
Abstract
“ Physical inactivity was more strongly associated with hypertension in middle-aged adults than in older adults.”
Background
Hypertension is a major public health concern in the United States contributing, significantly to cardiovascular disease, stroke, and early mortality.1,2 The prevalence of hypertension increases with age, affecting 54.5% of adults aged 40 to 59 and 74.5% of those 60 and older. 3 Age-related factors such as increased vascular rigidity, endothelial dysfunction, and cumulative lifestyle exposure increases the odds of developing hypertension. Consequently, the prevention and management of hypertension become particularly crucial in the aging population. 4 Despite advancements in hypertension treatment and health education strategies, population-level control remains insufficient. This highlights the need for tailored modifiable lifestyle strategies for middle and older adults who have the highest prevalence of hypertension. 5
Physical activity and sleep are key modifiable health behaviors that influence the likelihood of developing hypertension.6,7 Regular physical activity improves blood circulation, facilitates healthy weight management, and consequently lowers blood pressure.8,9 Among adults aged 40 years and older, higher levels of physical activity are associated with reduced morbidity and mortality from hypertension related cardiovascular disease, leading to improved survival rates.10,11 Adequate sleep, defined as 7 to 9 hours of sleep per night for adults, 12 has been linked to better blood pressure management. In contrast, both short (<7 hours per night) and long sleep (>9 hours per night) are associated with dysregulated blood pressure and increased odds of hypertension.13,14 In the United States most adults sleep for short duration due factors such as insomnia, night shifts, and sleep disorders like obstructive sleep apnea, all of which increase odds of hypertension. 15 These issues are especially common among middle-aged and older individuals, who often experience changes in sleep patterns and circadian rhythms, further increasing their susceptibility to hypertension.16,17
Age-related changes in both sleep and physical activity further compound the likelihood of hypertension among middle-aged and older adults. 18 Middle-aged adults often have reduced physical activity due to occupational and family demand, whereas older adults may face limitations from comorbidities and decreased mobility.18,19 Simultaneously, sleep quality generally deteriorates with age, resulting in fragmented rest and altered circadian rhythms. 20 Furthermore, physical activity and sleep are interrelated: regular exercise can improve sleep quality, while inadequate sleep may reduce the cardiovascular benefits of physical activity. 21 Understanding these interactions is essential for developing effective lifestyle interventions aimed at mitigating hypertension.
Although substantial evidence supports the individual benefits of physical activity and sleep, their impact on hypertension in middle-aged and older adults respectively remains understudied. Most research have examined these factors separately overlooking potential differences in their roles for hypertension among middle-aged and older adults.22,23 Hypertension is more prevalent in older age; however, middle age is the life stage in which hypertension start to emerge. The same lifestyle factors may play different roles in the likelihood of hypertension among different age groups.
Addressing this gap is crucial to offer age group sensitive insights that can guide prevention and management strategies during periods of increased exposure to cardiovascular diseases. Therefore, the purpose of this study was to examine the association between physical activity, sleep and hypertension among middle and older adults in the United States for both middle-aged and older population as well as the two age groups separately. The specific aims were: (1) to examine the association between physical activity levels and hypertension prevalence; (2) assess the relationship between sleep duration and hypertension; and (3) evaluate age-specific association between physical activity, sleep, and hypertension among U.S. middle-aged and older adults.
Methods
This study presents a cross-sectional analysis of data from the National Health and Nutrition Examination Survey (NHANES). The earliest NHANES data were collected between 1971 and 1974. Since 1999, the Centers for Disease Control and Prevention (CDC) has continuously collected NHANES data in 2-year cycles from a nationally representative sample of the civilian, noninstitutionalized U.S. population.24,25 The study protocol was reviewed and approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board. All participants provided written informed consent prior to enrollment. The survey’s multistage probability sampling design ensures that data are representative of the civilian, noninstitutionalized U.S. population. 25 We conducted an analysis of data from 3 consecutive NHANES cycles (2013-2018). More details of the sample are described in the analytics sample section.
Measures
Outcome Variable: Hypertension
Certified clinicians conducted blood pressure measurements in the mobile examination center (MEC) using a mercury sphygmomanometer and appropriately sized cuffs, following standardized American Heart Association (AHA) protocols. Participants were seated and rested for 5 minutes before measurement. Three consecutive readings were taken at 30-second intervals, with a fourth taken if any reading was incomplete. The mean of the 3 valid readings was used to calculate systolic and diastolic blood pressure. Variables from the NHANES used for this assessment include BPXSY1, BPXSY2, BPXSY3 (systolic) and BPXDI1, BPXDI2, BPXDI3 (diastolic). Hypertension was defined according to the 2025 AHA/ACC guideline as SBP ≥130 mmHg, DBP ≥80 mmHg, or current use of antihypertensive medication. 1 This study focused on adults with current hypertension, identified through MEC blood pressure measurements or ongoing antihypertensive therapy. Participants who reported “ever been told by a doctor or other health professional that they had high blood pressure” were not classified as under hypertension unless they met the current measurement or medication criteria, as prior diagnoses may have resolved or been transient.
Independent Variables
Physical Activity
Physical activity was measured using the Global Physical Activity Questionnaire (GPAQ), adapted from the World Health Organization. 26 The NHANES questionnaire captures self-reported aerobic physical activity over the past 30 days across leisure, work, transportation, and recreational domains. Data on muscle-strengthening or balance exercises are not available for the current cycle included in this study and therefore were not reported in this analysis. Participants reported the number of days per week and average duration per day for vigorous and moderate activities, as well as walking or biking for transportation. Weekly minutes for each activity type were calculated by multiplying frequency by duration and converted to metabolic equivalent (MET) minutes per week (MET-min/week) using standard NHANES-recommended MET values (8 METs for vigorous, 4 METs for moderate and transportation activities). Total weekly MET-minutes/week were summed across all activity types. Participants were categorized according to physical activity guidelines (PAG): below physical activity guidelines (<500 MET-min/week), meeting physical activity guidelines (≥500-999 MET-min/week; reference), or exceeding physical activity guidelines (≥1000 MET-min/week). 27 This approach allows assessment of dose–response effects, as exceeding guideline levels may confer additional cardiometabolic benefits, including improved blood pressure regulation.27,28
Sleep
Sleep duration was assessed in NHANES using self-reported data collected during household interviews. Participants answered the question, “How much sleep do you usually get at night on weekdays or workdays?” (NHANES variables SLD010H and SLD012). Sleep duration was categorized as short (<7 hours/night), recommended (7-9 hours/night; reference), or long (>9 hours/night), consistent with guidelines from the American Academy of Sleep Medicine and the American Heart Association recommendation for sleep.1,29
Covariates
The covariates considered in this study included age, gender, race/ethnicity, marital status, education, income, health insurance status, and diabetes status. Age (RIDAGEYR) was grouped into 2 categories: middle-aged adults (40-64 years) and older adults (65-80 years). Gender (RIAGENDR) was classified as male or female. Race/ethnicity (RIDRETH3) was categorized as non-Hispanic White, non-Hispanic Black, Hispanic, and Other/Multiracial. Educational attainment (DMDEDUC2) was defined as less than high school, high school graduate/General Educational Development (GED) certificate, some college or associate (AA) degree, and college graduate or higher. Marital status (DMDMARTL) was categorized as married or living with a partner, never married, and widowed, divorced, or separated. Household income (INDHHIN2) was grouped into 3 levels: low income (<$25,000), middle income ($25,000–$74,999), and high (≥$75,000). Health insurance coverage (HIQ011) was classified as insured or uninsured. Diabetes status (DIQ010) was defined as present or absent based on self-reported physician diagnosis. Body mass index (BMI) and other comorbidities were not included in the primary analyses because they may lie within the causal pathway linking physical activity and sleep to hypertension, so adjusting for them could introduce overadjustment bias.
Analytic Sample
The analytic sample was derived from 29,400 participants across 3 combined NHANES cycles (2013-2018). Pregnant women (n = 11) and individuals outside the target age range of 40-80 years (n = 18,406) were excluded, leaving 10983 eligible participants.
A detailed evaluation of missing data was conducted for study variables. The number of participants with missing values was as follows: hypertension (n = 239), sleep category (n = 64), physical activity group (n = 53), marital status (n = 7), income (n = 1108), education (n = 11), insurance status (n = 9), and diabetes status (n = 359). Some missing values overlapped across participants. In total, 1850 participants were excluded due to missing data. After all exclusions, the final analytic sample included 9133 participants (Figure 1). Sample flow chart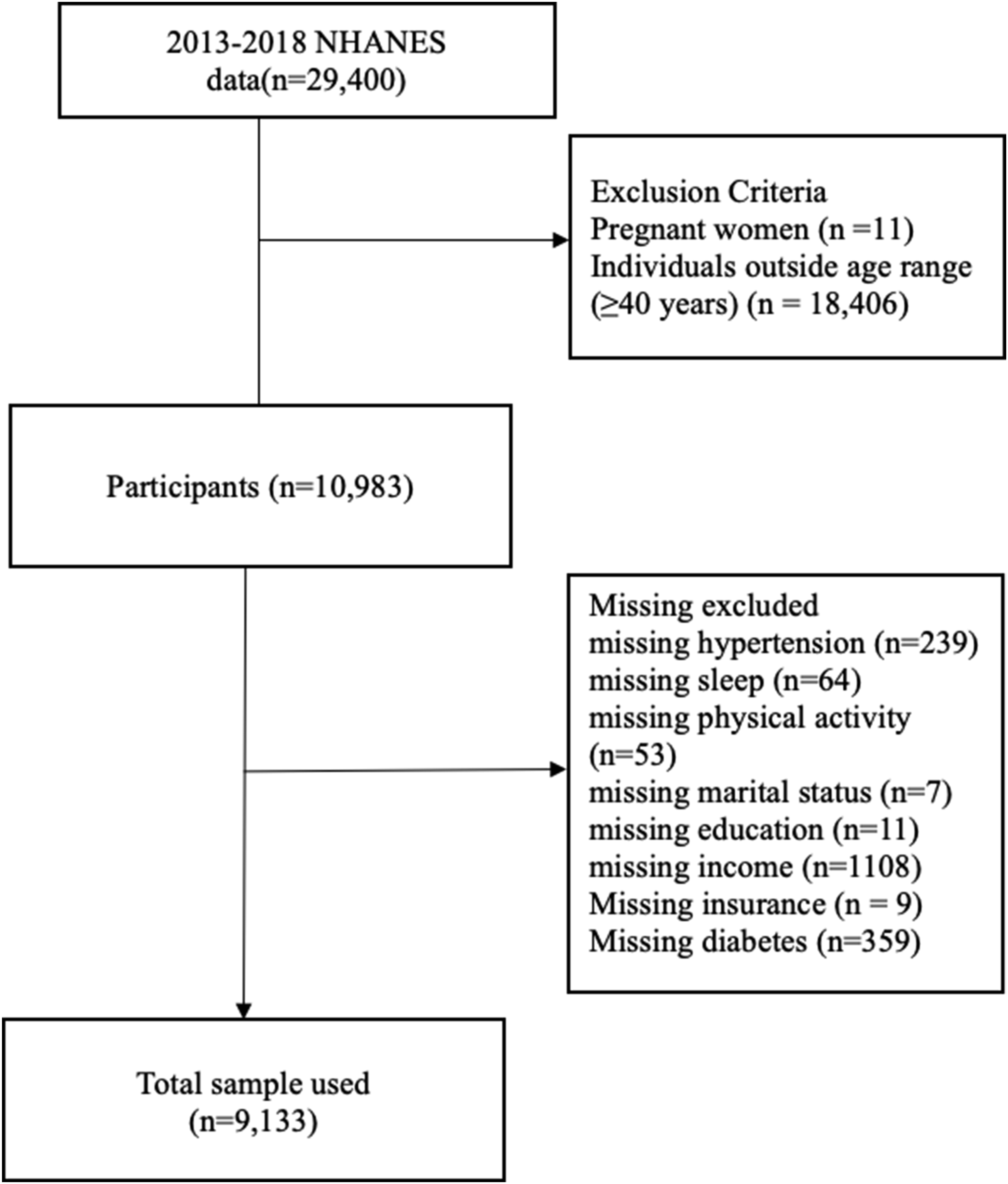
Data Analysis
All statistical analyses were performed using STATA version 19 (StataCorp LLC, College Station, TX). A complete-case approach was employed, excluding participants with missing data to obtain the final analytic sample. The complex NHANES survey design was accounted for by incorporating sample weights (WTMEC4YR), primary sampling units (SDMVPSU), and strata (SDMSTRA). Thus, in line with NHANES analytic guidelines, we adjusted the 2-year MEC weights by dividing them by 3 to account for the combination of 3 survey cycles. This adjustment addresses unequal selection probabilities and ensures accurate estimation of standard errors. Applying the NHANES sample design and weights allows the results to be generalized to the broader noninstitutionalized U.S. adult population.
Weighted Descriptive Statistics by Hypertension Status.
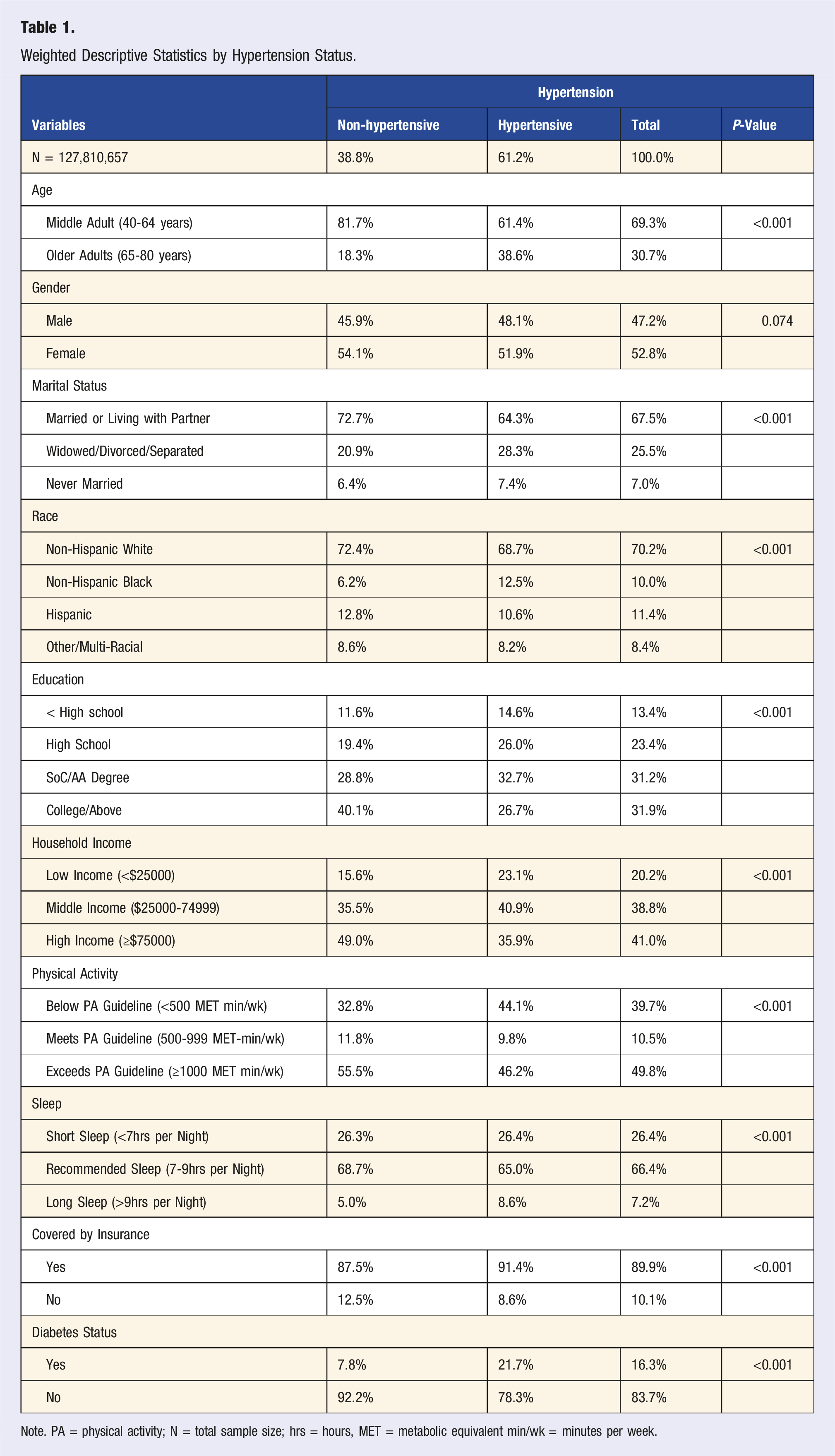
Note. PA = physical activity; N = total sample size; hrs = hours, MET = metabolic equivalent min/wk = minutes per week.
Weighted Descriptive Statistics by Age Groups.
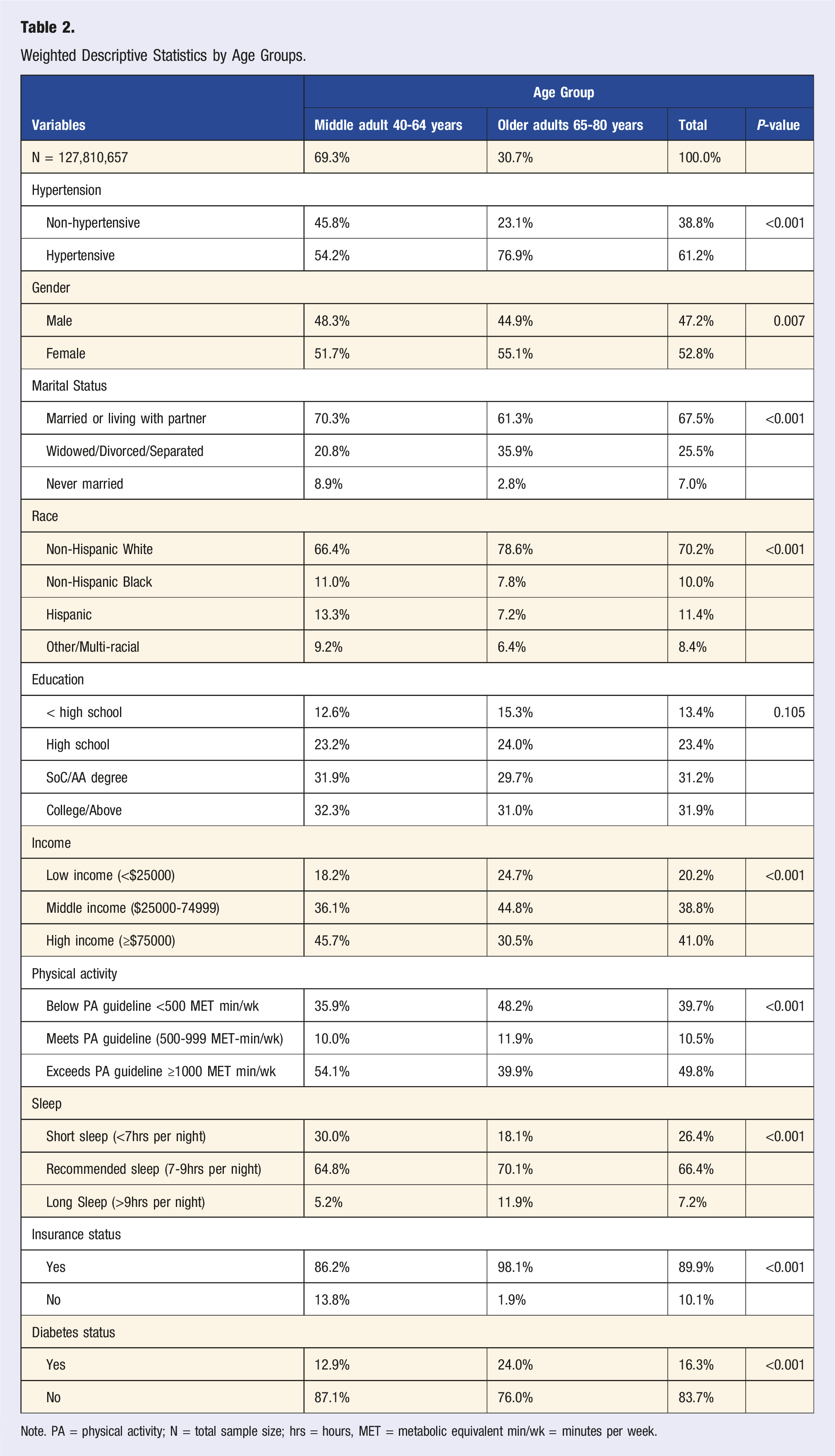
Note. PA = physical activity; N = total sample size; hrs = hours, MET = metabolic equivalent min/wk = minutes per week.
Weighted Multivariate Logistic Regression Showing Association Between Physical Activity, Sleep, and Hypertension Among US Middle-Aged and Older Adults.
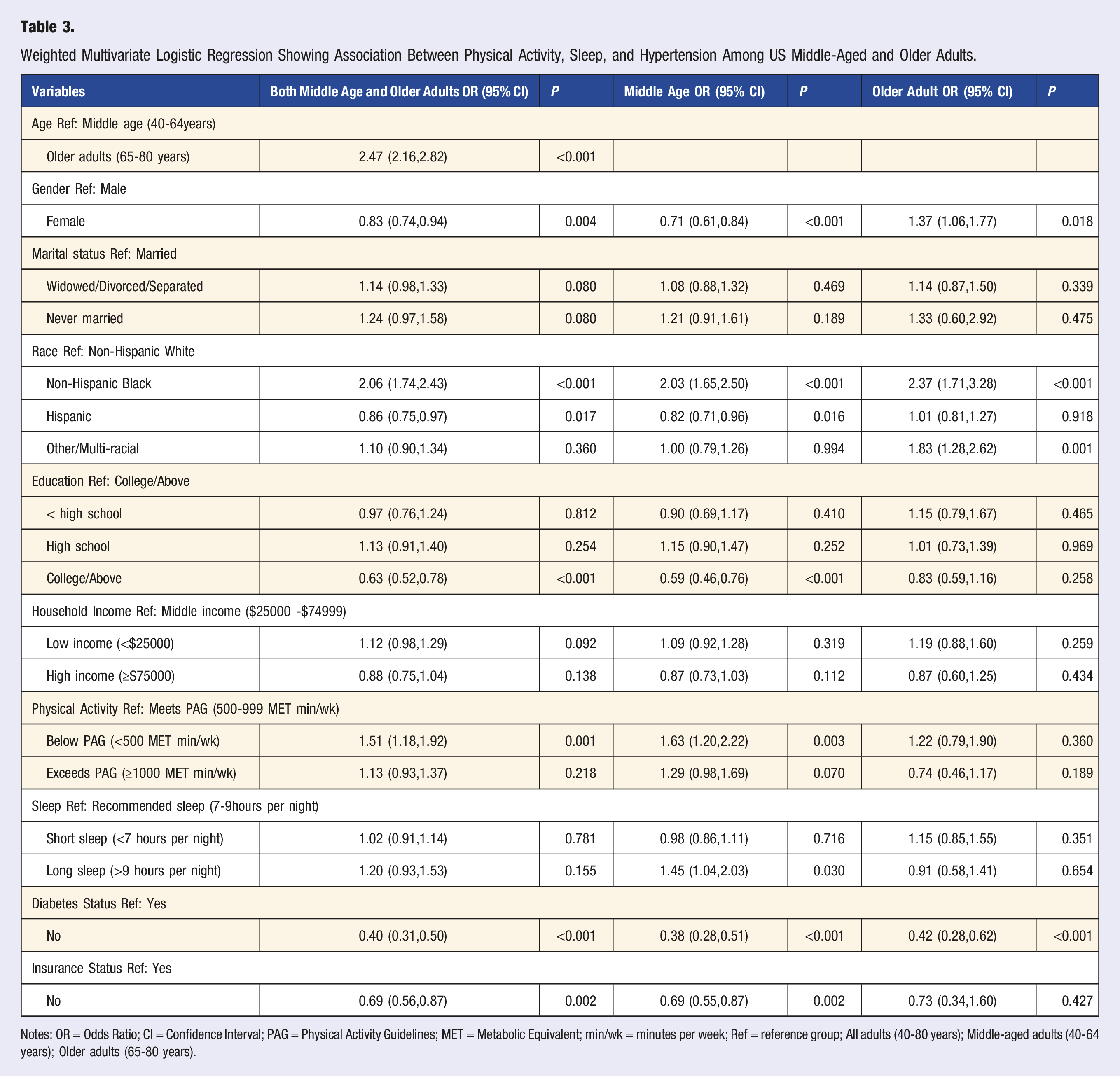
Notes: OR = Odds Ratio; CI = Confidence Interval; PAG = Physical Activity Guidelines; MET = Metabolic Equivalent; min/wk = minutes per week; Ref = reference group; All adults (40-80 years); Middle-aged adults (40-64 years); Older adults (65-80 years).
Results
A total of 9133 participants were included in this study representing a weighted sample of 127,810,657 U.S. adults aged 40-80 years. Overall, 61.2% of participants had hypertension (Table 1). Gender differences did not differ by hypertension status (P = 0.074). Adults with hypertension were less often married and more likely to be widowed, divorced, or separated (P < 0.001). Non-Hispanic Black adults had the highest prevalence of hypertension compared to other racial/ethnic groups (P < 0.001). Lower education and household income were associated with higher hypertension prevalence (P < 0.001). Adults who did not meet the physical activity guidelines exhibited higher prevalence of hypertension, while those exceeding physical activity guidelines were often individuals without hypertension (P < 0.001). Hypertension was more common among those reporting longer sleep duration (>9 hours per night) than those who met the recommended sleep durations (7-9 hours per night) (P < 0.001). Adults with hypertension had higher insurance coverage and were more likely to have diabetes (P < 0.001).
Moreover, in terms of age groups categories, older adults had a higher prevalence of hypertension (76.9%) compared to middle-aged adults (54.2%) (P < 0.001) (Table 2). Physical activity patterns differed by age groups, 48.2% of older adults were below the recommended physical activity guideline, while 54.1% of middle-aged adults exceeded physical activity guidelines (P < 0.001). However, sleep duration varied, short sleep was more common among middle-aged adults, whereas long sleep was more prevalent among older adults (P < 0.001).
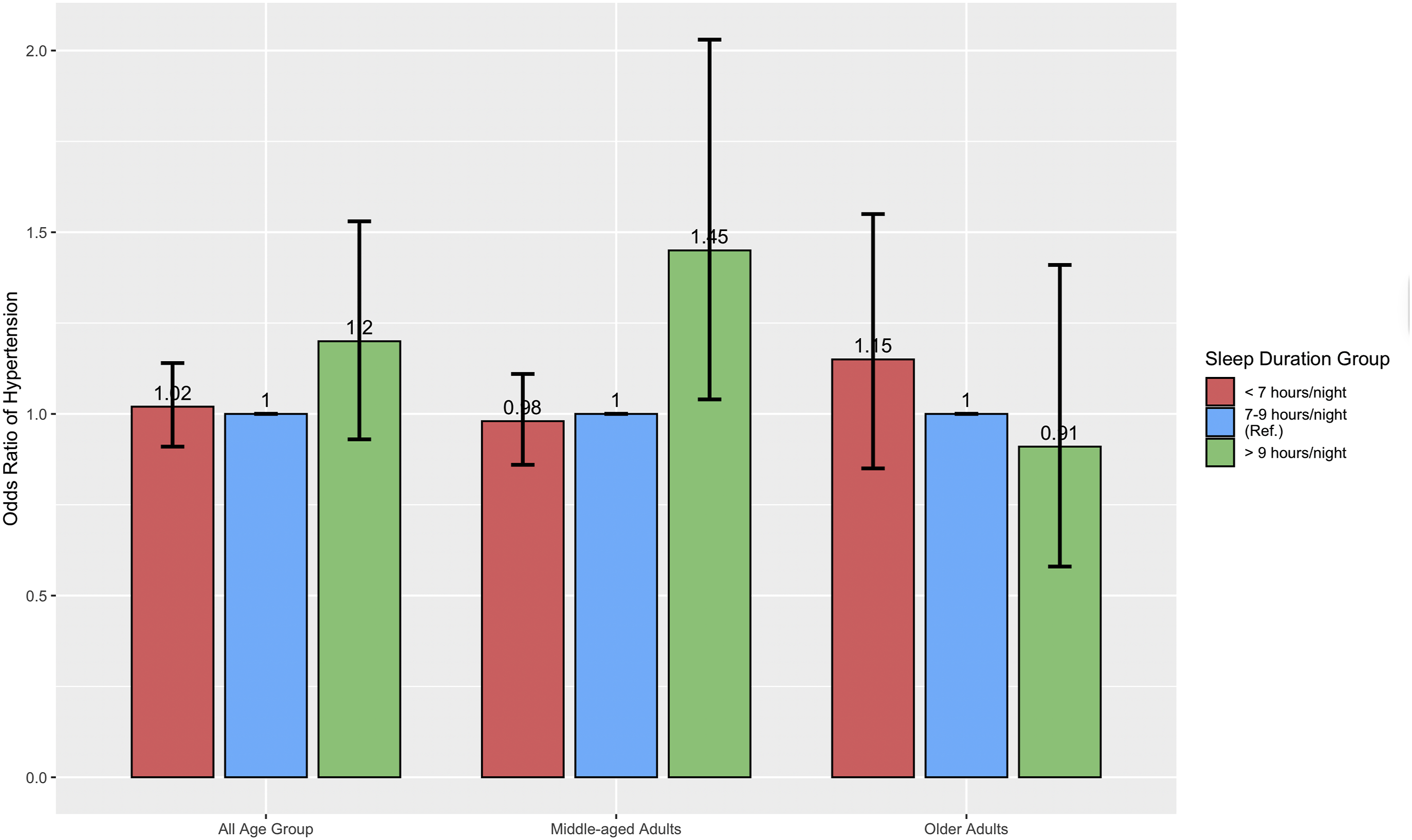
In the overall weighted sample of adults aged 40-80 years (Table 3), physical inactivity was significantly associated with higher odds of hypertension. Adults below physical activity guidelines (<500 MET-min/week) had higher odds of hypertension compared with those meeting physical activity guidelines (OR = 1.51, 95% CI: 1.18-1.92). Neither short sleep nor long sleep, were significantly associated with hypertension in the overall weighted sample.
When stratified by age, the results varied. Among middle-aged adults, those below physical activity guidelines had higher odds of hypertension (OR = 1.63, 95% CI: 1.20-2.22), compared to those who met the recommended physical activity guidelines (Figure 2). However, no significant relationship was observed for those who exceed the physical activity guidelines and hypertension. Also, middle-aged adults who had long sleep duration had higher odds of hypertension (OR = 1.45, 95% CI: 1.04-2.03) compared to those who met the recommended sleep guidelines. However, no significant associated was observed for short sleep and hypertension (Figure 3). Among older adults neither sleep durations nor physical activity were significantly associated with hypertension. Physical activity and hypertension: Odds ratio and 95% confidence interval Sleep duration and hypertension: Odds ratio and 95% confidence interval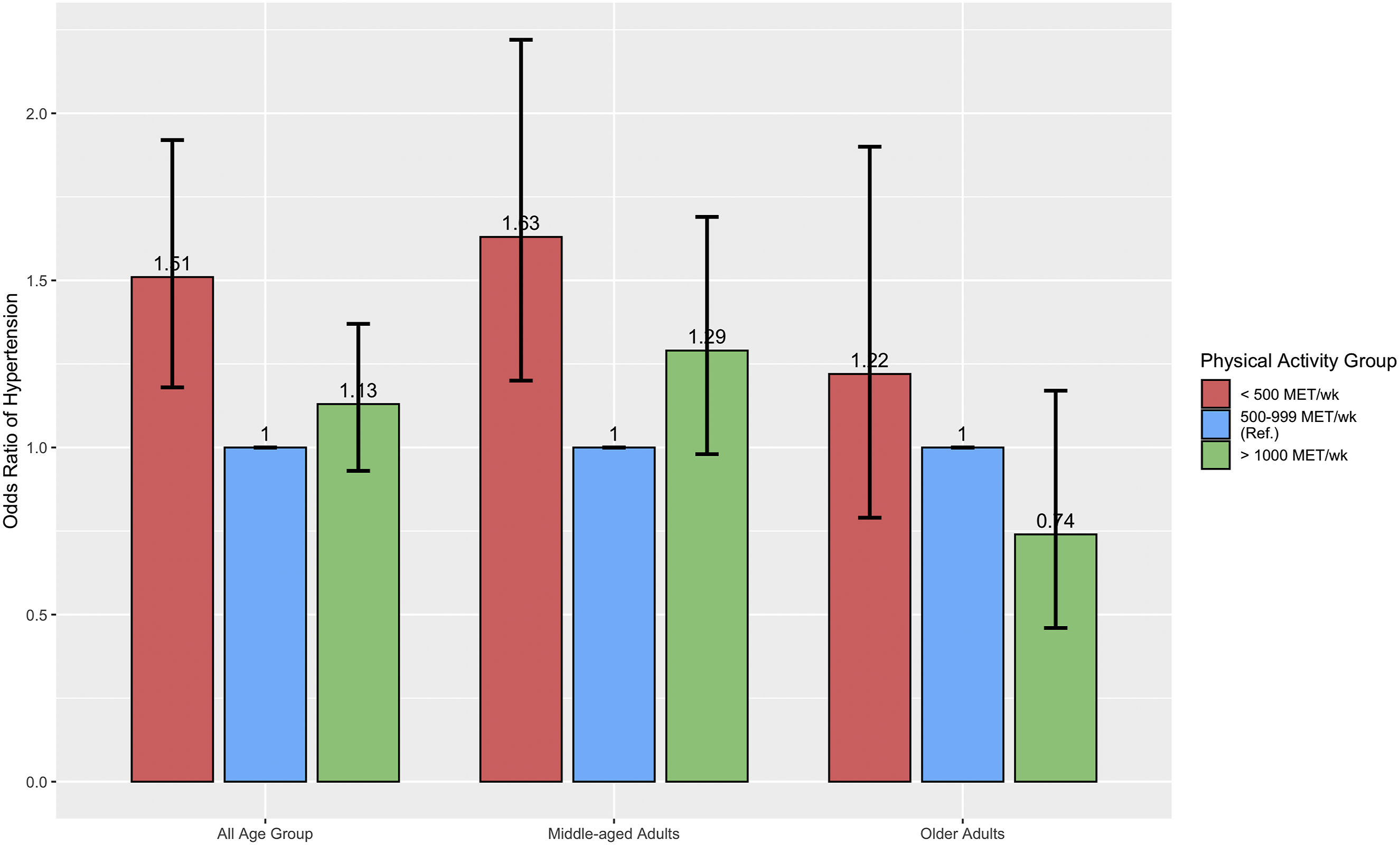
Discussion
The current study examined the relationship between physical activity, sleep duration, and hypertension, with a particular focus on age-specific patterns among middle-aged and older adults in the United States. The analysis conducted using NHANES data yielded several significant findings. We found that, not meeting physical activity guideline was associated with higher odds of hypertension in the overall sample and specifically among middle-aged adults. Long sleep duration was also associated with increased odds of hypertension among middle-aged adults, whereas short sleep duration was not significantly associated with hypertension in any age group. Among older adults, neither sleep duration nor physical activity showed significant associations with hypertension.
Our results highlight a significant association between physical activity and hypertension, particularly in middle-age. Consistent with prior studies, insufficient physical activity was associated with higher odds of hypertension in the overall sample. 30 However, this study extends the literature by demonstrating that the strength of this association differs by age. Specifically, low physical activity was more strongly associated with hypertension in middle-aged adults than in older adults.
These findings align with prior research demonstrating that insufficient physical activity contributes to increased odds of hypertension.31,32 The observed association in middle-aged adults supports evidence that midlife physical activity patterns are predictive of cardiovascular outcomes later in life. 31 There are greater cardiovascular benefits later in life for individuals who engage in vigorous or high-volume physical activity in early life.7,33 This study extends the literature by demonstrating that the strength of this association differs by age. Specifically, the relationship between low physical activity and hypertension was significant in middle-aged adults but not in older adults. In contrast, the lack of significant associations in older adults may reflect survivor bias or other age-related factors influencing blood pressure regulation, highlighting the complexity of hypertension etiology in later life.
To our knowledge, few nationally representative studies have examined whether the impact of physical activity on hypertension varies between middle-aged and older adults. Most prior research has either focused on general adult populations or targeted older adults.19,34 Thus, our findings suggest that middle-age may be a period during which physical activity is more strongly associated with hypertension prevalence. By identifying differential associations across age groups, this study provides novel evidence that physical activity may not weigh equally in hypertension prevention at all stages of adulthood.
The relationship between sleep and hypertension in our study exhibited greater complexity. Middle-aged adults, with longer sleep duration was associated with higher odds of hypertension. This finding aligns with existing literature that associates long sleep with cardiometabolic dysregulation, inflammation, and sleep disorders such as sleep apnea to higher odds of hypertension.35,36 However, this association did not persist in older adults. One explanation may be that extended sleep in middle-age may be associated with underlying health conditions or lifestyle factors associated with hypertension. Prior studies on sleep and hypertension have shown mixed results, with some reporting U-shaped associations, 35 and others finding no independent effect after accounting for comorbidities Our findings reinforce the need to contextualize sleep duration within broader health and age frameworks.
Collectively, these results emphasize adherence to physical activity recommendations as a modifiable lifestyle behavior that can reduce the burden of hypertension, particularly during middle-age, when the trajectory of cardiovascular health is often established. 37 Given the observed associations, maintaining adequate physical activity during this period may be associated with lower prevalence of hypertension and related health conditions later in life. 38 In contrast, the absence of significant associations in older adults suggests that interventions at later stages of life may require broader strategies that integrate management of multiple risk factors, including comorbidities, diet, stress, and medication adherence, rather than focusing solely on physical activity or sleep duration.
From a clinical perspective, these findings highlight the importance of incorporating both physical activity and sleep assessments into routine cardiovascular health evaluations in clinical practice. For middle-aged adults, screening for insufficient physical activity and prolonged sleep may help identify individuals with higher odds of hypertension, offering opportunities to provide targeted lifestyle guidance. Tailoring interventions to the life-course stage is essential while promoting guideline-concordant activity levels in midlife may yield the greatest benefits, approaches in older adulthood should be more comprehensive, addressing age-related changes, multimorbidity, and functional capacity. Together, these implications highlight the need for personalized, age-sensitive strategies in hypertension prevention and management.
Strengths and Limitations
This study has several strengths, including the use of a large, nationally representative sample, standardized blood pressure measurement. The simultaneous evaluation of physical activity and sleep across distinct age groups provides novel insights into how lifestyle factors influence hypertension across the life course. However, there are some limitations. The cross-sectional design precludes causal inference. Physical activity and sleep duration were self-reported, which may introduce recall and social desirability bias compared to objective measures.
Because this is a cross-sectional analysis, current physical activity may not reflect lifelong participation. Physical inactivity earlier in adulthood could have contributed to the development of hypertension in older adults, making it difficult to establish temporal relationships or rule out potential reverse causation. Also, study assessed only aerobic physical activity, as NHANES cycle used for this study (2013-2018) does not capture muscle-strengthening or balance activities, which also influence blood pressure and hypertension.
Finally, BMI and other comorbidities may act as intermediate variables between physical activity, sleep, and hypertension, so adjusting for them could distort the true associations of interest.
Future Directions
Future research should employ longitudinal designs to clarify causal pathways linking physical activity, sleep, and hypertension, and to determine whether interventions at specific life stages confer sustained cardiovascular benefits. Intervention studies are also needed to evaluate the effectiveness of promoting physical activity during midlife vs later life, and whether strategies should differ by age. Additionally, the role of sleep quality, circadian rhythms, and sleep disorders warrants further investigation, as these factors may interact with both aging and activity to influence the likelihood of hypertension.
Conclusion
In summary, this nationally representative analysis demonstrates that physical inactivity is strongly associated with hypertension in midlife, highlighting the importance of promoting guideline-concordant physical activity during this critical life stage. In contrast, no significant associations between physical activity or sleep duration and hypertension were observed among older adults, suggesting that the drivers of hypertension in later life may be more multifactorial and influenced by comorbidities or age-related physiologic changes. Long sleep duration was associated with hypertension among middle-aged adults but not among older adults, highlighting the need to consider age when interpreting sleep–blood pressure relationships. Collectively, these findings emphasize the importance of life course–specific strategies for hypertension prevention and management, with targeted promotion of physical activity in midlife and careful, context-specific assessment of sleep behaviors as integral components of cardiovascular health across aging populations.
Footnotes
Author Contributions
Dennis Miezah: Conceptualization, Data Analysis, Writing—Original Draft, Writing—Review and Editing.
Chaowalit Srisoem: Data Analysis, Writing—Review and Editing.
Rockson Ansong: Writing—Original Draft, Writing—Review and Editing.
Thomas Hinney: Writing—Review and Editing.
Richard Marfo: Writing—Review and Editing.
Musah Abubakari: Writing—Review and Editing.
Qian Song: Data Analysis, Writing—Review and Editing.
Funding
No funding was received for this study.
Declaration of Conflicting Interests
The authors declare no conflict of interest.
Data Availability Statement
Data is publicly available.