
Abstract
Objective:
To examine trends in child sleep, physical activity, and screen use during the COVID-19 pandemic in New York City with a prospective, longitudinal online survey of parents recruited from a large medical center.
Methods:
Data was collected Spring 2020 (“Complete Shutdown”) and Fall 2020 (“Partial Shutdown”). Outcomes were parental perceptions about changes in child sleep, physical activity, and screen time compared to before COVID-19; and contemporaneous measures of these child behaviors. We report contemporaneous responses and paired analyses to describe longitudinal changes.
Results:
Two hundred seventy-seven participants were surveyed during Complete Shutdown and 227 (81.9%) filled out a follow-up survey during Partial Shutdown. The largest percentage of parents at both time points perceived no change in child sleep, decreases in child exercise, and increases in child screen time. In paired analyses, perceptions shifted toward less sleep, more physical activity and less screen time from Complete Shutdown to Partial Shutdown.
Conclusion:
COVID-19 had negative impacts on child health behaviors that did not resolve over a 6-month period despite partial reopenings.
Introduction
On January 30, 2020, the World Health Organization declared a global health emergency in response to the COVID-19 pandemic, and on March 1, 2020, the first COVID-19 case was reported in New York State (NYS). 1 Children living through the COVID-19 pandemic shutdown in New York City (NYC) from March to June 2020 faced complete school closures and dramatic changes to their everyday lives and routines due to stay at home and social distancing orders. Beginning in summer 2020, the city began transitioning from tighter restrictions to a partial shutdown. Many have suggested that school closures related to COVID-19 may impact child health and development. 2 Sleep, physical activity (PA) and screen time are important drivers of child health and development, and have direct effects on risk for obesity, mental health problems, and other chronic diseases.3–6
Prior research on the impact of COVID-19 on child health behaviors has generally documented increases in screen time and decreases in PA during the initial shutdown period.7–17 However, the magnitude of effects vary based on time, location, and population. For example, a study in Sweden documented increases in preschool PA during the pandemic. 18 Pandemic effects on sleep have been less consistent, with some studies reporting increases in child sleep duration,7,8,10,19 and others documenting deceases in duration20–22 or shifts in timing or quality of sleep.12,15,16,19,23,24
Some studies of the pandemic’s impact on child health behaviors only collected data at one time point,7,9,10,12,19,23,24 while others longitudinally compared child behaviors pre-pandemic to behaviors during the initial, early lockdown period.8,11,13,14,16–18,20,21 Studies documenting longitudinal changes in childhood health behaviors during different stages of the lockdown are lacking. We are only aware of one study in Europe that assessed sleep in infants and toddlers during multiple periods of lockdown from April to June 2020, which documented an initial decrease in sleep followed by a complete return to baseline. 22 Another study in the southeastern United States (U.S.) longitudinally examined child health behaviors during the spring and summer of 2020 and compared results to data collected from the same children in the two calendar years prior, but their results did not focus on changes between two periods during the pandemic. 15
Washington Heights, Inwood, and Harlem are neighborhoods in northern Manhattan with high proportions of racial/ethnic minority residents, low-income households, and the highest COVID-19 case rates starting early in the pandemic. 25 Understanding child health behaviors during different phases of the COVID-19 pandemic among populations most burdened by COVID-19 is necessary to inform future efforts to address childhood obesity and pediatric developmental and mental health problems, and facilitate recovery efforts. Yet, little research exists on how modifiable drivers of child health and development in NYC were altered in the context of evolving public health measures to curb the spread of COVID-19. The overall goal of this study was to examine childhood health related behaviors of sleep, PA, and screen time during two distinct phases of the COVID-19 pandemic in a population of children at high risk for obesity and developmental and mental health problems. Among families receiving care in a large academic medical center in northern Manhattan, we aimed to examine contemporaneous and longitudinal change in parental perceptions of the COVID-19 pandemic impact and report of childhood health related behaviors of sleep, PA, and screen time at two time points: (1) Spring 2020 during complete shutdowns at the start of the pandemic in NYC and (2) Fall 2020 during partial reopening of schools and businesses.
Methods
Setting and participants
We conducted a prospective, longitudinal study of participants in the Family Health Study to examine child sleep, PA, and screen time behaviors at two time points in the COVID-19 pandemic, 6 months apart. The Family Health Study is an online survey of pregnant women and parents recruited from Columbia University Irving Medical Center (CUIMC), a large academic medical center in northern Manhattan, during the COVID-19 pandemic. CUIMC is located in the Washington Heights/Inwood neighborhood, a diverse community in which over 70% of residents identify as Hispanic and about a third are living in poverty. 26 The community is an “empowerment zone,” a label given by the U.S. federal government to economically distressed areas that are eligible for specific types of governmental aid. Due to socioeconomic and structural inequities, children from this area are at higher risk for a variety of health and developmental conditions including obesity. 27 The community surrounding the medical center also had some of the highest rates of COVID-19 early in the pandemic. 25
Participants were recruited from a research registry consisting of pregnant women or parents with a child under age 18 years who received ambulatory care at CUIMC between 2009 and 2020 and consented to contact for research. Participants were also recruited through an online recruitment service (RecruitMe) operated by CUIMC. Participants were eligible if they could answer questions in English or Spanish and had a child under 19 years of age or were pregnant at the time of recruitment. Participants were invited to take part in the study via emails sent out between April 16 and June 1, 2020, with an option to proceed to the study eligibility questions, consent form, and survey, or to opt-out. Those who did not have an email address listed were contacted by phone to elicit an email address. The study team followed up by phone with those who did not select to opt-out and did not click on the survey, to assess their interest and answer any questions. The study team also provided help by phone to those who had difficulty answering questions online. Written electronic informed consent was obtained from all participants before the study. After consent, participants responded to questions for themselves and their child. Surveys were available in both English and Spanish. For families with multiple children, parents were asked to fill out the survey in reference to their oldest child who was under 19 years of age. Participants who filled out the initial survey were recontacted by email 6 months later with an invitation to complete the follow-up survey. Phone calls were made to participants who expressed a preference for phone communication.
In total, 484 people clicked the survey link, and 282 enrolled and completed the survey (completion rate 58%). For this analysis, we excluded five participants who were without a child during the initial survey. Of the 277 participants with children who filled out the initial survey, 227 (81.9% follow-up response rate) completed a follow-up survey. Participants received US $45 (US $20 for the first survey and US $25 for the follow-up) for their participation. Ethical approval for this study was obtained from CUIMC Institutional Review Board (protocol #AAAS9876).
Main outcomes
See the appendix for survey questionnaires. We measured parental perceptions of changes in child sleep, PA, and screen time as compared to before the “shutdown.” The survey referred to the “shutdown” as the “stay at home” and “social distancing” orders put in place in March 2020 in response to COVID-19. Parents responded to the following questions created for this study that asked them to think about the past month (30 days): Compared to before the shutdown, how would you say that your child’s (1) sleep has changed? (a lot more sleep, more sleep, no change, less sleep, a lot less sleep, I don’t know), (2) exercise (PA, active play time, or tummy time) over the past month is different? (a lot more exercise, more exercise, about the same, less exercise, a lot less exercise, I don’t know), (3) screen time is different (a lot more screen time, more screen time, no change, less screen time, a lot less screen time, I don’t know)?
Parents responded to questions adapted from a prior study on obesity and sleep that measured child usual bedtime during the week in the past month (before 8 pm, 8–10 pm, 10 pm–12 am, later than 12 am) and child usual wake time during the week in the past month (before 6 am, 6–8 am, 8–10 am, later than 10 am). 28 Length of time in bed was estimated by subtracting the two responses coded as the midpoint of each time range or an hour before or after each cutoff (e.g., before 8 pm = 7 pm, 8–10 pm = 9 pm, later than 10 am = 11 am).
For children ⩾5 years old, PA was measured using the National Institutes of Health Patient-Reported Outcomes Measurement Information System (PROMIS) Parent Proxy Short Form v1.0-Physical Activity. 29 The PROMIS Pediatric PA instrument is a validated measure of a child’s performance of PA over the past 7 days with a score that is standardized with a mean of 50 and a standard deviation of 10. For child screen time, parents responded to four questions adapted from a previously validated survey.30,31 Questions were updated to reflect the variety of modern screen time options for children and assessed child daily hours in the last 7 days of computer or tablet time for school, video time not for school, video games and computer games not for school, and tablet use not for school. Response options were “I don’t know,” “None,” “<1,” and hourly up to “6 or more hours per day” and coded accordingly with “<1” recoded as 0.5 hours and “6 or more hours per day” as 6. Composite nonschool screen time was calculated by summing responses to the three nonschool screen time questions. Analysis for the screen time for school question was restricted to children ⩾5 years old. Demographic data including child age and gender, parental race/ethnicity and education, and household income and primary language were also collected. All questionnaires were pilot tested by 10–15 study staff members (~5% of study sample size) prior to their use.
Definitions of survey time periods
“Complete Shutdown” was defined as the period of time in Spring 2020 following NYC Mayor Bill de Blasio’s conversion of all public schools to fully remote learning on March 16, 2020, and NYS Governor Cuomo’s executive order on March 22nd mandating all nonessential businesses close statewide in response to the COVID-19 pandemic.32,33 Responses to the initial survey from April 16 to June 1, 2020, are referred to in results as “Complete Shutdown.” “Partial Shutdown” was defined as the period in Fall 2020 when a phased reopening of businesses was underway. On October 1, 2020 NYC schools re-opened to optional hybrid in-person learning for all grades and remained open to in-person learning until temporary reclosure on November 19, 2020, in response to increasing COVID-19 test positivity rates.34,35 “Partial Shutdown” surveys were completed from September 18 to October 16, 2020.
Statistical analysis
We examined data for completeness and errors. Using descriptive statistics, we examined distributions and calculated frequencies (%), mean ± SD, or median interquartile range (IQR) as appropriate for all variables. For contemporaneous analyses at each time point, we used descriptive statistics to examine outcomes. We ran χ2 tests to compare parental race/ethnicity and education of those who completed the follow-up Partial Shutdown survey and those who only completed the Complete Shutdown survey. To examine change in outcomes over time, we performed paired analyses for participants with data from both time points. Participants who responded “I don’t know” were excluded from paired analysis. For continuous variables, we used the Wilcoxon Signed-Rank Test to compare responses during Complete Shutdown to during Partial Shutdown. For ordinal variables, we used the Sign test. As a sensitivity analysis to account for those lost to follow up in the Partial Shutdown survey, we also fit linear and generalized mixed models to assess for longitudinal changes in child behaviors. These models included random intercepts to account for within-subject correlation, and controlled for child age, parental ethnicity and parental education.
Results
Two hundred seventy-seven eligible participants with children at the time of recruitment completed the Complete Shutdown survey. Of those 277 initial participants, 227 (81.9%) completed the Partial Shutdown follow-up survey 6 months later). See Table 1 for participant characteristics. Participants had a wide range of household incomes. A large percentage of parents reported Hispanic ethnicity (56.0%) and about half of parents completed college (47.7%). Participants who completed a follow-up survey did not differ significantly from participants who did not complete a follow-up survey in terms of parental race/ethnicity (p = 0.27), but did tend to have higher levels of parental education (p = 0.02).
Child, household, and parent characteristics.
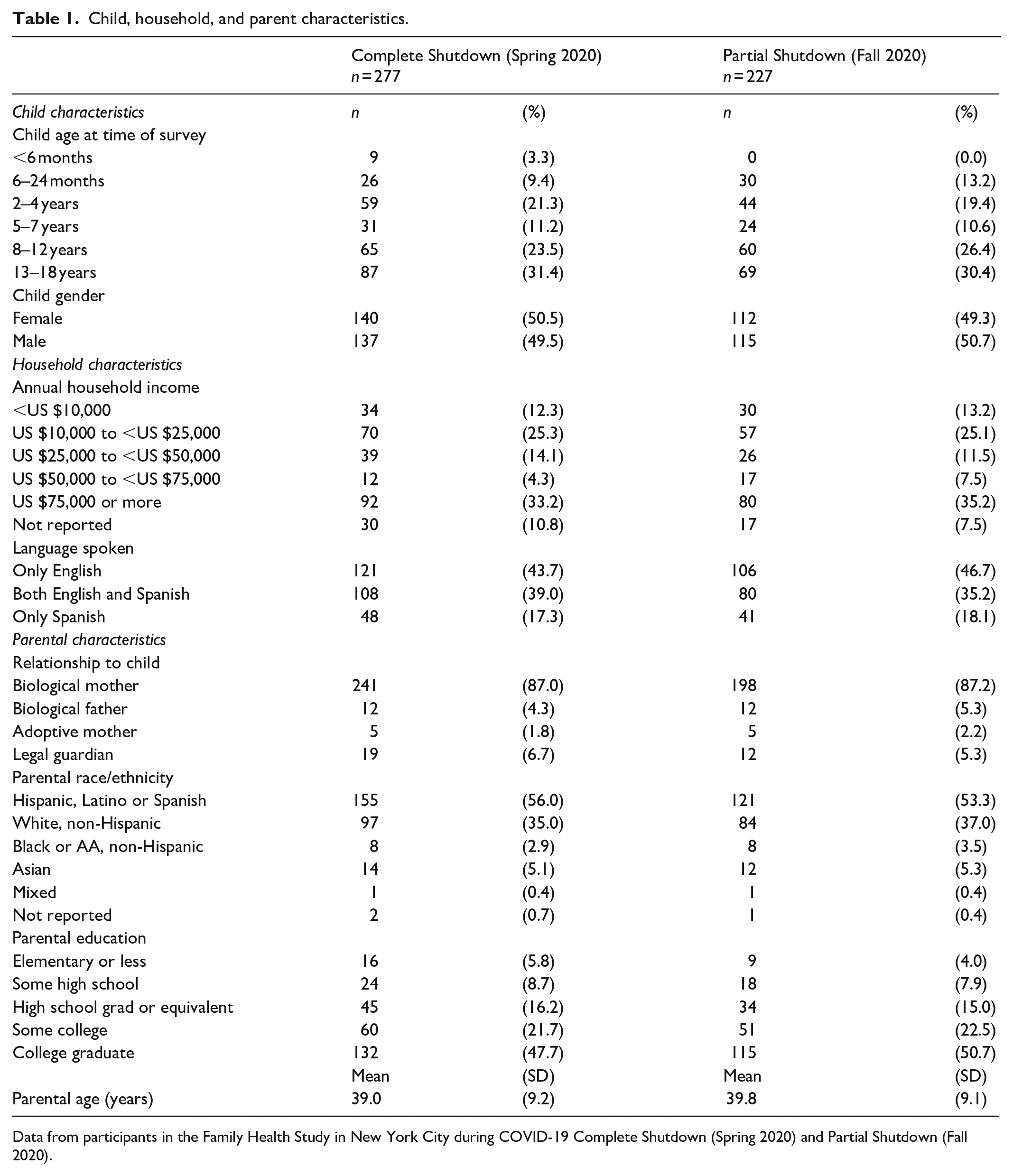
Data from participants in the Family Health Study in New York City during COVID-19 Complete Shutdown (Spring 2020) and Partial Shutdown (Fall 2020).
Table 2 displays summary responses to all surveys during Complete Shutdown in Spring 2020 and Partial Shutdown in Fall 2020. Parental perceptions about changes in child sleep, PA, and screen time at the time of the survey compared to before the pandemic were diverse.
Complete contemporaneous and longitudinal parental perceptions and child behaviors related to child sleep, physical activity, and screen time during COVID-19 Complete Shutdown (Spring 2020) and Partial Shutdown (Fall 2020).

Data from participants in the Family Health Study. h: hours; IQR: interquartile range.
n = 276 at Complete Shutdown (one missing bedtime) and 227 at Partial Shutdown.
n = 183 at Complete Shutdown (restricted to participants ⩾5 years old) and 153 at Partial Shutdown (restricted to participants ⩾5 years old).
n= 179 at Complete Shutdown (restricted to participants ⩾5 years old, four responded “I don’t know”) and 150 at Partial Shutdown (restricted to participants ⩾5 years old, three responded “I don’t know”).
n = 267 at Complete Shutdown (10 responded “I don’t know” to at least one question included in the composite measure) and 216 at Partial Shutdown (11 responded “I don’t know” to at least one question included in the composite measure).
Paired analyses included the 227 participants with data from both surveys, excluding subjects who responded “I don’t know” for either time point. Paired analyses for parental perceptions about child behavior change compared to before the shutdown are displayed in the Sankey diagrams in Figure 1. As depicted by the various branches in the Sankey diagrams, survey response changes from Complete Shutdown to Partial Shutdown were diverse. Parental responses to the question, “Compared to before the shutdown, how would you say that your child’s sleep has changed?” significantly shifted in the direction of less sleep from Complete Shutdown to Partial Shutdown (p = 0.04). Responses to the question, “Compared to before the shutdown, how would you say that your child’s exercise over the past month is different?” significantly shifted in the direction of more exercise from Complete Shutdown to Partial Shutdown (p < 0.001). Lastly, parental responses to the question, “Compared to before the shutdown, how would you say that your child’s screen time is different?” significantly shifted in the direction of less screen time from Complete Shutdown to Partial Shutdown (p = 0.01).

Longitudinal parental perceptions about changes in drivers of child health and development compared to before the shutdown. Data from participants in the Family Health Study in New York City during COVID-19 Complete Shutdown (Spring 2020) and Partial Shutdown (Fall 2020). *p < 0.05; **p < 0.01.
Paired analyses for survey responses about child behaviors are displayed in Table 3. In paired analyses, compared to the Complete Shutdown time point, child bedtimes and wake times were earlier during Partial Shutdown (p < 0.001 for both). We found a significant shift toward less time in bed during Partial Shutdown compared to Complete Shutdown (p < 0.001). In sensitivity analyses, findings for bedtime, wake time, and time in bed were similar when children under age 2 years at baseline were excluded (data not shown). We found no significant changes in PROMIS PA scores or screen time for school. Nonschool screen time significantly decreased from Complete Shutdown to Partial Shutdown (p = 0.04). Results were similar for nonschool screen time when children under age 2 at baseline were excluded (data not shown). Results from mixed model analyses controlling for child age, parental ethnicity, and parental education and accounting for within-subject correlation found similar results (Table 4).
Paired analysis of child sleep, physical activity, and screen time behaviors during COVID-19 Complete Shutdown (Spring 2020) and Partial Shutdown (Fall 2020).

Data from participants in the Family Health Study with complete data at both time points. h: hours; IQR: interquartile range.
Bedtime and wake time values from Sign test, all others from Wilcoxon signed-rank test.
n = 226 participants with data at both time points (one participant missing wake time in Complete Shutdown survey).
n = 153 participants with data at both time points (restricted to participants ⩾5 years old).
n = 148 subjects with data at both time points (restricted to participants ⩾5 years old, five subjects responded “I don’t know” in at least one of the surveys).
n = 214 subjects with data at both time points (13 responded “I don’t know” to at least one question included in the composite measure in at least one of the surveys).
p < 0.05; **p < 0.01.
Child sleep, physical activity, and screen time behavior change during COVID-19 pandemic at Partial Shutdown (Fall 2020) compared to Complete Shutdown (Spring 2020).

Data from participants in the Family Health Study. M indicates the number of clusters (number of subjects included in the analysis), and N indicates the number of observations in the analysis (maximum of 2 and minimum of 1 per subject). h: hours; CI: confidence interval.
Restricted to participants ⩾5 years old.
Logistic mixed-effects models adjusted for child age (continuous), parent ethnicity (Hispanic versus non-Hispanic), and parental education (high school/high school equivalent or less versus some college or more).
Linear mixed-effects models adjusted for child age (continuous), parent ethnicity (Hispanic versus non-Hispanic), and parental education (high school/high school equivalent or less versus some college or more).
Reference group: Complete Shutdown (Spring 2020).
p < 0.05; **p < 0.01.
Discussion
In this prospective, longitudinal study of a diverse cohort of children recruited from a large academic medical center in northern Manhattan during the COVID-19 pandemic, we found that parents perceived substantial negative effects of COVID-19 on childhood health related behaviors of PA and screen time. Perceptions about effects on child sleep were mixed. We found that children had earlier bedtimes, earlier wake times, and shorter time in bed at Partial Shutdown compared to Complete Shutdown. PA scores for this population were below average at both time points. Children had persistently high screen time for school at each time point, and nonschool screen time improved but remained high at Partial Shutdown. Parental perceptions both during Complete Shutdown and Partial Shutdown suggest that pandemic effects on these drivers of child health and development occurred and were ongoing, with incomplete return to pre-pandemic behaviors despite partial reopening of schools and businesses. Taken together, our findings suggest that urgent intervention is needed to increase PA, decrease screen time, and stabilize sleep routines in order to ameliorate childhood health related risk factors during recovery from COVID-19.
At both time points, parental perceptions of child sleep length were largely reported as unchanged compared to before the pandemic. In the Partial Shutdown, parental perceptions about changes in sleep compared to before the shutdown shifted toward children sleeping less as compared to the Complete Shutdown. This was consistent with results of parentally reported bedtime and wake times which showed a shift toward earlier bedtimes and wake times during Partial Shutdown, resulting in overall less time in bed. A possible explanation for alterations in sleep patterns could be that when the pandemic started and the lockdown began, some children’s sleep routines were dramatically altered due to changes in school schedules and home routines, similar to changes that occur over summer break. 36 Some children’s sleep likely benefitted from later school starts and less outside distractions, while other children had their normal sleep patterns negatively disrupted by the lockdowns.
In addition, increases in anxiety and familial stress secondary to the pandemic may have had effects on child sleep patterns and length. Some likely had shifts in their sleep schedules without changes to their overall sleep time. Our results suggest that these alterations partially normalized as the pandemic continued and bedtimes and wake times shifted earlier. This hypothesis is consistent with studies from Asia, Europe and San Francisco that generally found that children shifted toward delayed bedtime and wake times and overall longer sleep times early in the pandemic.7,8,10,12,13,15,19,23,24 This partial normalization after an acute change has been described in other European studies of COVID’s impact on children’s sleep.7,22 In contrast, a study of Italian preschoolers found an increase in sleep time in the initial pandemic that stabilized a month into the pandemic, however longer follow-up in this group may have shown a different trajectory. 20 Healthy and consistent sleep patterns are critically important for child growth and development, and alterations in routines during the pandemic have the potential to impact health outcomes including obesity and mental health.3,37 Pediatricians should be aware of the varied effects that the pandemic may have had on their patients’ sleep habits and screen patients to better understand their needs. Helping families establish consistent bedtimes and appropriate sleep hygiene should be part of every well child care visit.
We found that parents perceived children had less PA and more screen time as compared to before the shutdown. With schools closed and many families quarantining inside small apartments, children’s opportunities for active versus sedentary activities were likely limited. This is consistent with research finding that obesogenic behaviors worsen when children are in unstructured settings. 38 Our results are consistent with many other international studies and three American studies that found decreases in parentally reported PA and increases in sedentary behaviors during the pandemic.7–17
Our study is the first study we are aware of to compare parental reports of child PA and screen time use from two different periods of the pandemic shutdown. During Partial Shutdown parental perceptions comparing child activities to before the pandemic shifted toward more child PA and less child screen time compared to responses in the Complete Shutdown survey, suggesting a partial normalization and in some rare instances resilience. This change was consistent with reports of daily nonschool screen time dropping from the Complete Shutdown survey to Partial Shutdown survey, but was not reflected in the PROMIS PA Scores which remained stable. This could potentially be explained by recall bias in the Partial Shutdown survey with perceptions shifting but child PA remaining low. The stable PROMIS results are consistent with a Spanish study that compared cross-sectional child behaviors in strict versus relaxed confinement and did not find significant difference in reported child PA time. 7 Once routines are changed and physical deconditioning occurs, it is likely that returning to an active lifestyle is challenging, especially when areas to safely exercise remained low.
Overall, a large percentage of parents reported decreased child PA and increased child screen time during Partial Shutdown as compared to before the pandemic. The American Academy of Pediatrics (AAP) recommends no screen time for children under 18 months of age (with the exception of video-chatting), an hour or less for preschoolers and consistent limits for older children to prevent screen time from interfering with sleep, PA and in person social engagement. 39 The World Health Organization’s guidelines for sedentary screen time are similar. 40 These recommendations do not include screen time for school. Our findings suggest that screen time for school in this population is high and may also impact the long-term health of children. Nonschool screen time for this population was median 4.5 h in the Complete Shutdown and 3.5 h during Partial Shutdown, well above cutoffs for young children set by the AAP. Decreased levels of PA and increased levels of sedentary activity could increase risk for childhood obesity and associated chronic illnesses as already documented in a recent study tracking obesity during the pandemic. 41 Pediatricians and policy makers alike should focus on helping children safely return to outdoor and indoor physical activities and reduce sedentary screen time during the COVID-19 pandemic.
Our study’s strengths include its longitudinal nature that allowed us to look at the progression of changes in child behaviors as the pandemic continued. With paired analyses we naturally control for many stable individual characteristics but recognize that both changes in age over time and external factors outside of the pandemic could contribute to changes seen between surveys. Our study population also includes a high number of racial/ethnic minority children in an urban setting, a population vulnerable to COVID-19 and related closures. Our study also has limitations. We recruited from a single institution and given COVID restrictions on research recruitment, a convenience sample was utilized. Sample size was not driven by power calculations for this analysis so it is possible that some null findings were underpowered. Although our study sample consists of families disproportionately impacted by the pandemic early on, findings may not be widely generalizable. Because of the nature of recruitment, we cannot determine how many individuals received information about the survey, and our baseline completion rate was 58%. This completion rate is comparable to other similar online surveys during the COVID pandemic.42,43 We lack pre-pandemic survey measures so we can only make inferences based on parental report about how reported bedtimes, wake times, PROMIS score and screen times compare to pre-pandemic levels. In addition, given limitations in availability of COVID specific questionnaires and desire to rapidly capture data from an important period in history, some of the questionnaires were not validated. Finally, recall bias can exist in any survey study.
Conclusion
In this prospective, longitudinal study of children in NYC during COVID-19, we found parentally reported changes in child sleep patterns, lower PA frequency, and higher screen time during the COVID-19 pandemic. Although some improvements in child behaviors were found later in 2020 during Partial Shutdown, many children continued to have unhealthy behaviors that may put them at higher risk for obesity and a variety of adverse physical and mental health outcomes.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221147851 – Supplemental material for Longitudinal trends in parent-reported child sleep, physical activity, and screen use during the COVID-19 pandemic in New York City
Supplemental material, sj-docx-1-smo-10.1177_20503121221147851 for Longitudinal trends in parent-reported child sleep, physical activity, and screen use during the COVID-19 pandemic in New York City by Morgan A Finkel, Alexis Bryan, Ivette Partida, Laura Raaen, Ngoc Duong, Jeff Goldsmith and Jennifer A Woo Baidal in SAGE Open Medicine
Footnotes
Acknowledgements
We are grateful to the families who participated in this research, to Dr. Elise Kang for providing feedback and conducting pilot tests of the survey instrument, and to Kelsey Nichols and Kristina Parkinson for assisting with study recruitment.
Author contributions
MAF conceptualized the initial study research question and analysis plan, analyzed the data, drafted the initial manuscript, and reviewed and revised the manuscript. AB assisted with creating the study analysis plan, analyzed the data, and reviewed and revised the manuscript. IP coordinated recruitment and data collection, assisted with creating the study analysis plan, and reviewed and revised the manuscript. LR and ND assisted with creating the study analysis plan, aided in study analysis, and reviewed and revised the manuscript. JG oversaw creation of the analysis plan, supervised data analysis and interpretation, and reviewed and revised the manuscript. JWB conceptualized and designed the study, designed the data collection instruments, coordinated and supervised recruitment and data collection, conceptualized the study analysis plan, supervised data analysis, and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All phases of this study were supported by National Institute of Diabetes and Digestive and Kidney Diseases 1K23DK115682 (Woo Baidal) and Columbia University Department of Pediatrics Children’s Health Innovation Nucleation Fund (Woo Baidal). Funders had no role in the design and conduct of the study.
Consent statement
Ethical approval for this study was obtained from Columbia University, Irving Medical Center Institutional Review Board (protocol #AAAS9876).
Informed consent
Written electronic informed consent was obtained from all participants before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.