
Abstract
Objective:
Continuity of care is considered foundational to high-quality care. Traditional continuity of care constructs may adequately characterize care quality in general populations, but may merit reconceptualization for patients with multiple chronic conditions. Specifically, interactions between multiple chronic condition patients and providers involve complex medication management; therefore care continuity measurement may be more relevant if focused on the provider subset who prescribes essential medications for chronic conditions—a construct we call continuity of medication management. Our objective was to explore conceptual distinctions between continuity of medication management and continuity of care, survey existing evidence in this area, and discuss implications of our findings for future research and intervention development.
Methods:
In this topical review, we discuss conceptual distinctions between continuity of medication management and continuity of care, review the limited continuity of medication management–related empirical evidence, and discuss implications for future research and interventions.
Results:
Continuity of medication management represents a potential conceptual and measurement advance by reflecting interpersonal continuity and management continuity, and may provide a means of identifying patients at high-risk of adverse events. Empirical evidence also establishes support for continuity of medication management as a meaningful measure of care continuity. Finally, continuity of medication management may also be a potential target for future intervention to improve care delivery among multiple chronic condition patients.
Conclusion:
If continuity of medication management is validated in diverse populations, correlated with patient outcomes, and responsive to change, then it may be an important target for improving the health and health care of multiple chronic condition patients.
Introduction
Continuity of care is a well-established concept spanning five decades of research and is considered fundamental to high-quality primary care.1–9 Prior observational research indicates that more coordinated care, defined as receiving care from a single provider (or single team), is associated with better care experiences,3,10,11 fewer emergency department visits, and fewer hospitalizations.3,12 Conversely, fragmented care from multiple providers has been associated with duplication of services, medications, diagnostic tests, and procedures.13–16 Increasing number of providers and chronic medications has been associated with greater risk of adverse drug events and drug–drug interactions.17–20
Continuity of care is a centerpiece of Accountable Care Organizations (ACOs) and Patient Centered Medical Homes (PCMHs),21,22 although evidence is mixed about whether these care delivery models improve care coordination and quality of care or reduce health expenditures.23–26 Most improvements in health and economic outcomes appear to be concentrated in patients with multiple chronic conditions (MCCs). 27 To realize the greatest outcome improvements for MCC patients, it may be useful to reconceptualize continuity of care in terms of the clinical realities of MCC patients. These patients incur a disproportionate share of health expenditures,28,29 often see more providers, 30 and require more complex medication regimens than patients with a single chronic condition. 31
For MCC patients, continuity of care may be more relevant if considered in relation to the subset of providers who prescribe medications essential for managing their chronic conditions. We refer to this restriction of continuity of care to prescribers of medications for managing chronic conditions as continuity of medication management (COMM). The degree of conceptual and empirical overlap between traditional continuity of care measures and COMM is unknown. Our definition of medication management focuses upon actions taken by a physician or other health-care provider prescribing medications, because we seek to understand the role of potentially divergent medical care received from multiple autonomous prescribers on outcomes for MCC patients. COMM is considered from the perspective of the prescriber who must manage the medication regimen of an MCC patient in terms of changing doses, switching medications, adding medications, and conducting medication reconciliation more generally. Conceptual clarity about the role of discordant medical care from prescribers could eventually inform refinement of existing care coordination interventions32–35 designed to improve the acquisition, organization, and administration of necessary medications for MCC patients.
Conceptual framework for continuity of care
Continuity of care has been conceptualized as comprising three distinct but related latent constructs that are essential elements of an idealized conceptualization of continuity: interpersonal continuity, management continuity, and informational continuity (Figure 1).36,37 Interpersonal continuity has been defined as an ongoing therapeutic relationship between a patient and the same provider (or care team) in the same place with the same medical record. Saultz 36 referred to interpersonal continuity as a special type of longitudinal continuity in which provider and patient interactions are “characterized by personal trust and responsibility.” Without interpersonal continuity, the therapeutic relationship may suffer due to lack of mutual familiarity and trust between patients and their providers. Management continuity has been defined as the extent to which services delivered by different providers are timely and complementary such that care is experienced as connected and coherent. 37 Ideally, management continuity should also incorporate patients’ preferences and changing priorities in care planning. Without management continuity, patients may experience discordant plans from different providers, leading to poorer outcomes and lower patient satisfaction. Informational continuity refers to a provider’s access to comprehensive information about a patient’s previous health-care encounters, medical history, and circumstances. Without informational continuity, care may be duplicative and wasteful.

Conceptual model of continuity of care and component dimensions.
These three constructs underlying the latent construct of idealized care continuity are represented by solid lines in Figure 1. The dotted lines between constructs in Figure 1 represent the inter-relationships between constructs, because one construct may influence or build upon another. Interpersonal and management continuity are enhanced by high-level informational continuity. For example, complete provider knowledge of all care provided to a given patient augments interpersonal continuity by facilitating provider–patient rapport and trust. Complete provider knowledge also facilitates greater care coordination and resolution of discordant care plans, which should bolster management continuity. Informational continuity may be improved by multiple providers seeing a single patient if they all utilize a single integrated electronic health record (EHR). In the absence of integrated EHR, informational continuity remains possible if providers communicate directly with one another.
Although interpersonal and management continuity are generally likely to be positively correlated, patients may experience high continuity along one dimension but discontinuity along another dimension. For example, management continuity might be optimal if all pharmaceutical, procedural, and other care for a particular patient were clinically appropriate and had undergone comprehensive review by a single provider to avoid drug–drug interactions and duplicate tests. However, interpersonal continuity might be suboptimal if this patient had frequent clinical encounters with other providers (even if in the same practice). Management continuity for this patient would worsen if the various providers made changes to the patient’s medication regimen or made new treatment decisions without the primary provider’s knowledge. In the absence of complete informational continuity enabled by a comprehensive integrated EHR or receipt of all care in the same medical group, it is common for such treatment decisions to be made in isolation.
Ideally, continuity of care measures should reflect all three conceptual domains, but most claims-based measures primarily represent interpersonal continuity because they aggregate the number of providers seen in face-to-face encounters over a defined period of time. 38 Existing continuity of care measures typically do not account for the individual clinical actions taken by different providers that reflect management continuity. Similarly, we are unaware of any validated claims-based measure of informational continuity, but survey-based continuity of care measures have been developed to measure all three constructs.39,40 However, such survey measures are more costly to collect and thus less scalable than claims-based measures. As a result of these conceptual and measurement limitations in existing measures, much of the claims-based evidence base between continuity of care and patient outcomes is based on measures of interpersonal continuity. There remains a need for claims-based measures that reflect a greater number of continuity of care domains. COMM was developed to fill this need.
Methods
We introduce a novel conceptual construct, COMM, which complements existing continuity of care measures and may be particularly relevant to MCC patients. We discuss how COMM reflects more of the domains of care continuity (interpersonal, management, and informational) than traditional continuity of care measures, and their conceptual similarities and distinctions. We then provide a topical review of empirical studies that examine COMM-related constructs to provide context to the preceding discussion of conceptual issues. We conclude with a discussion of implications of COMM as a target for intervention development or a mechanism to identify target subgroups for care coordination interventions. As ACOs and PCMHs evolve in the coming years to increase their effectiveness, COMM may represent an important means by which health and health care for MCC patients can be improved. Human subjects approval was obtained from the Institutional Review Boards at the Durham Veterans Administration Medical Center (VAMC), Duke University, and the University of North Carolina.
Results of COMM and continuity of care construct comparison
We define our novel concept, COMM, as the subset of providers who prescribe essential medications for managing chronic conditions among MCC patients. In prior work, we have operationalized COMM as a count of prescribers of essential medications.41,42 COMM is conceptually related to but distinct from traditional continuity of care measures in three respects (Table 1). First, the unit of measurement for each construct differs. Most continuity measures are calculated based on the number of unique provider–patient encounters for preventive, acute, and chronic care in a specified timeframe, such as 1 year. In contrast, the unit of measurement for COMM is the number of unique provider-prescriptions for essential medications in chronic disease management because these medications are a central, measurable clinical “product” of health-care interactions with many MCC patients. Not all providers prescribe essential medications for managing chronic conditions, so prescribers of essential medications often represent a subset of the providers included in a typical continuity of care measure.
Conceptual issues in continuity of medication management and care continuity.
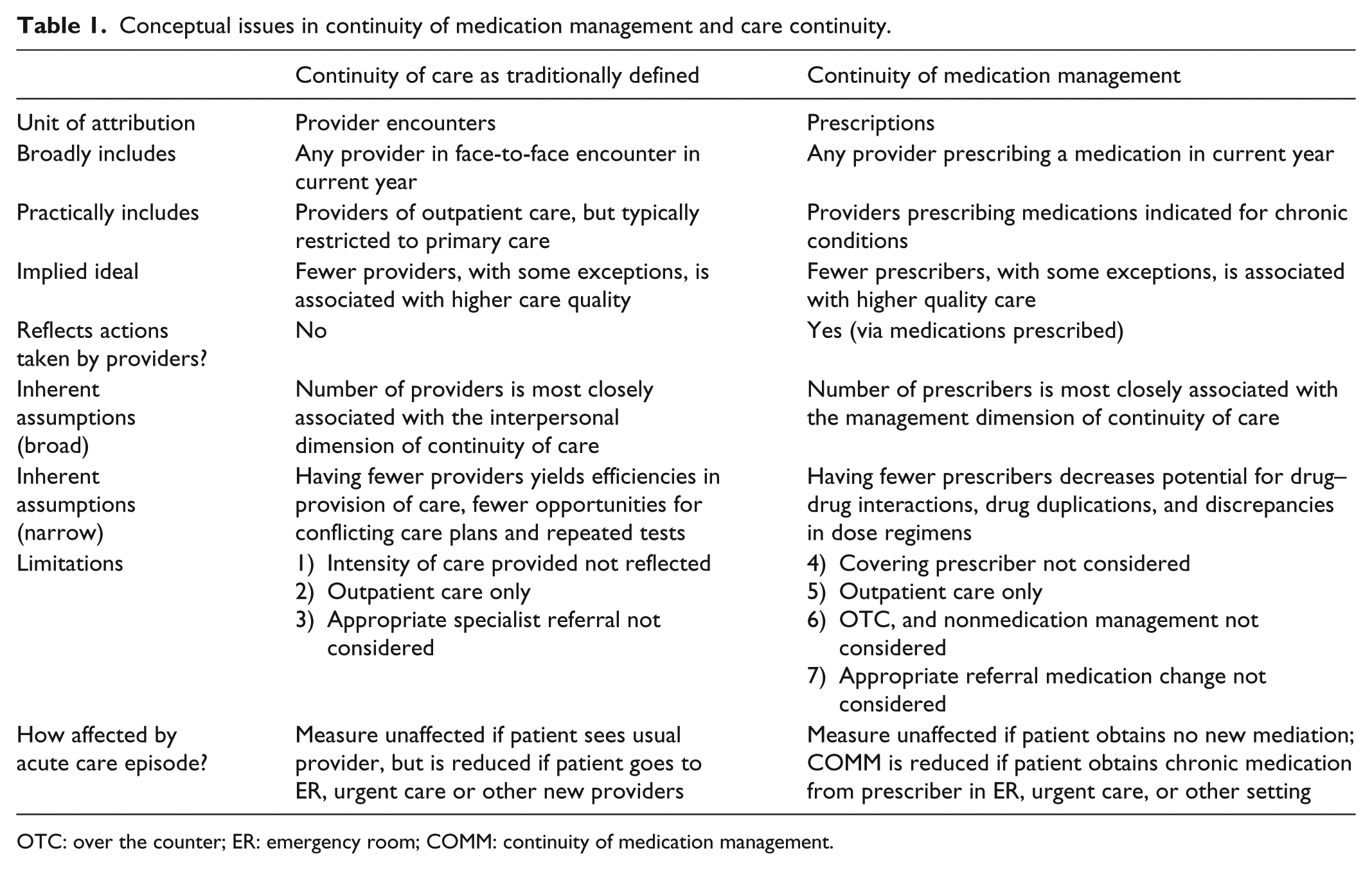
OTC: over the counter; ER: emergency room; COMM: continuity of medication management.
A second implication of differing units of measurement is that COMM is relatively unaffected by acute or preventive care encounters. That is, providers are excluded in the measure if they do not prescribe essential medications for managing a chronic disease. Excluding acute and preventive care from continuity considerations among MCC patients may be appropriate for two reasons. For these patients, discontinuity in preventive care may be less impactful on their health and care utilization than discontinuity in their chronic disease care, and discontinuity in acute care may be less impactful for short-term medications that do not induce interactions with essential medications. For example, consider a situation in which an MCC patient visits one provider for treatment of a urinary tract infection who prescribes antibiotics, a second provider for a flu-shot who does not prescribe medications, and a third provider who prescribes diabetes medications. In this example, a traditional continuity of care measure would include all three providers, whereas our COMM measure would only include the third provider.
A third way in which continuity of care and COMM measures differ is that claims-based continuity of care measures solely represent interpersonal continuity, while COMM represents interpersonal and management continuity. Claims-based measures of continuity of care weigh all encounters with all providers equally, regardless of care (acute, preventive, or chronic) or services provided (counseling, procedure, or prescription). In traditional continuity of care measures, a 5-min flu-shot weighs equally with a comprehensive 45-min medication reconciliation visit. This strategy may be adequate for measuring interpersonal continuity, but does not reflect management continuity. Management continuity may be as important as or more important than interpersonal continuity in caring for MCC patients, so a claims-based measure that represents both domains may be particularly meaningful for MCC patients. Since COMM is constructed on the basis of medication data (a central, measurable product of the encounter), it represents both interpersonal continuity (the number of prescribers involved in a patient’s care) and management continuity (clinical actions providers take as a result of jointly determined therapeutic plans). Thus, COMM reflects the clinical reality that encounters for MCC patients that address medication management and disease control may be particularly influential on health relative to preventive or acute care encounters.
Results of topical review
These conceptual distinctions between COMM and continuity of care suggest that poor COMM, operationalized as a greater number of prescribers, would be a significant risk factor for adverse events among vulnerable or MCC patients. Despite an increasing number of studies associating patient outcomes with multimorbidity17,28,43–51 and the well-known risks of poorly managed polypharmacy, there are few studies of COMM. The first study (to our knowledge) of COMM-related associations in a sample of 315 elderly inpatients found that risk of hospital admission due to medication nonadherence increased with the number of physicians regularly seen, even after adjusting for sex, the number of prescription medications, and patient recall of medication regimen. 52 In a study of 51,587 elderly patients taking cardiovascular, psychotropic, or nonsteroidal anti-inflammatory drugs, the number of prescribers was a stronger predictor (Odds Ratio (OR) = 1.44–1.71) of potentially inappropriate drug combinations than the number of providers (OR = 1.17–1.39). 53 In a study of 384 elderly veterans, having multiple prescribers was more predictive (OR = 3.35, p = 0.03) of having unnecessary drug use at hospital discharge than age, gender, race, marital status, education, employment, the Charlson index, activities of daily living, or number of prescribed medications. 54 In a study of 405 elderly Medicare beneficiaries enrolled in a Pennsylvania managed care plan, having more prescribers was associated with a greater risk of adverse drug events (OR = 1.3, p = 0.02), 55 but was less predictive than having four or more chronic conditions.
We recently conducted analyses of outcomes associated with having multiple prescribers for patients with chronic conditions in Medicaid and the Veterans Administration (VA). In a study of 7868 Medicaid patients with schizophrenia in North Carolina, patients with three prescribers were significantly more likely than patients with one prescriber to switch anti-psychotic medications (p < 0.01) and to be either fully adherent or over-adherent (p < 0.001). 41 In a sample of Veterans with diabetes, hypertension, dyslipidemia, or heart failure during 2008–2010 at a single VAMC in North Carolina, we found that more prescribers of cardiometabolic medications was associated with medication refill nonadherence. 56 We also found that the number of cardiometabolic medication prescribers was positively associated with more all-cause and cardiometabolic-specific emergency room (ER) visits (all-cause: two prescribers, OR = 1.16; three prescribers, OR = 1.21; 4+ prescribers, OR = 1.39) and inpatient admissions (all-cause: two prescribers, OR = 1.27; three prescribers, OR = 1.30; 4+ prescribers, OR = 1.34). 42 Results from these studies indicate that having multiple prescribers is one of the strongest predictors of adverse drug events and avoidable utilization, which suggests that COMM may be a critical risk factor by which multimorbidity is associated with health-care utilization.
Discussion
There is value in greater conceptual and empirical clarity about whether all three continuity domains or specific domains are particularly relevant to MCC patients, because persons with MCC under care of multiple providers are increasingly prevalent. Furthermore, intuitively promising care models have not been able to effectively improve health outcomes and contain expenditures of MCC patients.27,35,57–59 Bending the cost curve in any segment of the US health-care system will require improved management of MCC patients, and care continuity is likely to be an important part of effective care models. COMM represents a potentially useful conceptual and empirical refinement of continuity of care that may be particularly relevant for improving the care management of MCC patients. Existing empirical evidence suggests that increasing number of prescribers is strongly associated with adverse medication-related outcomes and avoidable utilization, suggesting that COMM may be a meaningful construct for identifying patients at risk of adverse events.
To have greater confidence that COMM is a predictive risk factor for adverse events, future research is needed in two areas. First, there is a need to evaluate whether COMM is more strongly associated with adverse events of MCC patients than traditional claims-based continuity of care measures. In a study of 5586 adolescents, the number of prescribers of asthma medications was significantly associated with ER visits and hospital admissions for asthma, but a care continuity measure representing the total number of prescribers was uncorrelated with these same outcomes. 60 Similar comparative analyses need to be conducted in adult populations across a broader array of outcomes.
Future research is also needed that examines whether results from the prior COMM-related studies in Veteran,42,54,56 Medicaid, 41 and Medicare Advantage 55 populations generalize to Medicare and commercially-insured populations. If COMM is shown to be more strongly associated with a range of outcomes in adult populations than continuity of care measures and significant associations are found across treatment settings, then this would suggest that COMM may be a novel indicator of risk for suboptimal quality of care.
In addition to a care quality measurement, COMM may have predictive value for broadly defined preventable adverse events. Marek and colleagues 33 have demonstrated positive effects of nurse care coordination on patient self-management of medications, while Naylor and associates 32 have described benefits of a comprehensive transitional care intervention for heart failure patients. However, several recent care coordination interventions for MCC patients failed to improve outcomes or reduce expenditures on average,27,58,59 but realized expenditure reductions among a subset of high-risk patients.27,34,59 Comparison across these interventions is difficult because the definition of high-risk varied between these three studies; addressing either risk of hospital readmission34,59 or including a broad risk adjustment score based on costs, diagnosed conditions, and demographic factors. 27 COMM represents a potential alternative mechanism to characterize patients at high-risk for adverse events across a range of outcomes, not limited to hospital readmission risk. However, this will also require validation and will likely need to be delivered alongside patient-level interventions effective at improving medication taking behavior of MCC patients, because nonadherence is a complex multi-modal challenge.
Finally, COMM may be a suitable target of intervention for care coordination. In order to further pursue COMM in this manner, the “active ingredient” or construct among MCC patients must be established. 61 If management continuity is the “active ingredient,” then patients of providers with current and comprehensive care plans that match patient priorities and desires should have optimal outcomes. If, however, interpersonal continuity is the “active ingredient,” then patients with a single provider or patients with a primary care provider (PCP) that coordinates well with specialists and other PCPs should have optimal outcomes. If informational continuity is the “active ingredient” and EHRs are optimally structured for efficient information extraction by providers, then patients in health systems with such EHRs and providers who excel at information extraction should have optimal outcomes. To investigate this, future research should be conducted to develop and validate a measure of informational continuity from claims data or EHR data. A claims-based measure would enable examination of whether informational continuity is a key factor differentiating effective care coordination interventions, such as high-quality PCMHs, from ineffective interventions, such as low-quality PCMHs.
Greater insight about the key domains of continuity of care that improves patient outcomes, particularly for MCC patients, is needed. Such insights could further inform the value of COMM among MCC patients as well as the next generation of ACOs and PCMHs. Until these issues are well understood, it will be difficult to improve upon current care continuity measurement and care coordination interventions or to develop new interventions to improve outcomes of MCC patients.
Conclusion
This topical review outlined the conceptual distinctions between COMM and continuity of care and reviewed the limited research related to COMM. COMM represents a potential advance on conceptualization and measurement for continuity of care by reflecting both interpersonal continuity and management continuity. Opportunities exist to substantiate COMM as a predictive construct for research and clinical practice. If COMM is validated in diverse populations, correlated with patient outcomes, and responsive to change, then it may be an important target for improving the health and health care of MCC patients.
Footnotes
Acknowledgements
We would like to thank Elizabeth Bayliss for helpful comments. A preliminary version of this article was presented as a poster at Academy Health Annual Research Meeting 2014.
Declaration of conflicting interests
Drs Maciejewski and Farley have received consultation funds from Daiichi Sankyo. Dr Maciejewski has received consultation funds from ResDAC at the University of Minnesota, and owns stock in Amgen due to his spouse’s employment. Other authors have no known conflicts of interest. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veteran Affairs, Duke University, or the University of North Carolina at Chapel Hill.
Funding
This research was funded by the Agency for Healthcare Policy and Research (R21 HS019445). This work was also supported by the Office of Research and Development, Health Services Research and Development Service, Department of Veterans Affairs. Dr Maciejewski was also supported by a Research Career Scientist award from the Department of Veterans Affairs (RCS 10-391).