
Abstract
A growing body of literature suggests that regular exercise among older individuals regardless of the degree of frailty, with or without underlying chronic disease, may attenuate the consequences of age-related changes on exercise capacity. The purpose of this article is to review the effects of age-related changes on exercise capacity and the benefits of prescribing exercise to older persons.
Keywords
‘As such, exercise capacity is an important determinant of healthy independent living in elderly populations.’
Introduction
Modern medical advances and aging populations have led to a rising number of patients with multiple chronic medical conditions. 1 It is estimated that >75 million people live with 2 or more chronic medical conditions in the United States alone. 2 The burden of these chronic diseases disproportionately affects elderly people, who are also the most rapidly expanding segment of the population. 1 The number of Americans aged >65 years will increase from 40 million in 2010 to 81 million by 2040.3,4
Increasing numbers of seniors with multiple medical conditions will place considerable strain on health services. Patients older than 65 years seek care from generalists at a rate of twice that of those younger than 65 years. 5 Given the projected increase in this older demographic, the workload of family physicians and general internists in the United States is expected to increase by 29% between 2005 and 2025. 5 Diseases and disorders of the circulatory system account for a significant proportion of comorbidities among seniors.6,7 Between 2005 and 2015, inpatient use in this group is expected to increase by 11.8% at a rate of 1.12% per year. 7 Such conditions include coronary artery disease, heart failure (HF), and stroke. In addition, a number of other geriatric conditions (frailty, cognitive impairment, and functional decline) have increasingly been thought of as reflections of vascular aging.8,9 The decline in capacity with age is accelerated in patients with these conditions. Exercise among elderly people can have significant benefits for exercise capacity and overall quality of life (QoL).
A growing body of literature suggests that regular exercise among older individuals, regardless of the degree of frailty or comorbid chronic disease, may attenuate the consequences of age-related changes on exercise capacity and one’s ability to function independently.8,9 Optimization of exercise capacity in elderly populations through physical activity has far-reaching benefits for independence and overall QoL as recorded by questionnaires such as the SF-36 (Short Form 36).8-10 As such, exercise capacity is an important determinant of healthy independent living in elderly populations. For physicians, encouraging physical activity may serve as a highly effective means of reducing morbidity and maximizing independence among older patients through improved exercise capacity.
This review will highlight changes to the aging body as they relate to exercise capacity in elderly populations. The beneficial effects of exercise as a means of counteracting or attenuating the decline in exercise capacity with age will also be discussed. Finally, we will outline recommendations for prescribing exercise programs in elderly populations, including those who are frail.
Normal Aging and Its Effect on Exercise Capacity
Normal aging results in a number of changes that culminate in a decline in exercise capacity. In the cardiovascular (CV) system, these changes include alterations to the cardiac anatomy, vascular remodeling, and endothelial function. Changes to skeletal muscle, the respiratory system, and the cerebrovascular system also contribute to declines in exercise capacity. Atrophy of skeletal muscle and increases in pulmonary anatomical dead space are observed with age. In the cerebrovascular system, changes with age may predispose individuals to developing dementia, an important determinant of exercise capacity in elderly populations. Increasingly inflammatory environments and changes in brain perfusion are seen in the cerebrovascular system of elderly individuals.
These normal age-related changes result in a decline in exercise capacity compared with when the individual was younger. The age-related decline in exercise capacity can be exacerbated if the individual, because of the demands of life, develops a relatively more inactive lifestyle with advancing age. The development of chronic conditions such as diabetes mellitus or obesity will accelerate the age-related changes, resulting in an even greater reduction in exercise capacity, with an increase in the risk of developing frailty and cognitive impairment. Maintaining a physically active lifestyle will help prevent a decline in exercise capacity that is greater than what would be expected with normal aging.
Cardiovascular System
Changes in Vascular Structure and Function
There are significant age-related structural and functional changes in the vascular system. The endothelium undergoes a progressive reduction in nitric oxide (NO) production and availability, resulting in increased smooth muscle–mediated stiffness of arteries.11,12 This progressive decline in endothelial-dependent vasodilation occurs earlier in men than in women. 12 The impairment of NO is coupled with an enhanced reactivity to a number of vasoconstrictors. 13 Proposed mechanisms of age-related reductions in endothelial function include attenuated endothelial NO synthase expression and increased vascular formation of superoxide anions. 14 Together, they function to reduce the availability of NO through decreased production and increased clearance, respectively. 14
Significant changes occur in elastic arteries, including wall thickening and stiffening, wider lumens, collagen deposition, fractures to the elastic lamellae, and hypertrophy of smooth muscle cells.12,15,16 Arterial stiffness increases the risk of CV events, dementia, and death.17,18 Among older adults, arterial stiffening contributes to orthostatic intolerance and dyspnea with exertion; factors that often limit an individual’s ability to complete required daily activities. 18
The development of arterial stiffening occurs in a nonuniform pattern throughout the vascular system. The vascular stiffness tends to occur in the larger central and conduit arteries, whereas more peripheral arteries are often spared. 18 Aortic stiffening with age is primarily attributable to repeated mechanical forces over time, leading to largely irreversible fracturing of the elastic lamellae and collagen deposition. 19 Hormones also play an important role in vascular stiffening. Angiotensin II induces matrix remodeling and arterial hypertrophy, increases collagen production, decreases synthesis of elastin, and increases oxidative stress. Through stimulation of cytokines and growth factors, angiotensin II promotes an inflammatory response that further disrupts the balance of collagen and elastin. 20 Aldosterone also promotes vascular stiffening. Its primary mechanism is through hypertrophy and fibrosis of vascular smooth muscle. 21
The age-related changes to vascular function and structure are accelerated by a number of common chronic diseases, including diabetes mellitus, atherosclerosis, and renal compromise. 18 These conditions increase intraluminal pressure through hypertension and elevated pulse pressure.18,22 Higher intraluminal pressures amplify the deregulation of collagen and elastin. 12 The result is further arterial stiffening through an increase in the production of abnormal collagen and a decrease in the amount of elastin. 13
Changes in Heart Structure and Myocardium
The stiffened arterial tree results in increased left-ventricular (LV) afterload, thus promoting the development of LV hypertrophy, impairing coronary perfusion, and raising systolic blood pressure (BP) and pulse pressure.16,19 Progressive stiffening and LV hypertrophy are primarily a result of myocyte loss, followed by enlargement of remaining myocytes and increased fibroblast and collagen deposition. 17 Loss of myocytes in the sinoatrial node and the fibrosis/calcification of the adjacent cardiac skeleton predisposes older individuals to arrhythmias, including heart block. 23
Diastolic function declines steadily after 30 years of age and is an important predictor of increased mortality and reduced exercise capacity in elderly populations.24,25 Abnormal cardiac filling, relaxation, or stiffness are characteristics of diastolic dysfunction. It is associated with significant remodeling of the LV and left atrium through cardiomyocyte hypertrophy, increased extracellular matrix, collagen deposition, and fibrosis of the myocardium.26-29 The abnormalities seen in diastolic dysfunction are exaggerated by the body’s response to exercise. To meet the demands of exercise on the CV system, the rate of diastolic flow across the mitral valve must increase. In young healthy individuals, a normal LV is able to rapidly decrease its pressure to permit increased transmitral flow. 30 A patient with diastolic dysfunction is unable to do so as a result of significant remodeling. Instead, pressure in the left atrium is increased and pulmonary congestion results. 31 The Umea General Population Heart Study found a significant decrease in diastolic velocity from 16 cm/s in patients at 30 years of age to 9 cm/s at 80 years of age on Doppler ultrasound. 25 Ultimately, patients with diastolic dysfunction have significant dyspnea on exertion and reduced exercise capacity.
Atherosclerosis, hypertension, and volume overload (eg, as a result of valvular abnormalities such as mitral regurgitation) have a significant impact on structural changes to the heart.32,33 Marked LV hypertrophy (increase in LV mass) is seen in patients with chronic pressure overload and in those with chronic volume overload. Pressure overload increases LV wall thickness out of proportion to the increase in LV volume, resulting in concentric LV hypertrophy. In patients with volume overload, there is an increase in LV volume out of proportion to the increase in LV wall thickness, resulting in eccentric LV hypertrophy. 32 Diabetes mellitus and obesity are other conditions that have also been found to promote the development of LV hypertrophy.34,35
Epidemiological studies have shown that LV hypertrophy is a significant risk factor for CV mortality, morbidity, and frailty.36-39 LV hypertrophy is associated with an increased risk of stroke, sudden death, myocardial infarction, and chronic HF. 39 In both men and women, the finding of LV hypertrophy on the electrocardiogram has an age-adjusted 5 times increased risk of all-cause mortality. 40 The cause of this excess mortality and morbidity is complex and poorly understood.
Exercise and Age-Associated Arterial Stiffening, Endothelial Function
There is evidence to support the benefits of exercise training to protect against age-related central arterial stiffening. Compared with their sedentary counterparts, individuals who engage in a regular exercise regimen tend to have less-advanced arterial stiffening.41-43 Additionally, regular exercise has been found to improve arterial compliance in older adults. 41 Tanaka et al 44 looked at arterial compliance in 3 groups of men: young (25-30 years old), middle-aged (47-52 years old), and older (62-69 years old). Each group was further divided into sedentary, recreationally active, and endurance trained. Among middle-aged and older men, arterial compliance was 20% to 35% higher in the endurance-trained groups (vigorous aerobic-endurance exercise ≥5 times per week and active in local road running races). The same study also looked at the effect of a 3-month aerobic exercise regimen on 20 middle-aged (53 ± 2 years) sedentary men. The exercise regimen consisted of a mix of walking or jogging to reach an intensity of 70% to 75% of maximal heart rate toward the end of the regimen. On completion, the men experienced increased central arterial compliance to levels similar to that seen in endurance-trained middle- and older-aged men. 44
Exercise and Diastolic Dysfunction
There is evidence that exercise capacity can be increased in patients with diastolic dysfunction through physical activity. Smart et al 45 compared outcomes following a 16-week exercise training program in patients (mean age = 65 years) with systolic dysfunction and those with diastolic dysfunction. A total of 30 patients with diastolic dysfunction were randomized to either an exercise or nonexercise group. Significant improvements were observed among patients with diastolic dysfunction in peak oxygen consumption (VO2peak) and QoL as measured by the Minnesota Living with Heart Failure and Hare Davis questionnaires. However, these improvements did not correlate with changes in diastolic function on the echocardiogram. Sandri et al 46 followed 30 elderly patients (mean age = 72 years) with diastolic dysfunction and reduced ejection fraction over the course of a 4-week supervised endurance-training program. Participants were matched to a control group who did not receive any exercise intervention. The exercise group had a 26% reduction in LV isovolumetric relaxation time, suggesting improved diastolic function with exercise.
Exercise and CV Risk Factors
Physical activity modifies a number of CV risk factors for both middle-aged and older adults, including hypertension, diabetes, and obesity. The initiation of an exercise program produces modest but clinically significant reductions in BP among older adults with hypertension at baseline.9,47 In a meta-analysis of randomized controlled trials, 6 months of moderate-intensity aerobic exercise among adults aged 50 to 87 years led to a 2% decrease in resting systolic BP. 47 Studies included in this analysis showed reductions in resting systolic and diastolic BPs ranging from 2 to 8 mm Hg and from 0 to 5 mm Hg, respectively. 47 More significant reductions have been observed with low-intensity exercise. 48 Hagberg et al 48 subjected older (64 ± 3 years) men and women with hypertension to 9 months of either low- or moderate-intensity aerobic exercise. Those in the low-intensity (walking for 1 hour at 50% peak VO2 3 times/wk) group had an average decrease of 20 mm Hg in their systolic BP, compared with 8 mm Hg in the moderate-intensity group.
It is well established that regular exercise is an important means of preventing the development of type 2 diabetes among individuals of all ages.49-51 For those with the disease, it offers a means of reducing the risk of diabetes-related complications and comorbidities.51,52 Exercise is a major component of the management of type 2 diabetes mellitus and has been found to increase insulin sensitivity as well as improve glycemic control and carbohydrate/fat metabolism.49,50,52
Among those with diabetes, an exercise intervention results in a significant reduction of glycosylated hemoglobin (HbA1C) by 0.6%. 51 This is similar to the reduction obtained through pharmacological intervention with metformin (0.9%). 53 Lower levels of HbA1C reduce the risk of microvascular complications in diabetes. 54 Studies have shown successful reductions in HbA1C through a wide range of exercise programs, including low-intensity aerobic exercise regimens and high-intensity weight training regimens. 51 The majority of these studies were conducted among middle-aged patient populations, limiting their application to elderly populations.
Aerobic exercise training has also been found to be of benefit in obese elderly individuals.55-57 Physical activity programs in elderly populations have been shown to reduce obesity-related consequences.56-58 Many obesity-related complications are concentrated around the metabolic syndrome. Obesity is also related to osteoarthritis, pulmonary dysfunction, urinary incontinence, and sexual dysfunction in elderly populations. 56 Weight loss in elderly obese (body mass index >30 kg/m2) patients has wide-reaching benefits for these comorbidities and many others, including improved respiratory function, lipid and glycemic control, BP control, ability to complete daily tasks, and overall QoL. 56
Exercise in Coronary Heart Disease
An inverse relationship between regular exercise among older individuals and the risk of developing coronary heart disease (CHD) has been shown for even moderate levels of physical activity.59-61 A number of mechanisms have been proposed to account for the reduction in mortality associated with regular exercise. Improvements in exercise capacity, myocardial revascularization, CV risk profile through risk calculators such as the Framingham Risk Score, and increased patient surveillance may all play a role. 62 With higher intensities of regular exercise, a risk reduction of nearly 30% for the development of CHD has been observed.59,60 Regular aerobic exercise among older CHD patients has also proven to be beneficial by increasing the ischemic threshold, improving QoL, and reducing mortality.61,62
Improvements in VO2peak through regular exercise training are well documented among older individuals with CHD.63,64 Compared to control groups, a net increase in VO2peak of 2.3 mL/kg/min is observed with regular exercise training. 64 These improvements have been documented for a number of exercise regimens and rehabilitation programs. The majority of studies describe either aerobic exercise alone or in combination with resistance training. A meta-analysis comparing combined resistance and aerobic training to aerobic training alone found that combined regimens improved VO2peak by 0.41 mg/kg/min more. 63 Though this increase may seem minor, even small improvements in VO2peak among elderly patients with CHD have been shown to have significant prognostic and functional benefits. 65
Both total and cardiac mortality are reduced among middle-aged and older CHD patients randomized to exercise-based rehabilitation programs. There is some evidence that an exercise intervention reduces hospital readmission rates; however, this holds true only for studies with follow-up durations of up to 12 months. A Cochrane review of exercise intervention for CHD found that the reduction in mortality was not significantly influenced by the duration, intensity, frequency, and length of the exercise intervention. 62 It is important to note that this analysis consisted primarily of middle-aged men.
Exercise and Heart Failure
The mechanism through which exercise training is of benefit to HF patients is complex. Studies have shown that exercise in HF patients results in improved endothelial function and a subsequent increase in myocardial perfusion. 66 Exercise has also been shown to attenuate LV hypertrophy and ventricular remodeling in these patients. 67 Improved diastolic filling and myocardial contractility have also been reported. 68
Regular aerobic exercise has shown promising clinical outcomes for HF patients as well.69-71 There is considerable heterogeneity in QoL outcomes among HF patients as well as data regarding improvements in VO2peak. In terms of QoL, a small number of studies using validated disease-specific questionnaires (Minnesota Living with Heart Failure Questionnaire and the Kansas City Cardiomyopathy Questionnaire) have found significant improvements in QoL following exercise intervention. 70 The HF-ACTION study, a large multicenter randomized controlled trial of exercise intervention for HF patients, found a significant treatment effect on QoL. 72
Compared with usual care, HF patients enrolled in an exercise training program had increased 6-Minute Walk Test distance and VO2peak.69,70 Increases in exercise time have been shown at 3 and 12 months postinitiation of an exercise training program.70,72 Though significant increases in distance walked in the 6-Minute Walk Test are observed at the 3-month follow-up, the effect is less clear at 6 and 12 months. 70
HF-related hospital admissions are decreased among those who receive exercise intervention.69,70 The reduction in hospitalization is most significant for those with systolic HF. 69 Exercise training may result in a slight reduction in mortality, especially in those patients who are most compliant with the exercise training (Table 1).73,74
Summary of Age-Related Changes to and Effects of Exercise on the Cardiovascular System.
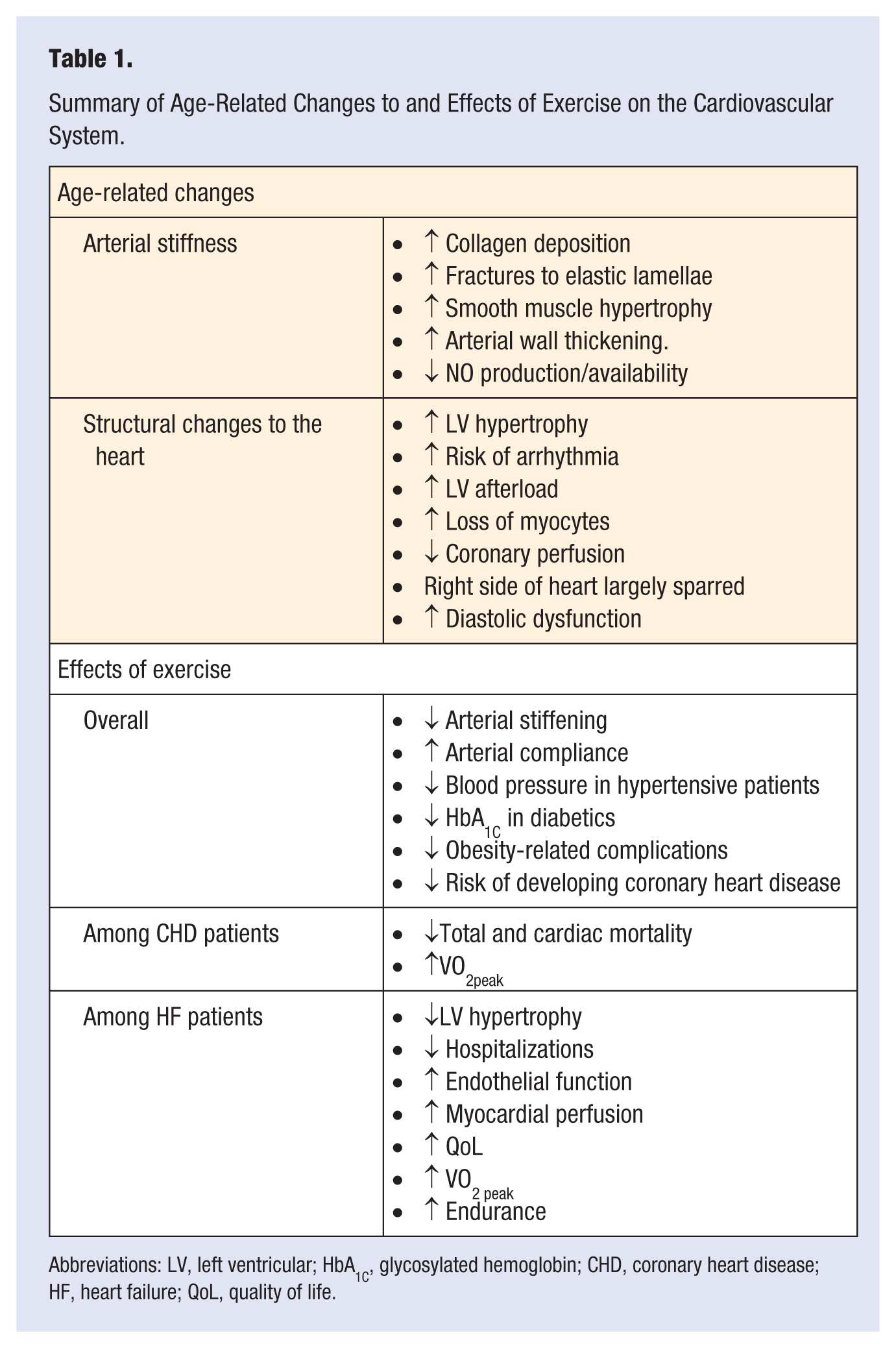
Abbreviations: LV, left ventricular; HbA1C, glycosylated hemoglobin; CHD, coronary heart disease; HF, heart failure; QoL, quality of life.
Respiratory System
With age, the respiratory system undergoes a number of anatomical changes. Anatomical dead space increases in the lungs through enlargement of alveolar ducts. 75 These ducts undergo a progressive loss of elastic tissue that ultimately results in reduced surface area for gas exchange. 75 Ventilation-perfusion mismatching is increased because the more dependent portions of the lung, which are better perfused, remain closed for part or all of the respiratory cycle. Arterial oxygen partial pressure (PO2) declines with age, whereas alveolar PO2 stays the same.76,77 This creates an increased alveolar-arterial gradient, an indication of a diffusion defect of the lungs. 77 In terms of pulmonary function, functional reserve decreases with age. Both forced vital capacity (FVC) and forced expiratory volume (FEV1) decrease with age. The decline is greatest among those older than 70 years. Total lung capacity is largely unchanged. 78 Changes to muscles of respiration with aging also decrease older individuals’ exercise capacity. With age, the diaphragm becomes less efficient, and respiratory muscle strength is decreased. Work of breathing during exercise is increased by as much as 30%. 79
Accelerated aging of the respiratory system is seen in patients with chronic lung disease. This is particularly evident among patients with chronic obstructive pulmonary disease (COPD). Decreased vital capacity and reductions in the strength of respiratory muscles are observed at a much younger age in COPD patients compared with their non-COPD counterparts. The mechanism is believed to be sustained exposure to cigarette smoke and pollutants. 80 Osteoporosis can also significantly influence an elderly individual’s pulmonary function through spinal fractures. Reductions in both vital capacity and FEV1 are observed among patients with osteoporotic spinal fractures. 81
Together, the anatomical and functional changes of the aging respiratory system reduce individuals’ exercise capacity and increase their risk of adverse outcomes, including pneumonia and hypoxia.75,79,82
Exercise, Pulmonary Function, and COPD
Aerobic exercise training programs have produced significant improvements in pulmonary function and QoL in elderly patients.83,84 In a sample of inactive men and women older than 55 years (mean age = 62.5 years), Martin-Valero et al 83 observed a significant improvement in pulmonary function following the implementation of a 12-week exercise program. The program consisted of two 60-minute sessions per week of aerobic and strength training as recommended by the American College of Sports Medicine. Both FVC and the ratio of FEV1 in 1 s to FVC (FEV1/FVC) showed significant improvement. QoL, as measured by the EuroQoL-5D questionnaire, was also significantly improved. Similarly, Huang and Osness 84 randomized sedentary elderly people (mean age = 83.7 years) to a control group (no exercise program), a moderate-intensity aerobic exercise group, or a high-intensity aerobic exercise group to assess the effect of aerobic exercise on pulmonary function. Following the 10-week exercise program, the moderate-intensity group showed significant improvements in FEV1, whereas the high-intensity group showed significant improvements in both FEV1 and FVC. No improvement in pulmonary function was found in the control group. 84
Pulmonary rehabilitation programs for elderly COPD patients have shown improvements in domestic function (ability to complete daily tasks at home), QoL, and exercise capacity.85-88 Trooster et al 85 randomized 100 patients (mean age = 63 years) to either usual medical care for COPD or an exercise program consisting of cycling, walking, and strength training for 6 months. Patients who completed the exercise program had improvements in 6-minute walking distance, QoL, and muscle strength. Pulmonary rehabilitation has the potential to reduce mortality among COPD patients because it has been significantly correlated with exercise capacity (Table 2). 86
Summary of Age-Related Changes to the Respiratory System and Effects of Exercise on the Aging Respiratory System.
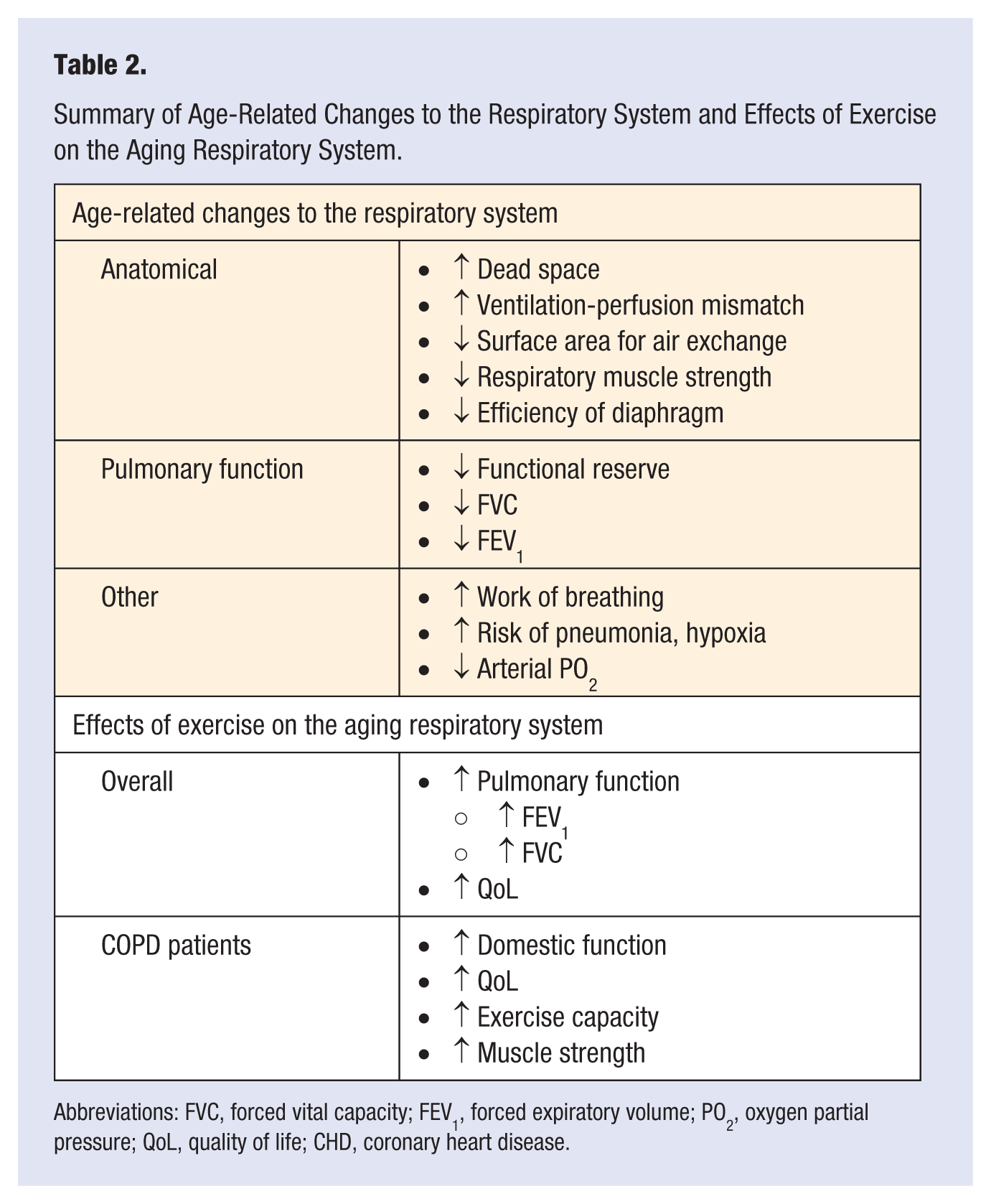
Abbreviations: FVC, forced vital capacity; FEV1, forced expiratory volume; PO2, oxygen partial pressure; QoL, quality of life; CHD, coronary heart disease.
Cerebrovascular System
As an individual ages, there are changes that take place in the structure and function of the brain that lead to a decline in cognition. Perfusion in the aging brain, especially in the deeper cerebral structures supplied by end arteries, becomes increasingly dependent on BP as these vessels become longer and tortuous, their walls thicken, and perivascular spaces enlarge. 89 These changes particularly affect the frontal lobes, and their severity has been correlated to the severity of ischemic white matter changes in the subcortical and periventricular regions.90-92 The resulting increased susceptibility to ischemia may predispose to the development of cognitive impairment. 91 In turn, cognitive decline in elderly populations has been associated with poorer QoL and reduced physical activity.93,94
A growing body of evidence suggests that increasingly inflammatory environments in the older body facilitate cognitive decline. 95 With normal aging, there is an increase of proinflammatory cytokines, including interleukin (IL)-6. Higher levels of such cytokines are associated with poorer scores on the Mini Mental Status Exam (MMSE), difficulties in new learning, and memory deficits. 96 Older individuals with underlying comorbid conditions may be at increased risk of inflammation-related cognitive decline and dementia. Obesity, COPD, and diabetes are all common comorbidities that create a heightened proinflammatory environment.97,98 The relationship between chronic comorbid disease and cognitive decline is complex and involves many factors beyond inflammation. Among people with diabetes, for example, the risk of developing dementia is doubled compared with that in age-matched counterparts. 99 However, the underlying mechanisms are poorly understood. Cognitive decline among elderly individuals is associated with an increased risk of depression, dependence, and a sedentary lifestyle.93,94 Combined, these factors reduce physical activity and exercise capacity with age by rendering individuals less active.
Exercise and Age-Associated Changes to the Cerebrovascular System
Regular exercise in sedentary adults has been shown to improve cognitive function, depressive symptoms, and mood; promote neurogenesis; and increase brain volume.100-111 Higher levels of aerobic fitness among older individuals are associated with increased hippocampal volume and smaller declines in the prefrontal and parietal regions.104,110 As such, exercise in seniors may translate to improved cognitive function, maintenance of brain volume, and reduced risk of onset of mild cognitive impairment, Alzheimer’s disease, and vascular cognitive impairment. 110 Among older individuals with cognitive impairments and dementia, there is evidence that exercise increases physical fitness and cognitive function. 112
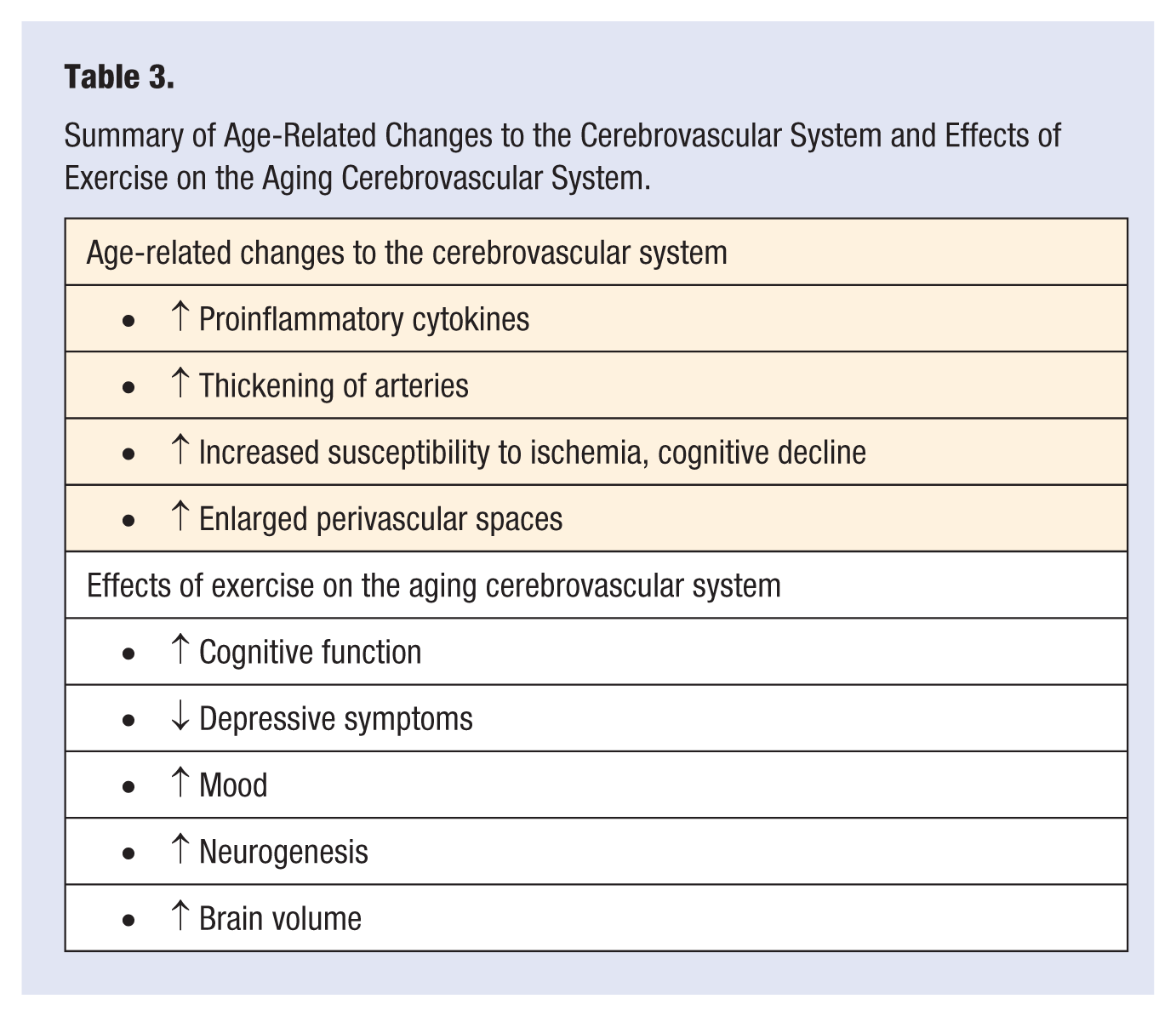
A recent Cochrane review confirmed that there is sufficient evidence that aerobic physical activity leads to improved cognitive function among older adults and, therefore, regular physical activity should be recommended for elderly populations to maintain cognitive function. 111 This included improved motor function, cognitive speed, and auditory and visual attention. However, there were insufficient data to confirm that these benefits are the result of improved cardiorespiratory fitness through aerobic exercise. Higher-quality studies are required to determine whether the aerobic component of exercise, as opposed to other forms of physical exercise, is necessary to produce these cognitive benefits (Table 3). 111
Summary of Age-Related Changes to the Cerebrovascular System and Effects of Exercise on the Aging Cerebrovascular System.
Skeletal Muscle
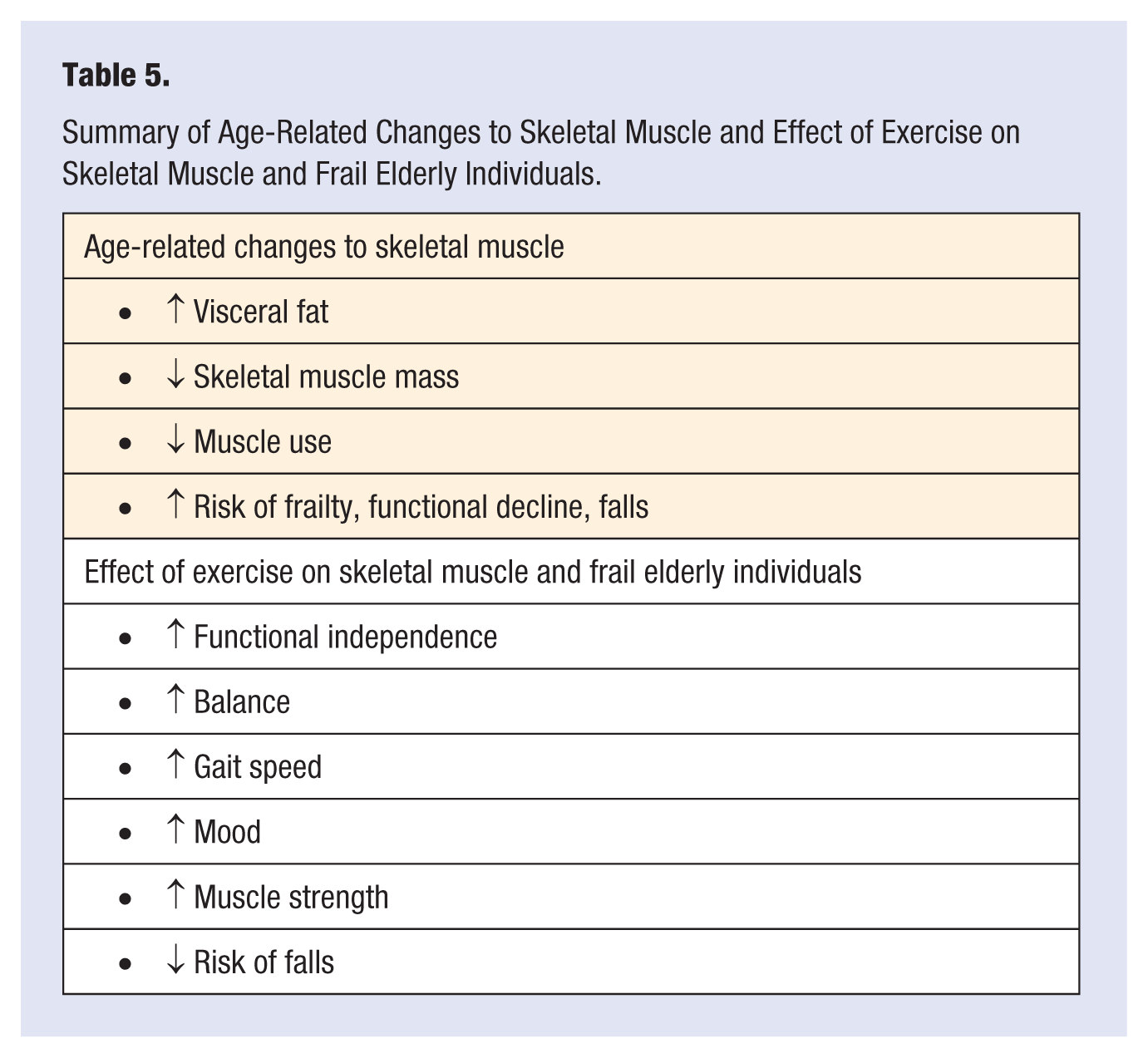
There are age-associated changes in skeletal muscle structure and function. 113 Sarcopenia, the age-related atrophy of skeletal muscle mass, plays a key role in the development of age-associated decline in exercise capacity. 113 Reduction of skeletal muscle mass occurs at a rate of 0.5% to 1% per year from ages 20 to 50 and accelerates thereafter. 114 More than 50% of the elderly population older than 80 years exhibit sarcopenia. 115 Normally occurring age-related changes to the endocrine system and inflammatory pathways are important contributors to the development of sarcopenia.115-118 Decreases in hormones such as growth hormone and insulin-like growth factor-1 are accompanied by decreases in lean body mass and an increase in visceral fat with age. 118 Adrenal androgen dehydroepiandrosterone (DHEA-S) is an important mediator of skeletal muscle synthesis and indirectly influences inflammatory pathways known to promote a decline in muscle mass. Levels of DHEA-S also decrease with age.115,116 A number of proinflammatory cytokines also influence the development of sarcopenia in elderly people.118,119 These cytokines promote myofibrilar protein degradation and decrease protein synthesis. Higher levels of IL-6 in elderly populations have been shown to have an adverse effect on skeletal muscle and appetite. Similarly, higher levels of tumor necrosis factor-α impair skeletal muscle protein synthesis. 118
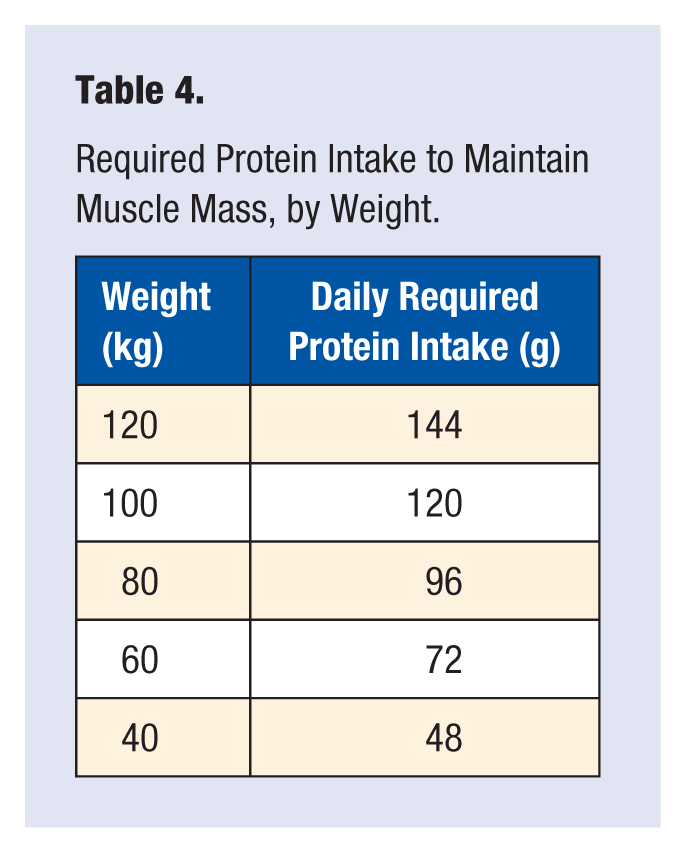
The age-related decline in skeletal muscle is accelerated by inactivity and poor dietary intake of protein.120,121 Progressive inactivity with age accelerates the development of sarcopenia through underuse of muscles. Inadequate dietary intake of protein inhibits proper muscle regeneration. At least 1.2 g/kg of protein per day is required for an older person to maintain muscle mass (see Table 4). 112
Required Protein Intake to Maintain Muscle Mass, by Weight.
Sarcopenia results in numerous consequences for the elderly patient. Frailty and vulnerability to adverse outcomes, including functional decline, falls, emergency room and long-term care admissions, depression, loss of independence, poor QoL, and ultimately even death have been reported.113,120,121 The associated loss of muscle strength ultimately decreases older individuals’ ability to withstand physical activity and reduces their exercise capacity.
Exercise, Sarcopenia, and Frailty
Generally, frailty refers to an increased vulnerability to a range of adverse outcomes, including death, institutionalization, and worse health. 122 More recently, frailty has come to be regarded as “a geriatric syndrome of decreased reserve to stressors, resulting from cumulative declines across multiple physiologic systems.” 123 (p675) Though sarcopenia is often a fundamental component of frailty, it may occur as a clinical sign outside of the syndrome of frailty. 123 A number of years ago, a randomized, placebo controlled trial by Fiatarone et al 124 found resistance training to be a feasible and effective means of counteracting physical frailty in older adults. Since then numerous studies have confirmed their findings. 125
Resistance and aerobic exercise training both have positive effects on frail individuals. Neural adaptation to increased muscle loading, protein synthesis, release of testosterone and growth hormone, and muscle hypertrophy are all mechanisms through which resistance training positively affects sarcopenia, which can contribute to the clinical presentation of frailty in elderly populations.126-129
Frail older adults respond remarkably well to exercise training, experiencing improved cardiorespiratory fitness and even restored functional independence.129-133 The greatest benefits of exercise training are observed among those who are the most debilitated and frail. 129 Increased gait speed, improved balance, and ability to complete activities of daily living have all been reported. 134 Exercise among older individuals has been shown to improve clinical depression with a comparable efficacy to antidepressant medications. A randomized control trial by Singh et al 135 found that a weight lifting exercise program in a group of elderly patients (71.3 ± 1.2 years) significantly reduced clinical depression. After 20 weeks, depression resolved in 73% of the exercise group compared with 36% of the control group. Controls received a series of health lectures and did not have any exercise intervention. A significant improvement in clinical depression remained at 26 months of follow-up among those who participated in the weight lifting regimen (Table 5).
Summary of Age-Related Changes to Skeletal Muscle and Effect of Exercise on Skeletal Muscle and Frail Elderly Individuals.
Peak Oxygen Consumption and Its Effect on Exercise Capacity
Peak Oxygen Consumption
Peak oxygen consumption (VO2peak), a person’s peak capacity to transport and use oxygen during exertion, provides a global measure of an individual’s fitness. 58 On average, VO2peak decreases 10% per decade, with an even greater rate of decline after 45 years of age.136,137 This decline is linked to aging and is seen even among athletes. Studies have shown that the process can be exacerbated by decreases in physical activity as well as concomitant illness.136-139 VO2peak is a key factor in an elderly individual’s ability to live independently in the community. A VO2peak of 18 mL/kg/min is needed to support the necessary activities associated with independent living. 140
Exercise and Peak Oxygen Consumption
All individuals, regardless of physical activity, experience a decline in VO2peak with age. 58 Many, but not all, studies have demonstrated that habitual physical training attenuates the decline in VO2peak.58,136-146 Ogawa et al 141 studied the decline in VO2peak in sedentary individuals as compared with their counterparts who underwent regular exercise training. The exercise-trained group was defined as those who participated in strenuous exercise of >30 minutes 3 to 4 times per week over several years. VO2peak declined by 40% to 41% in the sedentary group compared with 25% to 32% in the trained group. Data suggest that for individuals who were very active in early adulthood, maintaining a high VO2peak may require continuing an intensive exercise program into old age. Katzel et al 142 found that the decrease in VO2peak among older male endurance athletes is highly dependent on continued high-intensity exercise regimens. The older athletes (64 ± 1 years) who continued intensive exercise training did not experience a significant decline in VO2peak over a mean follow-up of 8.7 years. Among athletes who significantly reduced their exercise training with age, the decline in VO2peak over time was 2 to 3 times that of their sedentary counterparts. Therefore, those who experienced the greatest reduction in exercise training also experienced the greatest rate of decline in VO2peak with age. However, the absolute VO2peak of older individuals who exercise regularly remains higher than that of their age-matched sedentary counterparts.136,143,144
A cross-sectional meta-analysis by Wilson and Tanaka 136 found that the rate of decline in VO2peak was not different among men varying in habitual exercise status (Figure 1). A similar cross-sectional meta-analysis by Fitzgerald et al 144 found that the most physically active group of women had the greatest absolute decline in VO2peak with age. One explanation for this finding is that this group of women undergo the greatest decline in the extent and intensity of their exercise regimens with age. For those who maintained rigorous exercise regimens as they aged, the rate of decline in VO2peak was significantly reduced. It is unclear as to why this would be observed in women and not in men. Regardless of the rate of decline, absolute levels of VO2peak in both men and women were found to correlate with physical activity.136,144
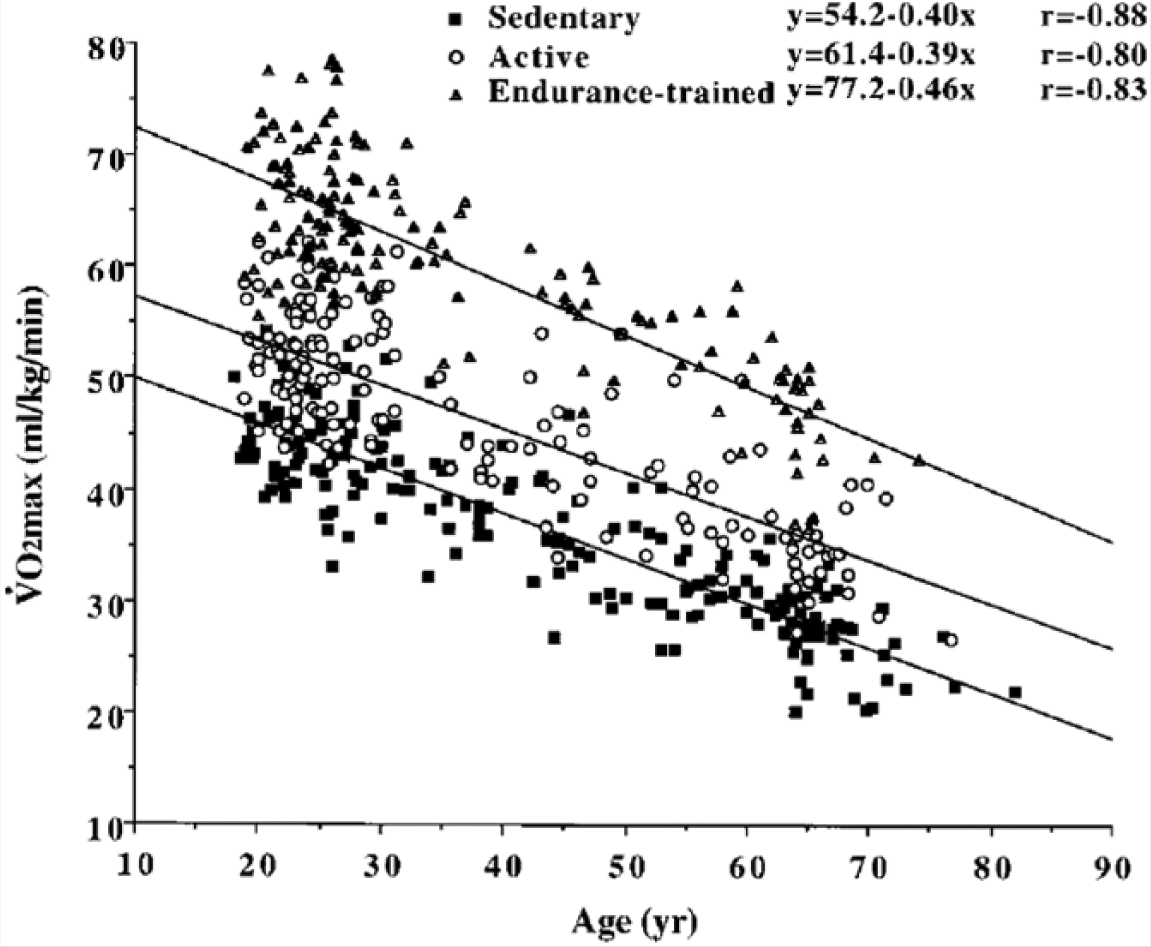
Rate of Decline in VO2peak in 3 Groups of Varying Habitual Exercise Status: Data of a Cross-sectional Meta-analysis by Wilson and Tanaka. 136
Overall, current evidence suggests that maintaining an exercise regimen into old age may play a role in reducing the rate of decline of VO2peak. However, this may depend on maintaining an intensive exercise regimen into old age, as was noted in the above-mentioned study by Katzel et al. 142 In terms of absolute levels of VO2peak, there is strong evidence to suggest that physically active elderly individuals surpass their sedentary counterparts. This may translate to more successful aging because VO2peak is a critical determinant of dependence/independence in older adults. 58
Prescribing Exercise for the Elderly Patient
Components of a Successful Exercise Regimen
Exercise regimens for the elderly patient should aim to improve exercise capacity, strength, range of motion, balance, flexibility, and QoL while limiting the risk for injury and harmful outcomes. 8 Warm-up and cool-down exercises are important to reduce injury and encourage flexibility. 147
The American College of Family Physicians has released a set of physical activity guidelines for older adults adapted from a similar set of guidelines proposed by the Centers for Disease Control and Prevention. The recommendations have been divided into “Minimum activity for achieving important health benefits” and “Increased activity for achieving additional health benefits.” They can be found in Table 6. 147
American College of Family Physicians Physical Activity Guidelines.
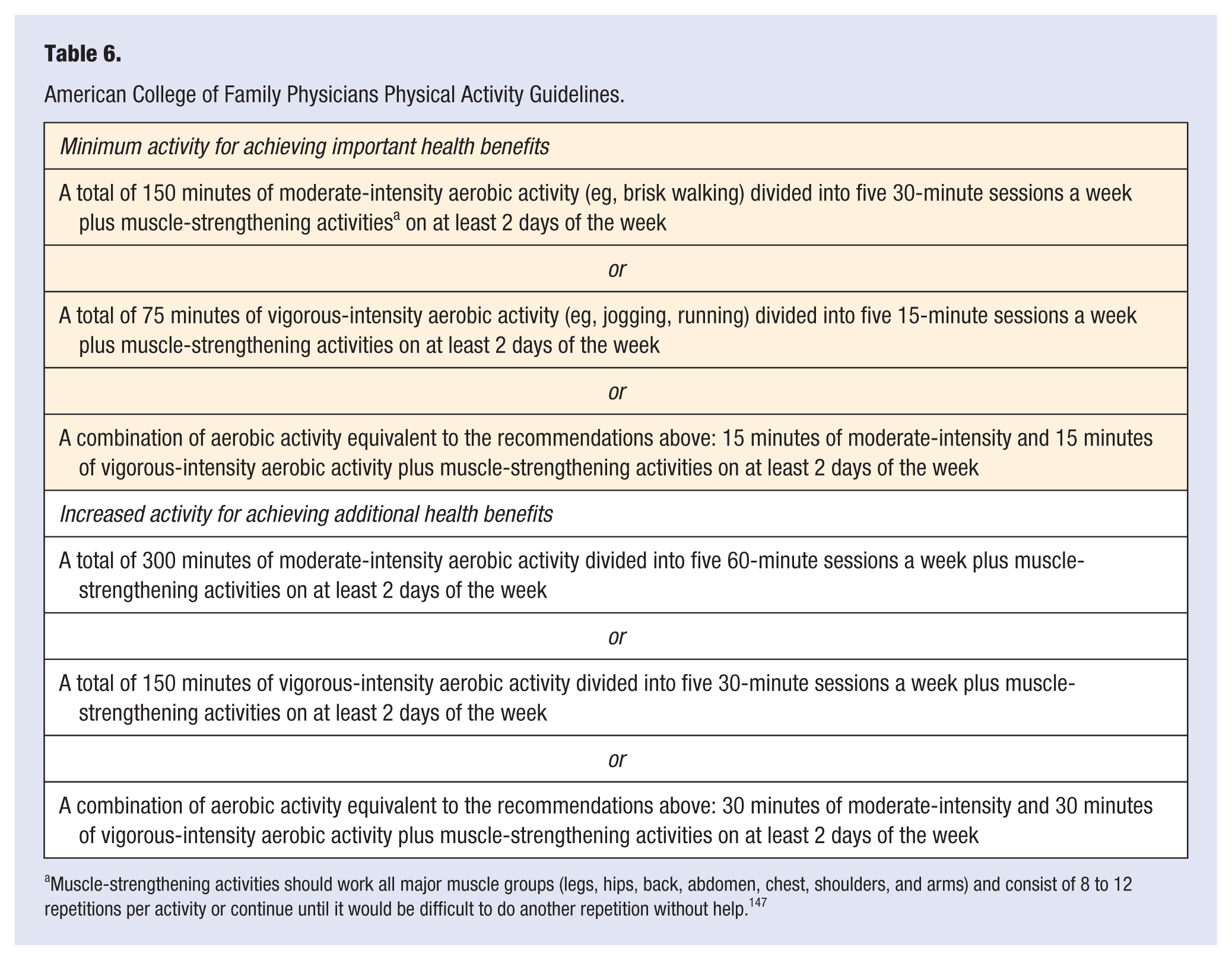
Muscle-strengthening activities should work all major muscle groups (legs, hips, back, abdomen, chest, shoulders, and arms) and consist of 8 to 12 repetitions per activity or continue until it would be difficult to do another repetition without help. 147
Encouraging Adherence to Exercise
A number of variables have been identified as factors that influence the initiation and subsequent adherence to an exercise regimen among elderly populations. This includes social support, self-efficacy, history of physical activity, and knowledge of the benefits of exercise. 148 Physicians play an important role in motivating elderly patients to initiate a regular exercise regimen. 149 In a survey of 301 Medicare beneficiaries, 40% said that they had initiated an exercise regimen because of recommendations made by their physician. 150 Counseling on the benefits and outcomes of exercise programs for elderly populations by their physician improves compliance. 151 Likewise, low rates of physician recommendation of exercise regimens can act as a barrier for older persons. 58 In the United States, low rates of referral to supervised exercise-based cardiac rehabilitation programs have been reported for Medicare beneficiaries. 152 Other barriers to exercise among elderly populations include access to programs and facilities, fear of injury, and self-perception. 10
Contraindications and Screening
Prior to initiating exercise training in elderly populations, each patient’s medical status must be considered, including their current diagnoses, medications, risk factors, and personal goals.8,10,58 In general, the initiation of low-intensity exercise does not require a full evaluation by a physician. A number of contraindications to exercise training in elderly populations have been identified: unstable angina, decompensated HF, critical aortic stenosis, active myocarditis or pericarditis, recent pulmonary embolism, uncontrolled complex arrhythmia, significant ischemic changes on electrocardiogram, uncontrolled systemic or pulmonary hypertension, known cerebral or enlarging abdominal aortic aneurysms, uncontrolled diabetes mellitus, acute or unstable musculoskeletal injury, recent ophthalmological injury, severe dementia, or other significant illness. 8 Also, the development of new symptoms during exercise warrants medical evaluation and reevaluation of the exercise regimen.
Older patients should be screened prior to commencing more intense exercise regimens. The American College of Sports Medicine recommends that anyone >50 years old have a physician-supervised stress test before starting a vigorous exercise program. 147
Exercise for Frail Individuals
Exercise regimens consisting of a mix of aerobic and resistance training should be prescribed based on the frail patient’s current status. 153 Consideration should be given to hand weights, adding hills, or adding arm movements rather than increasing velocity as a means of increasing the intensity of the exercise regimen. 154 In this patient group, an emphasis should be placed on exercise programs that are enjoyable, can be done in groups, and do not result in exhaustion. In doing so, frail patients are more likely to develop a more favorable attitude to exercise and may improve compliance. 153 There is considerable evidence of the benefit of exercise as a means of reducing the risk of falls in frail elderly individuals. 153 A balance and flexibility component should also be included to maximize the potential reduction in falls risk. Short, frequent exercise may be more suitable for frail patients. Initially, exercise may be as short as 6 minutes in duration. As little as 30 cumulative minutes per week have been shown to be of benefit in frail elderly patients. 153 For patients who are unable to complete full body movements initially, isolated movements of the upper and lower body from a stationary position are most appropriate. 153 Among the frail elderly population aged 80 to 100 years in nursing homes, there is an absence of reports of serious CV events, sudden death, myocardial infarction, or exacerbation of hypertension as a result of exercise training. 155
Conclusions
Regular physical activity in elderly populations has the potential to attenuate many of the age-related changes that result in decreased exercise capacity. Maximizing exercise capacity has wide-reaching benefits that address many of the complications, risk factors, diseases, and comorbidities found in aging populations. All older adults, regardless of their frailty and comorbidities, should be encouraged to engage in regular exercise regimens that have been prescribed to accommodate their individual needs and goals. To achieve successful aging in our most rapidly expanding patient population, an increased emphasis on regular exercise in elderly populations is needed.