
Abstract
This article covers some important concepts and controversies in modern nutritional science. It describes a diet style designed to maximize health, longevity, and disease reversal—foundationally structured on the quality and comprehensive adequacy of nutrients rather than the balance of macronutrients, as is more popular today. I call such a diet, which attempts to optimize micronutrients, a nutritarian diet. I will review a small case series demonstrating typical results in diabetics and some of my clinical observations over the last 25 years treating people with a nutritarian diet, which could be either vegan or flexitarian. I will also discuss health concerns observed from an unsupplemented vegan diet, specifically the risk of depression and later life dementia in individuals with enhanced need for long-chain omega-3 fatty acids.
Americans consume about 55% of calories from refined foods and approximately 30% of calories from animal products . . .
Three Primary Learning Objectives
To understand nutritional considerations in designing the most favorable diet for successfully reversing obesity and type 2 diabetes.
The lifestyle medicine approach versus a drug-centered approach to most effectively and safely treat and reverse diabetes and heart disease.
Understand the potential risks of an unsupplemented low-fat vegan diet, and how to prevent them.
I divide food generally consumed into 4 main categories: produce, whole grains, refined or highly processed foods, and animal products. Americans consume about 55% of calories from refined foods and approximately 30% of calories from animal products, with only about 15% of calories from a combination of whole grains and produce. This small amount of produce, especially greens, mushrooms, onions, seeds, colorful vegetables, and fruits, leads to an overall deficiency in micronutrients, especially antioxidants and phytochemicals necessary for normal health, cellular repair, and immune function.
Using the presence or absence of animal products as the distinguishing characteristic is a narrow and unsatisfactory way to characterize a diet designed to maximize health and disease reversal. A nutritarian diet style, designed to maximally support health and longevity in a diverse population base, has 4 distinguishing characteristics.
It strives to be high in micronutrients per calorie. It achieves this with increased consumption of nutrient-rich plants, such as greens, berries, seeds, and other colored produce.
It strives to be hormonally favorable, avoiding excess hormones that can promote aging and disease, especially insulin and IGF-1.
It strives to be nutritionally adequate, comprehensively, using supplements when necessary to assure optimal levels of vitamin D, vitamin B12, iodine, zinc, eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA), based on dietary history, and when available, blood work.
It strives to avoid food containing toxins, contamination, and infectious agents.
It is well established that modest micronutrient insufficiency is ubiquitous and can lead to DNA damage, mitochondrial decay, and telomere decay. If we classify phytochemicals as a form of micronutrients, because of their relation to immune function, disease protection, and longevity, then we must classify almost all Americans (both vegetarians and meatatarians) as micronutrient deficient, especially regarding micronutrients derived from green vegetables.1-10
I present the equation H = N/C to portray the basic principle that to maximize healthy life expectancy (H) we have to eat a diet rich in micronutrients (N) per calorie (C). My ANDI (Aggregate Nutrient Density Index) is a useful tool to help visualize the high concentration of micronutrients in greens and other colored produce compared with animal products and processed foods. It utilizes over 30 separate nutritional parameters to estimate a food’s overall level of micronutrients per calorie. This has been demonstrated to be effective in increasing the sales and consumption of nutrient-rich produce, in Whole Foods Market.
However, this is not all you need to know to devise a diet with maximal health benefits, because some foods with only a moderate nutrient density have salient features that make them valuable for disease resistance. For example, mushrooms and flax seeds contain powerful anti–breast cancer components, not adequately appreciated in their aggregate nutrient density score, and likewise nuts, though calorie-dense, have cholesterol-lowering and other therapeutic benefits.
Hormonal Favorability: Insulin and Insulin-Like Growth Factor-1 (IGF-1)
Furthermore, we have to consider the second principle of a nutritarian diet—hormonal favorability. It has become increasingly evident that higher levels of IGF-1 are linked to increased early life mortality, higher incidence of cancer, and premature aging, including aging of the brain.11-14 It is also well established that diets with excessive amount of animal protein elevate IGF-1, and that optimally low levels are not achieved until a significant reduction in animal products is maintained in the diet. However, the exact percentage of calories or amount of animal products below which would optimize IGF-1, and whether a higher IGF-1 might be more favorable in the elderly, is yet to be determined.15-17 More details about various protein sources and varying animal protein and plant protein intake to achieve favorable IGF-1 in all decades of life is not the topic of this presentation. However, studies demonstrate that with more than 5% to 10% of calories from animal products IGF-1 can rise significantly. 18
There is also an overwhelming amount of evidence that excessive production of insulin in response to high glycemic foods is disease-promoting and lifespan-shortening. Elevated insulin does not merely increase risk of diabetes and heart disease but has pro-angiogenic and cancer-promoting effects.19-23 For example, in a meta-analysis of 39 studies, a high glycemic load was associated with increased risk of colorectal and endometrial cancers, 21 and a meta-analysis of 10 prospective studies demonstrated a link between higher glycemic load and breast cancer.24,25 Another study demonstrated for every 100 grams of white rice consumed per day, breast cancer risk increased 19%, whereas the same amount of whole grain, brown rice, or beans had almost the direct opposite effect. 26
High glycemic processed foods are so disease-causing, recent research suggests their promotion of heart disease is even more powerful than saturated fats from animal products, a chilling concern considering all the white bread, white rice, and white potato products consumed by populations around the world and in this country. 27 Table 1 provides the glycemic load of common foods.
Glycemic Load of Common Foods 29 .
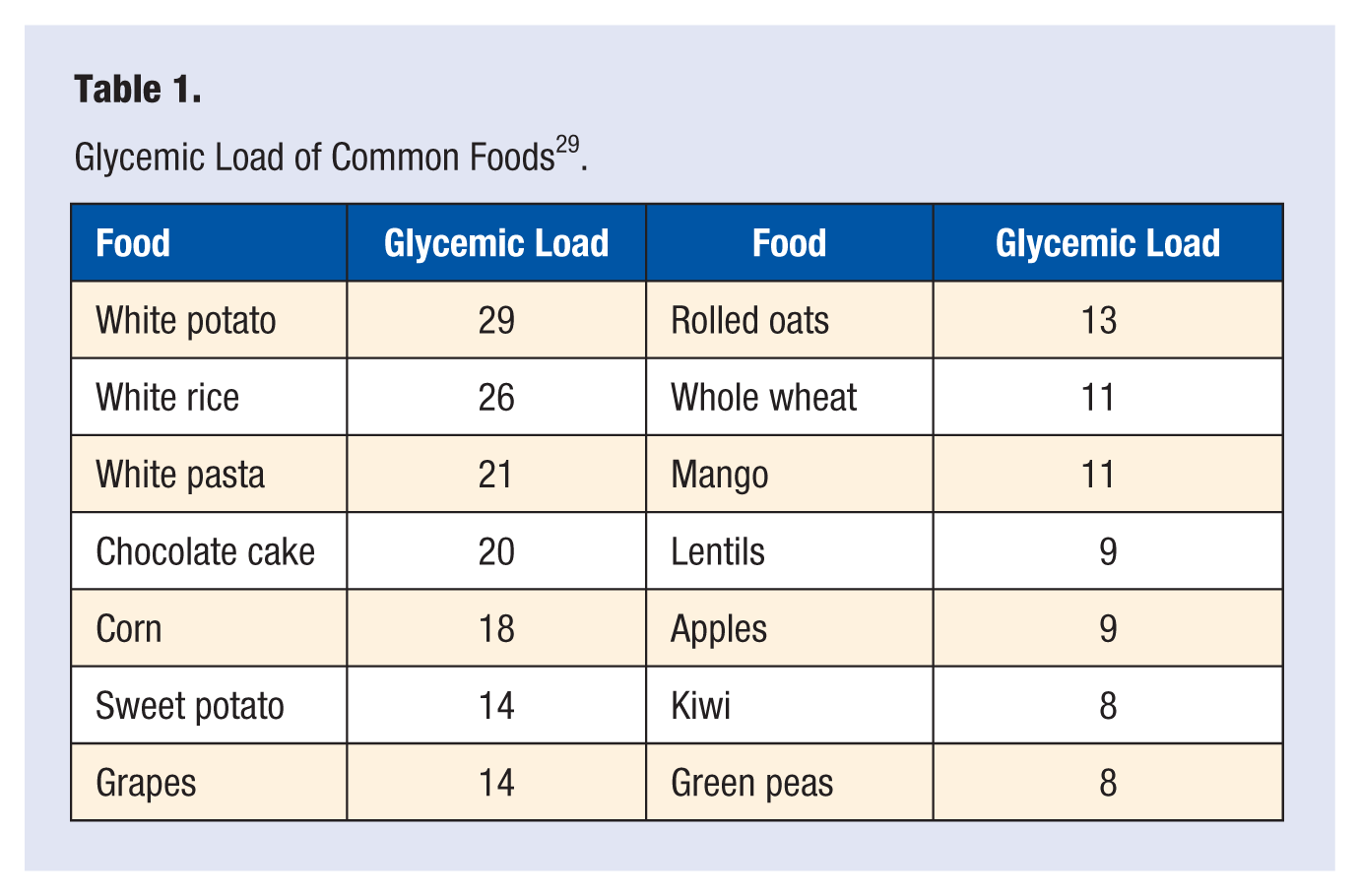
Consider white potatoes as an example of a high glycemic carbohydrate, with a favorable caloric density. The Nurses’ Health Study demonstrated an 18% increased risk of diabetes for each potato eaten daily by overweight women. Notably, the glycemic load of potatoes rather than the added or associated butter or oil was implicated. 30 Ominously, data from the North Carolina Colon Cancer Study, with more than 1000 cases of colon cancer compared against more than 1000 controls, demonstrated a more than 50% increased risk of rectal cancer in those eating 3 potatoes a week compared to those eating 1 potato a week, and more than an 80% increase comparing 5.6 servings a week to 1 serving. 31 Quite shocking findings, but note these heightened risks were only observed for non–whole grains and potatoes, and not for discretionary fat suggesting the association is demonstrating significant glycemic risk, and not merely an association with a dietary pattern or fatty toppings used on a potato. When we observe the association with disease risk becomes more pronounced as body weight and insulin resistance increases, it specifically identifies the potato’s glycemic effect, which becomes a more significant stimulator of excess insulin release as a person’s body weight increases. And because of the fat-promoting effects of insulin, high glycemic foods can make it more difficult for the overweight to lose weight. 32
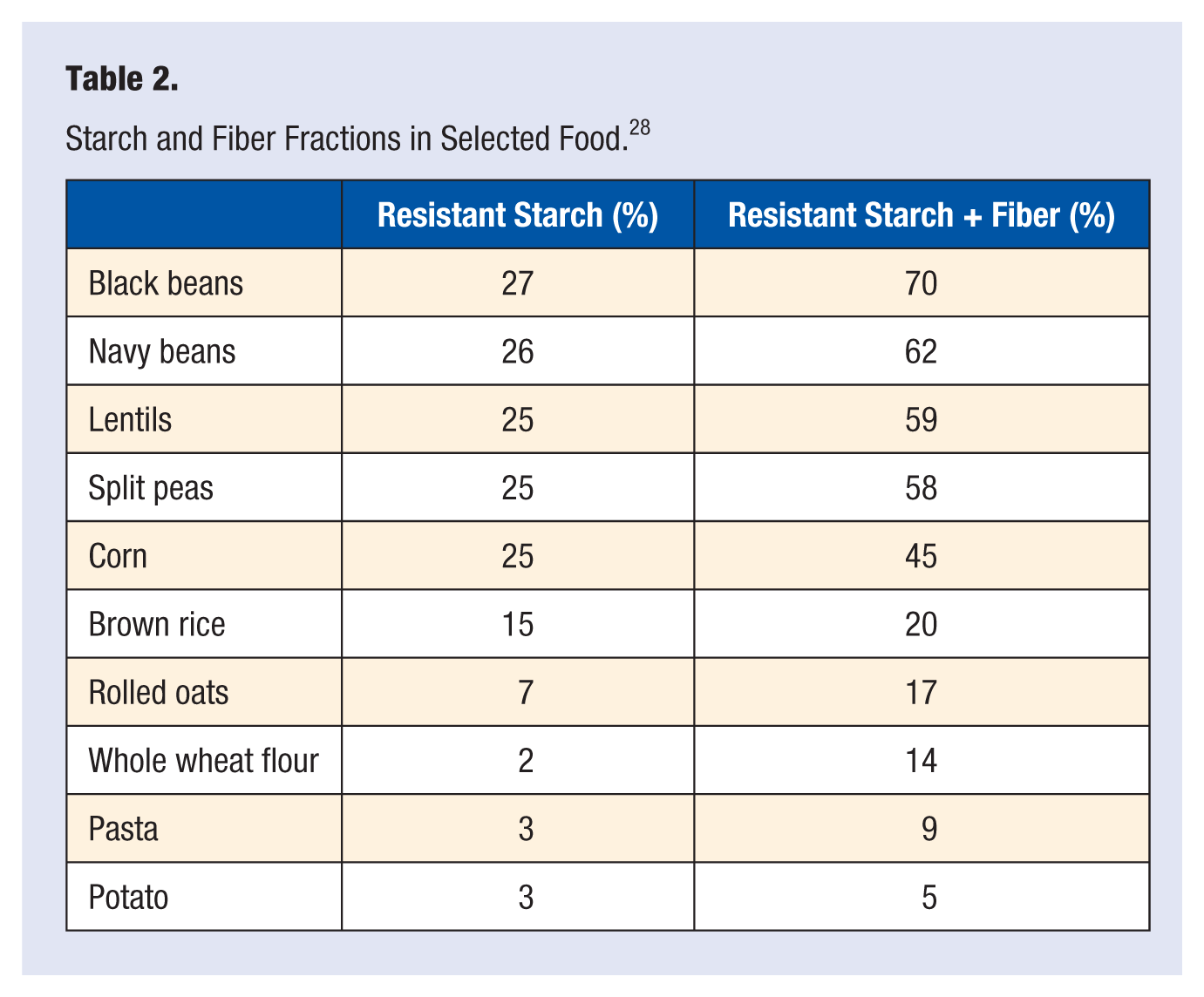
This information becomes clinically relevant when treating overweight diabetics, as meat, sweets, and high glycemic carbohydrates promote unfavorable hormonal influences. We can classify carbohydrate-rich foods on a hierarchal scale based on their nutrient levels, fiber content, and amount of resistant starch. As the amount of fiber and resistant starch increase (see Table 2), more dramatic benefits for the overweight and/or diabetic are noted. Resistant starch is counted as calories on labels and charts, but during digestion, 90% of resistant starch calories are lost, thus acting more like a type of fiber.
Starch and Fiber Fractions in Selected Food. 28
Beans
By considering this hierarchal scale of carbohydrate quality, we can utilize this information to devise a dietary protocol that reduces exposure to the highest glycemic carbohydrates and incorporates more beans, more raw and cooked greens with other low glycemic vegetables, and more nuts and seeds to achieve dramatic glucose favorable benefits for the diabetic, prediabetic, or those with metabolic syndrome. As an example, a 2-group controlled trial encouraged one arm to increase legume intake by 1 cup a day, and then another arm to increase their intake of whole grains by the same amount. A clear benefit occurred for adding more whole grain, but more dramatic benefits occurred for the addition of beans from individual baseline (Table 3). 33
Changes From Baseline Between Whole Grain and Bean Groups 33 .
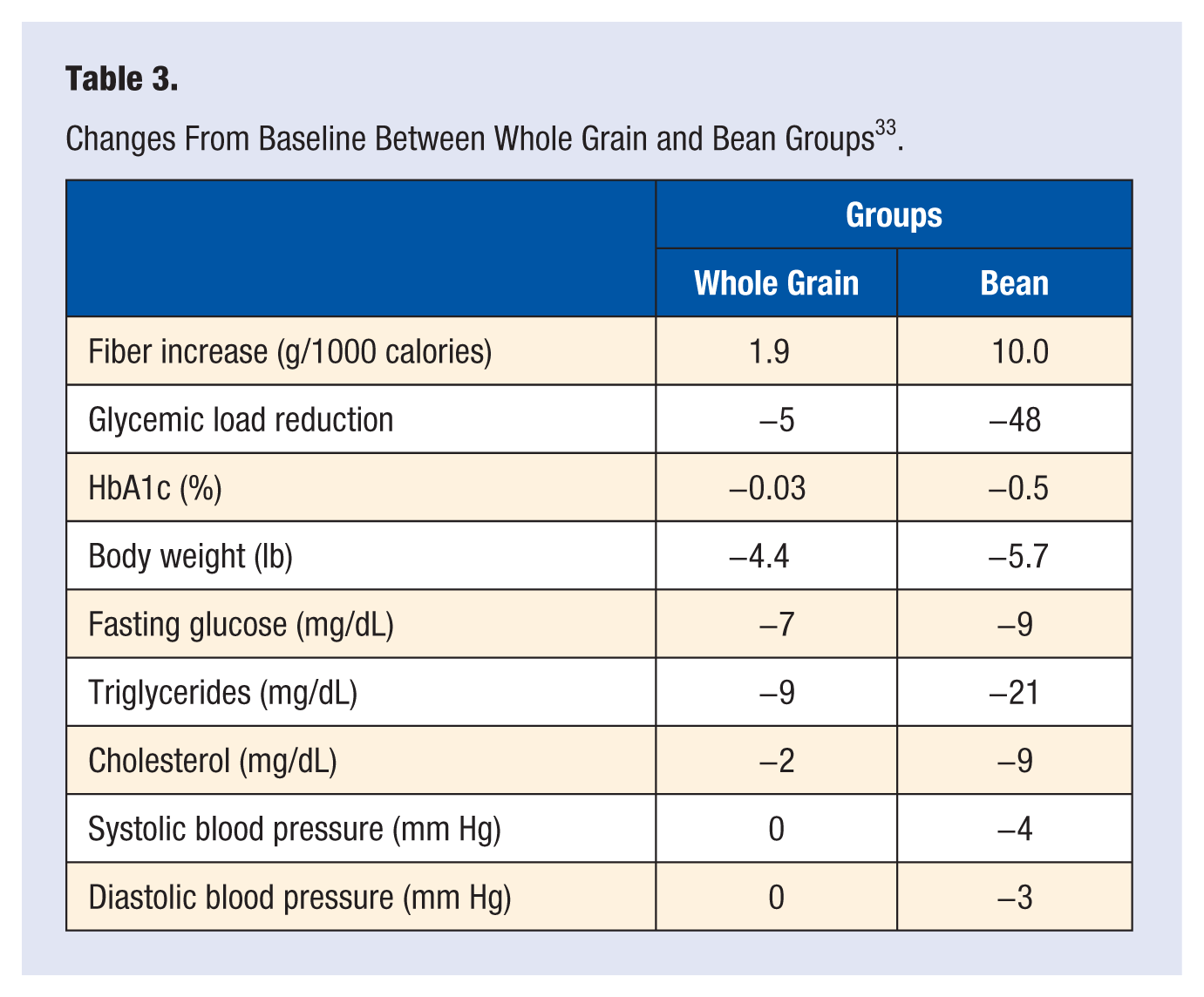
Beans are not merely glycemically favorable themselves, but their fermentation and prebiotic effects lower the glucose absorption from other foods in the diet. These glucose-lowering benefits occur not merely in the meal eaten with the beans but later as well when no beans are eaten. This has been called the “second-meal effect.”34-36 Beans have multiple benefits for favorable glycemic response, weight reduction, and anticancer effects. Across a broad spectrum of different regions and ethnicities, beans/legumes were found to be the most consistent and reliable predictor of longevity. An 8% reduction in death was reported for every 20 grams (2 tablespoons) of beans eaten daily. 37 There are numerous anticancer compounds in beans, nuts, and seeds, including phytic acid and inositol pentakisphosphate, which have been shown in animal studies to inhibit tumor growth, migration, and invasion, and also augment NK (natural killer) cell activity.38-40
Nuts and Seeds: Therapeutic Efficacy in Disease Reversal
Including more calories from nuts and seeds enables one to reduce glycemic calories, further increasing therapeutic potential, leading to further reductions in HbA1c and lipids. 41 Observational studies on this topic demonstrate that those who consume nuts regularly tend to have a lower body mass index (BMI) than nonconsumers and more weight loss compared to equal calories of carbohydrate in the diet.42-44 Interventional studies corroborate these findings. For example, a study demonstrated a 62% greater reduction in BMI and 50% more waist circumference reduction in the group given nuts instead of more carbohydrate.44,45 The main properties of nuts that contribute to weight maintenance are high satiety, increased oxidation of fat, and all of their calories are not accessible for absorption (15% to 20%), increasing stool fat.42-44
The idea that there is some health or therapeutic advantage of extreme fat restriction by excluding seeds and nuts for lowering weight, improving diabetic parameters, or reversing heart disease is not supported by the preponderance of evidence today. Nuts and seeds also effectively lower low-density lipoprotein (LDL) cholesterol. A pooled analysis of 24 (3-8 weeks) interventional trials confirmed an average of 4.9% LDL reduction for 1.5 ounces nuts/day, and a 7.4% reduction for 2.4 ounces. 46 And it is not merely risk factor measurements; the use of nuts and seeds is associated with a reduced risk of cardiovascular events and overall mortality. The best and largest cohort studies in nutritional epidemiology, such as the Adventist Health Study, the Iowa Women’s Health Study, the Nurses’ Health Study, the Physicians’ Health Study, and the CARE Study all confirm that eating nuts and/or seeds is associated with a 30% to 50% decreased risk of coronary artery disease (CAD) death, primarily sudden cardiac death, and dramatic increases in all-cause mortality. For example, in the Physicians Health Study, which followed 21 454 male physicians for 17 years, the most dramatic relationship between any food and survival was the reduced mortality associated with nut consumption 2 or more times per week (compared to no nuts or seeds). In this study, nuts and seeds had antiarrhythmic and antiseizure effects—associated with a 60% reduction in sudden cardiac death. 47 These benefits are not limited to meat-eating populations; significant lifespan benefits are seen in nut-eating vegans as well. In the oldest Adventists (over 84), a 39% decrease in coronary heart disease death was demonstrated comparing those with higher (5 times weekly) to low nut and/or seed intake.48,49
The Adventist Health Study confirmed that the consumption of nuts was one of the most dramatic features, accounting for extended lifespan benefits, a variable producing a greater benefit than vegan status. The graph on the life expectancy in Adventist men is reproduced in Figure 1. 50 Each column is displayed as expected age at death at low and high risk, assuming medium risk for all columns to the right, and the same risk (low or high) for all columns to the left. For example, for nuts, Adventists who are vegetarian, exercise regularly, and eat 5 servings of nuts/week can be expected to live to age 87, assuming medium-range risk values for BMI and smoking. Adventists who are not vegetarian, do not exercise regularly, and do not eat nuts regularly would be expected to live to age 79.2. These data suggest that these variables cumulatively add 7.8 years of life expectancy. Nuts alone account for a 5.6 year variance in lifespan in the Adventist Health Study data. 48 These data also mean that flexitarians who ate nuts and seeds generally lived longer than vegans, who excluded them.
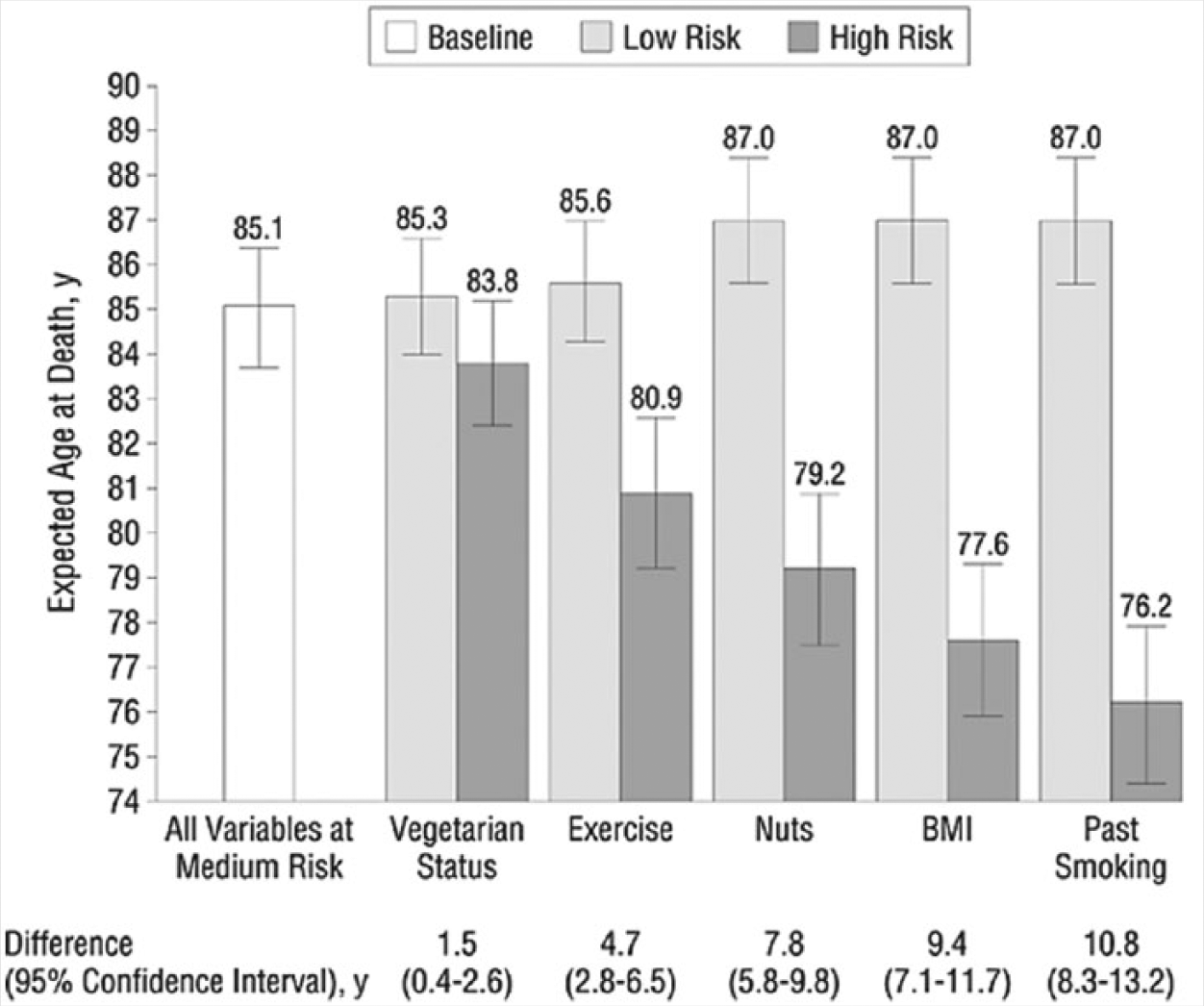
Expected Ages at Death (95% Confidence Intervals) in Men With Jointly High- or Low-Risk Values for the Risk Factor in a Particular Column and Those to Its Left (Other Variables at Medium-Risk Values).
Multiple potential mechanisms exist for these dramatic lifespan benefits of nuts and seeds, including the effects of polyphenols, sterols, vitamin E fragments, nitric oxide promoters, cancer inhibitors, and enhanced micronutrient absorption of phytonutrients from other foods (from having nuts and seeds in the meal). In the past 25 years of my treating thousands of patients with high blood pressure, diabetes, and advanced heart disease, I have observed dramatic results utilizing these principles. Excluding nuts and seeds in favor of more low- or mid-quality carbohydrates is undoubtedly unfavorable for those medically or metabolically challenged with chronic disease, and would presumably increase mortality risk. For maximum benefits they should be incorporated into meals rather than being used as a snack. If a rare individual uses them excessively, and not for replacement calories, then their use would need to be curtailed.
Walnuts, hemp seeds, chia seeds, and flax seeds are those nuts and seeds with the most favorable omega-3 content. Walnuts, in particular, have been associated with enhanced cholesterol efflux, increased vessel elasticity and endothelial function, decreased LDL and triglycerides, increased high-density lipoprotein, lower particle number, lower serum glucose, reduced oxidant load on brain cells, and improved interneuronal signaling and neurogenesis.51,52 They are a valuable part of a dietary protocol designed to reverse heart disease.
Lightening the Absorptive Rate of Calories Into the Bloodstream
The glycemic index or load considers the rate at which glucose builds up in the bloodstream over time. The more rapid and concentrated the elevation of glucose in the blood, the more significant the risk. The same can be said of fat entering the blood quickly (Figure 2). Whereas oils and even concentrated animal fats can enter the bloodstream rapidly, the fat content of seeds and nuts is absorbed over several hours, allowing the calories to be burned for energy rather than stored as fat, which can delay hunger and more effectively reduce calorie demand signaling.
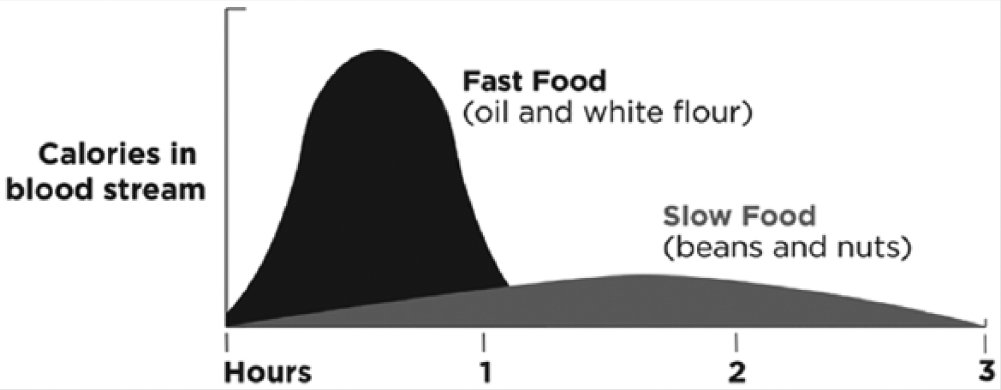
Speed of Absorption of Calories in Fast Food Versus Slow Food.
I propose that the vast majority of informed nutritional scientists and physicians who have no predetermined agenda or bias, after reviewing the preponderance of evidence on these issues, would be forced to agree on the following 3 dietary principles:
Vegetables, beans, seeds, nuts, fruits, are good for you.
Excessive amounts of animal products increase chronic disease risk.
Refined carbohydrates promote chronic disease and lead to overweight and obesity.
Consuming more greens, mushrooms, onions, tomatoes, beans, nuts, and seeds, to replace lower quality carbohydrates, results in a dramatic lowering of glycemic load and diabetic and cardiovascular parameters. For example, in a trial of 117 diabetics randomized to eat an equal caloric amount of nuts daily, or muffins or both, the nut group showed dramatic improvement in both glycemic control and serum lipids, including improvement in apoproteins. 41 Utilizing these dietary principles, we conducted a small pilot study of 11 poorly controlled diabetics, resulting in them earning nondiabetic parameters after following this portfolio of dietary recommendations for a mean of 7 months. 53 Of note was the 27-point reduction in systolic blood pressure, while blood pressure medications were lowered by more than 50%. Plus, those remaining on blood pressure medications, and the one person still left on metformin, were only on medications, because their primary physicians did not taper and discontinue appropriately in accordance with recent guidelines for medication use. The aggressiveness of this dietary approach enables patients to reduce and eventually eliminate dependence on diabetic medications, blood pressure medications, and statin drugs. The elimination of medication then further improves the results and sustainability, as many medications in use today contribute to metabolic derangement and lead to weight gain. The most metabolically unfavorable medications include insulin, sulfonylureas, β-blockers, and statins. For example, on February 6, 2008, the National Heart, Lung, and Blood Institute stopped the ACCORD Study (Action to Control Cardiovascular Risk in Diabetes) as the results showed that intensive treatment of diabetics to better control their fasting glucose increased the risk of dying compared to those patients treated less aggressively. 54 This demonstrated the harm of increasing dependence on medications, which cause weight gain as they drive the failing β-cells to produce insulin, with the goal to reduce glucose. Getting better short-term glucose numbers results in more β-cell death and more insulin resistance leading to long-term enhanced morbidity and mortality.
A Nutritarian Diet Features
Large green salads with seed-nut-based dressings
Bean soups with carrot/tomato juice and cruciferous vegetables
Steamed or wokked green vegetables, onions, and mushrooms
Animal products limited to 0 to 3 small servings per week
No dairy, white flour, white rice
Remove all processed foods, cold cereals, and sweets
No sweeteners, except fruit and limited unsulfured dried fruit
Carbohydrate with high nutritional quality such as peas, squashes, lentils, and intact whole grains
Use of protective foods, such as walnuts, mushrooms, onions, berries, and seeds
Weight Loss and Cardiovascular Benefits That Are Permanent
I have observed for more than 20 years that a diet designed around natural plant foods with the liberal use of greens, nuts, and beans has resulted in long-term sustained weight loss in thousands of overweight individuals. We surveyed 768 of these people and tracked a reduction in their caloric drive and addictive sensations that drove overeating behavior in their past. 55 Those most adherent to the program had the most modified reduction in hunger. The interesting finding was that it took a significant time (4-6 months) before their food preferences changed, but the majority became satisfied with the enjoyment of their new eating style compared to their prior standard diet. It became their permanently adopted lifestyle not a short-term diet (Table 4).
Changes From Baseline in High Nutrient Density Diet. 53
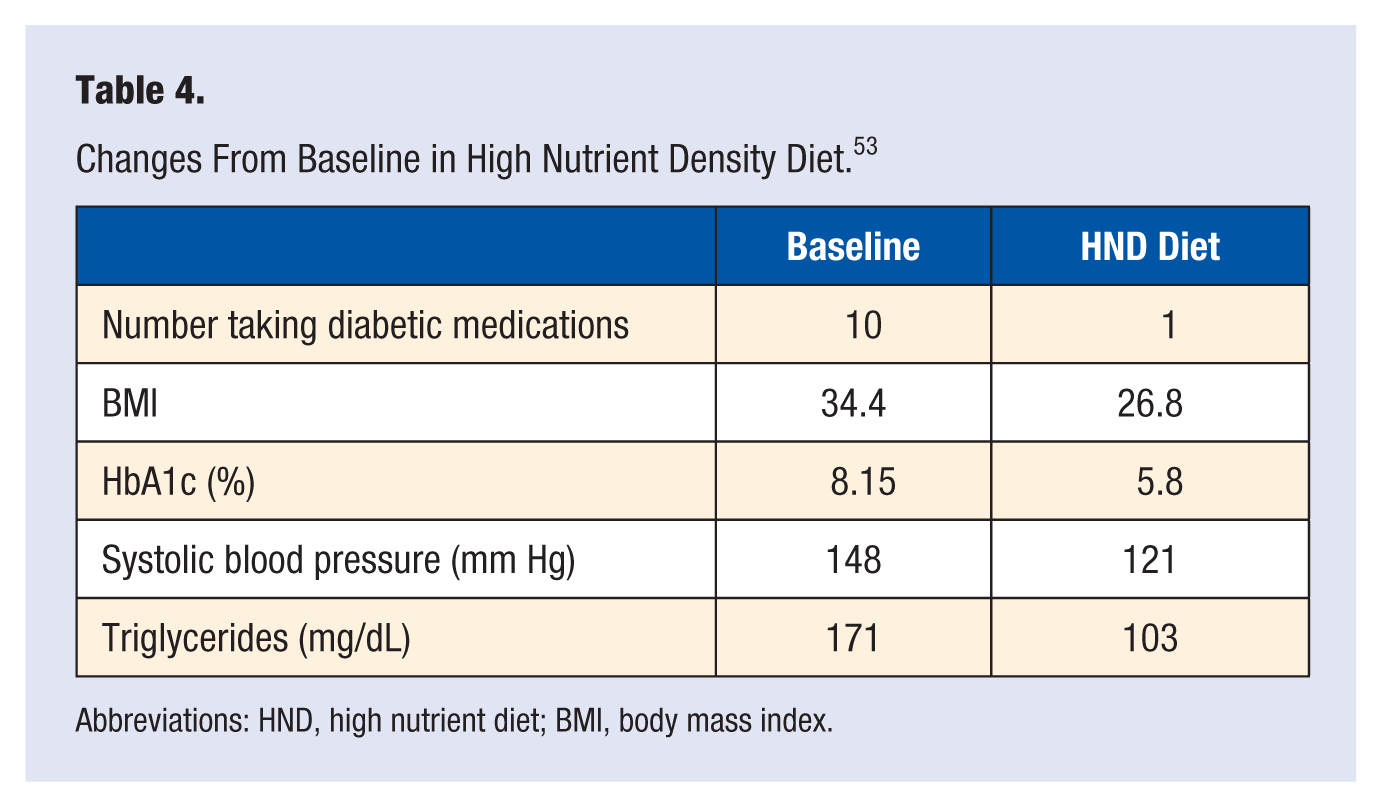
Abbreviations: HND, high nutrient diet; BMI, body mass index.
The potential of this program to reverse advanced heart disease and diabetes is also demonstrated not merely by the thousands of clinical disease reversals but by looking at some case histories of the most severely ill individuals. A good example is Ronnie from Texas, who had re-occlusion and chest pain 4 years after coronary artery bypass surgery (Table 5). He then underwent triple angioplasty, only to experience restenosis within a few months, leaving him homebound. Ronnie has been totally free of heart disease and all medication use since.
Nutritarian Diet Case Study: Ronnie From Texas.
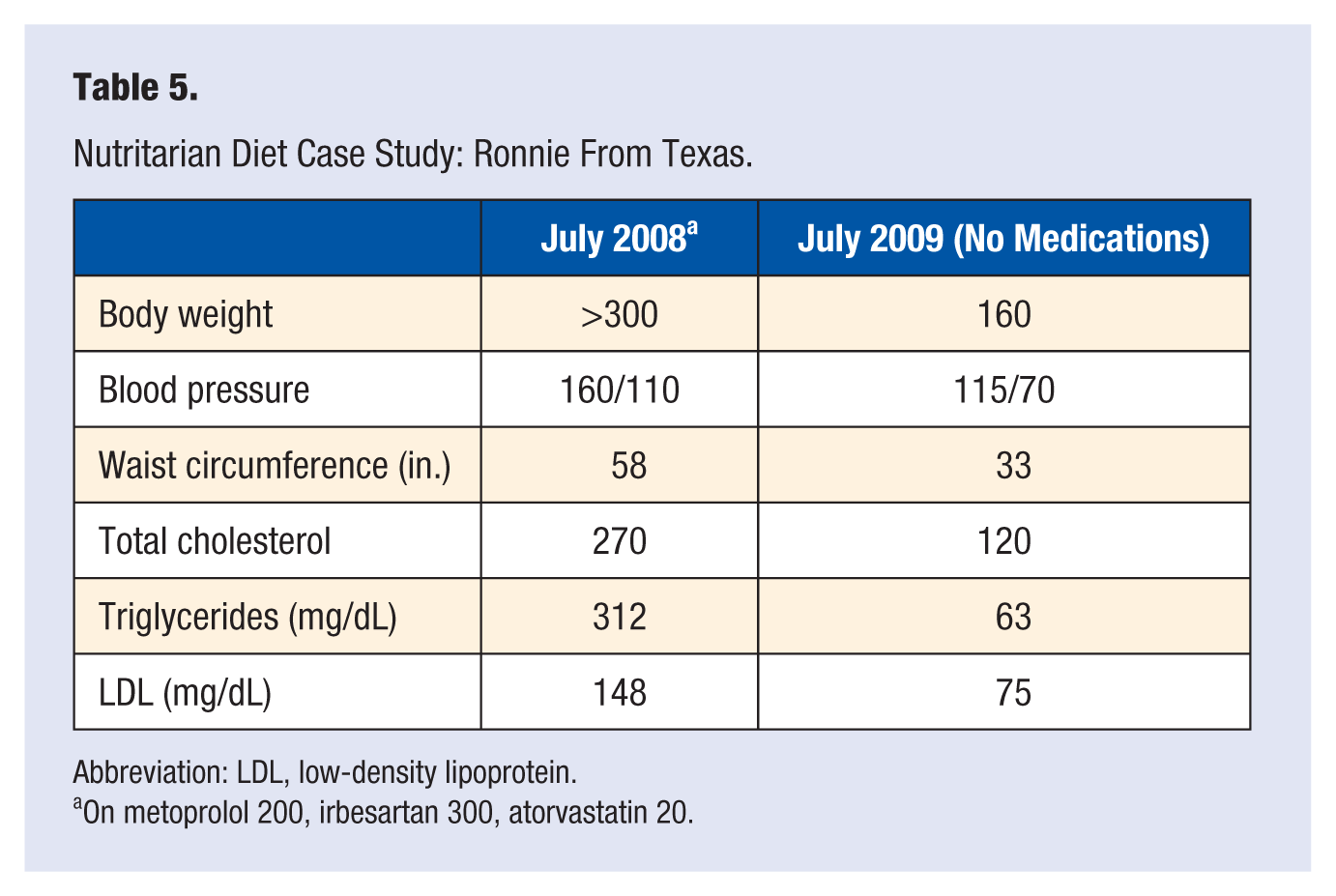
Abbreviation: LDL, low-density lipoprotein.
On metoprolol 200, irbesartan 300, atorvastatin 20.
Similarly, Julia from New Jersey had 5 angioplasty procedures in 3 years and 3 heart attacks in a 3-month period leaving her a cardiac cripple in a wheelchair. She was unable to care for herself, and she was on 10 medications for her heart and high blood pressure. She lost 105 pounds within a year and requires no medications. Today, she dances, shops, takes exercise class, gardens, and has a normal life. The reversal from advanced coronary occasions include patients who presented with unstable angina (at rest) refusing surgical and procedural interventions that still made complete recoveries in a relatively rapid amount of time. Some of these cases with advanced CAD are people who have been followed by me for more than 20 years, who are now into their 90s, with no reoccurrence of CAD. None of them excluded nuts or seeds.
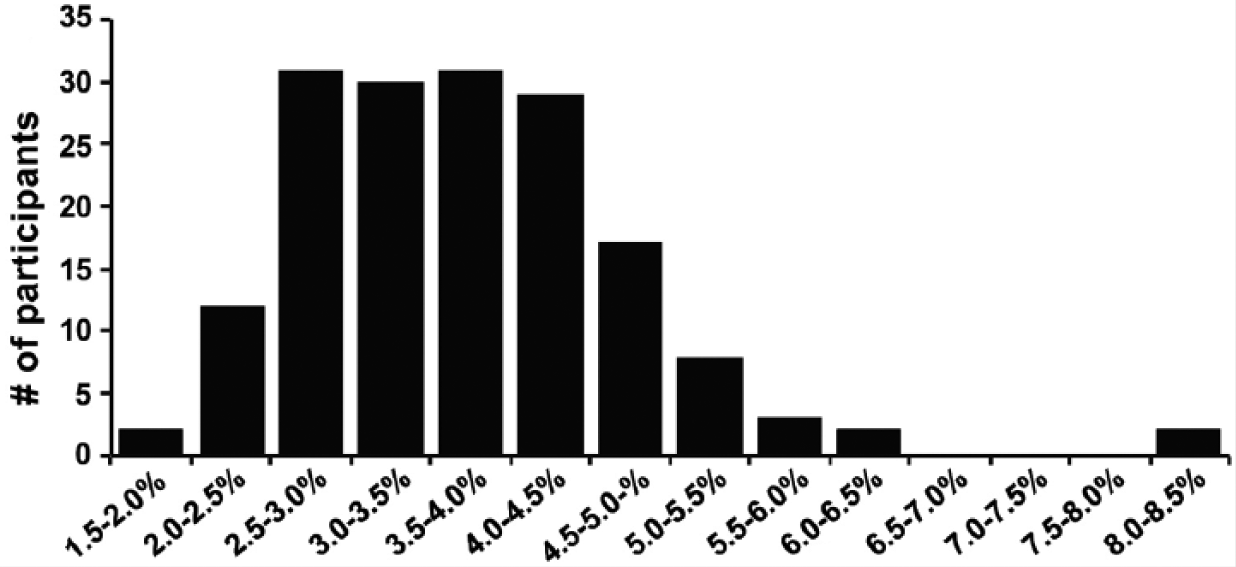
A recent survey of individuals following a nutritarian diet for multiple years gave the following uncorroborated, self-reported results for weight loss. HIPPA-compliant chart review is presently in process by researchers to corroborate the data. Although this data is not ready for peer-review publication, the results speak loudly about the efficacy of this approach (Figure 3).
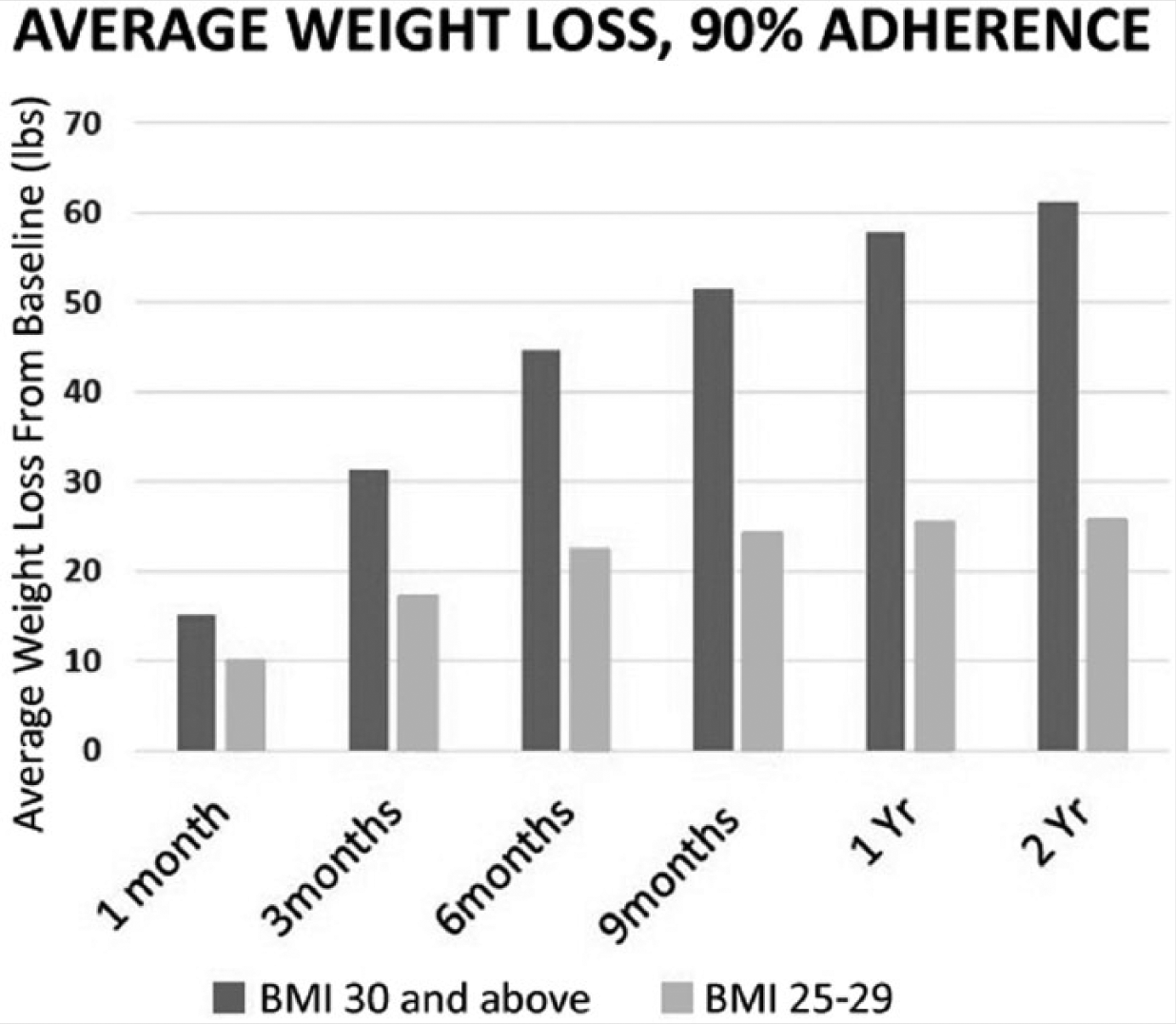
Self-Reported Average Weight Loss Following a 2-Year Nutritarian Diet.
Preventing Dementia and Preventing and Treating Depression
An important concern with following a low-fat vegan diet for therapeutic benefits is the potential for risk of depression and dementia from fatty acid deficiency, especially from chronically low EPA and DHA. More than a dozen epidemiological studies have reported that reduced levels of long-chain omega-3 fatty acids are associated with increased risk for age-related cognitive decline or dementia such as Alzheimer’s disease.56-59 DHA promotes neurogenesis and improved cognition. Not only does DHA, in animal models, prevent amyloid accumulation, but clinical trials show increased brain shrinkage with aging in those with lower blood levels of DHA evaluated 8 years later after DHA measurements. 60 The hippocampus area plays an important role in memory and usually begins to atrophy before symptoms of Alzheimer’s appears, and was particularly vulnerable to this shrinkage associated with low omega-3 index (3.4% compared to 7.5%).
This is particularly concerning considering the large number of unsupplemented vegans that demonstrate deficiency as measured by the DHA–EPA omega-3 index (Figure 4). 61 In this study, 166 healthy vegans showed a wide range in DHA–EPA index, which did not correlate with the amount of short-chain omega-3 intake. That means more ALA from flax seeds and walnuts did not translate into higher levels of EPA and DHA, suggesting that the major variation was primarily due to genetic differences in conversion enzymes. A significant percentage had levels below 3, suggesting serious risk of later life brain compromise.
Omega-3 Index in Vegans.
Omega-3 Index in Vegans
My more than 20 years of clinical experience treating vegans who have some failure to thrive on a vegan diet has repeatedly demonstrated a proportion whose lack of DHA and EPA resulted in an episode of depression or anxiolytic depression. These findings are consistent with a meta-analysis demonstrating patients with depression commonly have lower EPA and DHA levels.62-64 DHA deficiencies in depressed patients relative to healthy controls is consistent with impaired peroxisome function linked to anxiety and depression, and the low omega-3 fatty acid status commonly observed in patients with MDD (major depressive disorder) may reduce the effectiveness of selective serotonin reuptake inhibitors (SSRIs).65,66
Low 25(OH)D levels can also exacerbate these risks of dementia and depression and have been associated with diminished global cognitive function and greater decline over a 4-year period. In this study, those with 25(OH)D above 30 ng/mL showed insignificant decline, 20 to 29 moderate decline, and below 20 severe decline. 67 These findings were matched almost perfectly in a more recent study as well. 68 It is important to pay attention to all of these factors (because of the varied needs of individuals) to assure those counting on our dietary advice are not left with some irreversible loss of memory and brain function. I see many patients eating healthfully, following the advice of leaders in this community, with this constellation of risks.
Zinc levels and needs can also vary among individuals with some people requiring more than is biologically accessible through a vegan diet. A meta-analysis of 17 studies measuring zinc levels demonstrated zinc concentration averaged 1.85 µmol/L lower in depressed subjects versus controls, and greater depression severity was associated with greater relative zinc deficiency. 69 The research also corroborates my clinical experience that women are more susceptible to depression from low and borderline zinc intake compared to men. 70 I have found that supplemental zinc added to the antidepression protocol has been extremely effective, especially in speeding up the response to therapy and ameliorating anxiety associated with the depression or anxiolytic depression. Some studies do corroborate this experience.71,72
My protocol to treat depressed individuals includes the following:
Morning light therapy
Zinc supplementation
Saffron
Exercise
EPA and DHA from fish oil or algae (vegan source)
A nutritarian diet (high vegetable intake), including avoidance of refined and high glycemic carbohydrates
Since many of these treated patients were relatively SSRI-resistant, using the extra zinc and EPA and DHA became lifesaving for them. The sensitivity to SSRI-resistant and partially resistant patients to long-chain omega-3 has also been noted in clinical trials. 73 This study demonstrated symptom remission in 40% of those treated with low-dose fish oils and 100% symptom remission using high-dose fish oils among SSRI-resistant adolescents, although the study only had 7 people in each group. Nevertheless, it is consistent with what I have observed in my practice hundreds of times over the past 25 years.
Understanding Failure to Thrive in a Small Percentage of Vegans
A number of critical trials have confirmed the benefits of dietary supplementation with omega-3 fatty acids not only in several psychiatric conditions but also in inflammatory, autoimmune, and neurodegenerative diseases. Unique to my clinical experience is observing severely deficient levels of DHA (testing almost zero) on a small number of long-term vegans and near vegans who developed Parkinson’s disease. It is possible that this long-standing severe omega-3 deficiency sensitized their brain cells to some type of toxic exposure as is hinted at by animal trials looking at this issue.74-76
It is unfortunate, but understandable, that many people have been turned away from a vegan diet, and go back to eating lots of meat and fish again, when they develop emotional disorders or other symptoms. However, the most unfortunate part is they too often swing back to the other extreme, encouraged to consume a diet too high in animal products, which has a new constellation of risks, instead of understanding their deficiencies and repairing them conservatively.
Although this presentation only touches on some main concerns, it has become apparent from my clinical experience that an unsupplemented low-fat vegan diet should ignite a spark of caution; it is not natural to our genetic heritage, and has never been pursued for generations. Its promotion as the perfect diet for all can result in failure to thrive in children, can be unsafe for pregnancy and nursing, increase risk needlessly for some patients with advanced heart disease, as well as increase risk for depression and later life dementia.
We must always err on the side of caution when we have a framework of controversy or inadequate definitive studies. Very little in the world of nutritional science is known with 100% certainty, so we need to consider the preponderance of the evidence, within a conservative framework, along with broad clinical experience. My 25 years of a very busy clinical practice catering to this population of vegans and health seekers may place a different light on some of these issues, and I have communicated with other practitioners with similar practices, which have reported similar or identical findings. It is not merely B12, and maybe iodine from not using salt or seaweed and seafood, but we need to be aware that some may even require more amino acids, especially taurine and carnitine, especially as protein assimilation diminishes with aging. Our loyalty must always be to the patient, to assure their outcome is favorable, not a dietary position or philosophy. The open communication and shared experiences of participants in this conference are an important part of advancing the science of lifestyle medicine.
Footnotes
Authors’ Note
This article is based on a presentation made at Lifestyle Medicine 2014; San Diego, CA; October 19-22, 2014