
Abstract
American dietary patterns have shifted over the past 100 years, resulting in a diet based on animal foods and highly processed carbohydrates. This shift has produced the current epidemics of obesity, type 2 diabetes, heart disease, as well as many cancers. In addition, the Western diet is also negatively affecting the reproductive capacity of the population. The birth rate is in decline and infertility and subfecundity are on the rise secondary to both ovulatory infertility and declining sperm quality. Pregnancy outcomes and maternal morbidity and mortality are also being affected. This diet, high in fat and sugar, is also contributing to the epidemic levels of autism.
“In times of economic uncertainty, there is typically a decline in the birth rate that recovers with economic improvement.”
Declining Birth Rate
The live birth rate in the United States is at an all-time low. It is currently 63.0 live births per 1000 women aged 15 to 44 (Figure 1). In 2010 it was 64.1, and the previous historical nadir was in 1997 at 63.6. 1 These live birth rates are actually a worldwide phenomenon, with the exception of Sub-Saharan Africa. Several factors might account for this phenomenon, including the economic recession of 2008. In times of economic uncertainty, there is typically a decline in the birth rate that recovers with economic improvement. We saw a similar pattern during the Great Depression of the 1930s, and the subsequent economic improvement that coincided with the Second World War that ultimately led to the birth of “Boomer Generation.” With the introduction of oral contraceptives in 1960, there was a rapid decline in the birth rate, with a steady, slow decline subsequently.
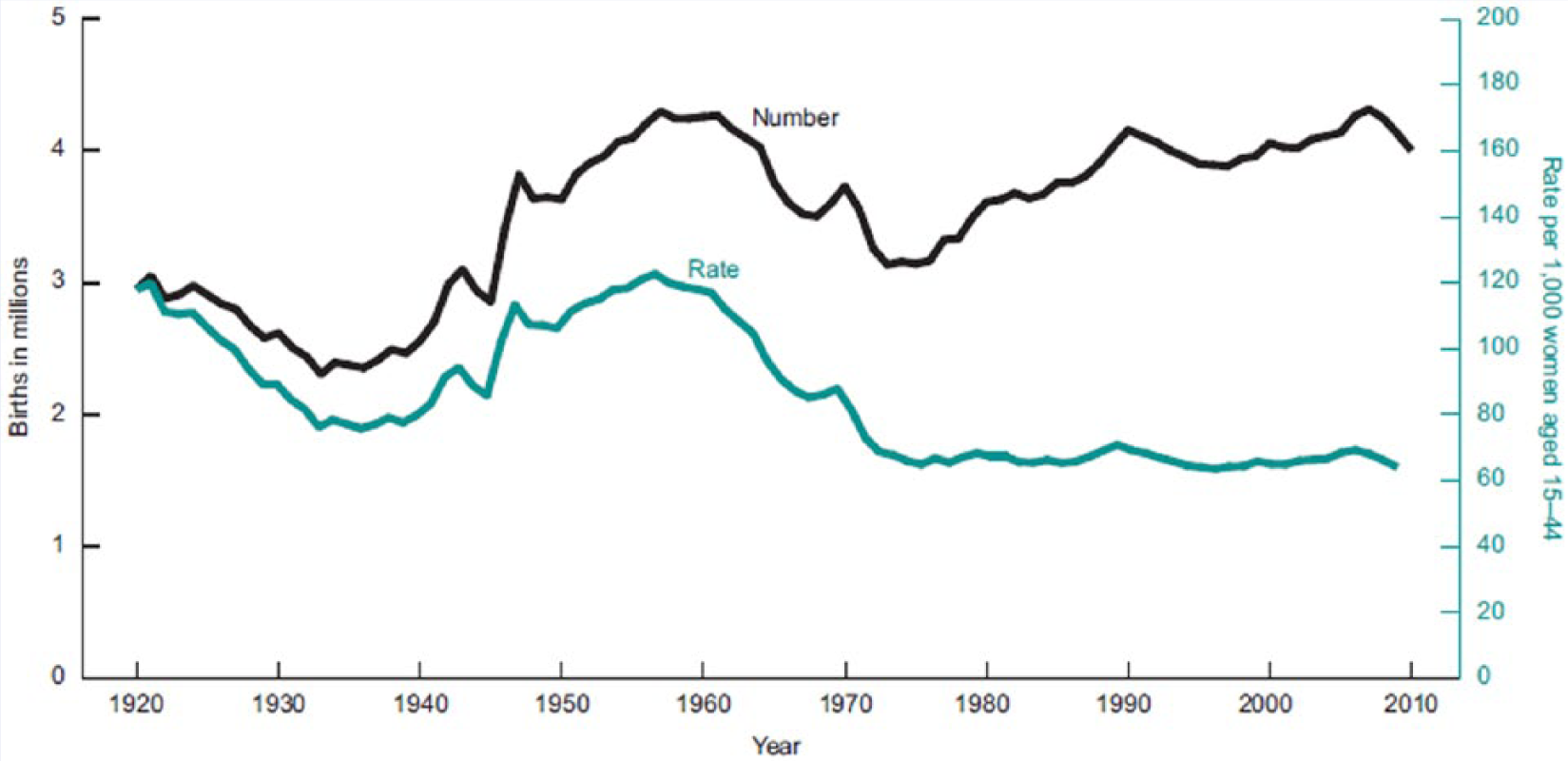
Live Births and Fertility Rates: United States, 1920-2010 1 .
Several factors might be contributing, including continued access to contraception, delaying childbearing to older ages when fecundity is in decline, and a shift of cultural norms placing more importance on careers or self-fulfillment rather than on the rearing of children. The decision to not have children might be in part based on the absence of a maternity leave policy, especially when compared to other industrialized nations. The US Family and Medical Leave Act (FMLA) sets a minimum standard for parental leave, but due to the exclusion of small employers and short-tenure workers, about 40% of US workers are not eligible for the FMLA. In general, US employers as a group have not stepped in to fill the gap. While about 60% of workers are eligible for FMLA-related leave, only about one fourth of US employers offer fully paid “maternity-related leave” of any duration, and one fifth of US employers offer no maternity-related leave of any kind, paid or unpaid. 2
Another way that shifting culture norms can affect birth rates is through media exposure. In India, media exposure correlates inversely with fertility rates almost identically. 3 We have even seen this exposure in the United States. In 2014, an economic study on teen childbearing found that MTV’s television series, 16 and Pregnant, was responsible for a 5.7% reduction in teen births in the 18 months following its debut. 4
There is, however, a compelling argument to be made that obesity and diabetes epidemics might be factors in the declining birth rate. We have seen a steady rise in diabetes and obesity since 1960, and then dramatic rise in both in the mid-1970s and early 1980s. At both extremes of the body fat/body mass index (BMI) scale, there are increases in infertility and declines in fecundity. Maintaining a normal BMI helps retain reproductive capacity, which is important because humans have one of the lowest fecundity rates of all animals. The chance of conception during any month of unprotected intercourse is about 20% when a woman is 30 years old, and declines to only about 5% by age 40—with only 30% of all conceptions actually resulting in a live birth.5,6 Data from the Centers for Disease Control and Prevention (CDC; 2011-2012) tell us that 69.0% of adults age 20 years and older are overweight or obese (http://www.cdc.gov/obesity/data/adult.html). This prevalence is most certainly affecting the capacity for reproduction in various ways, including ability to conceive and to maintain a pregnancy. Pregnancy outcomes are also being affected deleteriously by the obesity and diabetes epidemics. Dietary patterns are directly affecting ovulatory infertility, male factor infertility, and maternal and fetal complications.
Ovulatory Infertility
According to the data from the National Survey of Family Growth (NSFG), infertility is defined as a lack of pregnancy in the 12 months prior to survey, despite having had unprotected sexual intercourse in each of those months with the same husband or partner. Impaired fecundity is defined as physical difficulty in either getting pregnant or carrying a pregnancy to live birth. 7 The data from the NSFG reveal that the percentage of married, infertile women aged 15 to 44 fell from 8.5% in 1982 to 6.0% in 2010. Impaired fecundity among this same group increased from 11% in 1982 to 15% in 2002, but then fell again in 2010 to 12%. It is very difficult to assess the actual rates of infertility and subfecundity; however, there is an argument to be made that the rates of both are significantly higher even when considering ovulatory infertility only and dismissing male factor.
Ovulatory infertility is directly related to polycystic ovarian syndrome (PCOS). PCOS gets its name from the appearance of the ovary on ultrasound, but metabolically what is happening is a constellation of obesity, insulin resistance, and oligo, or anovulation. As women become obese, they become insulin resistant. These elevated levels of circulating insulin suppress the synthesis of sex hormone binding globulin (SHBG), which is crucial in binding free androgens. So, when SHBG synthesis is suppressed, free androgens rise. Infrequent ovulation is the result of these elevated free androgens. 8 A study done by Barnard and colleagues showed that SHBG is increased when women consume a low-fat plant-based diet. 9 This increase happens because insulin resistance and free insulin are reduced and the synthesis of the SHBG is no longer suppressed.
Ovulatory infertility is affected by dietary intake. A study in the American Journal of Obstetrics and Gynecology showed that consuming 5% of total energy intake as animal protein, rather than in the form of carbohydrates, was associated with a 19% greater risk of ovulatory infertility. 10 In contrast, consuming 5% of energy as vegetable protein, rather than as carbohydrates, was associated with a 43% lower risk of ovulatory infertility. Also, consuming 5% of energy as vegetable protein, as opposed to animal protein, was associated with a greater than 50% lower risk for ovulatory infertility. 11
It is prudent to think that the obesity crisis in this country is changing the rates of infertility and subfecundity. These rates are difficult to assess, but the current best estimates are that 6% of married women 15 to 44 years of age in the United States are unable to get pregnant after one year of unprotected sex (infertility) and that about 11% of all women ages 15 to 44 in the United States have difficulty getting pregnant or carrying a pregnancy to term (impaired fecundity). 7 Population studies have shown that approximately 30% of overweight and obese women have PCOS and that the condition is present in 5% of normal-weight women. 11 In cases of ovulatory infertility, 90% are a result of PCOS. 12 As previously mentioned, the CDC (2011-2012) reported that 69% of the population in the United States is overweight or obese, which means that out of 100 000 reproductive-aged women, 69 000 are overweight or obese and 30% (20 700) of those women will have PCOS. That means that 20.7% of adult women have an impaired capacity to become pregnant secondary to oligo or anovulation.
Obese women who receive donor eggs from normal-weight women are also 23% less likely to have successful implantation, 19% less likely to have a clinical pregnancy, and 27% less likely to have a live birth. 13 But even in ovulatory obese women, they are less likely to conceive, their oocyte and embryo quality are reduced, and they have impaired endometrial receptivity. 13 Poor oocyte and embryo quality and impaired endometrial receptivity are likely secondary to oxidative stress. Oxidative stress is defined as an imbalance between pro-oxidant molecules including reactive oxygen species and antioxidant defenses. 14 Oxidative stress has been linked to several reproductive diseases, including endometriosis, PCOS, and unexplained infertility—as well as pregnancy complications such as miscarriage, preeclampsia, and intrauterine growth restriction. It appears that excessive reactive oxygen species production overpowers the body’s natural antioxidant defense system, creating an environment unsuitable for normal female physiologic reactions that are requisite for successful reproduction. 14
Dietary behaviors resulting in obesity and malnutrition are linked with oxidative disturbances and chronic, low-grade inflammation. Studies have shown, repeatedly, that animal foods, and their accompanying saturated fats, trans fats, arachidonic acids, cholesterol, and proteins, are associated with systemic inflammation.15-18 Highly refined carbohydrates have also been implicated in the causation of inflammation.19-21 The data are also clear that whole, minimally processed or unprocessed plant foods are anti-inflammatory in nature.22-25 According to data from the 2009 US Department of Agriculture (USDA) Economic Research Service, the composition of American diet consists of 25% animal foods, 63% processed food, and only 12% plant foods (www.ers.usda.gov/publications/EIB333). The result of this diet is an obese female population that is oligo or anovulatory with oxidative stress, a reduced capacity to become pregnant, because of infrequent ovulation, an egg or embryo of poor quality, and a hostile in utero environment.
Declining Sperm and Semen Quality
Oxidative stress and dietary patterns not only affect the reproductive capacity of women but also affect sperm and semen quality. Male factors are identified in 40% to 60% of cases of couples with infertility. 26 Smoking, alcohol, excessive marijuana, and heat exposure to the testes have all been implicated, but diet plays a huge role in the quality of semen and sperm. Studies reveal that saturated fat consumption negatively affects both sperm counts and sperm concentration in a dose–responsive fashion.26,27 In contrast, sperm morphology is positively influenced by a higher intake of omega-3 fats.
There is a general consensus that semen quality has been in decline in several areas of the world over the past 50 years. 28 This decline is thought to be secondary to a global change in environmental exposures. Specific macronutrients in food, like saturated fat, can negatively affect sperm and semen quality, but food is, in many cases, the vector for other environmental pollutants and endocrine disruptors that are affecting male reproductive capacity. A mother’s consumption of beef can negatively affect her son’s sperm quality as an adult. 29 Perinatal dioxin exposure can also permanently impair semen quality. 30 Presumptively, the maternal beef consumption and dioxin exposure, resulting in reduced semen quality in male offspring, has to do with the endocrine disrupting nature of hormones that are given to cattle during the farming of these animals, and the endocrine disrupting nature of dioxins. Six hormones are commonly used in Canadian and American beef production, which include both natural and synthetic estrogens, androgens, and progesins. 29 Dioxins are a group of compounds that are considered persistent environmental pollutants and are found throughout the environment. They are lipophilic compounds, so they accumulate in the food chain, mainly in the fatty tissue of animals. More than 90% of human dioxin exposure is through food, mainly meat, dairy, fish, and shellfish. 30 These studies represent a small sample of all the studies that show the negative impact of animal food consumption on the quality of semen and sperm. It is clear that both men and women would benefit from a diet high in antioxidants and low in saturated fat and contaminated animal foods to improve the opportunity for conception and live birth.
The Rise of Maternal Mortality
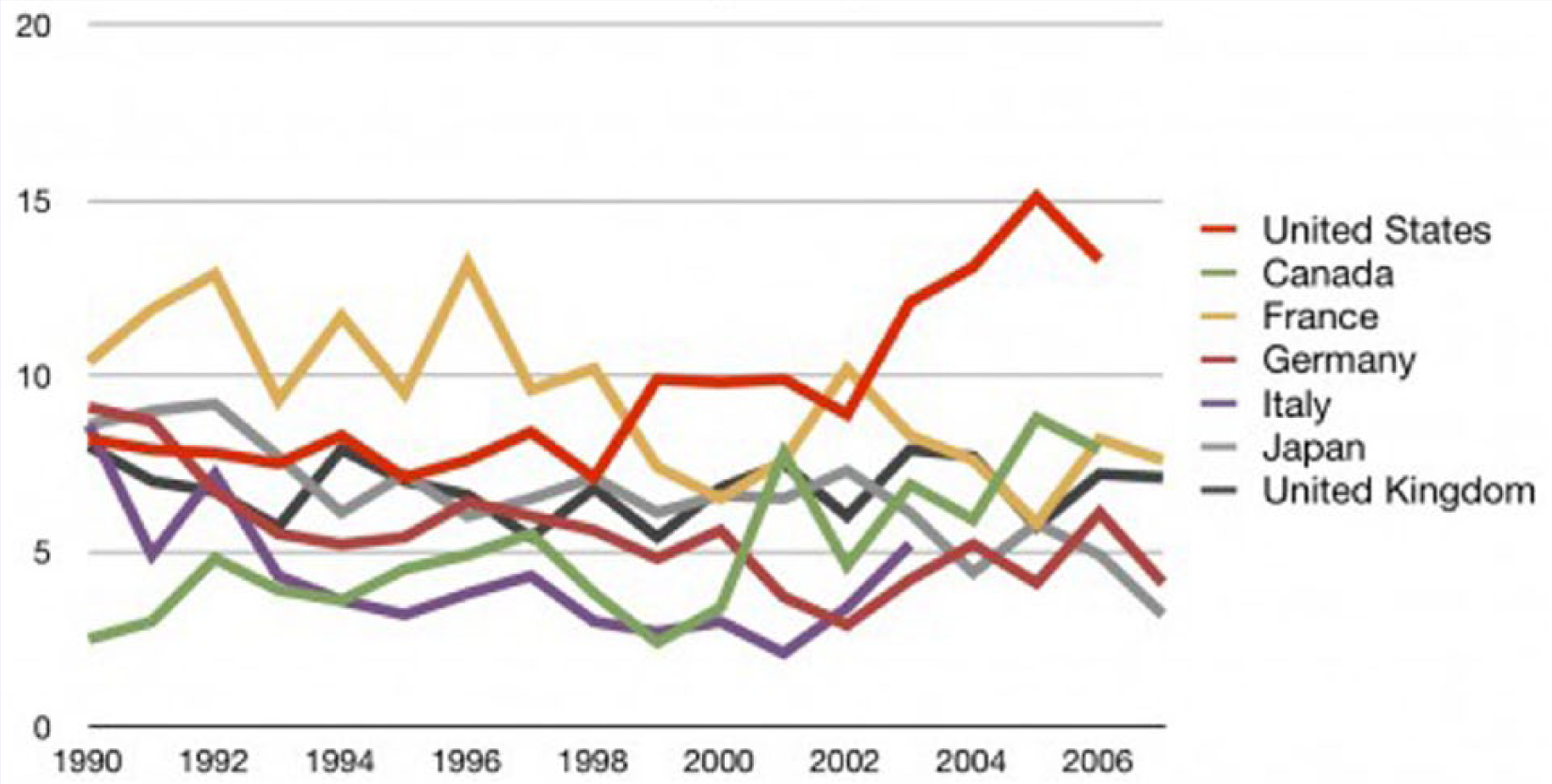
Another disturbing trend in this story is the rise in the maternal mortality rate in this country. According to the CDC, the maternal mortality rate in 1915 was 608 deaths per 100 000 live births. In 1986, it reached a nadir of 8.5 (Figure 2). However, every year since it has risen. In 2003, it was up to 14.1 and it is now at 18.5 with the suggestion that this may be a low estimate. 31 According to the World Health Organization, the number is closer to 28, which is equivalent to the US maternal mortality rate in 1967. 31 This leaves the United States with the highest maternal mortality rates of any other industrialized nation (Figure 3), and 60th among all nations. Our previous ranking in 1996 was 50th. 30
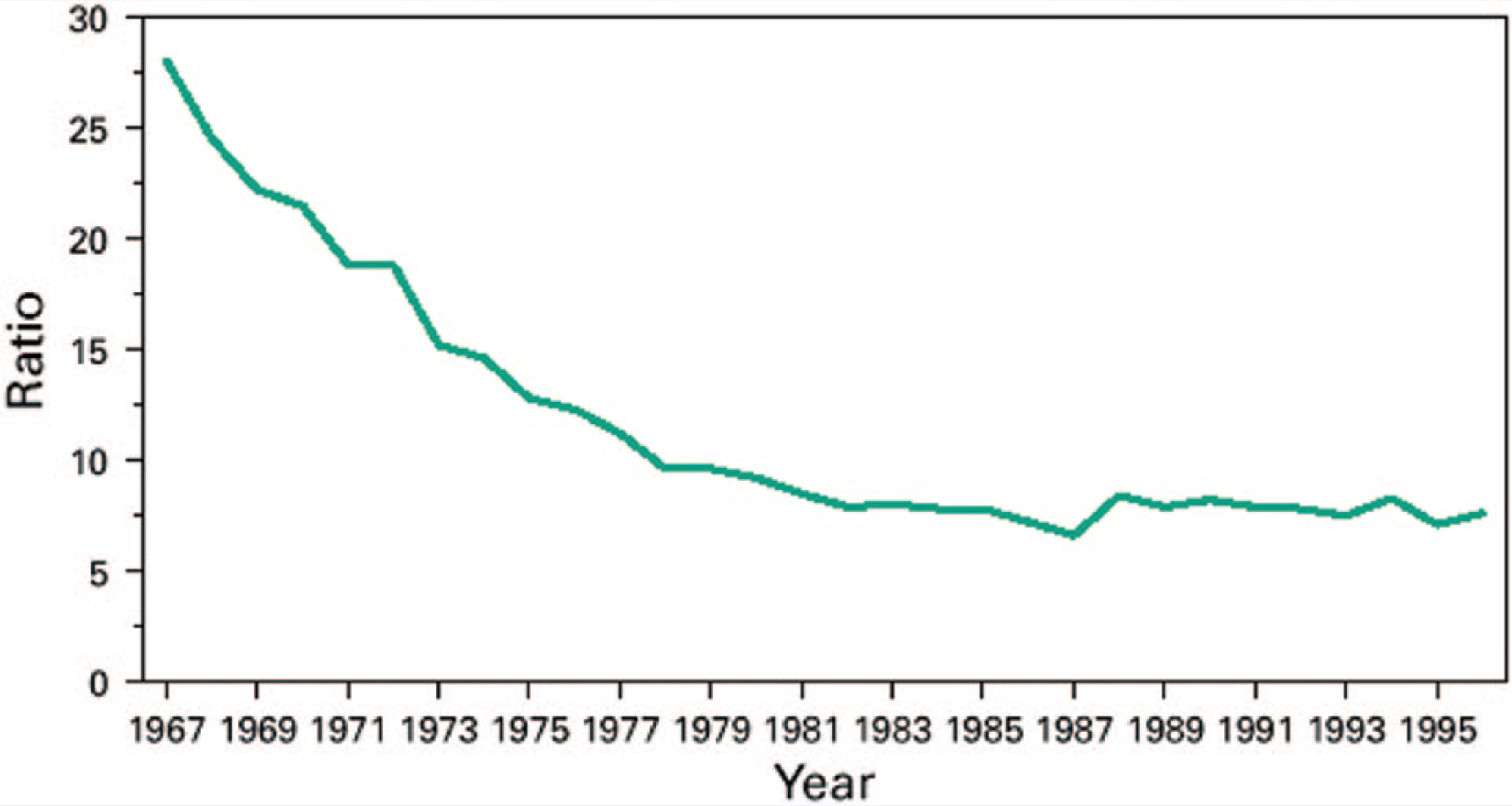
Maternal Mortality Ration, by Year—United States, 1967-1996.
Number of Maternal Deaths per 100 000 Births.
The causes of maternal mortality have changed in the developed nations. Historically in this country and still in the developing world, hemorrhage has been responsible for one quarter of maternal deaths. 31 Today in this country, cardiovascular disease, stroke, and hypertensive diseases of pregnancy combined cause 30% of maternal deaths and hemorrhage, which is now responsible for only 11% of deaths (Figure 4). Pregnancy has become riskier, because there has been such a significant rise in reproductive aged women with obesity, diabetes, and prepregnancy hypertension.
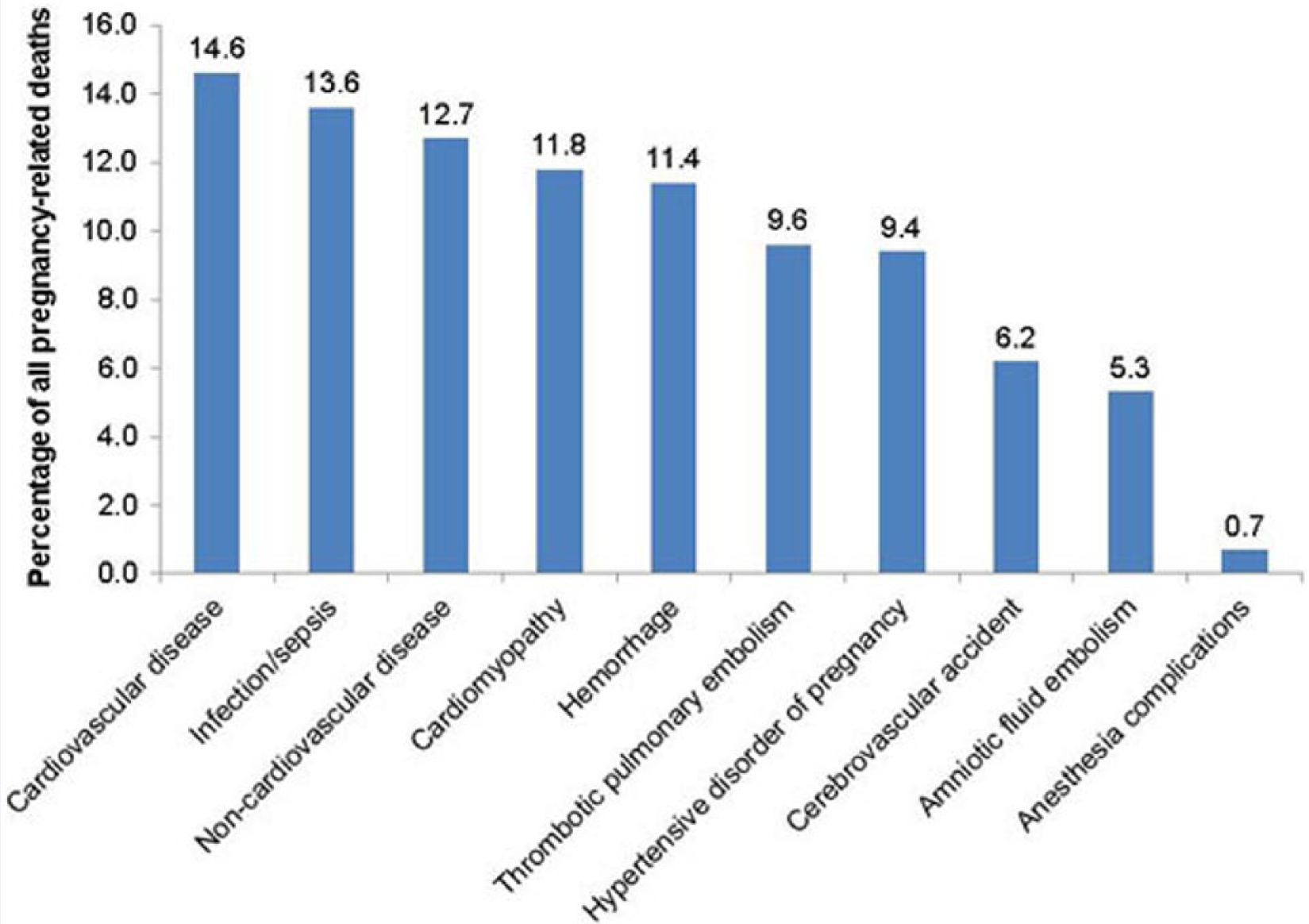
Leading Causes of Pregnancy-Related Deaths.
Maternal and Fetal Complications, Preeclampsia
These maternal morbidities during pregnancy also increase risks for the fetus. Multiple studies have shown that obese mothers, whether or not they have diabetes, are more likely to have a stillbirth.32-35 The risk of stillbirth increases in a dose–responsive fashion, with the more obese the mother is, the higher the risk. 35 Infants born to obese mothers are also at an increased risk of having a congenital anomaly, including cleft lip and palate, neural tube defects, and cardiac defects. 36
One complication of pregnancy that can have dire outcomes for both mother and fetus is preeclampsia. Preeclampsia is a constellation of signs and symptoms that include hypertension, proteinuria, edema, and in more severe cases, headache, elevated liver enzymes, pulmonary edema, and thrombocytopenia that can lead to seizure, stroke, and death for both mother and infant. Twelve percent of maternal deaths in this country are related to preeclampsia. The exact pathogenesis remains uncertain, but the presumption is that it has to do with abnormal placentation, which can result in placental ischemia and release of inflammatory and oxidative stress factors into the maternal bloodstream. In addition, even with normal placentation, preexisting hypertension, diabetes, and other inflammatory conditions (such as lupus) that lead to endothelial dysfunction can activate systemic inflammatory and oxidative stress processes. 37 This explains why obesity, diabetes, and hypertension are risk factors for development of the disease. Once a pregnant woman develops preeclampsia, the only treatment is delivery, regardless of gestational age.
Given the current demographics of the adults in this country, it would be an obvious assumption that the incidence of preeclampsia is on the rise. And, of course, that is exactly what we have seen. And there has been a 322% relative increase in the rate of severe preeclampsia. 38 There has been much research into prevention of preeclampsia, and some studies have shown that aspirin use in women at high risk of developing preeclampsia can reduce development of the disease by as much as 24%. 39 This is presumably from the anti-inflammatory effects of the aspirin. Other studies have shown no such risk reduction. 40
In regard to diet and prevention of preeclampsia, there is one observational study that looked at a community of vegan women. In this community of 775 women who gave birth while living on “the Farm” in Summertown, Tennessee, only one met the criteria for preeclampsia. 41 This is a rate of 0.001%, which is obviously much lower than the 3.8% rate we see in this country.
Preeclampsia, like other cardiovascular diseases, is a result of endothelial dysfunction and inflammation in the blood vessels. Chronic inflammation is also present in diabetics, in the obese, and in patients with autoimmune disease. It has been well verified that dietary patterns that are high in fat, particularly saturated and trans fats, and highly refined carbohydrates cause systemic inflammation resulting in disease.15-21 It has also been well verified that diet based on whole or minimally processed plant foods can reverse these inflammatory processes.22-25
Epidemic of Autism
The incidence and prevalence of autism spectrum disorders have risen to epidemic levels. In 1981, it was 1 in 10000. In 2000, it was 1 in 150, and our most recent estimate is 1 in 68. If the current rate of increase continues (Figure 5), it will be 1 in 2 or 50% by the year 2050. A debate has ensued regarding whether the incidence of autism spectrum disorders is falsely elevated secondary to changes in diagnostic criteria and improved surveillance, or whether there is some environmental factor that is causing an actual real rise in new cases. According to the CDC, there have been no changes in the criteria used to diagnose or treat cases of autism spectrum disorders since 2012, yet there has been a 30% increase in the rate since then. The rate increased from 1:88 in 2012 to 1:68 in 2014. 42
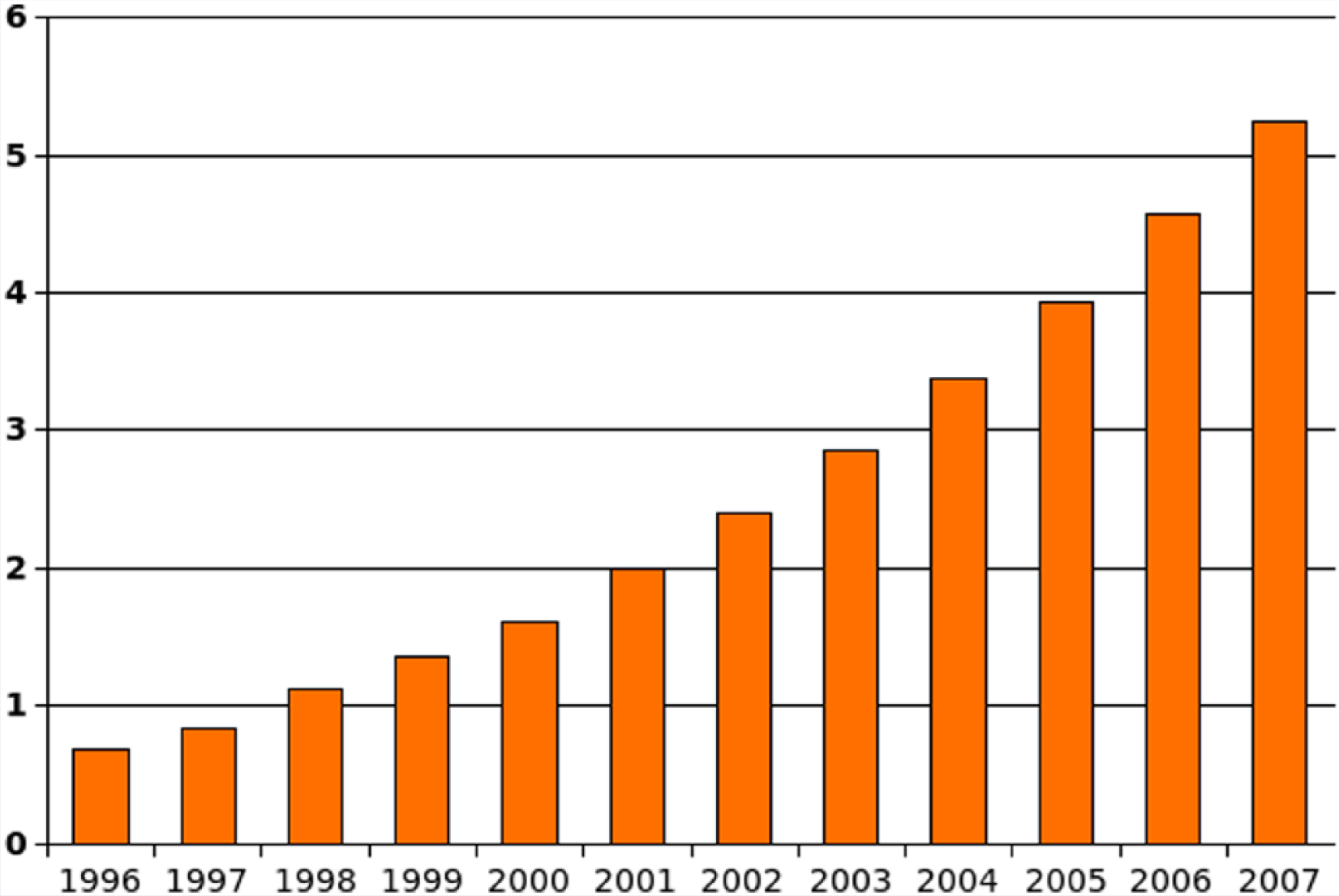
Number of Children Aged 6 to 17 With a Diagnosis of Autism (per 1000 US Residents), From 1996 to 2007.
New evidence reveals that the in utero environment is having an effect on the development of autism spectrum disorders. A recent study in the NEJM looked at brains of children with autism who had died of unrelated causes and compared them to brains of unaffected children. 43 It is known that the brains of children with autism tend to be larger with a relative increase in the overall number of neurons in the prefrontal cortex. This is a normal finding in fetuses during the second trimester of pregnancy, but it resolves by birth or shortly thereafter when there is maturation of the neuronal circuitry. In this study, they found that despite the increased numbers of neurons, there were focal patches with fewer cells expressing layer-specific markers that are normally present in fully differentiated cortical neurons. This means that the neuronal circuitry in these kids is not maturing appropriately through pruning and apoptosis and that proper neuronal migration is not occurring. The primary implication of this article is that these abnormalities almost certainly occurred in utero during key developmental windows, most likely between 19 and 30 weeks of gestation. 43 The pregnancies of these women in this study were unremarkable, but no discussion of routine exposures or obesity was mentioned. There is debate and uncertainty as to what is causing this abnormal brain development and why it so much more prevalent as compared to 15 to 20 years ago, but it does appear that maternal inflammation plays a role. 44 Targeting the inflammation is a key to prevention.
There are many factors that can contribute to the development of autism. There is some component of heritability, 45 but again it returns to epigenetics and how those genes are expressed based on exposures. 46 Exposures, such as pesticides and other persistent environmental pollutants, have been implicated as a contributing factor in a genetically susceptible individual. 47 Anything that results in elevated levels of inflammatory mediators in the amniotic fluid can result in an autistic child. Maternal metabolic conditions associated with chronic inflammation like obesity and diabetes also pose an increased risk. 48 Obesity during pregnancy increases the risk of having a child with autism 1.6 times, and diabetes during pregnancy doubles the risk. 48 Higher consumption of maternal dietary fat 49 and low consumption of preconception folate, found in fruits, vegetables, and legumes, 50 are both associated with an increased risk of having a child with autism. This phenomenon is present with other inflammatory conditions as well. Infections like influenza and rubella or any other infection that results in a fever that lasts 7 days or more increase inflammatory mediators. The relative risk for influenza and rubella infection in pregnancy are 4.1 and 3.3, respectively. 47 Another study revealed that maternal influenza doubles the risk, and a fever during pregnancy lasting more than 7 days triples the risk of an autistic child. 44
The Microbiome
Increasingly, we are finding that this inflammatory response is mediated by the intestinal flora, which is selected based on what humans are eating. By eating a plant-based diet, humans select for more favorable bacterial species that actually improve risk factors for metabolic diseases by reducing intestinal inflammation.51-54 This intestinal inflammation also contributes to the development of regressive autism. Some kids with autism are diagnosed relatively early in childhood, while others develop normally until age 18 months or so and then begin to regress. The bacteria that are implicated in these particular cases are Clostridium species, as well as Desulfovibrio. Desulfovibrio is a proteobacteria that reduces sulfate compounds into sulfides. The body produces sulfates from the amino acids cysteine and methionine. This regulation of sulfate may play a significant role in regressive autism, because the sulfide gas produced in the colon is toxic to all systems of the body, but is most toxic to the nervous system. 55 Desulfovibrio also contains a potent endotoxin. One study revealed that Desulfovibrio-derived endotoxins were far better at inducing tumor necrosis factor-α secretion than endotoxins from Escherichia coli and Salmonella. 56 In a study of children with regressive autism, 50% were colonized with Desulfovibrio, but none of the control children were. 57 Desulfovibrio species are also present in higher concentrations in the gut when the subject eats a diet low in fermentable carbohydrate. Fermentable carbohydrates include fructose (found in fruits and vegetables), fructans (found in breads, cereals, and pastas), galactans (found in beans and other legumes), and lactose. 58 These bacteria are being selected based on dietary patterns as well as antimicrobial use.
The proposed mechanism for the development of autism involves immunologic susceptibility that is either genetic or acquired through environmental exposures like diet. This can lead to an in-growth or overgrowth of Desulfovibrio species. This can result in production of a toxin or toxic metabolite, a disease-associated antigen, or utilization of key compounds needed by the host resulting in host tissue damage in the brain either directly or through a disease-related immune response. 57
It is becoming more apparent, however, that the development of regressive autism is not due to the presence or absence of one or a few bacterial species, but by functional alterations in intestinal microbiota. 59 Certainly, the alteration in sulfur metabolism, as described above, is a contributor and modulated by the intestinal tract. In addition, production of some short-chain fatty acids, propionic acid in particular, induces behavioral and functional alterations in the brains of exposed animals. These short-chain fatty acids are the result of anaerobic microbial degradation of carbohydrates. 59 It is also known that some autistic children improve on a gluten- and casein-free diet.59,60 The mechanism behind the improvement is unknown, but it is theorized that there is an alteration in the host–microbe metabolism of certain proteins. Biochemical evidence for this is shown by an altered urinary peptide profile in autistic children when compared to normal controls. 59
Maternal diet and the maternal microbiome play crucial roles in what happens to the fetus and infant. A recent study revealed that an infant’s first meeting with microbes and its first intestinal colonization happens in the womb. It is now known there is a placental microbiome consistent with the maternal oral microbial community. The next meeting with microbes is during birth, and then with breastfeeding. From the moment the placenta starts supplying the infant with nutrients, the microbiome is being developed and that microbiome will determine the health status of the infant. 61 Another recent study revealed that a high-fat diet in pregnancy and during breastfeeding causes a microbial dysbiosis in the infant. This dysbiosis can only partially be corrected by a low-fat diet after weaning. The authors provide evidence to support the theory that the maternal diet contributes to establishment of the fetal microbiota, which, in turn, affects intestinal maintenance and metabolic health. 62 This underscores the importance of maternal periconceptional, prenatal, and postnatal nutrition. Prospective trials examining lifestyle interventions in pregnancy have not borne lower rates of gestational diabetes or fetal macrosomia. However, the dietary interventions did not go far enough.63,64 One study recommended a low glycemic index diet 63 and the other recommended a more plant-based approach; however, dietary adherence was not measured objectively. 64 In addition, neither study measured markers of inflammation. Nevertheless, the importance of improving the health of young people before conception cannot be understated.
The Agricultural–Industrial Complex
According to the USDA’s Center for Nutrition and Promotion, Americans are consuming more food and several hundred more calories per person per day than their counterparts in the late 1950s. In 2000, dietary intake was just less than 2700 calories per person, per day. Approximately 40% of the increased calories are consumed as highly refined grain products. Much of the rest of the increase is in fats and oils and added sugars. In addition, Americans are eating 195 pounds of meat per person per year, which is 57 pounds more than the average annual consumption in the 1950s. We are also eating 4 times as much cheese, as compared to the 1950s. 65 This excessive consumption of refined grains, sweeteners, and animal foods, and the way these foods are produced, are responsible for the epidemic levels of chronic disease in this country. This would never have been possible without the advent of industrial agriculture.
Between 1900 and 1940, government investments in mechanization were made and farmer productivity rose rapidly. It is estimated that the total public investment in agriculture, including marketing assistance, favorable tax policies, credit programs, and commodity programs, in 1940 was $500 billion, compared with $2.5 trillion in 1990 (based on the value of the US dollar in 1992). The purpose of these investments was to provide sufficient, affordable animal products and some basic cash crops to provide starchy staples like bread. 66 American diets shifted accordingly. So much government money has been invested in these cash crops that prices have been artificially pushed down. For instance, the world price for beef has declined from more than $530 for 220 pounds in 1970 to less than $190 for the same amount in 1995. 66 Inexpensive animal foods have driven increased demand for the products. Subsidized crops like corn and soy reenter the food production industry in some way: as oils, sweeteners, fillers, and starches for junk foods, or as animal feed for meat, milk, and egg production. Through federal and state governments, the United States also subsidizes milk production and regulates dairy prices. By boosting prices, the dairy program encourages overproduction. This surplus milk is then given to schools for the school lunch program at extremely low prices.
The survival of any nation rests on its ability to feed its people. If we continue to feed our people this way, our nation will buckle under its own weight. The $3 trillion health care crisis will break us economically, both in terms of the price tag of health care and also via lost productivity from worker presenteeism, absenteeism, and disability. The financial impact of autism, alone, is staggering. It costs nearly $3.2 million dollars to care for one autistic person over his or her lifetime, which adds up to an estimated $35 billion per year. 67 It is incumbent on health care practitioners to help be a part of the solution to this fatal problem.
One novel solution can be borrowed, if you will, from Finland. In 1972, they launched The North Karelia Project as a national program to influence diet and lifestyle behaviors. There were low-cost community interventions implemented, but also food industry and policy changes. One policy change program, the “Dairy to Berry” project, that incentivized farmers make a switch from dairy farming to berry farming. The results were staggering. Finland saw a reduction in coronary heart disease mortality of 73%, a 44% reduction in cancer mortality, and a 49% reduction in all-cause mortality between 1970 and 1995. They also saw an increase in life expectancy for men by 7 years and by 6 years for women. 68 The United States must choose to implement farm policies that are good for the farmer and for the health of the people of this nation. We must choose the health of our land and our people over corporate interests.
Footnotes
Acknowledgements
Presented at Lifestyle Medicine 2014; San Diego, CA; October 19-22, 2014.