify and reward care which places a premium on optimizing value for both the patient and payer. 1
At a time when health care systems are realigning and universally moving to embrace the core elements of population health management (PHM) and value-based care within the context of the Triple Aim, they frequently struggle to identify and incorporate models of care for the chronically ill or those persons whom are at risk for chronic medical conditions (CMCs).1-3 Though several models for chronic care delivery have been defined and advocated to improve health outcomes, including the chronic care model, the patient-centered medical home (PCMH), accountable care organizations (ACOs), and community-centered health homes, most have reported mixed findings and have yet to demonstrate a systematic impact on the value of care or the overall health of a defined population.1-3 Equally concerning is the fact that while these models have primarily focused on the delivery and coordination of care at an acute or subacute level, they have done little to affect the daily health habits and behaviors of patients or populations that are known to contribute to disease risk, occurrence, and costs. 3
Professionals who make up the various disciplines of outpatient rehabilitation medicine are in a unique position to favorably affect the “value proposition” of health care, in large part due to the magnitude of patients they treat with CMCs. It is estimated that expenditures for rehabilitation services will exceed $35 billion by 2019, with 90% of this care being delivered in an outpatient setting. 4 Each year, approximately 28% of outpatient rehabilitation visits occur among adults older than 65 years, two-thirds of whom present with 2 or more CMCs, such as chronic pain, Parkinson’s, cancer, diabetes, cardiovascular disease and obesity. 5 As adherence to exercise therapies prescribed in outpatient rehabilitation settings continues to be a challenge, 6 it is imperative that community-based models be explored, which have the potential to improve long-term patient outcomes and engagement. Identifying appropriate models of rehabilitation medicine where the continuum of care can be extended into the community may be especially important in instances where care bundles are employed (ie, total joint replacement, cardiac surgery) or where providers and health care systems share in financial risk for achieving quality metrics. 7
Design and Overview of Community-Based, Supervised Exercise Programs
The rising spread of physical inactivity around the world has been well documented and is known to contribute to the occurrence of multiple CMCs, premature death, disability, and has a sizeable, adverse impact on the cost of health care. 8 A recent global analysis of the economic burden of physical inactivity reported that in 2013, $53.8 billion was spent on health care worldwide as a direct result of physical inactivity and physical inactivity–related deaths contributed to $13.7 billion lost in productivity, globally. All told, the authors concluded that worldwide, physical inactivity contributes to 1% to 4% of the total annual, health care spend. 8
The use of exercise and behavior change programs in the prevention and management of persons with CMCs has become the standard of care among most modernized health care settings. Decades ago, exercise was introduced as a therapy to help patients recovering from heart disease. 9 As the evidence has evolved, regular exercise is now being advocated as a core treatment strategy among patients with vascular disease, pulmonary disease, cancer, metabolic disorders, osteoporosis, chronic pain, Parkinson’s disease, and even dementia. 10
The primary aim of this study was to evaluate the feasibility of disease-specific, community-based supervised exercise programs (CSEPs) to improve biometric and functional outcomes among persons with a variety of CMCs. A secondary aim was to demonstrate a model through which CSEPs targeted to individuals with CMCs, could be integrated within the continuum of care of outpatient rehabilitation medicine. This study was reviewed and approved by a university institutional review board.
Methods
Program Design and Facilities
Working in collaboration with various health care systems throughout the states of New Jersey and Pennsylvania, small group, CSEPs were created to successfully transition patients with CMCs from outpatient rehabilitation into a community-based fitness setting. The process for development of the CSEPs is described in Figure 1. In each instance, the programs were reviewed and vetted by clinical and executive leadership affiliated with each health care system prior to implementation. The hospital-based fitness centers were built in collaboration with health care systems who had strategically committed to develop and integrate medical fitness centers within their continuum of care. The performance sites included 10, hospital-based fitness centers, collectively serving approximately 54 000 members throughout the Northeastern United States. The average age of the 54 000 members was 51 years, with 15% of members being older than 65 years.
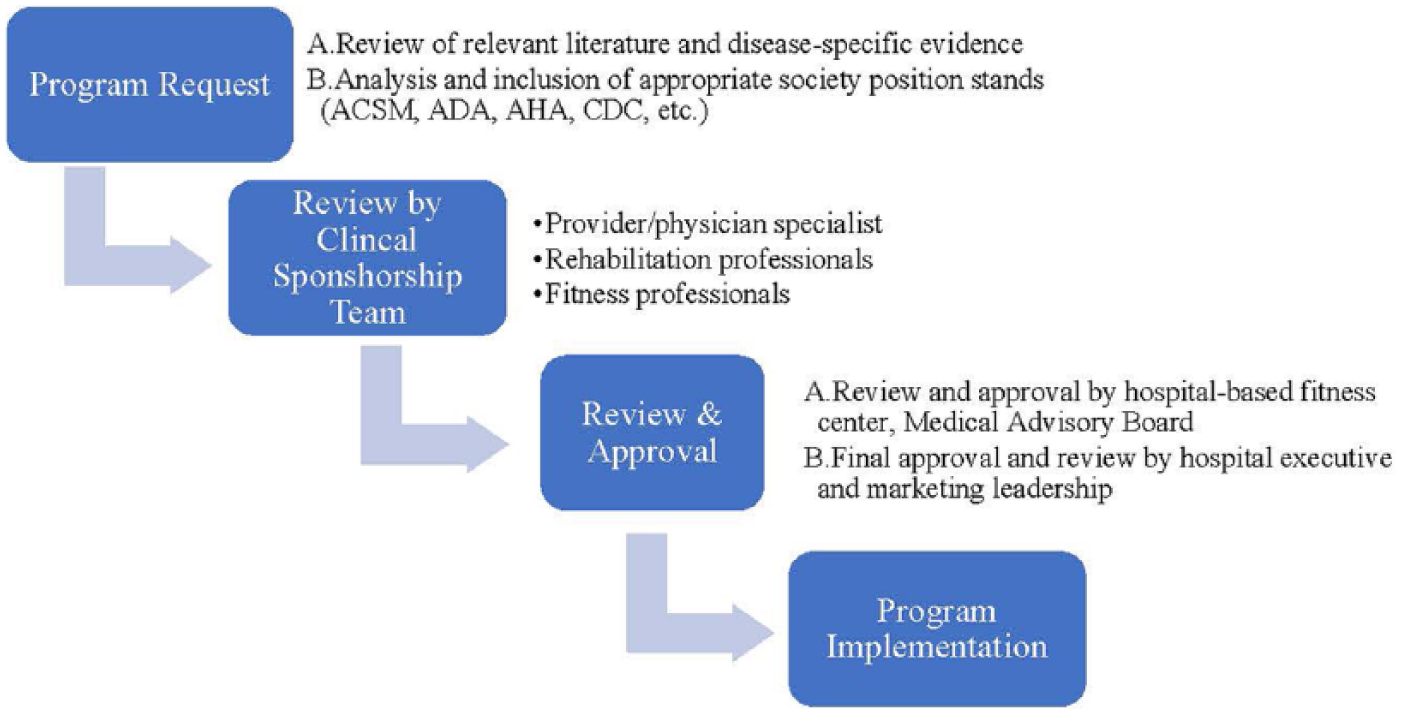
Community-based, supervised exercise program (CSEP) development and approval process.
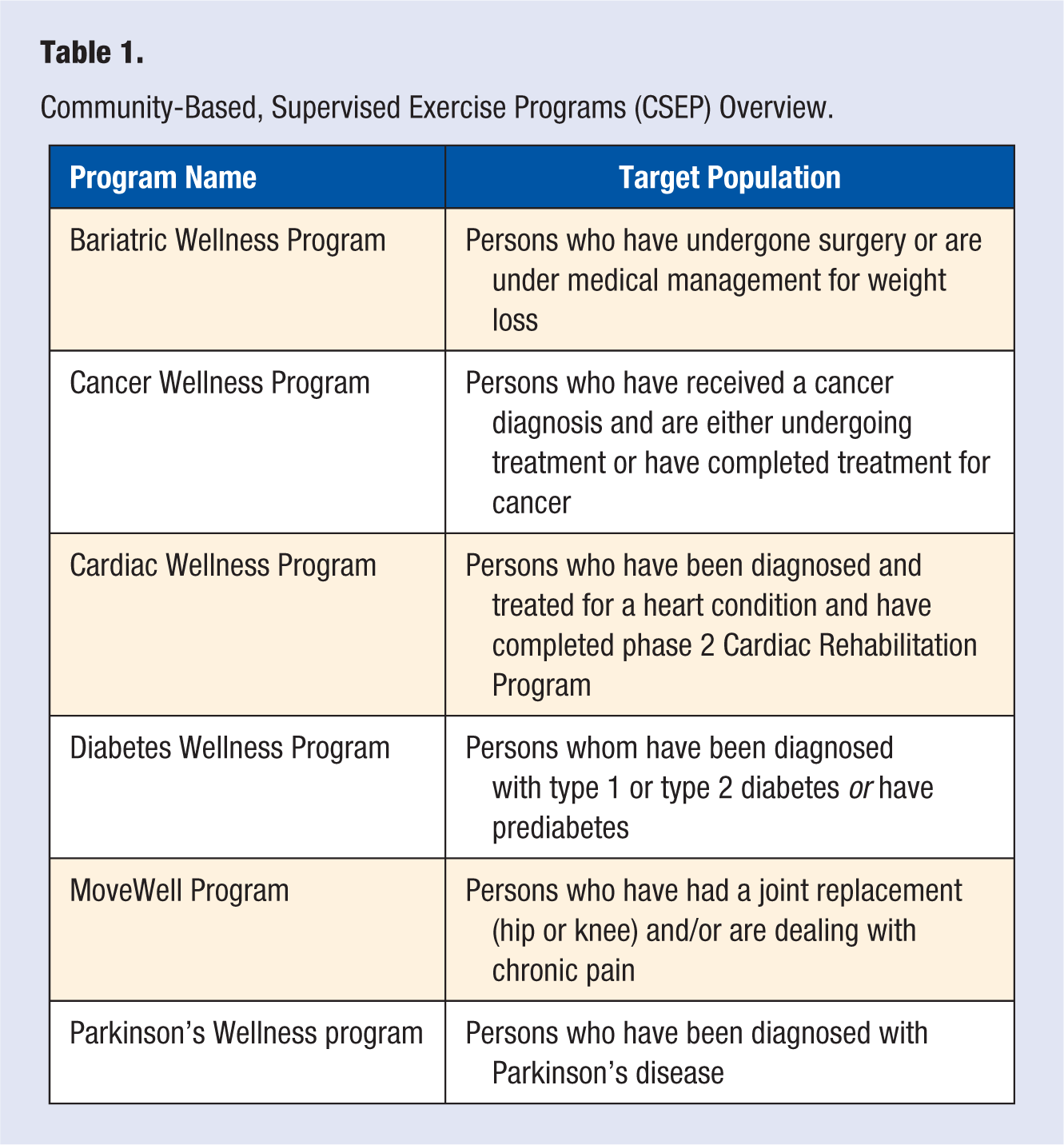
The bundled cost to the participant for each CSEP program was $199, which included 16 visits over the standard 2-month program. This equates to approximately $12.43 per visit. There were no direct health care costs affiliated with the delivery of any CSEP. The CSEPs typically met twice a week and used a small-group training (4-6 participants/trainer) format designed to optimize personal attention, socialization, and participant results. Oversight for all CSEPs was accomplished through the Medical Advisory Board (MAB) affiliated with each center and hospital partner. The MAB was ultimately responsible for reviewing and approving the participant enrollment process, exercise protocols, outcome measures, and marketing materials and strategies for each CSEP. In some instances, the MAB modified certain aspects of the programs, including program names, medical release forms, marketing materials, referral, and enrollment processes. The CSEPs were created for the following populations: bariatric, cardiac, cancer, diabetes, Parkinson’s, and chronic pain/joint replacement (named MoveWell) (Table 1). These chronic medical conditions were specifically chosen because they aligned with the clinical growth strategies of each hospital partner and supported the findings of their community needs assessment.
Community-Based, Supervised Exercise Programs (CSEP) Overview.
The CSEPs followed established exercise guidelines from the American College of Sports Medicine. 10 Using ACSM guidelines, disease-specific exercise protocols were developed for each CSEP. The protocols included aerobic conditioning activities, stretching and/or dynamic warm-ups, and 8 to 10 resistance exercises; the exact exercises and progressions varied by CSEP as shown in Table 2. In addition, the CSEP exercise prescription included target heart rate (HR) ranges for aerobic conditioning and detailed, movement-specific, resistance training guidelines. Also included was specific guidance for progressing and regressing the dose of exercise required to meet the needs and capabilities of each participant. The exercise protocols detailed weekly progressions for aerobic and resistance training for the duration of the 2-month program. The specific protocols were developed in partnership with physical and occupational therapists and physicians who treated the corresponding medical condition. All exercise protocols were approved by an MAB before implementation.
Comparisons of Exercise Protocols for Cancer Wellness and Bariatric Wellness Programs.
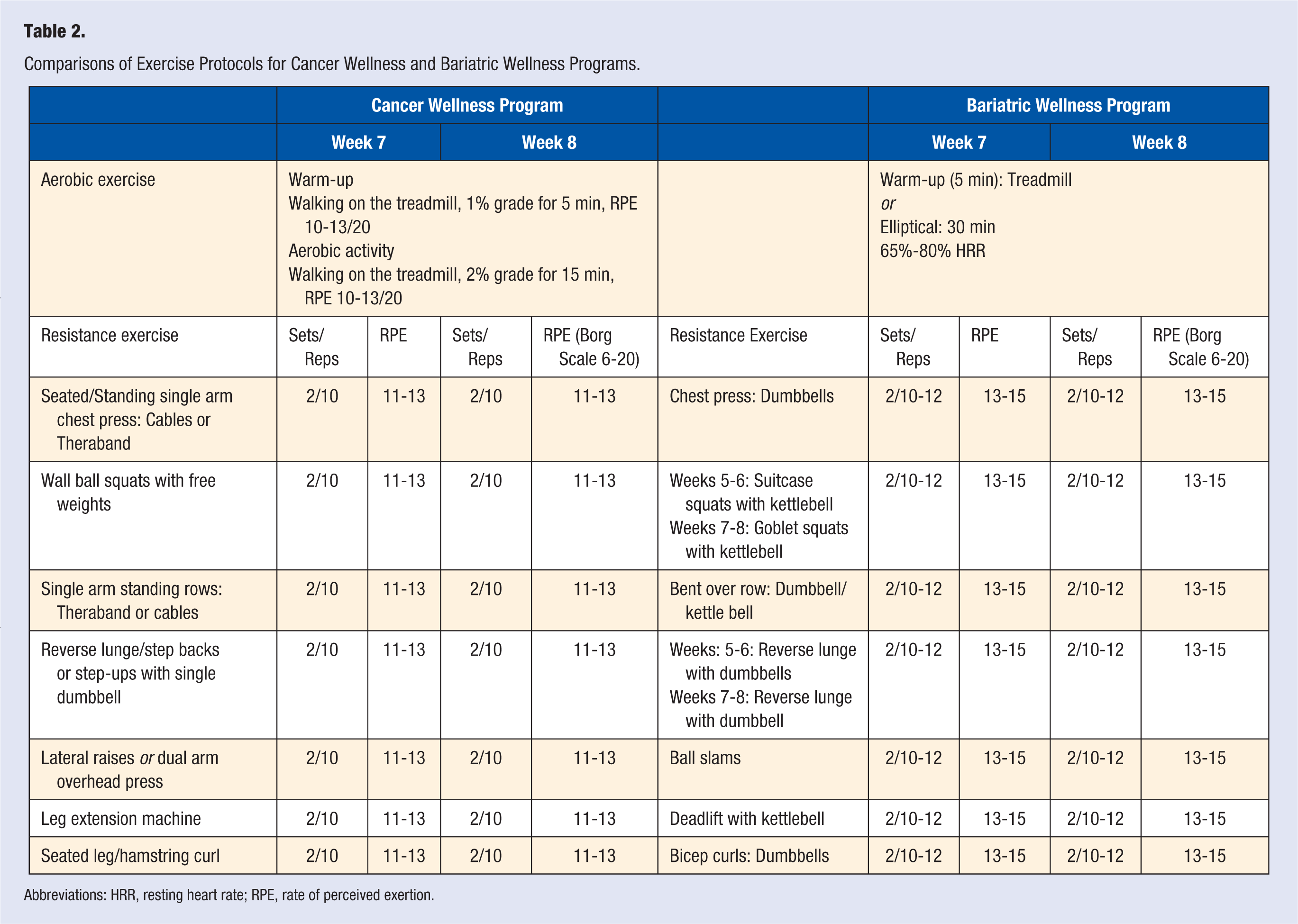
Abbreviations: HRR, resting heart rate; RPE, rate of perceived exertion.
Each exercise session was supervised by an exercise professional with a baccalaureate in exercise or health science from an accredited institution of higher learning and/or a nationally accredited, Personal Training certification. Each center was staffed with a part-time, “wellness coordinator” who was the on-site manager of the CSEP and was tasked with responding to program inquires, enrollment of participants, data management and collection, and serving as a liaison between the coordinating center’s staff and the participant’s provider. To ensure program fidelity, each trainer and wellness coordinator completed an educational class which focused on the consistent delivery of the CSEPs exercise protocol. The center’s wellness coordinator was responsible for ensuring the consistent delivery of each exercise protocol.
Before engaging in the CSEP, participants underwent a multi-step screening process. First, participants met with a licensed nurse who reviewed their medical history, and obtained biometric data and medical clearance. Participants who did not receive medical clearance were not permitted to participate in a CSEP. Next, participants were evaluated by an exercise professional who conducted several tests to ensure that no functional impairments were present which would contraindicate participation in a CSEP. If a significant functional impairment was identified by the exercise professional (Figure 2), the participant was referred to a physical therapist for a brief evaluation. Criteria for a referral to physical and occupational therapists for further evaluation consisted of:
Inability to complete 1 or more of the functional tests (5-time sit to stand, functional reach, 6-minute walk test [6MWT]) or
Scoring below the established thresholds in 2 of the 3 functional tests Timed up and go (TUG): >10.2 seconds indicates high fall risk 5-time sit to stand: >10 seconds indicates need for further assessment Functional reach: < 12.0 inches indicates fall risk
or
Passing the 3 functional tests but failing to pass a conditional, self-reported functional questionnaire and disability index (ie, Lower Extremity Functional Scale [LEFS], Western Ontario and McMaster Universities Osteoarthritis Index, Modified Oswestry Disability Questionnaire)
Scoring less than 60 on the Upper Extremity Functional Index (UEFI)questionnaire.
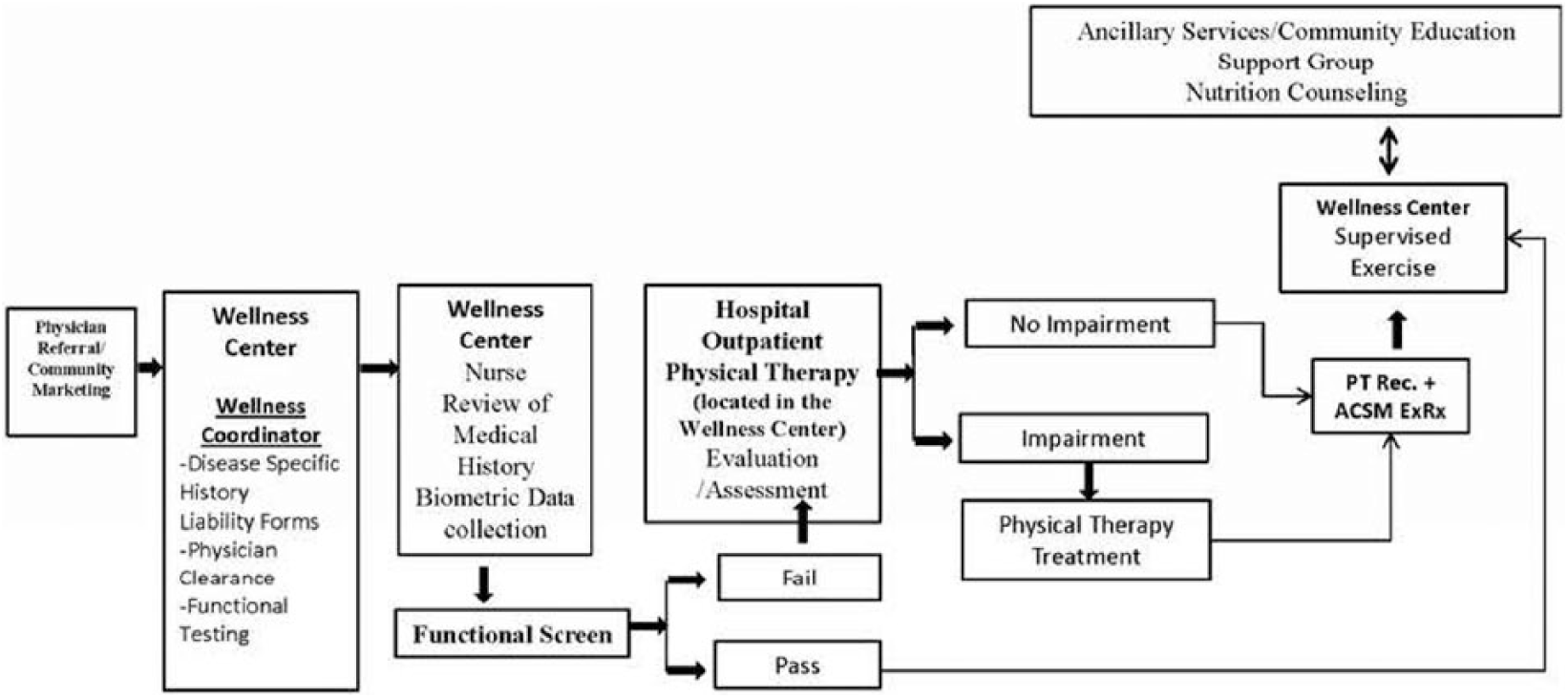
Community-based, supervised exercise program (CSEP) participant enrollment model.
The aforementioned questionnaires were used at the recommendation of rehabilitation professionals who reviewed the participant enrollment model. If the physical or occupational therapist determined that an impairment was present, the patient’s provider was contacted to facilitate a referral to physical or occupational therapy before initiating the CSEP. If no significant impairment was detected by the physical or occupational therapist, the participant was released to join the CSEP (Figure 2).
Participants and Recruitment
Participants included individuals aged 18 years or older. A description of the type of participants in each program can be seen in Table 1. Participants were recruited via flyers placed throughout the community and within provider offices located in or around the fitness center. A wellness coordinator conducting outreach would meet with local health care providers, including rehabilitation professionals, to educate them on the CSEP model. Interested participants could inquire several ways: (1) calling a dedicated phone line for the CSEPs, (2) submitting their information online through a landing (web) page dedicated to each CSEP, and (3) direct center walk-ins. In each instance, the wellness coordinator would meet or speak with the individual regarding the CSEP which most aligned with their interests and chronic medical condition. It was not uncommon for individuals to turn down the opportunity to enroll in a CSEP after they had been contacted by the wellness coordinator. Across all 10 performance sites, the CSEP enrollment rate averaged between 55% and 60% of program inquiries. The most frequent reasons given for patients declining participation were inconvenient class times, location of center, program costs, and interest in general membership. In addition, not all patients who enrolled in a CSEP were able to complete their 2-month program. Though participant adherence varied by center, program completion rates ranged from 71% to 79% across the ten performance sites.
Outcome Measures
Biometric Data
The licensed nurse collected the following biometric data: weight (lbs.), waist/hip ratio, body mass index (BMI), fat mass (lbs), lean mass (lbs), percentage body fat, systolic blood pressure, diastolic blood pressure, and heart rate (bpm). Fat mass, lean mass, and percentage body fat were determined using a Futrex-5500/XL, which uses near-infrared technology to assess body composition. After meeting with the nurse, the participant met with the exercise professional who collected the following baseline data: 6MWT distance, time to complete 5-time sit to stand (seconds), and functional reach (inches).
Patient-Reported Outcomes
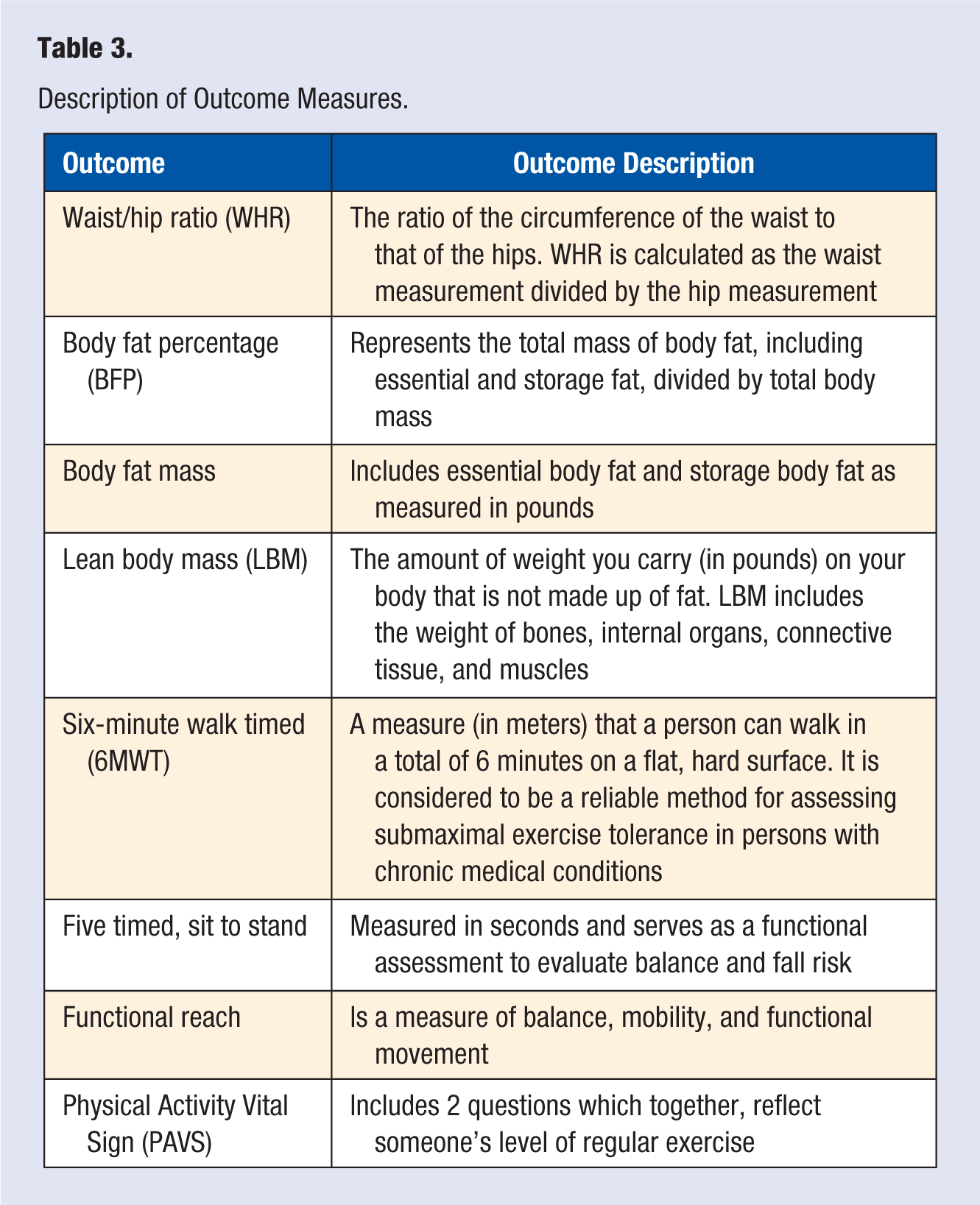
Exercise behaviors were determined by administering the Physical Activity Vital Sign (PAVS), which incorporates the following 2 questions: (1) on average, how many days per week do you engage in moderate to strenuous exercise (like a brisk walk)? and (2) on average, how many minutes do you engage in exercise at this level? The PAVS was calculated by multiplying the number of exercise days by the number of minutes of exercise per day. 11 After completing the CSEP, participants met with the nurse and exercise professional who collected identical post-program data. A detailed description of outcome measures is included in Table 3.
Description of Outcome Measures.
Data Analysis
Data included in this analysis were collected on participants in the various CSEPs from January 1, 2014 to June 1, 2017. Descriptive statistics were calculated and reported for biometric, functional, and patient-reported outcomes. For continuous outcome measures, a Wilcoxon signed rank test was used to test for statistically significant differences between baseline and the end of the wellness program, which was approximately 2 months. An alpha level of .05 was used for significance. The authors used SPSS version 24 to conduct the analysis.
Results
We report findings on a total of 382 participants who completed a CSEP in 1 of 10, hospital-based fitness centers.
Bariatric Wellness Program
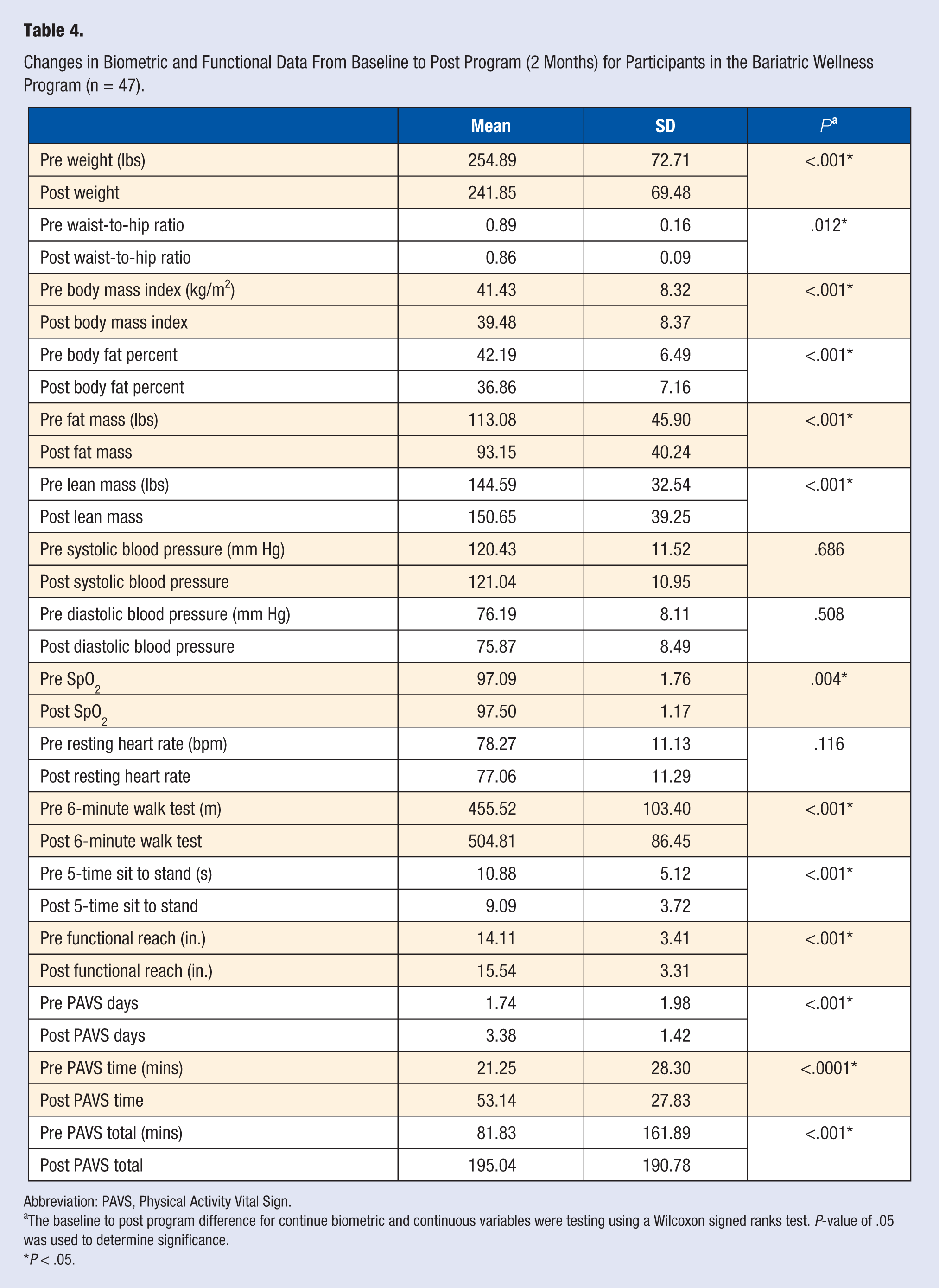
Data were obtained from 47 participants in the Bariatric Wellness Program. The average age of the participants in the Bariatric Wellness Program was 49 years (SD = 13.28). After completion of the Bariatric Wellness Program, participants demonstrated significant changes in biometric and functional data as well as the amount of accrued physical activity minutes (Table 4). Specifically, Bariatric Wellness Program participants experienced a significant reduction in weight (P < .001), waist-to-hip ratio (P =.012), BMI (P < .001), body fat percent (P < .001), and body fat mass (P < .001); participants also increased their lean muscle mass (P < .001), demonstrating significant improvements in body composition. Bariatric Wellness Program participants also significantly increased their PAVS from 81.83 minutes (SD = 161.89) to 195.04 minutes (SD = 190.78) (P < .001], which is above the threshold (150 minutes per week) recommended by the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC).
Changes in Biometric and Functional Data From Baseline to Post Program (2 Months) for Participants in the Bariatric Wellness Program (n = 47).
Abbreviation: PAVS, Physical Activity Vital Sign.
The baseline to post program difference for continue biometric and continuous variables were testing using a Wilcoxon signed ranks test. P-value of .05 was used to determine significance.
P < .05.
Cancer Wellness Program
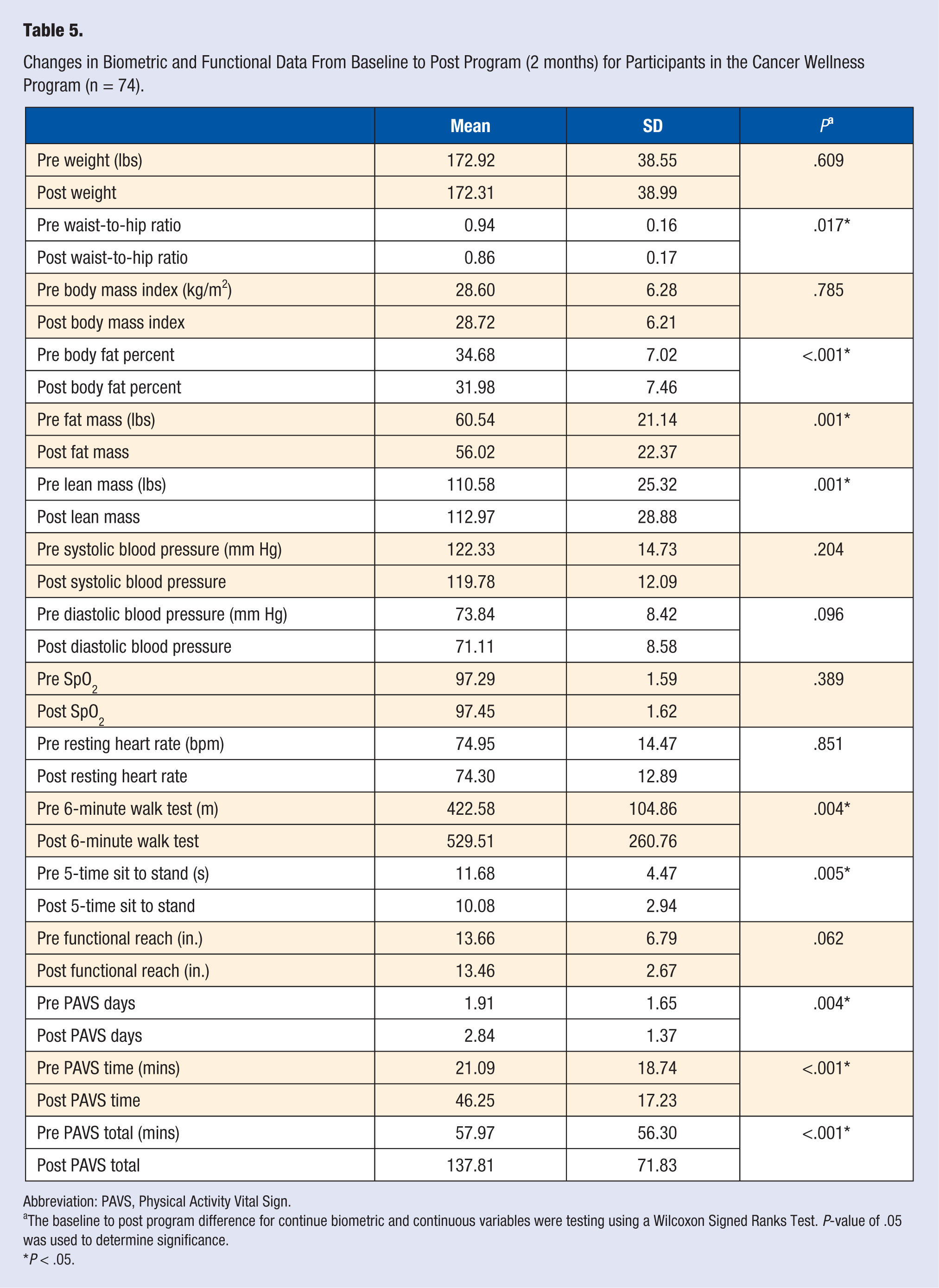
Data were obtained from 74 participants in the Cancer Wellness Program (Table 5). The average age of the participants was 63.01 years (SD = 11.55). After program completion, participants experienced a significant decrease in waist-to-hip ratio (P = .017), body fat percent (P < .001), and fat mass (P < .001); Cancer Wellness Program participants also experienced a significant increase in lean mass (P < .001) (Table 5). Functionally, Cancer Wellness Program participants significantly increased their 6MWT distance (P = .004) while decreasing their 5-time sit to stand time (P = .005); as well as significantly increasing their PAVS from 57.97 minutes (SD = 57.30) to 137.81 minutes (SD = 71.83) (P < .001).
Changes in Biometric and Functional Data From Baseline to Post Program (2 months) for Participants in the Cancer Wellness Program (n = 74).
Abbreviation: PAVS, Physical Activity Vital Sign.
The baseline to post program difference for continue biometric and continuous variables were testing using a Wilcoxon Signed Ranks Test. P-value of .05 was used to determine significance.
P < .05.
Cardiac Wellness Program
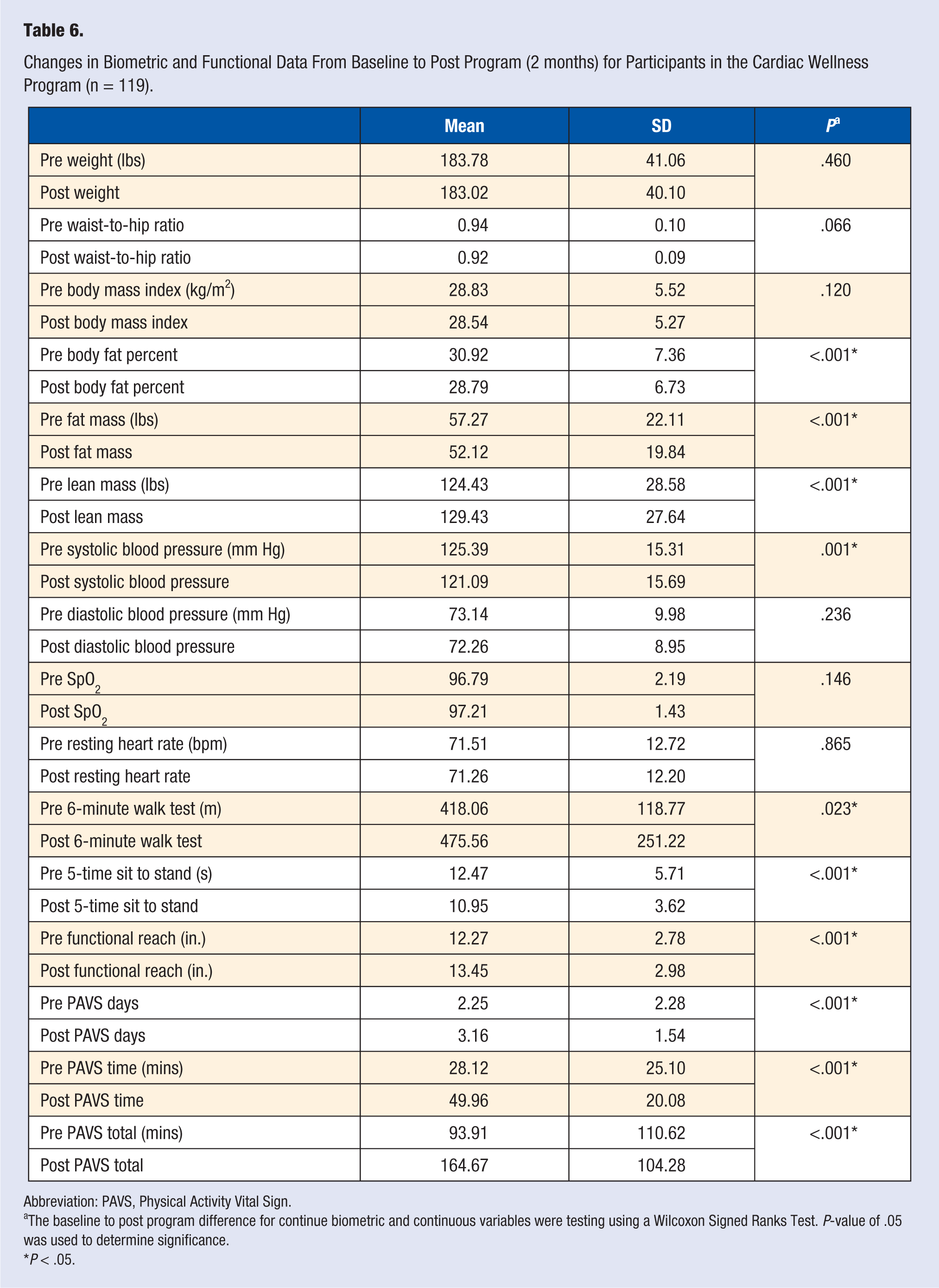
Table 6 displays the biometric and functional data collected from 119 participants in the Cardiac Wellness Program. The average age of the participants in the Cardiac Wellness Program was 71 years (SD = 9.78). In addition to significant improvements in body composition, participants in the Cardiac Wellness Program significantly lowered their systolic blood pressure from 125.39 mm Hg (SD = 15.31) to 121.09 mm Hg (SD = 15.69) (P < .001). Functionally, participants in the Cardiac Wellness Program increased their 6MWT distance (P = .023), while decreasing their 5-time sit to stand time (P < .001); participants also significantly increased their functional reach distance (P < .001) as well increased their PAVS from 93.91 minutes (SD = 110.62) to 164.67 minutes (SD = 104.28) (P < .001), which is above the 150 minutes physical activity per week that is recommended by the WHO and CDC.
Changes in Biometric and Functional Data From Baseline to Post Program (2 months) for Participants in the Cardiac Wellness Program (n = 119).
Abbreviation: PAVS, Physical Activity Vital Sign.
The baseline to post program difference for continue biometric and continuous variables were testing using a Wilcoxon Signed Ranks Test. P-value of .05 was used to determine significance.
P < .05.
Diabetes Wellness Program
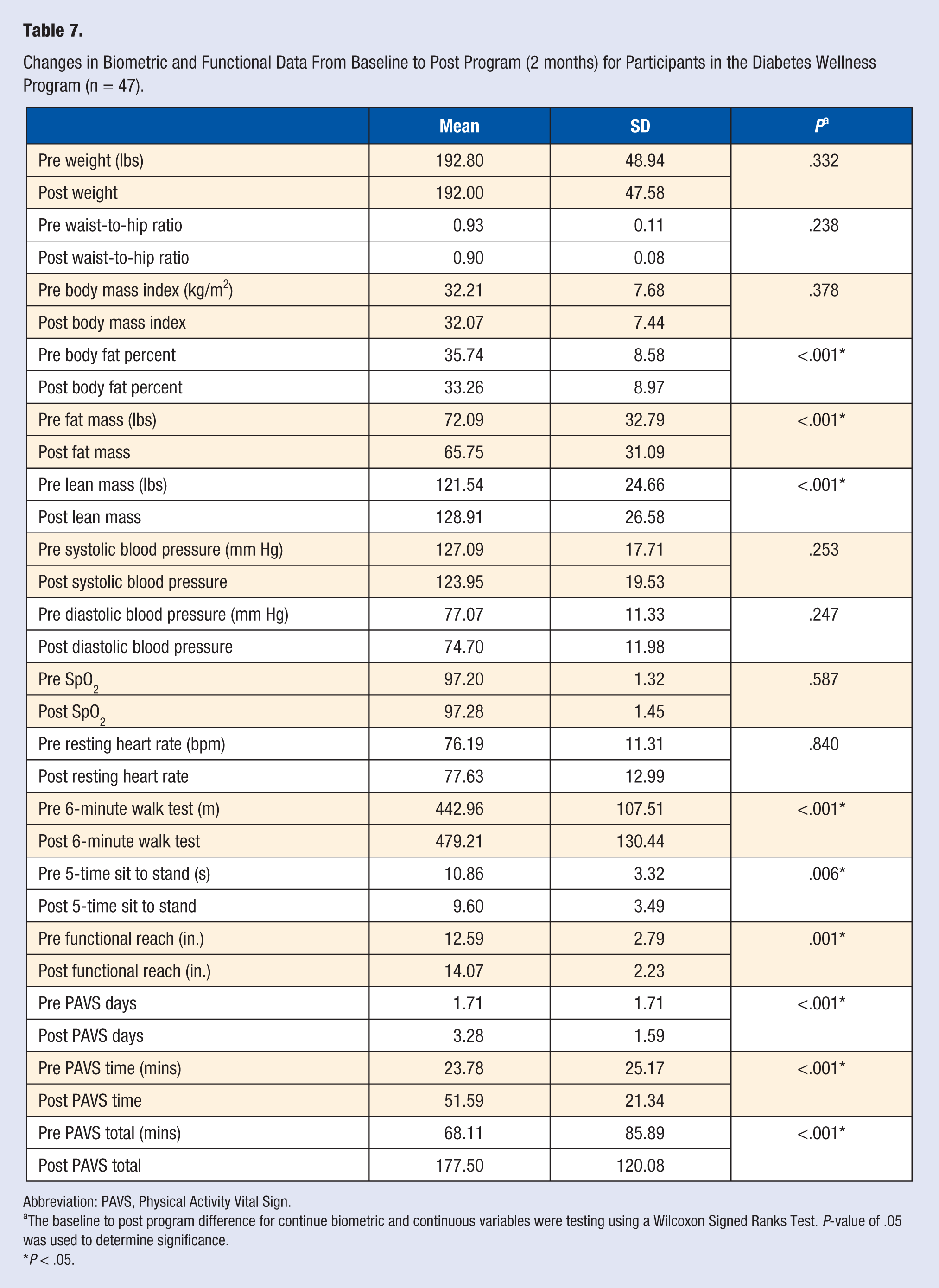
Data were collected from 47 participants in the Diabetes Wellness Program. The average age of the participants in the Diabetes Wellness Program was 60 years (SD = 10.92). After completion of the Diabetes Wellness Program, participants experienced significant changes in biometric and functional data as well as amount of accrued physical activity (Table 7). Specifically, Diabetes Wellness Program participants experienced a significant reduction in body fat percent (P < .001) and body fat mass (P < .001), while significantly increasing lean body mass (P < .001). Functionally, Diabetes Wellness Program participants increased their 6MWT distance (P < .001) and functional reach (P < .001), while decreasing their 5-time sit to stand time (P = .006). In addition, the Diabetes Wellness Program cohort significantly increased their PAVS from 68.11 minutes (SD = 85.89) to 177.5 minutes (SD = 120) (P < .001), by increasing the total number of days they engage in physical activity (P < .001) as well as the number of minutes per day (P < .001).
Changes in Biometric and Functional Data From Baseline to Post Program (2 months) for Participants in the Diabetes Wellness Program (n = 47).
Abbreviation: PAVS, Physical Activity Vital Sign.
The baseline to post program difference for continue biometric and continuous variables were testing using a Wilcoxon Signed Ranks Test. P-value of .05 was used to determine significance.
P < .05.
MoveWell Program
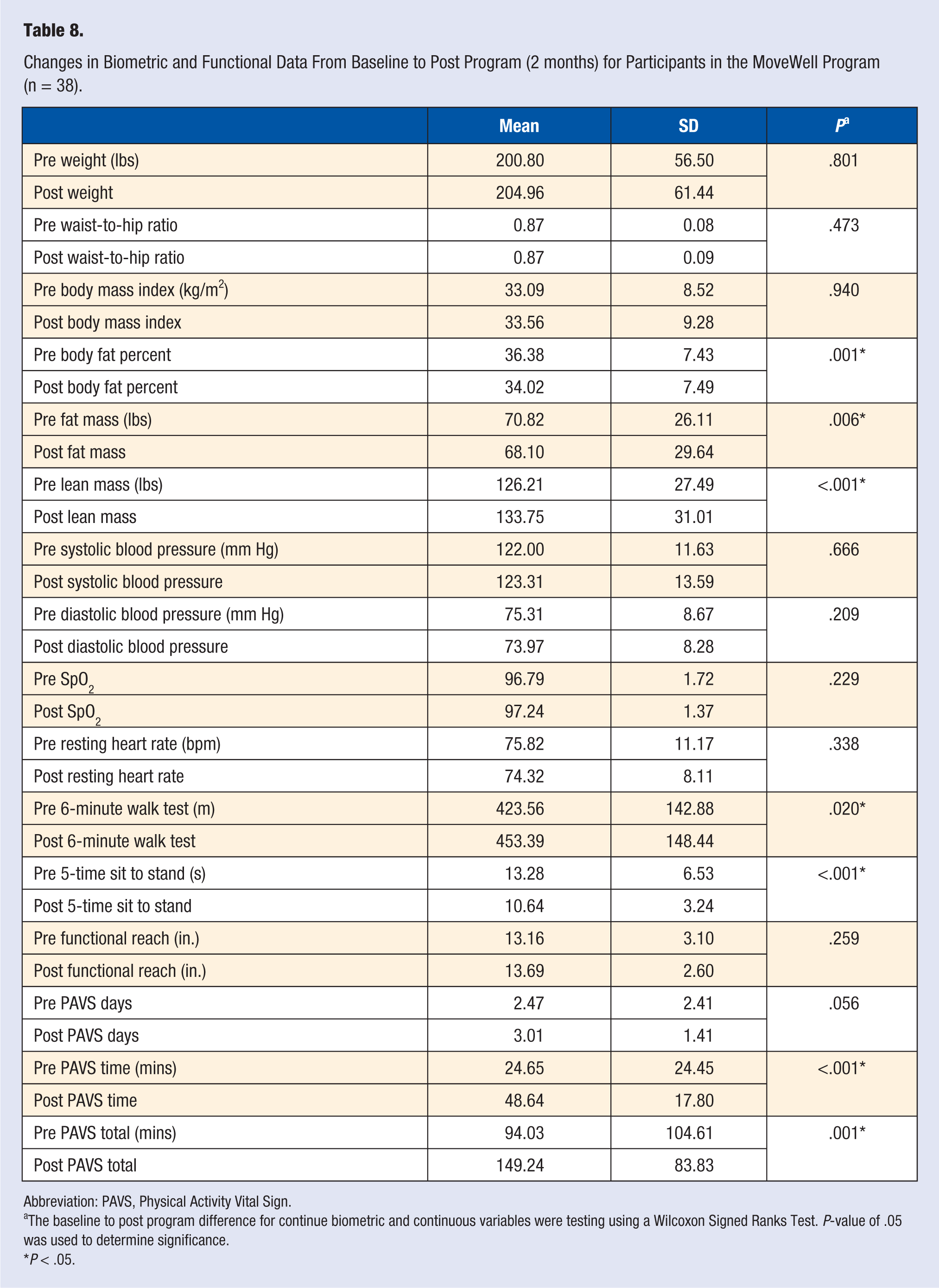
Data were collected from 38 participants in the MoveWell Program. The average age of the participants in the MoveWell Program was 61 years (SD = 12.95). After participating in the MoveWell Program, participants experienced a significant decrease in body fat percent (P = .001) and fat mass (P = .006), and an increase in lean mass (P = .001) (Table 8). Functionally, MoveWell Program participants significantly increased their 6MWT distance (P = .020) while decreasing their 5-time sit to stand time (P < .001). MoveWell Program participants also significantly increased their PAVS from 94.02 minutes (SD = 104.6) to 149.23 minutes (SD = 83.82) (P < .001). The improvement in the PAVS score for this cohort was primarily due to a significant increase in the number of physical activity minutes per exercise session (P < .001), and not days per week of physical activity (P =.056).
Changes in Biometric and Functional Data From Baseline to Post Program (2 months) for Participants in the MoveWell Program (n = 38).
Abbreviation: PAVS, Physical Activity Vital Sign.
The baseline to post program difference for continue biometric and continuous variables were testing using a Wilcoxon Signed Ranks Test. P-value of .05 was used to determine significance.
P < .05.
Parkinson’s Wellness Program
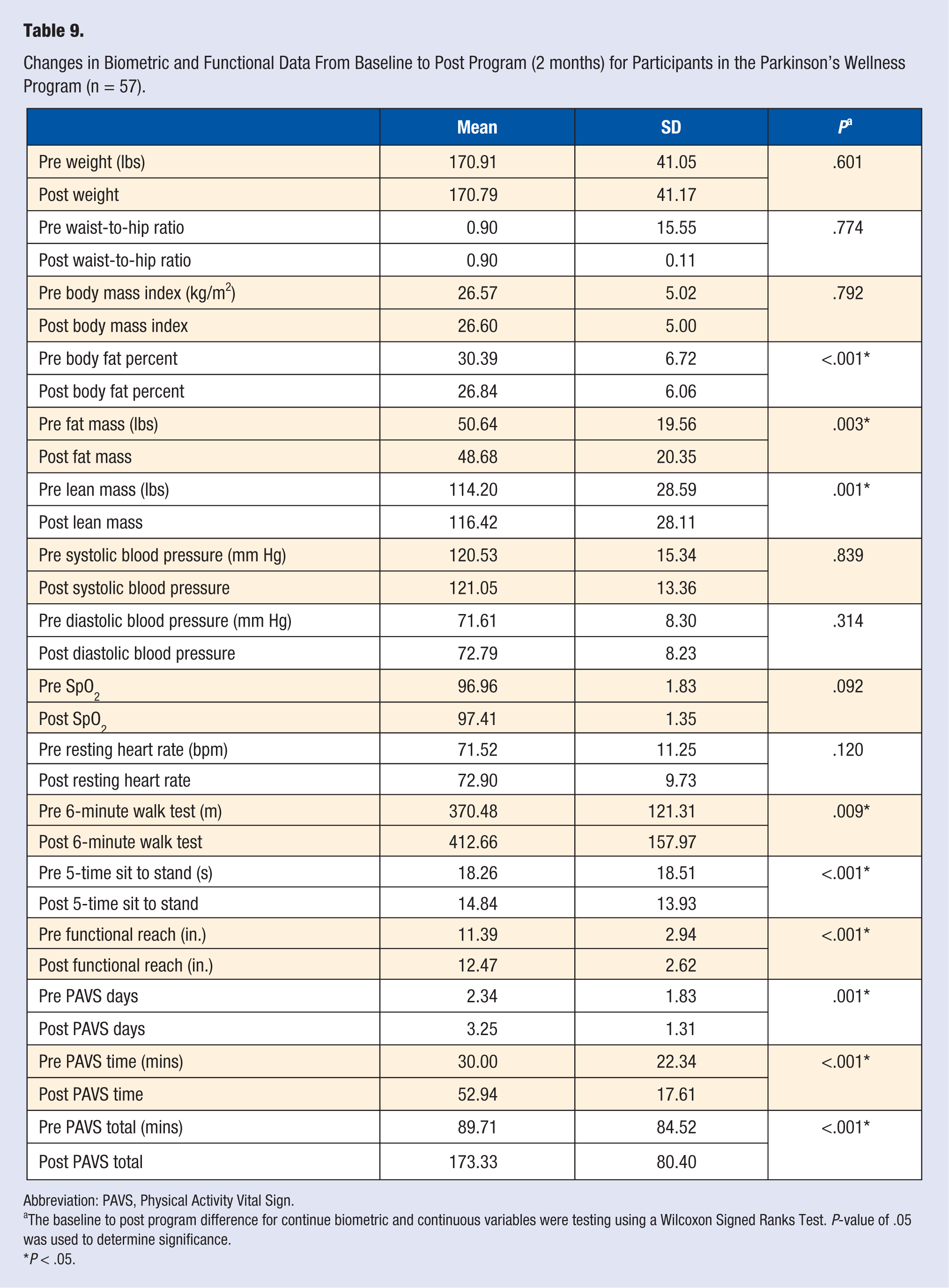
Table 9 displays data recorded from 57 participants in the Parkinson’s Wellness Program. The average age of the participants in the Parkinson’s Wellness Program was 70 years (SD = 8.12). After completion of the Parkinson’s Wellness Program, participants significantly decreased their body fat percent (P < .001) and fat mass (P = .003), and increased their lean mass (P = .001). Functionally, Parkinson’s Wellness Program participants increased their 6MWT distance (P = .011) and functional reach (P < .001), while decreasing their 5-time sit to stand time (P = .009). Parkinson’s Wellness Program participants also significantly increased their PAVS from 89.7 minutes (SD = 84.5) to 173.3 minutes (SD = 80.5) (P = .001) by significantly increasing the number of days of physical activity (P < .001) and number of minutes of physical activity (P < .001).
Changes in Biometric and Functional Data From Baseline to Post Program (2 months) for Participants in the Parkinson’s Wellness Program (n = 57).
Abbreviation: PAVS, Physical Activity Vital Sign.
The baseline to post program difference for continue biometric and continuous variables were testing using a Wilcoxon Signed Ranks Test. P-value of .05 was used to determine significance.
P < .05.
Discussion
Clinical Significance
To our knowledge, this is the first study to investigate the feasibility of implementing disease-specific, CSEPs for persons with a variety of CMCs among hospital-based fitness centers. While there have been numerous community-based exercise programs (Livestrong, Dance for Parkinson’s) evaluated and reported in the literature, most have studied a single cohort (vs the variety of CMCs we report on) and were not created with the intent of being integrated within the continuum of care of outpatient, rehabilitation medicine. In addition, this study is unique in its recommendation of minimum standards for the implementation for CSEPs, a discipline which is currently unregulated and poorly understood among the medical community and general public.12,13 The study findings reveal that for all disease-specific CSEPs, there was a consistent pattern of benefit among participants, suggesting a positive physiological and conditioning response to the exercise dose and program. The pattern of response among participants included (1) favorable changes in body composition as reflected by gains in lean body mass, a decrease in fat mass, percentage of body fat and for the Bariatric Wellness Program cohort, a statistically significant decrease in total body weight and BMI; (2) a significant increase in submaximal exercise tolerance, as measured by the 6MWT; (3) a significant improvement in functional outcome measures; and (4) in all cohorts, a significant increase in self-reported exercise as measured by the PAVS.
These findings are consistent with the evidence regarding the expected conditioning response and benefits of regular exercise for all CMCs included in our analysis.10,14 For each population targeted through our CSEPs, these physiological adaptations are commonly associated with numerous benefits, including decreased mortality (cardiac, diabetes, cancer, bariatric), decreased morbidity (cardiac, diabetes, cancer, Parkinson’s, bariatric, MoveWell) and reported improvements in activities of daily living (cardiac, diabetes, cancer, Parkinson’s, bariatric, MoveWell).15-23
Several clinically significant findings for both biometric and functional outcomes were found among the various cohorts. Specifically, participants in the Bariatric Wellness Program had a preprogram BMI average of 41.2 kg/m2, classifying them as class 3 (extreme) obesity. After completing the Bariatric Wellness Program, the average BMI was 39.4 kg/m2, which reclassified the cohort as class 2 obesity. 24 The change in BMI may have been aided by the significant reduction in body fat mass as well as a significant increase in lean muscle mass. The participants in this cohort also saw a reduction in weight greater than 5% and a reduction in body fat percent greater than 10%. This is significant because obese individuals who lose 5% of their weight have been shown to experience improved insulin sensitivity and β-cell function. 25 These favorable changes in body composition for the Bariatric Wellness cohort are clinically meaningful, as bariatric patients often face health concerns that include loss of lean body mass, which may impair strength, resulting in muscular fatigue that may impair their ability to perform functional tasks. Additionally, postsurgical patients may also experience a decrease in metabolic rate due to the loss of lean body mass. 19
Participants in the Cancer Wellness Program also experienced several significant changes in biometric and functional outcomes that were also clinically relevant. The reduction of the preprogram mean waist-to-hip ratio from 0.94 to 0.84 is important to note because waist-to-hip ratios greater than 0.90 are associated with increased risk of metabolic complications. 26 Functionally, the improvement in 6MWT distance exceeded the minimum clinically important difference (MCID) of 85 m, 27 as the postprogram 6MWT distance of 529.51 m was 106.42 m greater than the preprogram 6MWT distance of 422.58 m. The significant reductions in body fat percentage and waist-to-hip ratio combined with an increase in the PAVS and 6MWT distance are particularly important for this population. Numerous research studies have suggested that a reduction in weight when combined with increases in physical activity and cardiorespiratory capacity are important for survivorship, reducing the rate of recurrence and mortality for several cancers.18,28
Cardiac Wellness participants experienced significant improvements in their systolic blood pressure, 6MWT distance as well as their PAVS score, suggesting a continued training benefit beyond the completion of a traditional outpatient (phase II) Cardiac Rehabilitation Program. This is important to note because while cardiac patients will experience improved aerobic capacity during cardiac rehabilitation, adherence to a postcardiac rehabilitation exercise regimen is traditionally poor, with research suggesting that up to 80% of cardiac patients failing to maintain a regular exercise program after discharge from cardiac rehabilitation. 17 The lack of exercise adherence by cardiac patients after discharge may result in a decline in VO2 max and adversely affect other known cardiovascular risk factors. 17 Furthermore, participants in the Cardiac Wellness Program experienced a significant reduction in waist-to-hip ratio, body fat percent and increased lean mass. Considering that physical inactivity, being overweight, and hypertension are risk factors for heart disease, the participants in the Cardiac Wellness Program continued to reduce their risk-profile even after being discharged from a cardiac rehabilitation program. 29
The Diabetes Wellness Program provided several benefits to participants, including a significant reduction in body fat percentage and an increase in lean mass. Participants also significantly increased their PAVS score, averaging 68.10 minutes of physical activity per week before the program and 177.5 minutes per week after the program. These significant changes are note-worthy because obesity and physical inactivity are substantial contributors to insulin resistance. 23 Exercise can improve insulin sensitivity through mechanisms such as lowering fat mass and increasing lean body mass. 15
Participants in the Parkinson’s Wellness Program experienced clinically relevant improvements on both anthropometric and functional outcomes. Specifically, research suggests that resistance exercise can improve dynamic muscular strength, functional ability, gait, and balance in individuals with Parkinson’s disease. 21 Exercise may also improve motor function in Parkinson’s disease as well as executive function. 20 The results of the present study are consistent with these findings as participants in the Parkinson’s Wellness program significantly improved their 6MWT distance of 370.48m to 412.66 m, reduced their 5-time sit to stand time from 18.2 to 14.8 seconds, as well as significantly increased their functional reach from 11.38 to 12.47 inches. These are important clinical findings as studies indicate that a 5-time sit to stand score greater than 16 seconds is associated with an increased risk of falls. 30 Thus, the Parkinson’s Wellness Program may provide a mechanism for providers and health care systems to engage this patient population in a service that will help them maintain, if not improve, their function.
Finally, the MoveWell Program was developed for persons who have had a joint replacement (hip or knee) and/or were dealing with chronic pain of various etiologies. Studies have shown an association between obesity and chronic pain. 16 Obesity is also a risk factor for osteoarthritis, which further increases the risk of hip or knee arthroplasty. Furthermore, research suggests that obesity (BMI >35 kg/m2) is an independent risk factor of pain and recovery following total joint replacement. 22 The participants in the MoveWell Program experienced a significant reduction in body fat percent as well as an increase in lean mass, suggesting favorable improvements to body composition. Clinically, this is an important observation, as previous research has suggested that weight loss helps reduce self-reported pain levels. 16 This weight change may in part be attributed to the significant increase we observed in the PAVS score for the MoveWell cohort.
In summary, disease-specific CSEPs can be successfully implemented in a community-based setting and provide significant biometric and functional benefits among a variety of clinical populations. These programs may offer providers and health care systems an additional mechanism to engage and monitor these patient populations, while providing access to services known to maintain and/or improve their health outcomes, while potentially lowering the cost of care. Our findings clearly demonstrate that the physiological adaptations to exercise among persons with CMCs can be maintained and even enhanced in a CSEP that is integrated within the continuum of care of outpatient rehabilitation medicine.
Expanding the Continuum of Care of Outpatient, Rehabilitation Medicine
At the center of health care reform and the passage of the Patient Protection and Affordable Care Act were the issues of high cost, variable quality, and inconsistent access to care. This has important implications for rehabilitation professionals, as policy makers are beginning to critically analyze, and even question, patient outcomes relative to the cost of the service.
Several studies have noted the current gap in research on the quality of physical therapy services, especially for defined populations.31-39 However, numerous efforts have been made to both quantify and understand the cost of physical therapy services as a component to the annual health care spend. In 2007, $13.5 billion was spent on 88 million ambulatory physical therapy visits for approximately 9 million adults older than 18 years. This spending accounted for approximately 4.1% of all ambulatory health care expenses for adults. In 2007, Machlin and collegues 38 estimated that the average total cost per episode of physical therapy was $1184, which included 9.6 visits per episode at an average charge per visit of $130.
Machlin et al 38 included various health insurance payers in their analysis, which included private insurance, Medicare, Medicaid, out-of-pocket payments, and other miscellaneous payment sources. More recently, Xinliang et al 40 conducted a similar analysis, but only included individuals who had private health insurance. The authors found that the average annual expense for physical therapy services was $820, with patient’s receiving 23 total relative value units (RVU) of rehabilitation services during 10 visits, over an 84-day period. This analysis also found that the most commonly performed services by physical therapists were therapeutic exercises (35.01%), manual therapy (23.04%), and neuromuscular reeducation (9.24%). The mean payment per RVU for therapeutic exercise was $43.57, followed by $32.98 for manual therapy and $32.31 for neuromuscular reeducation. What was absent from both analyses were data on the efficacy of the treatment performed and/or patient-related outcomes. As the physical therapy profession continues to play a pivotal role in the health care delivery system, there is an obligation to demonstrate its value given its high associated costs. 40
At its core, outpatient rehabilitation medicine delivers care that is inherently patient-centered, while incorporating each patient’s values and treatment goals within the plan of care. Individualized care plans are required in all rehabilitation settings and are developed by the therapist, using best practices and measurable outcomes that are meaningful to each patient. However, in today’s era of health care reform in which payers are moving away from fee-for-service medicine toward value-based payment models, more attention must be given to the cost-effectiveness of outpatient rehabilitation medicine. 7 For nonacute patients with chronic medical conditions, alternative therapy (exercise) and treatment models which deliver similar quality (ie, appropriate screening, patient-centered care, evidence-based exercise interventions, individualized care, measurable outcomes) must be considered.
Potential Standards and Monitoring of Community-Based, Supervised Exercise Programs
Over the years, the Center for Medicare and Medicaid Services has made multiple attempts to identify and fund evidence-based, outpatient rehabilitation and community-based exercise services that target those with CMCs. Comprehensive outpatient cardiac rehabilitation programs are now considered to be the standard of care for patients following myocardial infarction and for procedures to improve coronary vascularization (angioplasty, coronary artery by-pass, grafting, stent, etc). 40 Despite the overwhelming evidence regarding the clinical and survival benefits of cardiac rehabilitation, utilization of such programs remains glaringly low (14%-35%). 40 It has been well documented that lack of accessibility to program sites, challenges with insurance coverage, and program costs ($125-$150 per visit) are primary contributors to the underutilization of cardiac rehabilitation services. 9 Additionally, for years, CMS has made free gym memberships available to patients enrolled in Medicare Advantage Programs (MAPs). In spite of convincing data that MAP enrollees who use their SilverSneakers membership one or more days per week experience measurable health benefits and lower annual health care costs,41,42 fewer than 10% MAP beneficiaries make any attempt to activate their gym membership in a given year. Of this group, half of eligible MAP members make only one visit to their center of choice before dropping out.41,42 There is ample evidence that the lack of engagement in the SilverSneakers program, which is free for MAP enrollees, can be attributed to the design of the benefit, which primarily provides access to exercise equipment and amenities, with minimal personal attention, supervision, coaching or measurement of individual and aggregate outcomes.
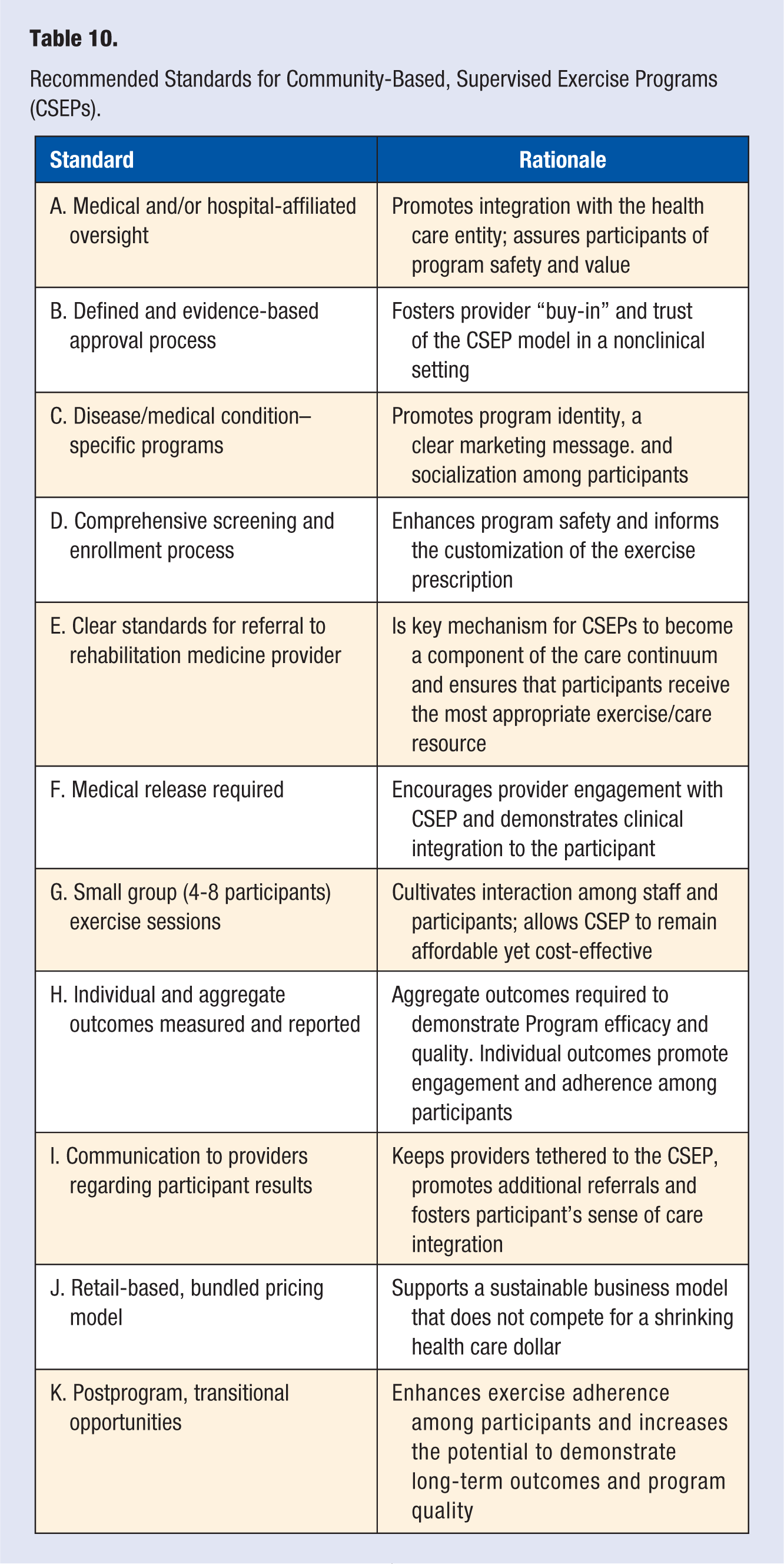
The present study suggests that there is an opportunity to improve the management and exercise adherence of persons with CMCs through a model that integrates CSEPs with the delivery of outpatient rehabilitation medicine. However, it is not within the scope of this article to determine the optimal setting or location for the delivery of CSEPs. Rather, it is the authors’ contention that supervised exercise programs for persons with CMCs can be delivered in multiple community venues (medical fitness centers, community centers, YMCAs, senior residential centers, etc) and should be accessible to as many patients as possible. What may be more important is the eventual development and adoption of recommended standards for CSEPs (see Table 10), which can be promulgated and enforced by an appropriate National agency such as the American College of Sports Medicine, the Medical Fitness Association, The American Association of Cardiovascular and Pulmonary Rehabilitation or the American Physical Therapy Association. This strategy parallels the approach taken by CMS and their implementation of the Medicare Diabetes Prevention Program MDPP. 43 By using an evidence-based program (the Diabetes Prevention Program)44-46 and creating national delivery standards, which are achievable in an assortment of community settings, CMS has made it possible for the MDPP to reach the greatest number of Medicare recipients while concurrently minimizing program variability. It is our recommendation that CSEPs follow a similar path to implementation, both to demonstrate their value within the continuum of care and extend their reach and impact among persons with CMCs.
Recommended Standards for Community-Based, Supervised Exercise Programs (CSEPs).
Finally, this study has provided useful information on the planning and implementing of CSEPs and identified the need for future research to test the efficacy of CSEPs compared to control and/or alternative intervention groups. Furthermore, more research is needed to understand the impact of CSEPs within the continuum of care in outpatient rehabilitation medicine, particularly among bundled or value-based payment models.
Limitations
While many significant findings were observed regarding the impact of CSEPs among persons with CMCs, this study was not without several limitations. First, the study did not use a randomized-control trial design; participants self-selected their participation into a wellness program (CSEP). Self-selection indicates a certain level of motivation, which in turn, can influence program outcomes. Additionally, some CSEP cohorts include broad age ranges for the participants, which could incorporate confounding variables, such as risk factors and comorbidities. Furthermore, the CSEPs were only 2 months in duration and did not include postprogram follow-up and monitoring. Therefore, we were unable to demonstrate longer term outcomes among participants. Future studies should follow patients over a longer period of time to understand the impact of CSEPs on biometric and functional data as well as exercise adherence. Finally, the data collected in the study consisted of biometric- and functional-based measures only. As we had no access to health claims or health care cost data among our participants, we unable to judge the true value of our CSEPs when compared to traditional outpatient, rehabilitation services.
Footnotes
Acknowledgements
We would like to thank the senior leadership of the Population Health Innovation Team (PHIT) of Fitness & Wellness Professional Services as well as all the staff, faculty and students, at the collaborating institutions- Kean University, RWJ BarnabasHealth, Outpatient PT&OT Department, Columbia University, School of Engineering & Applied Science. We would also like to acknowledge our hospital partners: Centrastate Healthcare System, Hackensack Meridian Health, Main Line Health, RWJBarnabas Health, & Princeton HealthCare System.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Timothy F. Marshall, Jay Groves, and Ronald Pietrucha II are employed by Fitness & Wellness Professional Services, the company which designed and implemented the Community-Based Supervised Exercise Programs (CSEPs) discussed in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was reviewed and approved by a university institutional review board.
Informed Consent
Written informed consent was waived by the University Institutional Review Board because this study involves a chart review of previous participants in the Wellness Programs over the past several years.
Trial Registration
Not applicable, because this article does not contain any clinical trials.