
Abstract
Despite its pervasiveness in primary care, deficient sleep often is underappreciated as a cue to other health risks. Accordingly, this review discusses contemporary evidence-based perspectives on impaired sleep and its associations with other lifestyle medicine concerns, including obesity, cardiovascular conditions, psychological problems, and health-compromising habits. The potential clinical benefits of promoting sleep health also will be considered.
Keywords
‘Nevertheless, accumulated data now underscore the important role of sleep in a dynamic circadian system that balances environmental responsiveness (eg, to cues such as light) with internal homeostasis.’
Introduction
Sleep is fundamental to health and well-being. With sweeping implications across psychophysiological systems, sleep both critically mediates and reflects biopsychosocial functioning and general quality of life. Indeed, impaired sleep has important links with other medical conditions and harmful lifestyle behaviors. Moreover, the remediation of deficient sleep offers considerable promise for holistic health enhancement. Yet, despite its extensive ramifications, sleep often is underappreciated as an essential aspect of healthy living.1-11
This review first discusses the current status of sleep as a lifestyle behavior, including its sociocultural and developmental dimensions as well as its link with other health-risk and health-protective factors. Next, evidence on improving sleep quality and quantity is discussed with an emphasis on the potential clinical and public health benefits. Given the voluminous extant literature potentially relevant to a discussion on sleep, this review takes a topical rather than exhaustive approach. Specifically, this review emphasizes current evidence-based perspectives on impaired sleep as it relates to common lifestyle medicine concerns (including cardiometabolic conditions, psychological problems, and health-compromising habits) as well as the potential for improving these hazards with optimal sleep. Although the treatment of sleep problems will be briefly mentioned, an in-depth discussion of treatment options is beyond the scope of the current article.
As a prelude to the primary focus, it is worth keeping in mind that the full repercussions of sleep and its disruption remain to be fully unraveled.12-17 Nevertheless, accumulated data now underscore the important role of sleep in a dynamic circadian system that balances environmental responsiveness (eg, to cues such as light) with internal homeostasis.12,14,15-20 Indeed, key system parameters (eg, cardiovascular function, thermoregulation, and glucose metabolism) are marked by circadian oscillations, with profound implications for daily sleep, eating, and activity rhythms as well as neuropsychological modulation essential for cognitive and emotional regulation.13,15,16,19,21,22 (For the interested reader, sleep and circadian science have been comprehensively reviewed elsewhere.12-17)
To be sure, circadian cycles and their disruption are manifested in a variety of guises.15,16 Among some of the most common illustrations are idiosyncratic differences in diurnal propensities. Specifically, individuals with a marked preference for earlier bedtime, awakening, and activity have been characterized as morningness chronotypes. By comparison, those with a penchant for evening activities and later rising have been described as eveningness chronotypes.13,15,16,23,24 Considering that circadian dyschrony has broad-spectrum effects on health and well-being,12,14-22 the developing but very active research focus on diurnal preferences will be reprised in the upcoming discussion of many sleep-related processes and outcomes.
Sleep Epidemiology
Converging evidence indicates that sleep duration and quality generally have declined in recent years.8,12,25-34 Illustratively, the Centers for Disease Control (CDC) reports that approximately one-third of US adults report fewer than 7 hours of sleep per night, with concomitant problems in daily living ranging from unintentionally falling asleep during the day to perceived sleep-related difficulties performing routine activities (eg, problems concentrating at work and/or when driving).1,4 Both laboratory and in vivo studies buttress these perceptions by demonstrating that even acute sleep loss may hinder performance, especially on tasks demanding mental focus and acuity.1,4,7 As sleep debt accrues over time, performance worsens. 7
It is interesting to note that chronic short sleep (fewer than 7 hours per night) is becoming ubiquitous as sleep recedes further into the background of contemporary lifestyle priorities.7,10,12,14,27,28,32-39 Beyond restricted sleep duration, sleep disorders also are widespread across the lifespan, with insomnia and obstructive sleep apnea (OSA) typically ranked among the most prevalent.8,21,28,40-43 Although rates vary somewhat depending on the specific definitional criteria and sample studied, about 30% to 40% of adults report some insomnia symptoms over 1 year, with chronic insomnia among approximately 10% to 15%.8,44 Likewise, breathing-related sleep problems are estimated to affect roughly 20% of adults, at least to some extent,11,45-48 and 10% of children depending on definitional criteria.49,50
Countless pressures currently impinge on sleep time. Some are less negotiable than others. For example, among the extrinsic, potentially less-modifiable influences are increased occupational/educational demands such as extended work/school hours and related travel times, shift work schedules, and required after-hours availability and tasks.7,8,10,12,14,26-28,30,31,34-36,38,39,51-56 However, lifestyle choices also may edge out sleep, including personal orientations toward eveningness (vs morningness), preoccupations with sleep-subverting technologies (such as cell phones and computers), and over-involvement in late-night social activities.7,8,10,12,14,26-28,30,31,34-36,38,39,51-56 Additional sources of sleep disruption (eg, medical and psychological comorbidities) will be discussed later.
Accordingly, the past decade has witnessed escalating public health concern about sleep deprivation and its adverse repercussions across numerous life domains. In addition to the significant impact on individual morbidity and mortality (discussed later in the section on sleep and health), inadequate sleep has been highlighted as a public safety hazard, increasing the risk of accidents and disasters of all kinds.1-4,7,10,21,34,41,42,57-61
Nationally, the estimated economic costs associated with sleep-related injury, health care utilization, and lost productivity have been enormous and rising.1-4,21,34,41,42,57-61 In fact, because of the serious public health ramifications, the National Institutes of Health (NIH) and National Highway Traffic Safety Administration have identified sleepiness and, in particular, drowsy driving as a high priority target for prevention and early intervention.7,10
The Social Context of Sleep
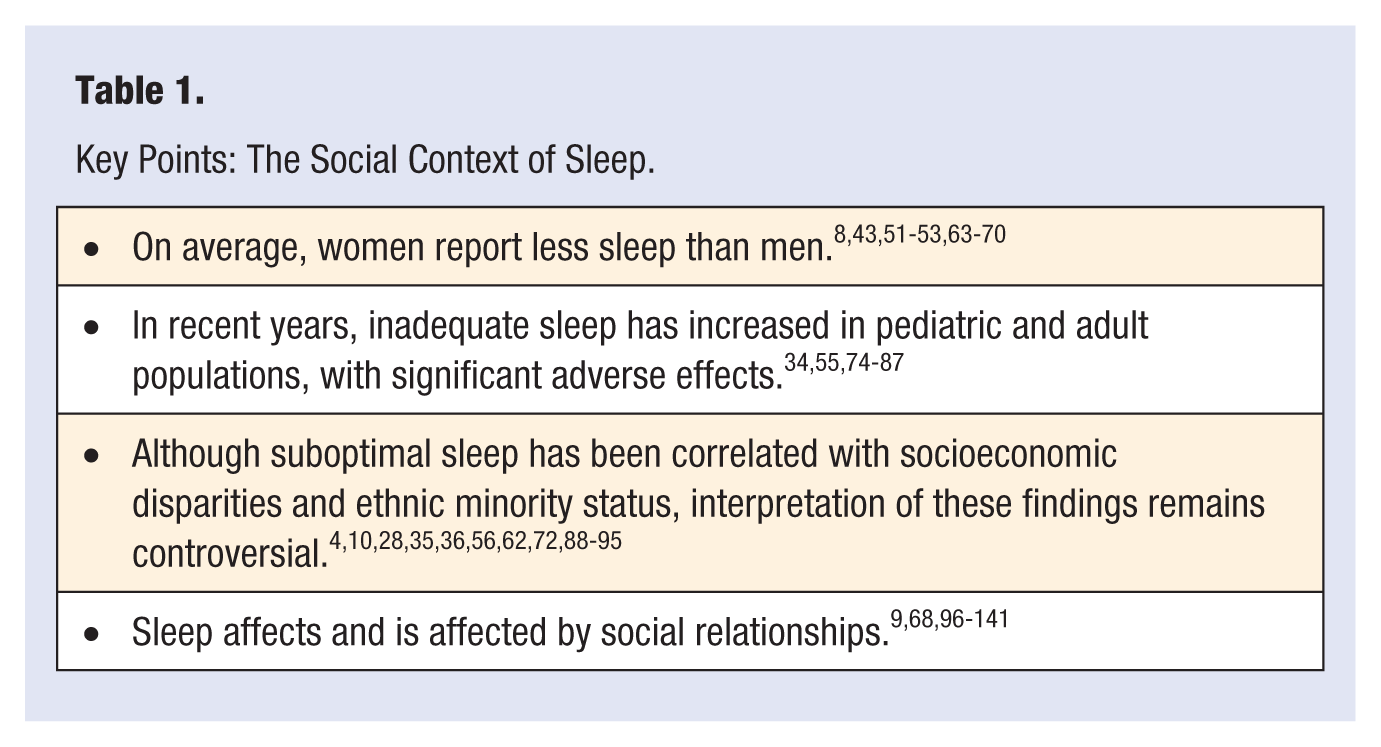
As Stamatakis et al 56 have so aptly noted, sleep may represent a health- promoting “resource whose price is beyond the reach of some segments of the population.”(56p948) Hence, to better understand the risk and protective factors that may affect sleep, considerable recent research has focused on the social context, including sociodemographic correlates, disparities, and co-occurring health quality-of-life indicators.10,55,37,38,56,62 A summary of key findings appears in Table 1.
Key Points: The Social Context of Sleep.
Gender
Most evidence suggests that women experience less sleep than men.8,43,51-53,63-65 Explanations for this gender discrepancy often emphasize women’s lived experiences in which the ascendancy of interpersonal priorities exacts a cumulative toll on health and well- being. For instance, the traditionally asymmetrical distribution of family responsibilities may lead some women to privilege their caregiving roles over their other needs, including sleep.63,64,66-68 Moreover, some research has suggested that, compared with men, women’s relationship dissatisfaction and distress may more readily undermine sleep,9,11,52,69,70 propelled, at least in part, by negatively biased rumination that prolongs presleep arousal.9,51-53,63,68
Finally, despite the paucity of controlled research and reports of considerable within-gender variation, some tentatively have proposed that the gender disparity may be, at least somewhat, influenced by sex and reproductive hormones that differentially affect women’s sleep.8,71,72 On the other hand, certain sleep disorders, especially OSA are diagnosed more often in men than women. 73
Developmental Trends
There has been a recent upsurge in the study and recognition of pediatric sleep problems. Consistent with broader population trends, the prevalence of suboptimal sleep is on the rise among children and adolescents.34,55,74-77 Not surprisingly, youngsters suffering disturbed sleep show age-appropriate biopsychosocial impairments comparable to those of their adult counterparts, including daytime sleepiness, need for weekend catch-up sleep, reduced sense of physical well-being, and neurocognitive deficits often manifested in mood problems, behavioral dysregulation, and academic underperformance34,55,74-77 (discussed in the upcoming section on psychological problems).
In addition to sleep-derailing sociocultural pressures (eg, early school start times, involvement in multiple extracurricular activities), pediatric medical and psychological comorbidities may reciprocally interact with sleep, such that distressing symptoms hinder optimal sleep, and poor sleep predicts increased symptomatology.76,78-80 For instance, chronic pain conditions often are marked by disturbed sleep.76,78 However, deficient sleep also has been shown to influence youngsters’ pain experiences, perhaps at least partially mediated by psychological influences such as mood. 78 Emerging research on developmental psychopathology similarly highlights an association between early sleep difficulties, concurrent emotional distress, and risk for later psychological maladaptation, particularly of the internalizing type (characterized by negative emotionality, social inhibition, and somatization).81,82 The relationship between sleep and psychopathology is the subject of a later section.
Among adults, sleep complaints tend to increase with age. Indeed, some estimates suggest that older age (after 55-65 years) is typically associated with at least some dissatisfaction with sleep quality and/or quantity as well as more daytime somnolence and napping.8,28,65,83,84 These changes have been attributed to the probable confluence of numerous biopsychosocial factors. For instance, polysomnographic findings have confirmed age-related changes in sleep architecture (with a shift toward a greater proportion of lighter rather than deeper sleep) as well as reductions in total sleep time, with increased nocturnal awakenings.28,83,84
Medical and psychological comorbidities, some of which may be more likely with advancing age, also may undermine sleep along with compensatory behavioral shifts (eg, coffee overconsumption) and unhealthy lifestyle habits (eg, physical inactivity, napping, and other counterproductive sleep hygiene practices).28,65,83-87 It is interesting to note that surveys have suggested that older adults may tend to perceive suboptimal sleep more as a predictable consequence of aging rather than a symptom requiring medical attention. 67
Socioeconomic Status (SES) and Ethnicity
Correlations between short sleep, sleep disorders, ethnic minority status, and socioeconomic inequities have been reported. However, interpretation of these findings has been somewhat controversial, given that ethnicity and SES both represent umbrella variables encompassing myriad other potentially sleep-relevant factors at the individual-, family-, neighborhood-, and macro levels such as health status, lifestyle habits, residential circumstances, and life stress (eg, discrimination, unemployment, family strain, financial worries, sleep-disrupting living, and sleep arrangements).4,10,28,35,36,56,62,72,88-91 Although the relative contribution of these potential influences remains to be clarified, efforts are under way.
For example, a recent well-controlled study 89 on the link between self-reported discrimination (overall, regardless of cause) and sleep (objectively and subjectively assessed) in a multiethnic female sample found that the discrimination-sleep association did not differ by race/ethnicity. On the basis of these results, Lewis et al concluded that “although everyday discrimination may not be the only important factor to consider in understanding racial/ethnic disparities in sleep, it does contribute to poor sleep across race/ethnicity. . . . [Thus] discrimination may be an important psychosocial stressor for everyone, irrespective of racial/ethnic background.”89(p816) The topic of stress and sleep is discussed later.
Other attempts to contextualize sleep within its broader ecological niche are driven by increasingly popular social epidemiological perspectives.6,9,56,92-95 To cite just one of many possible illustrations, Hale and Hale 6 contend that the socioeconomic inequities associated with poor sleep share an underlying lived experience in which personal autonomy, empowerment, and opportunity are constrained. Accordingly, they argue, any effort to address the nation’s sleep debt must go beyond a focus on sleep troubles per se to a more comprehensive remediation of underlying sleep-subverting life adversities. Clearly, there is a pressing need for more dismantling work on the constructs of SES and ethnicity to shed light on which aspects destabilize healthy sleep and to advance prevention strategies premised on them.10,62,94
Social Relationships
Decades of research now documents the health benefits of harmonious relationships and social involvement across the lifespan.9,68,96-99 However, conflictual or otherwise unsatisfactory liaisons may engender stress, with its attendant sleep-derailing sequelae.68,94,100-104 (See upcoming sections on morbidity risks associated with suboptimal sleep and on stress and sleep.)
Accordingly, the social dynamics of sleep have become a focus of intense interest.9,51,66,105 To provide a sampling of representative findings in this area, the discussion first will address marital and romantic partners and then family relationships.
Marital/Romantic
Among US adults, sleeping with a partner tends to be more the rule than the exception, 105 despite research demonstrating decrements in sleep architecture during cosleeping compared with sleeping alone.9,105,106 These potentially sleep-disturbing effects are brought into bold relief when one member of the dyad suffers from a sleep disorder. For instance, breathing-related sleep disorders such as loud snoring and OSA (with frequent nocturnal awakenings and restlessness) have adverse sleep and quality-of-life effects on both patients and their bed partners.107-110 Indeed, family members often prompt the patient to initially seek treatment and then adhere to the therapeutic regimen. 111 Likewise, remediation of the patient’s condition (eg, with continuous positive airway pressure has been shown frequently to benefit the sleep of both bed partners, although specific parameters assessed have varied widely from study to study.9,105,107,112 Hence, early intervention and treatment of sleep disorders have extended ramifications reaching well beyond the identified patient.9,105,110,111
As another illustration of social influences, consider the bidirectional connection between sleep and intimate relationship satisfaction. Because neurocognitive, emotional, and behavioral regulation both reflect and affect sleep,9,12,14,17,18,20,44,113-115 it is not surprising that interpartner relationship quality has been related to better sleep both cross-sectionally and longitudinally.9,94,105,112 Although the specific etiological pathways have yet to be empirically established, it has been suggested frequently that mutually satisfying, enduring partnerships may benefit sleep by the reciprocal modulation of psychological, behavioral, and physiological functioning, including both emotional and lifestyle stability.9,94,97
For instance, among happily partnered couples, even temporary physical separation has been associated with perceived stress and sleep difficulties.97,106 Dyadic influences on sleep also have been shown in partner conflict, which may either precipitate suboptimal sleep (by increasing stress and presleep arousal) or result from sleeplessness (via reduced cognitive-emotional self-regulation that lowers the bar for relationship strife).9,105,106,112,116
Interpersonal dynamics also may affect sleep through interpartner lifestyle influences. Indeed, the literature is replete with evidence for the benefits of high-quality marital relationships on mates’ lifestyles, with a traditional emphasis on the partner either as a source of encouragement for healthier choices or as a model that cues the (typically male) spouse’s self-regulation efforts.9,105,117,118 For this reason, significant others often are enlisted clinically to motivate better sleep hygiene behaviors and treatment adherence in patients.65,119
However, an interesting twist on traditional models of partner influence comes from a line of evolving research rooted in chronobiology, which has underscored the sleep-promoting effects of lifestyle regularity and circadian synchronization.9,17,38,105 Specifically, partners may facilitate mates’ sleep by serving as social timekeepers that help maintain regular daily routines (eg, eating schedules, sleep-wake habits, and social activities), such that endogenous circadian rhythms are in step with the exogenous 24-hour cycle.9,12,14,17-19,105 Indeed, circadian misalignment has well-documented detrimental consequences on health and well-being,14-16 as illustrated by individual preferences toward eveningness, which has been linked with circadian desynchronization, poor sleep quality, and a host of psychological and physiological derangements18,51-53,120,121 (discussed in the section on lifestyle). To the extent that partner-provided cues may help regulate important lifestyle routines, these social prompts may serve a sleep-promoting function.
Family Relationships
In contrast to cohesive family environments with routines and mutually affirming interactions, those marked by disorganization and conflict may set the stage for enduring sleep difficulties.53,66,93,113,122-129 Although the actual complexity of contributing factors defies any simple explanation, this type of early life stress has been implicated in numerous vulnerabilities for chronically disturbed sleep.113,122,123,126,128,130,131
To isolate one of many interconnected pathways, a history of family adversity may engender negative emotions that impair cognitive-emotional regulation throughout life.81,82,131,132 These psychological propensities not only subvert sleep in and of themselves but also increase the likelihood of other behavioral and cardiometabolic hazards (eg, imprudent eating, inactivity, and obesity) that may further undermine sleep.131-138 (See sections on morbidity/mortality and on lifestyle below.)
However, considering the reciprocal, synergistic nature of family interactions, it is worth noting that family functioning and parental sleep and stress also may be affected by the number, age, characteristics, and sleep habits of their children.51-53,69,70,124,132 Indeed, an extensive literature reinforces these multidirectional pathways of potential influence.124,125
For instance, Bell and Belsky 124 described a bidirectional relationship between child sleep and family functioning. Specifically, although family stress adversely affected child sleep, pediatric sleep difficulties negatively affected family functioning and maternal well-being, with increasing child sleep problems predicting more maternal mood dysfunction and parenting stress. Consistent with these results, recent research has raised the possibility that children’s chronotype synchronization within the family also may influence maternal sleep-wake rhythms. 139
Other evidence for reciprocal family influences comes from studies on the treatment of pediatric sleep disorders, which have linked better child sleep with posttreatment enhancements in parent and family functioning, including improved parent-reported sleep quality, daytime functioning, and family life satisfaction. It is interesting to note that in some cases, the perceived benefits even generalized to parental perceptions of enriched marital and occupational functioning.9,105,125,140,141
Yet methodological inconsistencies and interpretive conundrums have not gone unnoticed. Among the most frequently mentioned are the challenges associated with subjectively reported data, especially collateral reports such as parent descriptions of child behavior, and restricted samples (small size and homogeneous participants).9,52,66,105,124,125,127,140 Nevertheless, taken together, these findings serve as important reminders that a comprehensive understanding of sleep and its disorders requires consideration of the broader social context in which they occur.9,52,66,105,124,125,127,140
Sleep and Health
Although sleep complaints once were dismissed as an idiosyncratic concern of the “worried well,”142(p934) abundant data now document the hazards associated with sleep dysfunction. Notwithstanding the rapidly evolving nature of this research, a consensus is beginning to take shape around several key points.
Overall, there is clear evidence on the adverse effects of chronic sleep debt,30,31,39 even though an objective, universal definition of optimal sleep remains elusive, partly because of variability in the need for sleep.72,143,144 To the extent that natural short sleepers require substantially less sleep than natural long sleepers, individualized predictions of adequate sleep have been stalled for the time being pending development of more refined sleep deprivation metrics.72,143,144 Nevertheless, research at the population level has provided some evidence-based indications.
Most of the voluminous epidemiological research has highlighted a U-shaped relationship between sleep and health, with both ends of the sleep distribution representing heightened morbidity and mortality risk. Although operational definitions vary somewhat between studies, this range typically translates to an average of fewer than 6 or 7 hours per night (on the short side) and more than 9 hours per night (on the long side).5,29-31,35,36,145 (These findings have been extensively reviewed elsewhere.29-31)
Of course, population-level research is vulnerable to numerous methodological and interpretive criticisms. Among the most frequently mentioned points of contention are questions about direction of causality, possible contributions of unexamined influences, and unconfirmed explanatory mechanisms, notwithstanding some plausible hypothesized pathways.21,26,28,53,61,62,146 Yet the overall consistency and sweep of these epidemiological findings are remarkable.5,10,29-31,35,36,56,142,143,145,146
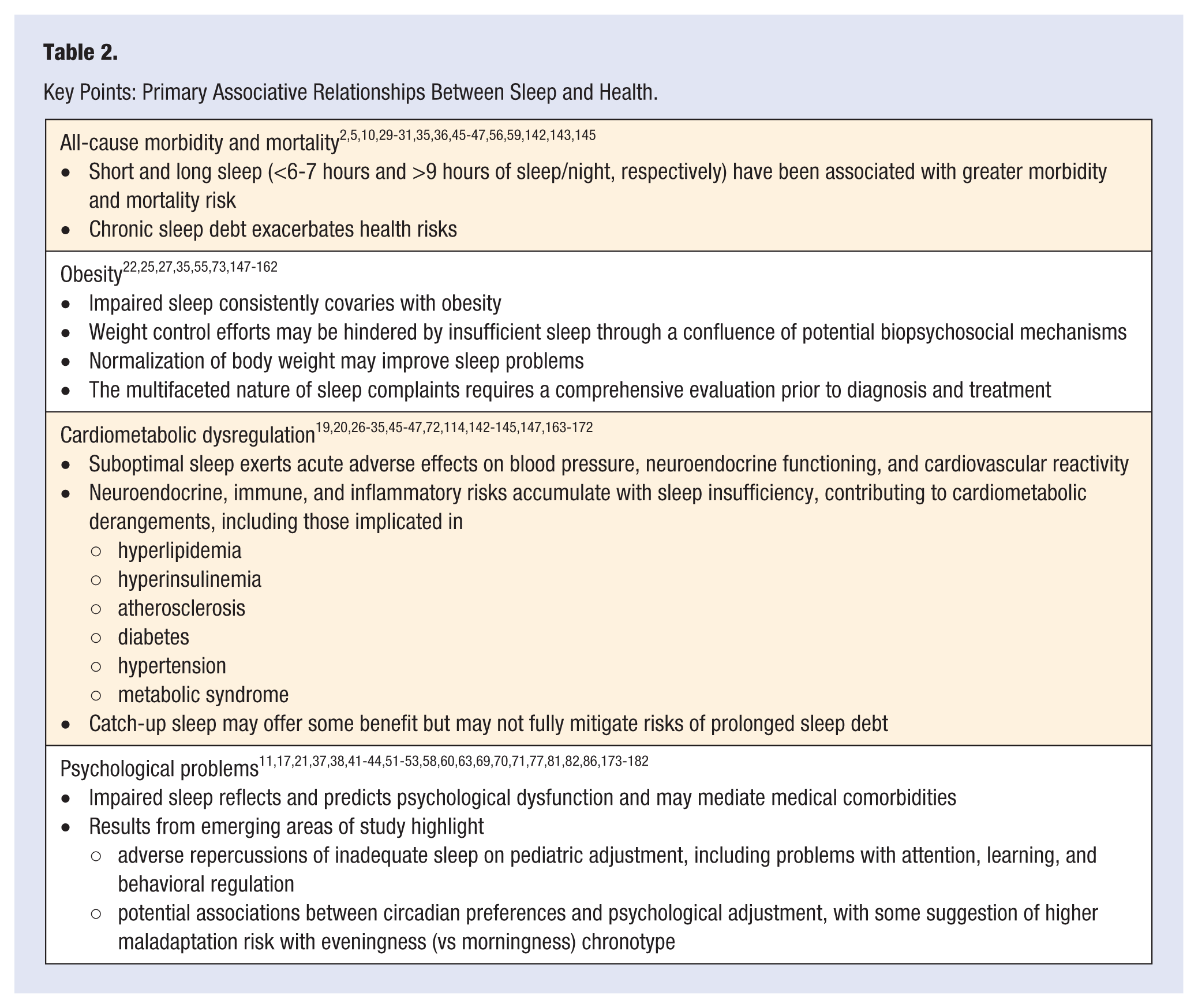
Indeed, deficient sleep has been flagged as a potential risk marker and cue to further action for most of the leading causes of US morbidity and mortality,2,5,10,29-31,35,36,45-47,56,59,142,143,145 including obesity, cardiometabolic dysregulation, and psychological problems. Given the sheer quantity of emerging findings, an exhaustive consideration of this literature is beyond the scope of the present review. Instead, the following discussion surveys recent results from this very active line of developing work that are particularly relevant for the practice of lifestyle medicine. In the process, some especially noteworthy reports will be highlighted for each area. A summary of key findings appears in Table 2.
Key Points: Primary Associative Relationships Between Sleep and Health.
Obesity
Sleep duration has been consistently linked concurrently and prospectively with obesity.22,25,27,35,55,73,147-154 In adult samples, adiposity has been associated with both short and long sleep35,73,153 (focused discussions on this point appear elsewhere 35 ), whereas inadequate sleep duration has been identified as a particularly robust risk indicator among children (albeit somewhat less reliably in adolescents, depending on the study).25,55,149,155,156
Along these lines, there is some indication that suboptimal sleep also may hinder weight control efforts.146,153,156-158 Conversely, compensatory catch-up sleep may attenuate weight gain, perhaps through both physiological and behavioral mechanisms of action. 150
For instance, inadequate sleep may derange metabolism, appetite, and weight-relevant hormones (eg, leptin, ghrelin, and cortisol)22,25,73,147; increase neural responsiveness to hedonic food cues27,148,154; and potentially extend exposure to obesity-promoting environmental cues that prompt health-detrimental dietary habits (eg, snacking, fast-food intake, and low fruit and vegetable consumption).39,72,130,151,153,154 Yet some research has raised the possibility that suboptimal sleep may be better characterized as an independent risk factor for obesity, separate from potential lifestyle influences.151,155-156 Hence, despite the generally consistent covariation between deficient sleep and obesity, mechanisms of action still remain to be empirically elucidated.
Sleep disorders (especially insomnia, OSA, and circadian rhythm disorders) also have been related to obesity in adult and pediatric samples.22,73,147,157,158 For instance, the comorbidity between OSA and obesity is alarmingly high, with OSA prevalence increasing linearly with BMI.73,159
However, in the context of obesity, somnolence may represent a complex symptom reflecting myriad, potentially interacting influences, such as BMI-related cardiometabolic derangements and their pharmacological treatment, co-occurring psychological problems (eg, mood disorders) and their pharmacotherapy, as well as broader health-detrimental lifestyles (eg, inadequate nutrient intake, physical inactivity, poor stress management), each of which must be assessed and, where appropriate, remediated.73,151,152,159 (For interested readers, this point has been thoroughly considered elsewhere. 152 ) Indeed, although sleep symptoms may complicate lifestyle modification efforts, normalization of body weight through lifestyle intervention and/or bariatric surgery improves and, in some cases, resolves many obesity-linked sleep dysfunctions.1,41,42,45-47,73,146,152,157-162
Cardiometabolic Dysregulation
Sleep quantity and quality exert subtle but cumulatively significant effects on cardiometabolic regulation.163-171 Although epidemiological evidence supports a U-shaped relationship between sleep, morbidity, and all-cause mortality5,29-31,35,36,145 (systematic review and meta-analysis appears elsewhere 5 ), much recent attention has been riveted on habitual short sleep and its potential relationship to the neuroendocrine, immune, and inflammatory markers that undergird many of the well-established health harms (such as hyperlipidemia, hyperinsulinemia, atherosclerosis, diabetes, hypertension, and metabolic syndrome).19,20,26,27,29-33,45-47,72,114,142-145,147,163-171 (Specific cardiometabolic conditions have been reviewed elsewhere.5,29,32,35,48,72)
Even acute sleep restriction has been associated with elevated blood pressure, neuroendocrine dysregulation, and cardiovascular reactivity.26,163,164,172 Although the route to postdeprivation sleep recovery remains uncertain and algorithms quantifying the potential process have yet to be mapped out, 35 daytime catch-up sleep may attenuate some of the derangements that typically presage downstream adversities.32,33,45-47,163 Yet in the context of chronic sleep debt, sporadic sleep episodes may not completely mitigate metabolic and immunological risk markers, leaving a trail of small but significant changes that cumulatively tilt the odds toward cardiometabolic disease.32,33,45-47
Psychological Problems
Sleep difficulties are a ubiquitous part of the diagnostic criteria defining many different psychological disorders. Indeed, sleep troubles figure prominently in problems as diverse as ADHD (attention-deficit hyperactivity disorder), personality, anxiety, mood, and psychotic disturbances.11,21,37,38,41-44,53,58,69,70,71,81,86,173-182
Considering the intricate bidirectional relationships between sleep and cognitive-emotional regulation, it is not surprising that suboptimal sleep would both reflect and foreshadow psychopathology in its protean manifestations.17,21,38,51-53,60,63,77,81,82,114,175,179,180,182-185 In fact, converging evidence highlights the diagnostic relevance of sleep problems across the life span, the neglect of which may hinder timely identification of maladaptation, complicate treatment, heighten relapse risk, and obscure a potential mediator in the psychological-medical nexus.38,133,172,176,178,180,183,184,186
The complexity of these synergistic transactions is remarkable. To single out one of many possible illustrative threads from a richly textured background, deficient sleep has been identified as both a predictor of negative psychological states (eg, depression) and a mediator of many cardiovascular morbidities to which it relates (eg, hypertension).172,174,187
Currently, research on the complicated associations between sleep and various types of psychological dysfunction represents a very active concentration of study with rapidly developing advances. Among some of the most intriguing recent findings are those linking suboptimal sleep with suicidal thoughts and completion,17,21,69,86,176,188 geriatric cognitive decline,60,168,189-192 and pediatric neurocognitive and behavioral maladaption.49,50,74,191,195,196 (Neurocognition in adult193,194 and pediatric49,195 samples have been reviewed elsewhere.)
Of these cutting-edge areas, the pediatric research is especially provocative in underscoring the repercussions of inadequate sleep and sleep-disordered breathing (even at subclinical levels) on children’s learning and behavior problems (particularly difficulties involving inattention, aggression, and hyperactivity).50,74,191,192,196,197 It is interesting to note that in many cases, treatment of sleep-disrupting medical problems (eg, via adenotonsillectomy, amelioration of upper-respiratory infections, and allergies) has shown considerable promise for improved neurocognitive and behavioral adaptation, even though remediation of delayed developmental tasks and/or skills may be necessary.49,50,195,196 Beyond the obvious implications for academic adjustment and broader well-being, these findings sound a cautionary note in the diagnosis of pediatric maladjustment (especially deficits in attention and behavioral regulation) without a thorough biopsychosocial assessment, including the comprehensive evaluation of sleep.40,49,180,191,195-197
Another novel line of developing research has focused on circadian preference as a potential marker of psychopathology risk. Here, evidence points to the eveningness chronotype as a liability for numerous sleep-related and psychological problems, such as mood, anxiety, substance use, and personality disorders as well as externalizing personality traits (eg, inattention, impulsiveness, and sensation seeking). Conversely, based on its repeated link with emotional stability, conscientiousness, and positive emotionality, morningness may bode well for psychological adjustment.51-53,92,93,198-216 However, as an evolving area of study, many unanswered questions remain regarding diurnal preference and psychopathology, including specification of potential mediators, possible developmental trajectories, and the reciprocal gene-environment interactions that, no doubt, are involved.51-53
Taken as a whole, the growing recognition of potential sleep-psychopathology synergies has importantly contributed to science and practice. Yet, despite its progress, this literature has not escaped methodological and interpretive critique aimed, for example, at sample limitations (eg, size and representativeness), measurement inconsistencies (eg, objectively assessed vs subjectively reported sleep and other symptoms), potentially unexamined confounds (eg, health conditions and medication side-effects), design discrepancies (eg, cross-sectional vs prospective), and their associated implications for attributions of causality and explanatory pathways.38,182,188,189 That said, this remains a promising area for advancing patient care as well as galvanizing efforts to promote sleep health.4,5,28,34,61,62,217
Sleep and Lifestyle
Suboptimal sleep not only is robustly related to leading morbidity and mortality indicators but also significantly covaries with other aspects of lifestyle, including stress, tobacco use, harmful eating habits, physical inactivity, and atypical work routines.1,4,10,28,54,61,144,218-220
Stress and Coping
The National Sleep Foundation 8 estimates that half of those reporting insomnia attribute their sleep problems to stress and worry. Congruent with this report, numerous studies have noted an association between suboptimal sleep, daily stress, and presleep arousal,28,34,43,51,63,81,126,144,186,221,222 with some evidence-based suggestion that chronic sleep deficiencies and prolonged stress exposure may exacerbate physiological wear and tear with predictable broad-spectrum health-detrimental effects.126,144,223,224 Of course, health problems also may heighten sleep difficulties and perceived stress.51-53,126,144,151,223,224
In keeping with the stressful life events research tradition, much of the work on the sleep-stress nexus has accentuated the sleep-subverting effects of assorted negative life events, including medical problems,78,186 financial strain,130,225,226 discrimination,89,227 family stress and childhood adversities,53,81,82,126,130,132,133,228 and accidents and other tragedies,34,184 just to name a few. However, studies focused on life events per se often are not designed to fully account for the interindividual differences in subjective appraisal that shape stress perceptions. For instance, when exposed to the same event, some may perceive stress where others perceive challenge or opportunity, with differing repercussions on sleep and broader health.81,89,150,229
Likewise, life events research may not fully capture potential bidirectional relationships between stress and sleep. That is, although negative life events may destabilize sleep, suboptimal sleep may derail cognitive-emotional regulation, thereby reducing coping effectiveness and potentially increasing actual or perceived stressful encounters.51,81,88,132,185,225,226,229 Illustratively, sleep difficulties have been shown to presage later psychological maladaption.11,38,58,82,174,180,185
Accordingly, the thrust of recent work progressively has shifted toward a more comprehensive perspective on the stress-sleep relationship. From this evidence-based vantage point, sleep problems are rooted in a synergy of individualized susceptibilities and exposures, such that idiosyncratic pre-existing liabilities (especially anxiety proneness, negative emotionality, and other tendencies toward psychological and physiological hyperarousal) complexly interact with perceived stressful encounters to undercut sleep. These emergent difficulties may be maintained or even exacerbated by maladaptive habits and coping propensities (eg, harmful lifestyle behaviors, cognitive rumination, negative emotionality, and dissonant social interactions).41,42,44,52,65,81,105,114,115,181,222,224,229,230
Clearly, more research is warranted to further elaborate the complex web of biopsychosocial risk and resilience factors affecting sleep. Clinically, the evidence for robust idiosyncratic differences emphasizes the need for an individualized assessment matched with multidisciplinary interventions tailored to the factors most relevant to each person.41-44,65,86,114,115,119
Tobacco/Nicotine Use
The relationship between sleep and nicotine use frequently has been described as a vicious cycle.71,231 Studies on current nicotine consumers (smokers and smokeless users) have revealed a high prevalence of sleep problems (especially insomnia and breathing-related sleep disorders) in users compared with their abstinent counterparts.133,147,177,220,231,232-235
However, deficient sleep also exacerbates smoking urges. 234 In this regard, smoking cessation research has suggested that the sleep problems and nocturnal arousals associated with nicotine withdrawal may nudge relapse odds beyond the tipping point, foiling even the best of quit intentions.71,232,233 (Detailed discussions on this point appear elsewhere. 71 ) Efforts to better understand these relationships are high priorities in the search for innovative nicotine cessation strategies.71,231-233
Above and beyond the profound ramifications of direct nicotine use, both in utero and second-hand exposure take a considerable toll on nonsmokers’ sleep and broader health. For instance, maternal smoking during pregnancy may raise the risk of low birth weight and sleep respiratory disorders in neonates and may also have broader downstream repercussions such as cognitive difficulties and obesity, with their own deleterious implications for sleep.236-239 Although the specific mechanisms remain to be empirically clarified, it is widely suspected that toxic tobacco exposures during critical developmental periods may adversely alter neurological and cardiometabolic programming, further complicating sleep risk pathways.237-239
Similarly, among infants and children, secondhand smoke is a well-documented hazard for sudden infant death syndrome (SIDS), sleep-related breathing disorders, upper-respiratory infections, and compromised lung function.177,197,240-242 Adult nonsmokers also are jeopardized by secondhand exposure, suffering disordered sleep, pulmonary difficulties, and cardiovascular derangements, just to name a few.177,240,241
Nutrient Intake and Eating Behaviors
As discussed, inadequate sleep has been shown to increase appetite, biasing attention and vulnerability to hedonic food cues.25,27,39,72,120,148,153,154,205,211,243 (Detailed discussions on this point appear elsewhere.72,153) In terms of specific dietary habits, deficient sleep has been linked with the intake of increased calories, saturated fat, snacks, soda, and fast food as well as with low fruit and vegetable consumption.130,153,155,156,244-246 By comparison, balanced prudent diets emphasizing whole foods may benefit sleep.247,248 (For interested readers, a thorough review appears elsewhere. 248 )
Although the explanatory pathways have yet to be confirmed, extant evidence indicates several plausible mechanisms potentially linking suboptimal sleep with unhealthy eating habits. Beyond the contributing physiological mediators previously discussed, sleeplessness may extend sheer exposure to palatable food prompts. In an environment saturated by unremitting cues for imprudent eating, more time awake may translate into more screen time and contact with predatory junk food advertising and other situational dynamics that promote health-detrimental food choices.150,153,249 Of course, nutrient-void diets also may lead to sleep-derailing feelings of malaise. Hence, reciprocal synergistic influences are likely.152,250
Beyond the correlational findings, emerging laboratory data are especially compelling in demonstrating a sleep-nutrition link. For instance, consumption of saturated fatty acids has been shown to adversely affect glucose metabolism and sleep-wake architecture in animals. By comparison, monounsaturated fatty acid–enriched diets benefited both metabolism and sleep, independent of obesity status. 251 Although direct generalizations to humans are premature at the present time, these laboratory findings are provocative and congruent with broader support for the health advantages of high-quality dietary fats.248,252,253
Amid the burgeoning literature on diurnal preferences, eveningness chronotype has been identified as a potential risk marker for unhealthy dietary practices, including consumption of more caffeinated beverages and inadequate intakes of vitamins, minerals, fiber, and protein.230,243,245,254-257 In addition to specific nutrient patterns, research on eating behavior has suggested that evening orientation may covary with eating disinhibition, perceived hunger, difficulties adhering to a healthy diet, and risk for eating disorders. In contrast, the morningness chronotype has been associated with more flexible control of eating behaviors, more meal regularity, and healthier food choices.230,243,245,254-258 Unfortunately, much of this literature has not yet examined possible reciprocal influences.
Nevertheless, to the extent that social and contextual time cues may entrain diurnal rhythms,13,15,16 it makes sense that eating habits may be part of this dynamic timekeeping process. Although findings are just beginning to coalesce, there are tantalizing hints that the regularity, timing, and nutrient composition of meals may serve as one of many extrinsic time cues.15,16,255,256,259
It is interesting to note that caffeine and other substances have been seen to affect melatonin levels. 15 Likewise, covariations have been reported between chronotype tendency and morning routine, with morningness linked with probability of breakfast consumption and eveningness with breakfast skipping.150,259,260 However, the interpretation of this broad association remains controversial, with many unanswered questions about the influence of possible mediators (such as breakfast nutrient composition and postbreakfast sunlight exposure 259 ), directions of causality, and the potential for chronotype modification, just to name a few.259,260 Given the nascent stage of this research area, conclusions probably are premature at the present time.
In sum, the relationship between sleep, nutrient intake, and eating behavior is an interesting, emerging area of study that merits further investigation to confirm extant results in larger, more diverse samples; explore possible confounding influences; and elucidate pathways of influence.
Exercise
Although some incongruous findings have been noted, the preponderance of empirical evidence has suggested a relationship between suboptimal sleep and physical inactivity. Generally speaking, epidemiological findings have supported this link. By comparison, results of experimental studies have been somewhat more mixed, in part, because of divergent methodologies, including various setting characteristics, exercise types (eg, differing modalities, intensities, and durations), participant characteristics, and sample sizes.1,4,160,168,220,261-263 (A detailed discussion on this point appears elsewhere. 263 ) Among developing areas of study are some reports on the potential sleep benefits of nontraditional exercise modalities (eg, yoga and mindfulness movement-based approaches)161,264 as well as a possible connection between eveningness chronotype and sedentariness.120,230,265
From an evidence-based clinical perspective, regular physical activity has long been widely prescribed as an effective sleep hygiene habit to prevent sleep difficulties and as a first-line treatment for emergent sleep problems.43,65,261,266 Conversely, treatment research has affirmed frequently that suboptimal sleep may represent an important barrier to healthful living.146,153,157
Although research has only just begun to trace the contours of potential explanatory pathways, attention increasingly has focused on several prime suspects at or near the epicenter of the sleep-exercise nexus. For example, the anxiolytic and mood-boosting effects of exercise may translate into better sleep.63,83,161,168,182 It is also plausible that activity-induced ameliorations in metabolism, adiposity, energy, and physical endurance may confer sleep benefits.83,153,165,167,168 Clearly, an understanding of mediating factors and pathways of influence remain works in progress pending further study.
Atypical Work Schedules
Shift work is common worldwide and becoming increasingly prevalent as businesses attempt to serve consumer demand. Indeed, estimates indicate that about 25% of employees may work atypical schedules, with many on the job for at least 10 hours each day.7,8,14,266-268 Shift workers frequently report sleep-related problems such as sleep deprivation, poor sleep quality, fatigue, depressed mood, and impaired cognition (eg, reduced concentration and reaction time),7,8,14,267,268 resulting from the synergistic effects of disturbed sleep and circadian misalignment.12,14,32,33,58,268,269 Paradoxically, it has been observed that long atypical shifts are especially characteristic of those professions requiring quick cognitive acuity in life-threatening situations (such as law enforcement, medical/emergency services, and the like).7,8,14,267-269
Over and above the adverse effects on job performance, shift workers suffer increased rates of morbidity and mortality—for example, secondary to cardiometabolic conditions, gastrointestinal disorders, some types of cancer, and drowsy driving accidents.7,8,12,20,32,33,58,268 Although a certain amount of shift work tolerance may develop in some individuals, the cumulative repercussions of long-term circadian dyschrony and sleep debt may not be fully neutralized.14,32,33,229,268,270 Accordingly, there is a pressing need for continued research on atypical work schedules, including a more refined delineation of the person-environment dynamics that may mediate acute and downstream ramifications for different shift workers.12,14,20,32,33,58,229,268-270
Intervention
As previously noted, an in-depth discussion of treatment options is beyond the scope of the current article. (Sleep disorder treatments have been extensively reviewed elsewhere.41-43,271-276) However, given the prevalence of sleep complaints in primary care,41-43,271,275 a brief mention of treatment seems warranted.
Pharmacological Treatment
Awareness of pharmacological treatments for insomnia and other sleep concerns is ubiquitous.271-276 Primary care patients may express familiarity with and interest in pharmacological sleep aids. Likewise, providers still predominantly rely on pharmacotherapy in primary care, where most sleep complaints are initially managed.41-43,271,275,276 Pharmacological treatments (including safety and efficacy comparisons, recommended doses, etc) have been extensively reviewed elsewhere.271,272,275 Here, suffice it to say, a variety of pharmacological options are available, including those that have been approved by the Food and Drug Administration for specific sleep indications (eg, benzodiazepine receptor agonists for insomnia) as well as those used off-label (eg, sedating antidepressants used for insomnia).41,271-273
Although brief pharmacotherapy may be helpful for some patients, there are disadvantages to an exclusive reliance on pharmacological approaches. For example, all medications have potential adverse side effects, especially in vulnerable (eg, pediatric and geriatric) populations for whom risks may outweigh benefits.41-43,271,272,274 Indeed, given the widely noted discrepancy between the chronicity of many sleep problems versus the limited duration of most clinical trials,271-275 extended medication management has become increasingly controversial.271-276 Because sleep symptoms tend to recur when medications are discontinued, the benefits of pharmacotherapy may be transient, at best.41-43,271
Accordingly, over the past decade, various professional groups (including panels convened by the NIH, 275 American Academy of Sleep Medicine, 273 and the National Sleep Foundation 274 ) have released reports repeatedly reaffirming the effectiveness and centrality of nonpharmacological (psychological and behavioral) approaches in the comprehensive management of sleep concerns. For example, in 2005, an NIH review 275 concluded that cognitive behavior therapy (CBT; discussed in the next section) is “as effective as prescription medications . . . for brief treatment of chronic insomnia”275(p1052) and that “the beneficial effects of CBT, in contrast to those produced by medications, may last well beyond the termination of treatment,”275(p1052) with no extant evidence of adverse side effects. 275 More recent reviews41-43,271,276 have further reinforced the importance of cognitive and behavioral self-management skills for initiating and maintaining healthy sleep.41-43,271,276
Unfortunately, both provider and patient barriers often undermine the widespread adoption of nonpharmacological approaches in primary care. Providers may perceive a lack of time, expertise, and resources to provide behavioral treatments.41,68,131,249,271,275 Even if nonpharmacological options are offered, some patients may request medications for more rapid symptom relief compared with the somewhat slower-to-emerge benefits produced by sustained behavior modification. For such patients, accepting and adhering to lifestyle recommendations may be especially challenging, particularly if insurance reimbursements privilege less costly prescriptions over nonpharmacological care that typically demands more dedicated resources (eg, provider and/or staff time and expense).41-43,276 However, some other patients may find a cogent rationale for behavioral interventions fully compatible with their preferences for holistic care,131,271 a topic to which the discussion now turns.
Lifestyle Interventions
The synergistic relationship between sleep and other traditional risk factors has important public health implications, given the extent to which a few hazardous lifestyle behaviors affect the nation’s morbidity/mortality and the substantial benefits that could accrue from their modification.10,70,91,148,170,277-282 Although an in-depth discussion of treatment options is beyond the scope of the current article, it is worth noting that some lifestyle intervention trials targeting other traditional risk factors (eg, unhealthy diets, inactivity, and tobacco use, either in isolation or combination) have noted improved sleep among their broad-spectrum benefits.45-47,83,161,162,283,284 In addition to the short-term advantages, some of these interventions focused on diabetes, obesity, and OSA have reported promising durability, typically 1 year posttreatment.45-47,283,284 A summary of illustrative studies appears in Table 3.
Illustrative Lifestyle Interventions With Reported Sleep-Related Benefits.
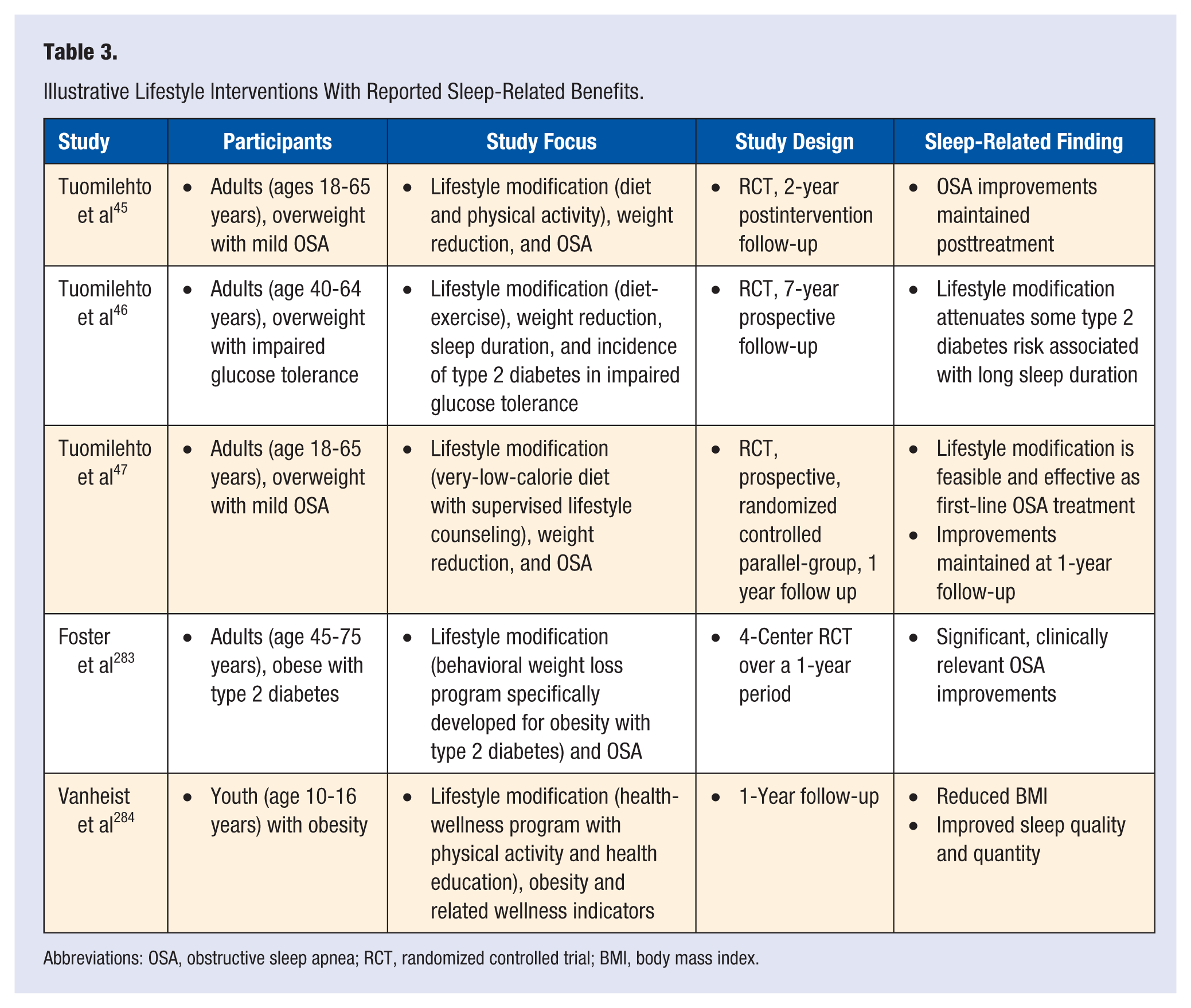
Abbreviations: OSA, obstructive sleep apnea; RCT, randomized controlled trial; BMI, body mass index.
Given these encouraging findings, there is a clear need for continued research on the lifestyle amelioration of suboptimal sleep, including systematic comparisons of different options (eg, diet, exercise, and various combinations) and the specification of dose-response relationships.45-47,83,161,162,283,284
In a similar vein, CBT has not only demonstrated efficacy for treating sleep troubles but has also been found to improve the management of medical and psychological comorbidities.41-44,65,86,114,115,119 As one of the most widely used evidence-based treatments, CBT takes a biopsychosocial approach to the treatment of sleep (and other) problems that encompasses premorbid vulnerabilities, lifestyle, and coping propensities. (CBT and its efficacy for the treatment of sleep problems have been extensively reviewed elsewhere.41-44,114,115,273,275,276) Given this holistic focus, it is not surprising that these results are compatible with those reported in the lifestyle modification literature just discussed.43,44,114,178 Taken together, these findings highlight the force-multiplying potential of relatively modest lifestyle improvements for ameliorating the nation’s current sleep debt and its associated comorbidities.
Conclusions and Future Directions
The associations between deficient sleep and other health risk conditions highlight disordered sleep as a potential marker of health liability across the life span.1-10,174,280 For front-line health care providers, this evidence accentuates the clinical relevance of sleep duration and patterns in the overall assessment of patient risk.1,4,61,62,280
Although the relationship between sleep and other disorders is largely correlational at the present time, the potential clinical benefits of improved sleep are relatively broad and holistic. In this regard, lifestyle modification is an especially attractive first-line treatment given its broad-spectrum, beneficial effects on impaired sleep and its comorbidities (eg, obesity, cardiometabolic, and psychological problems).68,118,277-284 As a further advantage, lifestyle approaches (eg, incorporating more activity into daily routines and successively approximating a Mediterranean-style diet) are associated with few risks. For these reasons, lifestyle interventions are well suited for pediatric and adult patients, in contrast to some pharmacotherapeutics.131,249,277-284
Unfortunately, lifestyle approaches to the management of sleep (and other health risk behaviors) are often underutilized in practice settings. Although the current care milieu presents barriers, provider recommendations for health behavior change do stimulate patient lifestyle improvements, especially when advice is explained in terms of each patient’s specific medical condition.68,131,249 Moreover, when sustained, provider coaching and encouragement for incremental lifestyle upgrades can yield significant clinical benefits across multiple risk factors.131,249,277-284
However, prioritizing the routine assessment and management of insufficient sleep will require action on multiple fronts.1-10 There is a crucial need to advance understanding of the myriad influences on sleep dysfunction and to further refine evidence-based heuristics for their assessment and management. This includes improved methodologies for evaluating and addressing the biological, psychological, and social factors specific to each individual.1-10,15,16,51-53,72
For instance, the increasing infusion of personalized medicine into routine clinical care holds promise for heralding an era more intent on matching individual somnolence susceptibilities with best-fitting treatment modalities. Toward this end, a sole reliance on self-reported sleep complaints may gradually give way to newer technological developments, such as the identification of biomarkers and other actionable variants to assess idiosyncratic sleep needs, guide individualized treatment planning, and track its progress.53,72
In addition, efforts to recalibrate the public’s sleep habits will be essential. Although educational outreach is basic, bridging the gap between information uptake and behavior change will require further development of ecological approaches that address sleep problems contextually at the individual, community, and macro levels.1-10,94,95,105