
Abstract
Depression is often diagnosed using the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5) criteria. We propose how certain lifestyle choices and non-modifiable factors can predict the development of depression. We identified 10 cause categories (hits or “blows” to the brain) and theorize that four or more active hits could trigger a depression episode.
‘The DSM-5 criteria used to diagnose a major depressive episode indicate that the individual must either have a depressed mood or a loss of interest or pleasure in daily activities consistently for at least a 2-week period.’
The Diagnostic and Statistical Manual of Mental Disorders is the most widely accepted nomenclature used by clinicians and researchers for the classification of mental disorders. The DSM-5 1 criteria used to diagnose a major depressive episode indicate that the individual must either have a depressed mood or a loss of interest or pleasure in daily activities consistently for at least a 2-week period. This mood must represent a change from the person’s normal mood. Social, occupational, educational, or other important functions must also be negatively impaired by the change in mood. A major depressive episode is also characterized by the presence of 5 or more of these 9 symptoms: (1) depressed mood most of the day, nearly every day, as indicated by either subjective report or outside observation; (2) markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day; (3) significant weight loss or weight gain or decrease or increase in appetite nearly every day; (4) insomnia or hypersomnia nearly every day; (5) psychomotor agitation or retardation nearly every day; (6) fatigue or loss of energy nearly every day; (7) feelings of worthlessness or excessive or inappropriate guilt nearly every day; (8) diminished ability to think or concentrate, or indecisiveness nearly every day; (9) recurrent thoughts of death, recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide. This standard is very useful for diagnosing depression, but the symptom constellation does not clarify causation. A system to more accurately pinpoint the causes of depression could help focus treatments and improve both short-term and long-term outcomes. It is rational to identify and treat each reversible cause systematically. Such focused intervention might also allow for effective preventive treatment strategies.
The origin of the hit hypothesis came after reading an article in 1990 that proposed that about 1 in 3 patients who come to the internal medicine physician suffers from depression. 2 An extensive literature search in the next few months on our medical journal subscriptions and in MEDLINE, Cochrane, and nearby libraries resulted in more than 100 factors that are associated with an increased risk of depression. We have grouped these 100 factors into 10 categories that we call “hits.” A person is considered to have an active hit when he or she meets at least one-third of the characteristics of a particular category hit. The only exception is the presence of any disease in the addiction or medical categories, which is considered an active hit in the corresponding area, regardless of the presence of any other factors in that group. The central hypothesis of the program is that a person with at least 4 of the 10 hits active, will likely experience depression. The goal of therapy in the program is to identify and decrease or eliminate the active hit categories to less than 4 as a mechanism to effectively acutely treat and increase the likelihood of a long-term remission. We have also designed a screening test to determine which of the hit categories any individual patient may currently have. This test has been validated, and a manuscript has been written that is in the process of being published. The test has been registered under the name Nedley Depression Recovery Program Assessment Test, registration TX 7-398-022. The 10 hit categories are the following: (1) genetic, (2) developmental, (3) lifestyle, (4) circadian rhythm, (5) addiction, (6) nutrition, (7) toxic, (8) social/complicated grief, (9) medical condition, and (10) frontal lobe. Of these 10 categories, only 2 are irreversible (genetic and developmental). In some patients, the medical condition cause may not be reversible because of treatment limitations or advanced secondary pathological effects. The characteristics of each hit are listed below. Again, having a ratio of at least 1:3 factors counts as an active hit.
Genetic hit category: Family history of depression or suicide in a first-degree relative. 3
Developmental hit category: Early puberty in girls (beginning menstruation by age 11 years or younger), 4 history of depression in adolescence, 5 not being raised by both biological parents, 6 sexual abuse, 7 and being raised or living with someone who is an alcoholic or drug addict. 8
Nutrition hit category: Low dietary tryptophan 9 ; low omega-3 fat intake10,11; low folic acid intake 12 ; low vitamin B intake 13 ; diet high in cholesterol, 14 saturated fat, 15 and sugar 16 ; and marked anorexia and weight loss. 17
Social hit category: Absence of social support,18-20 negative or stressful life events,21,22 low social class,23,24 being raised by grandparents, 25 and immediate family member being an alcoholic or drug addict.26,27
Toxic hit category: High lead levels28,29; high mercury levels 30 ; high arsenic, bismuth, or other toxin levels 31 ; or high risk of exposure to these toxins.
Circadian rhythm hit category 32 : Regular insomnia, routinely sleeping more than 9 hours per day or less than 6 hours per day, and not having regular hours for sleeping and eating.
Addiction hit category: Use of alcohol,33,34 cigarette or tobacco use,35,36 heavy caffeine use, 37 recreational drug use (including marijuana), 38 daily use of benzodiazepines, or chronic narcotic use for more than 30 consecutive days.
Lifestyle hit category: Not on a regular aerobic exercise program, 39 not regularly exposed to daylight or a medical-grade light box for at least 30 minutes a day, 40 and rarely breathing fresh air. 41
Medical condition hit category: Hepatitis C, 42 recent head injury,43,44 stroke, 45 heart disease, 46 terminal cancer, 47 Parkinson’s disease, 48 uncontrolled diabetes, 49 severe postpartum stress, 50 premenstrual tension syndrome, 51 inadequately treated thyroid disease, 52 lupus, 53 inadequately treated adrenal gland disease. 54
Frontal lobe hit category: On low carbohydrate diet,55,56 on high meat or high cheese diet or eating lots of rich food,57,58 entertainment TV or movie addiction,59-61 entertainment Internet or chat Internet addiction,62,63 frequent sexual stimulation that activates right frontal lobe,64,65 regular exposure to syncopated rhythm music and/or videos,66-68 conscious suppression of frontal lobe activity,69-75 lack of regular abstract thinking, 76 acting against one’s conscience or known value system. 77
Of these 10 hits, only the genetic and the developmental are not reversible. Most of the other reversible hits are directly related to lifestyle choices.
Methods
Sample
Participants were those from our 8-week community-based (n = 4272) depression recovery program (see Table 1 for demographics) who came from urban and rural settings from various countries. The program consisted of weekly 2-hour sessions. To test our hypothesis, we used the data from the Nedley DSM-Depression test administered to participants. We compared the DSM-5 criteria with the 4-hit hypothesis.
Demographic Characteristics.
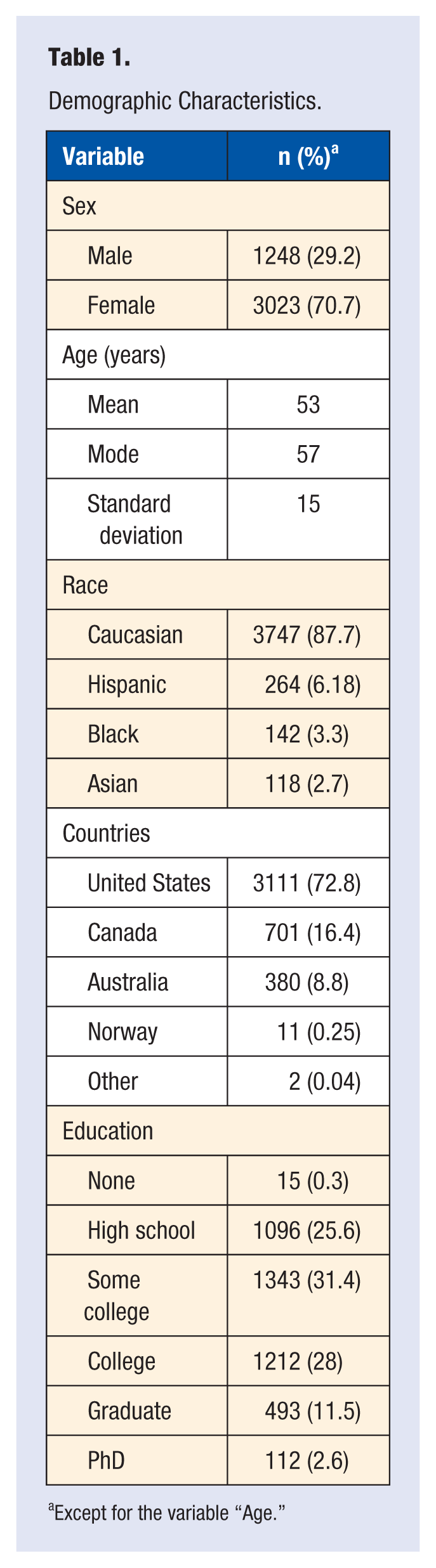
Except for the variable “Age.”
Measures
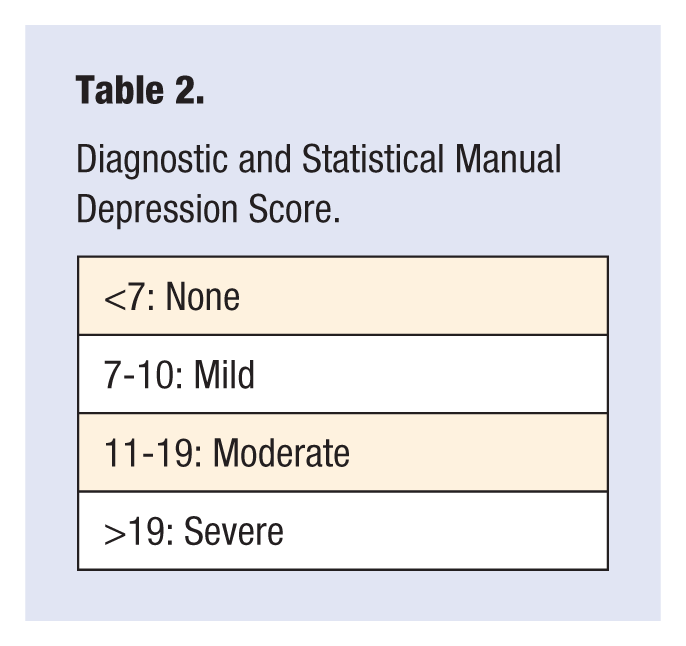
The Nedley DSM-Depression test is a 75-item self-reporting screening tool that assesses depression (a slightly modified PHQ-9 (Patient Health Questionnaire) test 78 ), anxiety level, emotional intelligence quotient, and demographic data. The copyright for the PHQ-9 was formerly held with Pfizer, who provided the educational grant for Spitzer, Williams, and Kroenke who originally designed it. 79 This is no longer the case, and no permission is required to reproduce, translate, display, or distribute the PHQ-9. The other test elements of the DSM-Depression were also from public domain tests. Changes were made mostly to the wording of the questions to get a more accurate response. For the depression value, we used the standardized DSM-5 criteria to arrive at the numerical value. See Table 2 for the interpretation of depression values. This tool was used to determine the active hits on the participant. We compared the value of the DSM-5 depression score with the number of active hits to see if they correctly predicted a depressed or nondepressed state. With these values, we calculated the true positives, false positives, true negatives, and false negatives in order to compute sensitivity, specificity, and positive and negative predictive values.
Diagnostic and Statistical Manual Depression Score.
Procedure
Participants took the Nedley Depression Recovery Program Assessment Test twice: at the beginning, on the first day of the program and at the end of the 8-week program. We scored the test using a Scantron system (Scantron Corporation, Eagan, MN). Statistical analysis was performed using SPSS software (SPSS Inc, Chicago, IL) and Excel (Microsoft Inc, Redmond, WA).
Results
After the initial test, the average depression score was 13 (standard deviation [SD] = 7.6), which indicates moderate major depression. Of the 4271 participants, 72.6% (n = 3104) were classified as having depression and 27.4% (n = 1167) participants were not depressed. At the beginning, on average, they had 5.2 active hits (SD = 2). The most prevalent active hits and the percentage of participants who had them, were as follows: lifestyle (79%), genetic (64.7%), circadian rhythms (69.3%), frontal lobe (64.7%), social (56.8%), nutrition (54.23%), medical (52.9%), developmental (40.2%), toxins (30.8%), and addictions (8.4). Comparing individual depression status with the 4-hit hypothesis resulted in 2777 true positives, 327 false negatives, 597 false positives, and 570 true negatives, which yielded a Matthew correlation coefficient (MCC) of .41, sensitivity of 89.4% (confidence interval [CI] = 88.3-90.52), specificity of 48.84% (CI = 45.94-51.75), positive predictive value of 82.31% (CI = 80.98-83.58), and negative predictive value of 63.55% (CI = 60.3-66.7).
The second test, taken by the 4271 participants in the eighth week of the program, resulted in an average depression score of 6 (SD = 6), which indicates no major depression. After 8 weeks, 57.6% (n = 2754) did not qualify as depressed. On average, participants ended the program with 2 active hits (SD = 2), which is consistent with the 4-hit hypothesis. The most common hits, by percentage, at the end of the program were as follows: genetic (62.2%), lifestyle (62.9%), circadian rhythm (52.6%), social (50.1%), medical (47.8%), frontal lobe (41.3%), developmental (39.2%), nutrition (28.8%), toxins (28.3%), and addiction (6.4%). Measuring individual depression status against the number of hits showed 1514 true positives, 295 false negatives, 1140 false positives, and 1322 true negatives, which resulted in a MCC of .38, sensitivity of 83.6% (CI = 81.9-85.5), specificity of 53.7% (CI = 51.7-55.6), positive predictive value of 42.3% (CI = 40.8-43.8), and negative predictive value of 81.7% (CI = 79.7-83.6).
Conclusions
Because the sensitivity and specificity of a test do not depend on the prevalence of the disease in the population, these markers gave similar results for the tests at the beginning and end. The most accurate valuation of this test was sensitivity (89.4% for the first and 83.6% for the last test). The specificity values were lower (48.84% in the beginning test and 53.7% for the end test). The sensitivity and specificity are reasonable compared to the Papanicolaou smear (sensitivity of 76% and specificity of 68% 80 ) and the Downtown fall risk index (sensitivity ranging from 81% to 95% and specificity of 35% to 40% 81 ).
We tested how sensitivity and specificity would behave if the hit threshold were raised or lowered (see Figure 1). A threshold of 3 hits would give a before sensitivity of 96.4% and specificity of 27.8%, and an after sensitivity of 93.7% and specificity of 32.9%. Lowering the threshold lowers the specificity excessively. Increasing the threshold to 5 hits gave a before sensitivity of 76.5% and a specificity of 70.7%, and an after sensitivity of 66.2% and specificity of 71.9%. Raising the threshold increases the specificity as expected at the expense of, the sensitivity. As expected, the more the number of active hits, the more specific the test becomes. The most helpful aspect of the test is that it provides insight into the possible causes of an individual participant’s depression and provides a tangible goal and specific focus of treatment for both the clinician and patient.
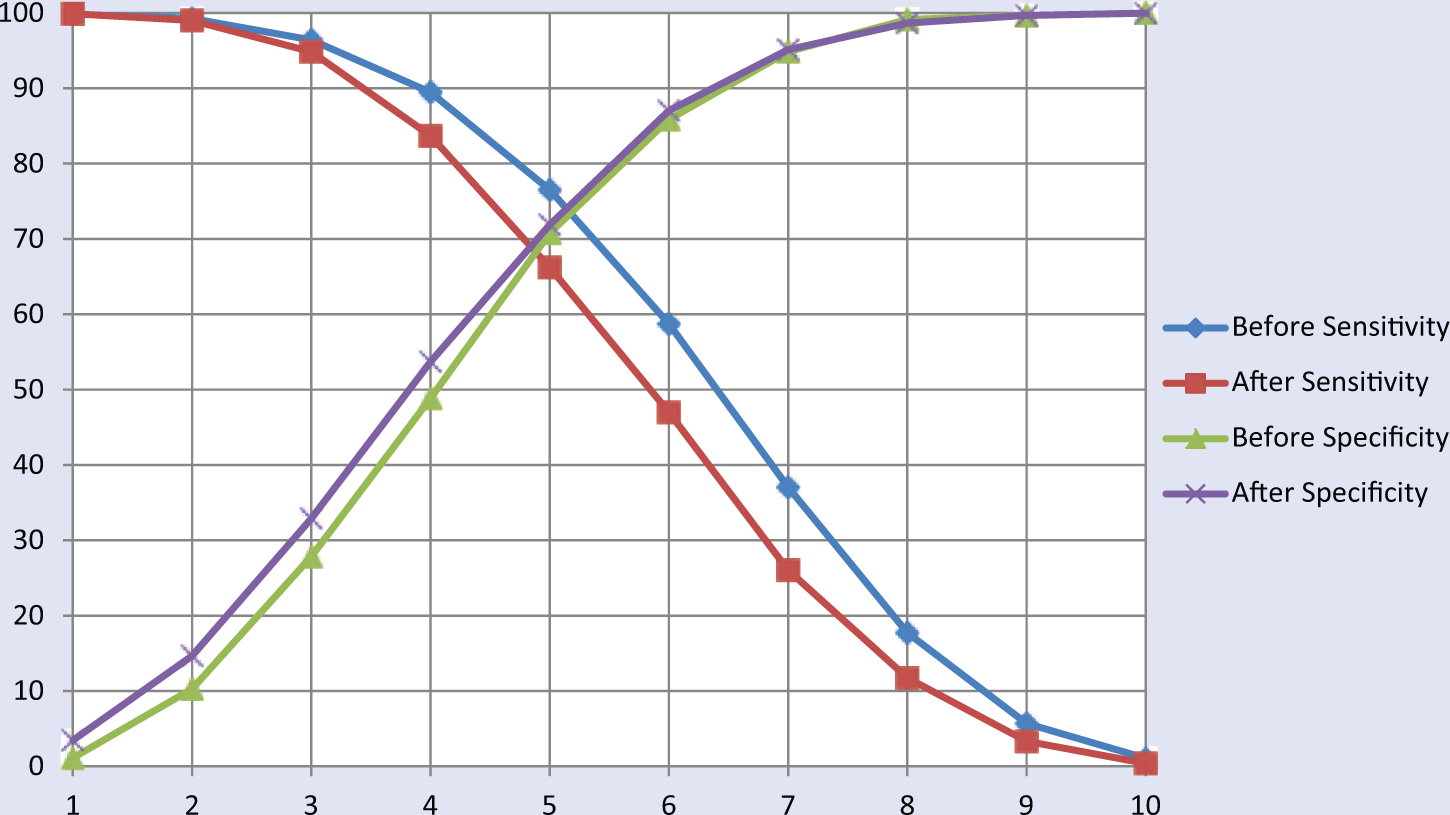
Sensitivity before and after, specificity before and after against number of hits (x).
Positive and negative predictive values tend to vary according to the prevalence of the depressed individuals. Because many of the participants improved, we expected these values to vary significantly between the first and second tests. Sensitivity and specificity are calculated only with some part of the true positive, true negative, false positive, and false negative values and cannot give a complete picture of the performance of the test. The MCC uses all 4 measurements to give a more balanced, representative, and comprehensive value. 82 The formula for the MCC is as follows:
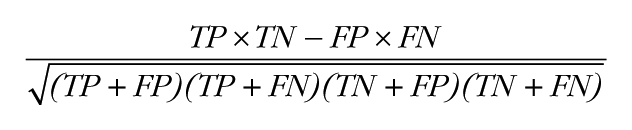
where TP, TN, FP, and FN are the true-positive, true-negative, false-positive, and false-negative values, respectively. MCC can help differentiate between random distribution and perfect correlation. It yields a numerical value that can range from −1 to 1, where 1 shows perfect positive correlation, −1 perfect negative correlation, and 0 a random distribution. A value of .5 means that 75% of cases are correctly predicted, whereas random distribution (0 value) would mean 50% positive and 50% negative. We found that the 4-hit threshold gave us the best MCC value, with .41 before and .38 after. If we increase the threshold to 5 hits, it will improve the before value to .43 but the after value actually worsens to .37, compared with the 4-hit threshold value. A graphic representation of the MCC against hits from 1 to 10 can be seen in Figure 2.
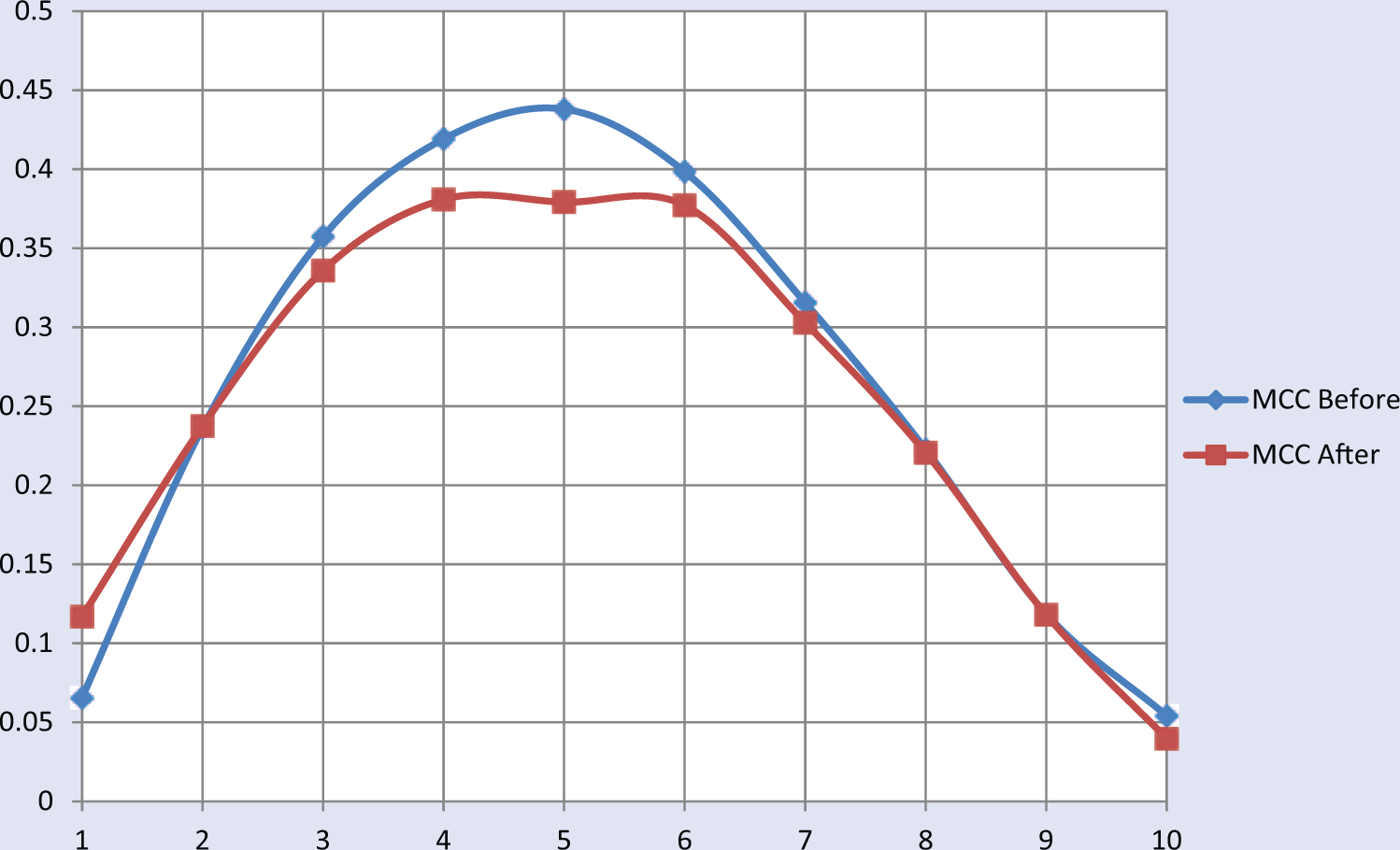
Matthew correlation coefficient correlated with the different hits.
Improving lifestyle and decreasing the number of hits not only helped the participants who were depressed but also those who were not depressed. According to the results of the before and after tests, they were able to improve their overall lifestyle, nutrition, health habits, and frontal lobe function as measured by their resulting hits.
Given the many potential causes of depression, it is truly amazing that even more people do not develop this prevalent mental disorder. We have found from our depression programs that the brain is resilient and can typically stand up to a combination of 3 risk factor categories and still function correctly. However, when the fourth risk factor category is added, even the healthiest brain will often develop major depression. The long list of possible factors that can contribute to or cause depression should highlight the importance of carefully considering causative factors. Because many of these factors are directly related to lifestyle choices, we foresee the future treatment of depression depending more on lifestyle changes than pharmacological treatment.
Limitations
This test was administered on a population already seeking mental health education. It would be interesting to test the 4-hit hypothesis on a wider sample, including those who are not seeking mental health education.
An important issue left unanswered is which hit categories are more likely to improve depression symptoms and the DSM score. Further studies need to be done to answer this question.