
Abstract
Traffic crashes are the leading cause of death among teens. Health care providers have an opportunity to address what works to keep teens safe on the road during the patient visit. An online survey was conducted of 1088 health care providers who saw patients at or near driving age. The survey assessed which road safety topics were discussed and which types of educational products were used most often. Family and general practice physicians represented 44.3% of the sample, followed by pediatricians (22.5%), nurse practitioners (17.6%), and internists (15.5%). Nearly all respondents (92.9%) reported addressing one or more driving safety factors (seat belt use, nighttime driving, fatigue, teen passengers, alcohol/drug use, speeding/reckless driving, and cell phone use/texting) with adolescent patients and/or their parents. Seat belt use was reported more often (83.7%) than other topics. The use of parent–teen driving agreements, a known effective intervention, was reported by less than 10% of respondents. Since health care providers expressed interest in receiving written resource materials, distribution of parent–teen driving agreements to health care providers might encourage greater uptake and use of this effective intervention.
Keywords
‘Motor vehicle crashes are the leading cause of death among youth in the United States.’
Motor vehicle crashes are the leading cause of death among youth in the United States. 1 During 2012, 1875 young drivers aged 15 to 20 years died, and an estimated 184 000 were injured in motor vehicle crashes. 2 The public health burden is large but there are known, effective strategies to prevent these deaths. For example, eliminating speeding, alcohol-impaired driving, and cell phone use/texting while driving will prevent crashes; seat belt use will prevent injury once a crash has occurred.
Health care providers who care for patients at this age have an opportunity to address motor vehicle safety and discuss, with both patients and their parents, what works to keep new drivers safe on the road. However, there is limited research that explores the counseling behaviors of health care providers regarding teen driving safety, or whether this counseling is effective in improving teen safety behaviors. A study by Campbell et al demonstrated that a sample of Connecticut physicians counseled teens on some driver safety topics (seat belts and alcohol) and not others (parent–teen driving agreements). 3 And in a national study, Weiss et al documented how often physicians reported discussing a more comprehensive list of safety factors, and their attitudes about the role of physicians in teen driver safety. 4 Neither the Campbell nor Weiss studies sought to evaluate the effectiveness of health care provider counseling on teen driver behaviors. In a study designed to assess counseling effectiveness, Leverence et al reported that a 2- to 3-minute brief motivational counseling intervention did not result in an improvement in seat belt or bicycle helmet use among 11 to 24 year olds. 5
Provider counseling has been shown to be effective in some areas of injury prevention and not others. For example, in a systematic review of 22 randomized controlled trials, DiGuiseppi and Roberts found that counseling in a clinical setting was effective at increasing restraint use, smoke alarm ownership, and maintaining a safe hot water temperature, but not effective for increasing bicycle helmet use or practices designed to protect young children in the home. 6 An earlier review of unintentional injury prevention counseling in the clinical setting that included literature from 1964 to 1991 found that 18 of 20 eligible studies had positive effects, although not all studies demonstrated declines in injury among children. 7
The American Academy of Pediatrics recommends anticipatory guidance by pediatricians on injury prevention topics for infants, children, and adolescents. Traffic safety topics recommended for adolescent patients include seat belt use, drug and alcohol-impaired crashes, distracted driving, cell phone use, texting while driving, speeding, reckless driving, graduated driver licensing (GDL) laws, limiting nighttime driving, teen passenger restrictions, and teen–parent written agreements.8,9
We have incomplete information about the current counseling practices of providers in the area of teen driver safety, or what circumstances make this counseling as effective as possible. To add to the knowledge base in this area, the purposes of this national study were to explore which driving-related topics health care providers addressed with their patients at or near driving age, describe provider characteristics associated with counseling practices, identify the resources providers used when educating patients about teen driver safety, and ascertain the type(s) of teen driving resources providers would be interested in receiving.
Methods
This report examines data from the 2010 DocStyles survey. DocStyles, a Web-based survey conducted in July 2010 by Porter Novelli, used a main sample of primary care physicians and additional samples of other specialties. The physician sample (n = 1250, including 1000 primary care providers and 250 pediatricians) was taken from the opt-in Epocrates Honors Panel of over 168 000 verified medical practitioners. Health care providers were invited to participate in market research if they made any Epocrates purchases, used Epocrates clinical software, registered any of their Epocrates products, and through limited Web-based advertising. Epocrates randomly selected a sample of physicians from their database to be invited to participate in the DocStyles survey. The physician sample was drawn to match American Medical Association master file proportions for age, gender, and US region. Nurse practitioners (n = 254) were drawn from the Epocrates Allied Health Panel. To be invited to participate in the survey, physicians and nurse practitioners were required to practice in the United States, have practiced for at least 3 years, actively see patients, and work in an individual, group, or hospital practice. Respondents were paid an honorarium of $40 to $60 for completing the survey. Respondents in these analyses were family and general practice physicians, pediatricians, internists, and nurse practitioners who saw patients at or near driving age (N = 1088). Response rates by specialty were 52.6% for nurse practitioners, 51.4% for pediatricians, and 45.2% for primary care physicians (including internists and family/general practice physicians). No information was available for nonresponders.
In order to better understand the teen driving counseling behaviors of health care providers, this report focused on responses to 3 questions: (1) Which of the following topics did you address with adolescent patients at or near driving age and/or with their parents, either through discussion or with a handout? Respondents could select one or more responses (seat belt use, alcohol/drug use while driving, speeding and/or reckless driving, cellphone use and/or texting while driving, driving with teen passengers, nighttime driving, state GDL law, driving while fatigued, other, none of these). (2) Which of the following resources do you currently use when educating adolescents and/or parents on teen driving? Respondents could select one or more responses (posters, video, written materials [ie, pamphlets, brochures], parent–teen driving contract/agreement, other, none of these). (3) Which of the following free resources about teen driving would you be interested in receiving? Responses mirrored question 2 (posters, video, written materials [ie, pamphlets, brochures], parent–teen driving contract/agreement, other, none of these). All analyses were conducted using SAS version 9.2 (SAS Institute Inc, Cary, NC). We calculated proportions and used Fisher’s exact test to assess associations between variables. For all analyses, P values <.05 were considered statistically significant.
Results
Fifty-five percent of respondents were male, 70.0% were between the ages of 35 and 54 years, and the majority (75.9%) were white. By specialty, family and general practice physicians represented 44.3% of the sample, followed by pediatricians (22.5%), nurse practitioners (17.6%), and internists (15.5%). Nearly all respondents (92.9%) reported addressing one or more driver safety topics with adolescent patients and/or their parents. This held true regardless of provider gender, age group, race/ethnicity, and specialty (Table 1).
Demographic Characteristics of Respondents, DocStyles Survey, 2010.
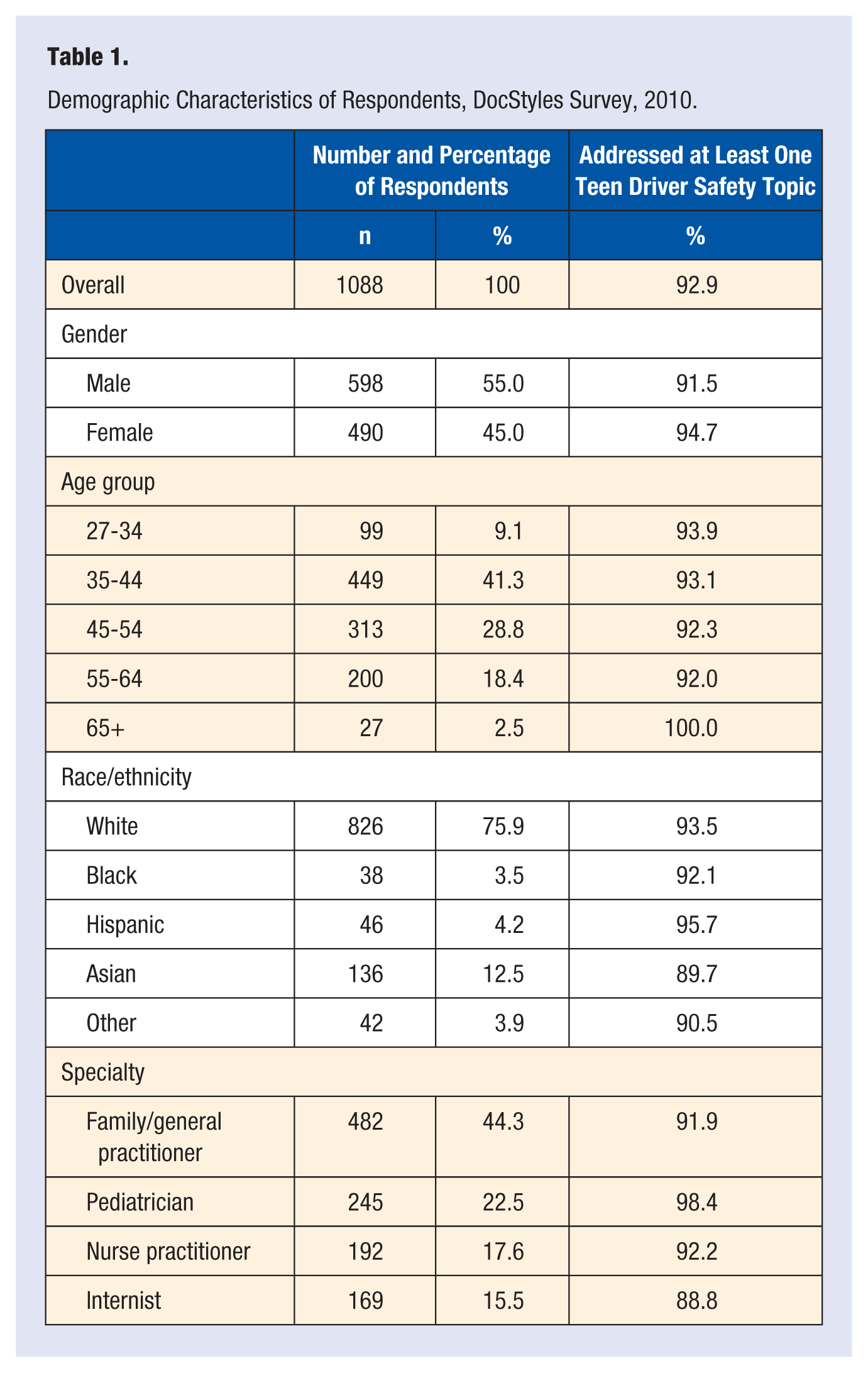
Differences by provider race/ethnicity were small. Asians reported counseling on at least one driver safety topic less frequently than other specialties, but the difference between the lowest (Asians 89.7%) and the highest (Hispanics 95.7%) group was not significant (P = .3654). However, differences by specialty were statistically significant; internists were lowest at 88.9% compared with pediatricians at 98.4% (P < .0001).
Seat belt use was reported more often (83.7%) than other driver safety topics, followed by alcohol/drug use (79.5%), cellphone use/texting (73.9%), speeding (51.5%), and driving with teen passengers (41.2%; Table 2). Pediatricians reported addressing these topics more often than other specialties. For example, 90.6% of pediatricians addressed alcohol/drug use while driving compared with 79.7% of nurse practitioners, 76.3% of family/general practice physicians, and 72.2% of internists. Driving with teen passengers and nighttime driving, well-documented risk factors for teen crashes, were addressed by less than half the respondents (41.2% teen passengers, 19.6% nighttime driving). Driving with teen passengers was addressed most often by pediatricians (51.0%), while nighttime driving was addressed most often by nurse practitioners (27.1%; Table 2).
Topics Addressed by Provider Specialty, DocStyles, 2010.
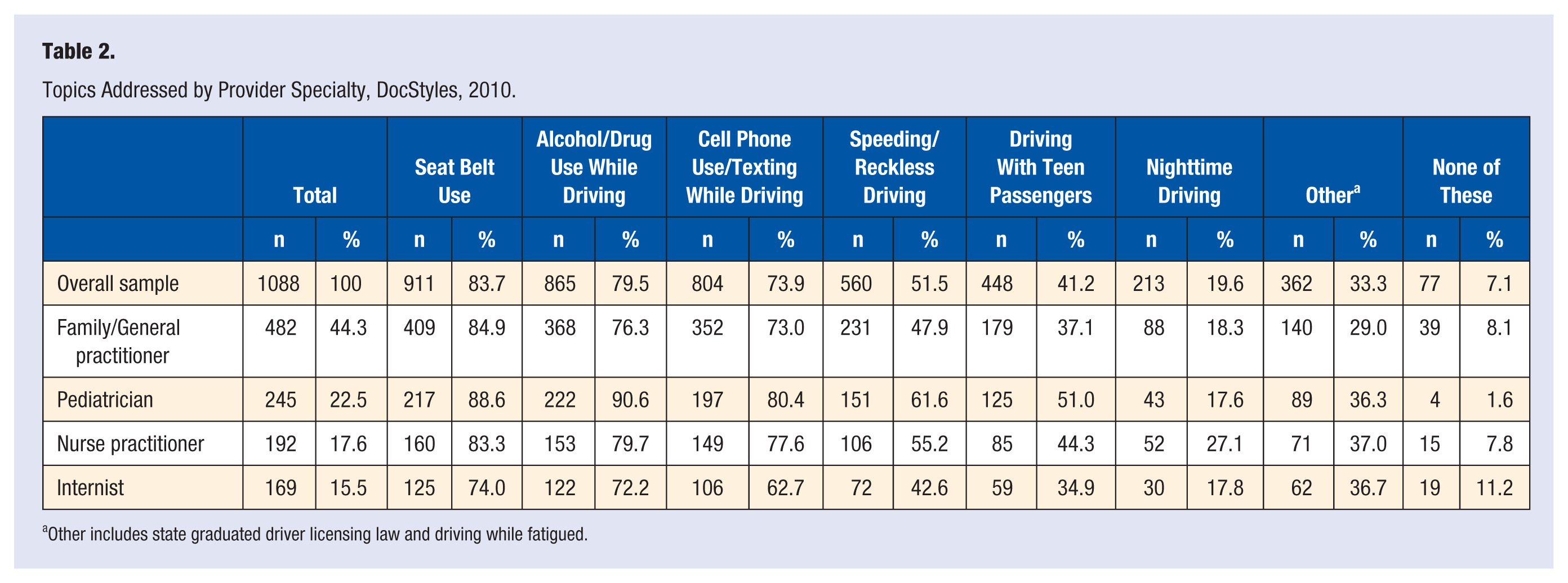
Other includes state graduated driver licensing law and driving while fatigued.
Educational resources were infrequently used by health care providers to educate adolescents or their parents on teen driving issues. More than half of all respondents (53.8%) reported using none of the specified types of materials. When resources were used, written materials such as pamphlets were used more often (32.2%) than other types of materials such as posters (9.7%). The use of parent–teen driving contract/agreements was reported by only 9.5% of respondents. When respondents were asked which types of resources they would be interested in receiving, written materials were reported most often (68.0%; Figure 1).
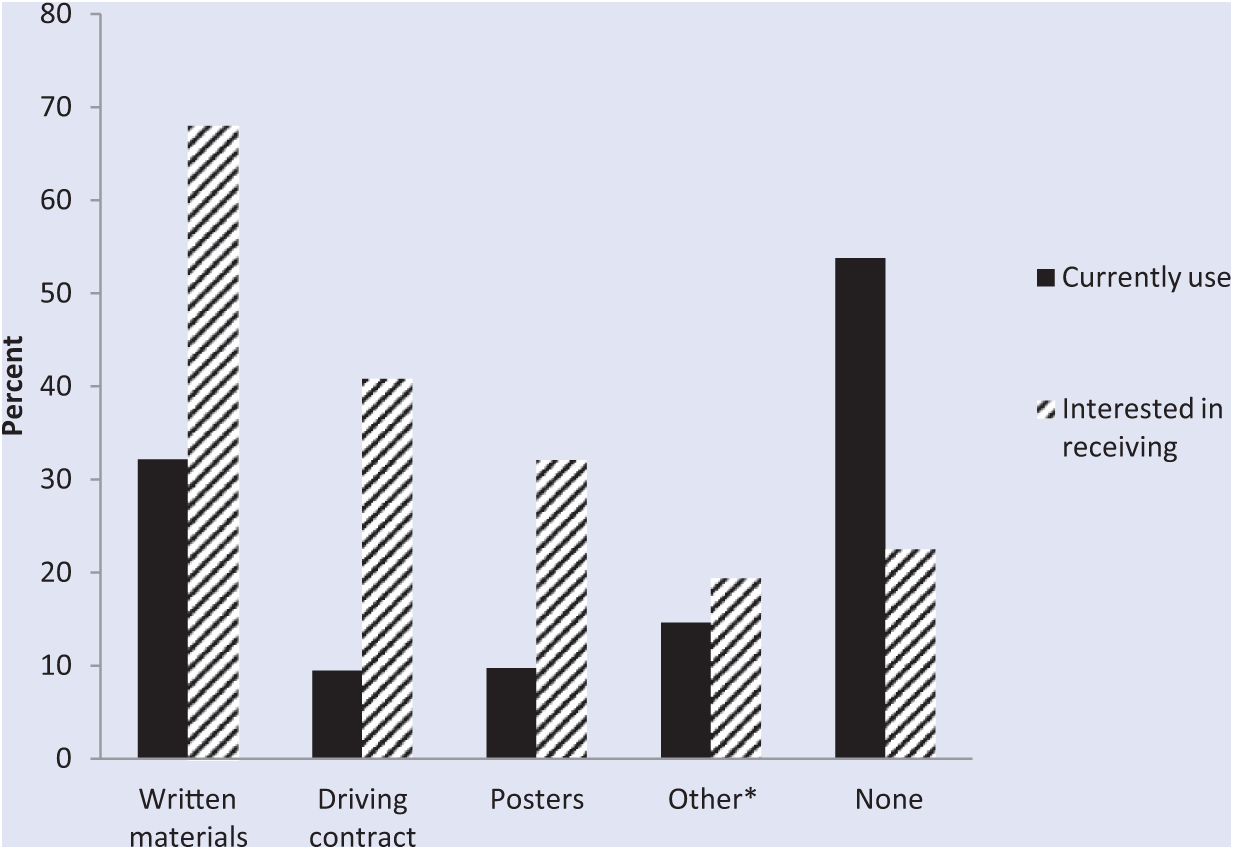
Teen Driving Resources Health Care Providers Reported They Currently Use and Would Be Interested in Receiving, DocStyles, 2010
Discussion
Most respondents in this study reported addressing at least one key driving safety topic. However, not all risky driving behaviors have the same effect on crash risk. The literature to date has identified driving with teen passengers and nighttime driving as 2 critical risk factors for teen driver crash deaths.10-13 Driving with 1 teen passenger increases the risk of being killed in a crash by 44% for drivers aged 16 to 17 years; transporting 3 or more young passengers quadruples the risk.
14
At night, the death rate is 2 times higher from 9:00
In the event of a crash, proper restraint use is the single most effective thing a person can do to reduce their risk of death and severe injury. 11 In 2012, seat belt use remained higher in the United States overall (86%), compared with teens and young adults aged 16 to 24 years (80%). 16 Physician counseling on seat belt use was reported by nearly 84% of responders in this study, 87% of pediatricians in the Weiss study, and 92% of physicians in the Campbell study.3,4 While none of these studies sought to evaluate the effectiveness of health care provider counseling on teen seat belt use, previous research has found counseling to be effective in other areas of restraint use. 6
Graduated driver licensing systems are effective in reducing crashes among young drivers, and comprehensive systems are most effective. 13 Only 1 out of 10 (10.2%) providers in our study reported counseling on their state’s GDL policy. Counseling on GDL serves overlapping purposes. First, adherence to GDL reduces crash risk overall. Second, passenger restrictions and nighttime driving curfews are components of most GDL systems; therefore, addressing this topic addresses 2 of the well-known risks for teen driver crashes. Third, compliance with GDL systems brings parents into the process. The phased approach to driving using GDL systems requires supervision usually provided by a parent. Bringing parents into the learning to drive process has documented benefits as illustrated by the Checkpoints program.
Checkpoints, a teen driver safety program for parents and their new drivers, used parent–teen driving agreements to increase parental monitoring of teen driving and was effective at decreasing risky driving and decreasing traffic violations. 17 Additionally, the use of parent–teen driving agreements by driver education instructors, and at the point of licensure at the motor vehicle administration, was effective at decreasing high-risk driving 18 and increasing limits on new drivers (eg, passenger limits, nighttime driving).18,19 Parent–teen driving agreements could be a useful and effective tool for health care providers when counseling parents and teens on driving safety. We found less than 10% of providers in our study reported using these agreements, indicating that providers could be a good target audience to reach with these materials. This fits with our finding that written materials were what the majority of respondents noted they would be interested in receiving.
A barrier to counseling by providers is the length of the office visit combined with the quantity of recommended advice for patients. A study by Belamarich et al documented 57 American Academy of Pediatrics policies that contained 162 unique health advice directives pediatricians were expected to deliver. Twenty-five recommendations pertained to adolescents, and 14 of these were injury related. 20 Finding the balance point for optimal treatment and realistic expectations will be a challenge. The adoption of technological advances is one approach. Electronic health records could help streamline this process using clinical decision support algorithms that are triggered by patient characteristics such as reaching driving age. In this way only those patients who are appropriate for the counseling would be automatically identified.
In this study, eligibility for participation included seeing patients at or near driving age. There was no information on the number of patients treated in this age group, or the proportion of their practice that fell into this category. Without this information it is difficult to tell whether any counseling differences we identified, for example, by provider specialty, were due to differences in counseling behavior or underlying differences in patient mix or other factors. However, pediatricians reported counseling on at least one driver safety topic more than the other specialties, and reported counseling on most of the individual topics more than the other specialties. This consistency suggests more frequent teen driver safety counseling by pediatricians.
This study is subject to limitations. The data presented are self-reported and could be overestimates or underestimates of counseling behavior. Also, there is possible self-selection bias since respondents could have agreed to participate due to increased interest in the topics covered in DocStyles 2010, including teen driver safety. Finally, differences in demographic characteristics between responders and nonresponders are unknown as no information was available for nonresponders.
This study confirmed gaps in provider counseling around teen driver safety and went further to identify the types of educational materials in use, and which materials providers would be interested in receiving. Most respondents reported addressing key driving safety topics with adolescents and/or their parents. This, coupled with health care providers’ expressed interest in receiving written resource materials, presents an opportunity for future progress in effective counseling on teen driver safety. However, the effectiveness of health care provider counseling specifically on teen driver safety practices remains undocumented. Rigorous evaluation of the effects of counseling on teen driver safety behaviors including seat belt use, nighttime driving, teen passengers, use of parent–teen agreements, adherence to state GDL requirements, and, ultimately, on the number of crashes, injuries, and deaths prevented is needed.
Footnotes
Acknowledgements
Michele Huitric, MPH, Arlene I. Greenspan, DrPH, MPH, National Center for Injury Prevention and Control, CDC, for composition of survey questions.
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.